
The Knowledge and Use of the International Classification of Functioning, Disability and Health (ICF) Framework in Athletic Training
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedures
2.4. Data Analysis
3. Results
3.1. Participants
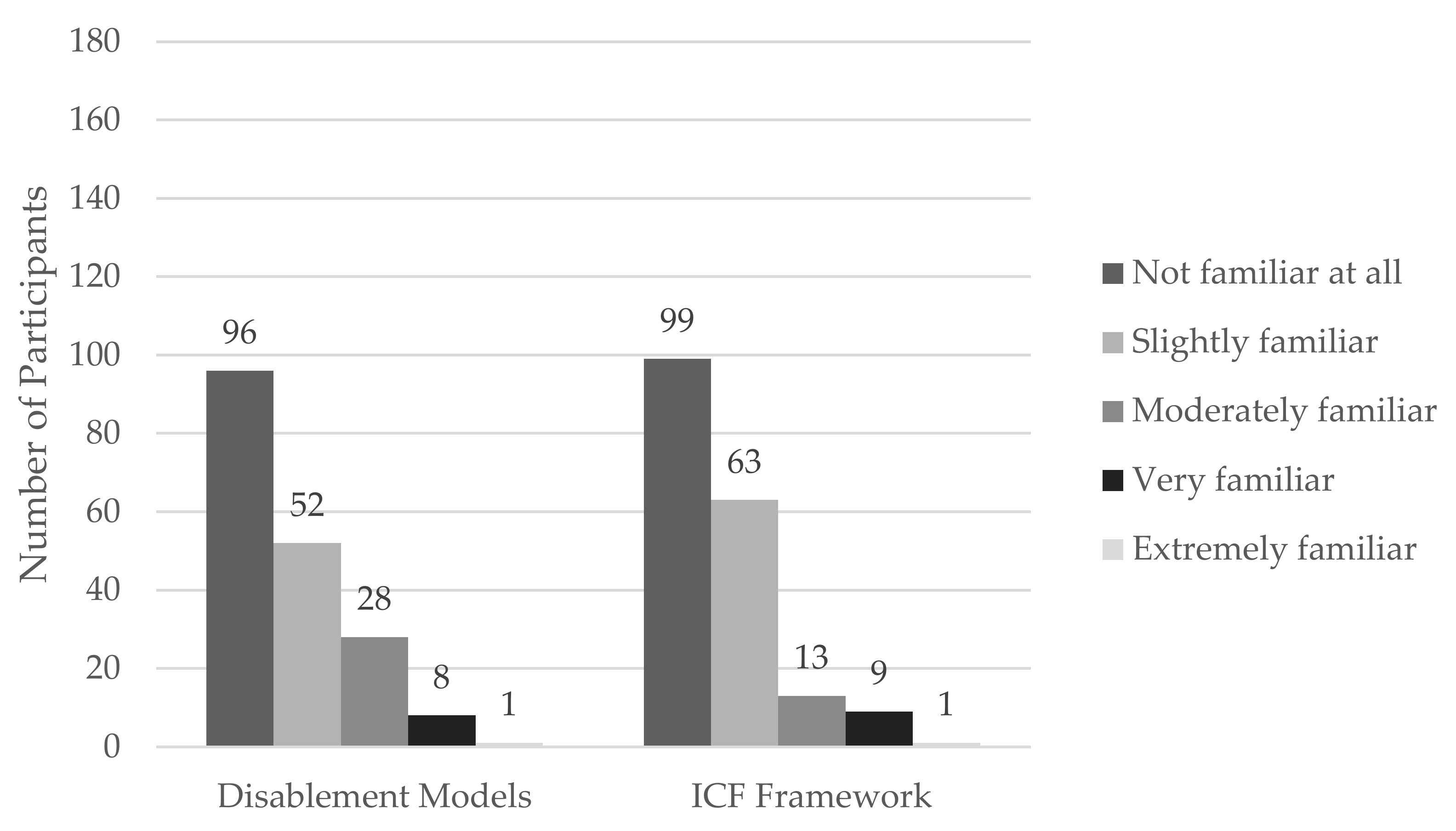
3.2. Familiarity and Knowledge
3.3. Sorting Application
3.4. Implementation and Use
4. Discussion
4.1. Familiarity with and Knowledge of Disablement Models
4.2. Application of the ICF Framework
4.3. Implementation of the ICF Framework in Clinical Practice
4.4. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Survey
| Question Type | Question |
| 1. Multiple Choice | Are you currently certified to practice Athletic Training by the Board of Certification (BOC) and do you treat patients on a daily basis? Yes (1) No (2) |
| 2. Multiple Choice | Do you agree to participate in this study? Yes, I agree to participate No, I do not agree to participate |
| 3. Fill in the Blank | What is your age? Please round to the nearest whole year |
| 4. Multiple Select | What gender do you identify as? Select all that apply Agender Genderqueer Man Transgender Man Non-binary/Gender Non-conforming Transgender Woman Woman Another option not listed here Prefer to self-describe Prefer not to say |
| 5. Multiple Select | What ethnicity do you identify as? Please select all that apply. American Indian/Alaskan Native/Indigenous Asian/Asian American Black/African American Hispanic/Latinx Native Hawaiian/Pacific Islander White/Caucasian 2 or more races Another option not listed here Prefer to self-describe Prefer not to say |
| 6. Multiple Choice | What is your current primary athletic training practice setting? If none apply, please select the one that most closely matches your current setting. Amateur, Rec or Youth Sports Clinic and Physician Practice College/University Health/Fitness/Sports Performance Clinic/Club Hospital Independent Contractor Military, Law Enforcement or Government Occupational Health (Industrial) Performing Arts Professional Sports Secondary School |
| 7. Fill in the Blank | How many years have you clinically practiced as a credentialed Athletic Trainer? Please round up to the nearest year |
| 8. Multiple Choice | What is the highest degree you have earned? Professional Bachelor’s Professional Master’s Post-Professional Master’s Post-Professional Clinical Doctorate (DAT) Academic Doctorate (PhD, EdD, etc.) Other: (Please write in your own response)____________________ |
| 9. Multiple Choice | How familiar are you with disablement models? Not familiar at all Slightly familiar Moderately familiar Very familiar Extremely familiar |
| 10. Multiple Choice | How familiar are you with the International Classification of Functioning, Disability, and Health (ICF) framework? Not familiar at all Slightly familiar Moderately familiar Very familiar Extremely familiar |
| 11. Multiple Select | How did you learn, if at all, about the ICF disablement framework? Mark all that apply. I have not learned about it During my Professional Athletic Training Program During my Post-Professional Athletic Training Program Continuing education session by an athletic trainer Continuing education session by a different healthcare provider Informally by a Colleague (another athletic trainer or different healthcare provider) Reading Journal Articles Informally through Self-Education (finding resources yourself) Required/Mandated In-Service by Employer Other |
| In This section, you will be asked to select the best answer related to the components of the ICF disablement framework. Please do not use outside resources | |
| 12. Multiple Choice | What component of the ICF framework does the following example describe? Physiological functions of body systems. Body function Body structure Activity Impairment I do not know |
| 13. Multiple Choice | What component of the ICF framework does the following example describe? The execution of a task or action by an individual. Participation Environmental factors Activity Body structure I do not know |
| 14. Multiple Choice | What component of the ICF framework does the following example describe? Problems an individual may experience during involvement in life situations. Participation restrictions Environmental factors Activity limitations Impairments I do not know |
| 15. Multiple Choice | What component of the ICF framework does the following example describe? Problems in body structure such as a significant deviation or loss. Participation restrictions Body functions Activity limitations Body structure impairments I do not know |
| 16. Multiple Choice | What component of the ICF framework does the following example describe? Difficulties an individual may have in executing tasks like lifting weights or combing hair. Activity Activity limitations Participation restrictions Participation I do not know |
| 17. Multiple Choice | What component of the ICF framework does the following example describe? Involvement in a life situation. Body functions Activity Participation Environmental factors I do not know |
| Please sort the statement into the correct ICF framework component by dragging the statement into the appropriate box. | |
| 18. Drag and Drop | Health Condition: Regulation of emotion Managing diet and fitness Individual attitudes of friends Muscles of shoulder region Generalized anxiety disorder Abuse of addictive drugs Heart rate Bursitis, related to use, overuse, or pressure Cornea Population density Living with family Managing daily routine Acute sinusitis Social cues in relationships Immediate family Female biological sex Power of muscles in lower half body Kidney |
| 19. Drag and Drop | Body Structures: Regulation of emotion Managing diet and fitness Individual attitudes of friends Muscles of shoulder region Generalized anxiety disorder Abuse of addictive drugs Heart rate Bursitis, related to use, overuse, or pressure Cornea Population density Living with family Managing daily routine Acute sinusitis Social cues in relationships Immediate family Female biological sex Power of muscles in lower half body Kidney |
| 20. Drag and Drop | Body Functions Regulation of emotion Managing diet and fitness Individual attitudes of friends Muscles of shoulder region Generalized anxiety disorder Abuse of addictive drugs Heart rate Bursitis, related to use, overuse, or pressure Cornea Population density Living with family Managing daily routine Acute sinusitis Social cues in relationships Immediate family Female biological sex Power of muscles in lower half body Kidney |
| 21. Drag and Drop | Activities and Participation: Regulation of emotion Managing diet and fitness Individual attitudes of friends Muscles of shoulder region Generalized anxiety disorder Abuse of addictive drugs Heart rate Bursitis, related to use, overuse, or pressure Cornea Population density Living with family Managing daily routine Acute sinusitis Social cues in relationships Immediate family Female biological sex Power of muscles in lower half body Kidney |
| 22. Drag and Drop | Environmental Factors: Regulation of emotion Managing diet and fitness Individual attitudes of friends Muscles of shoulder region Generalized anxiety disorder Abuse of addictive drugs Heart rate Bursitis, related to use, overuse, or pressure Cornea Population density Living with family Managing daily routine Acute sinusitis Social cues in relationships Immediate family Female biological sex Power of muscles in lower half body Kidney |
| 23. Drag and Drop | Personal Factors: Regulation of emotion Managing diet and fitness Individual attitudes of friends Muscles of shoulder region Generalized anxiety disorder Abuse of addictive drugs Heart rate Bursitis, related to use, overuse, or pressure Cornea Population density Living with family Managing daily routine Acute sinusitis Social cues in relationships Immediate family |
| Likert Scale Questions | |
| 24. Likert Scale | In terms of your patient load, and when relevant to the patient’s condition, how often do you elicit and/or document information on the functioning and disability of a patient specific to Impairments of Body Functions? (Never, Some Patients, About, Half the Patients, Most of my patients, and Always) Mental (ex: sleep, orientation, emotion) Sensory (ex: seeing, hearing, pain) Voice and Speech Cardiovascular, Hematological, Immunological, and Respiratory Systems (ex: heart, blood pressure, breathing, allergies) Digestive, Metabolic, and Endocrine Systems (ex: weight, hormones, defecation) Genitourinary and Reproductive (ex: urinary, sexual) Neuromusculoskeletal and Movement (ex: mobility, power, tone) Skin and Related Structures |
| 25. Multiple Choice | You selected you ‘never’ complete at least one or more of the tasks from the previous section. Please tell us why. Do not know what to do (1) Do not know how to do it (2) Did not know I should be doing it (3) Restricted from doing it (4) Will not do it (5) |
| 26. Likert Scale | In terms of your patient load, and when relevant to the patient’s condition, how often do you elicit and/or record information on the functioning and disability of a patient specific to Impairments of Body Structures? (Never, Some Patients, About, Half the Patients, Most of the patients, and Always) Nervous System structures (ex: brain, spinal cord, nerves) Eye, ear, and related structures Structures involved in voice and speech Structure of the cardiovascular, immunological, and respiratory systems Structures related to the digestive, metabolism, and endocrine systems Structures related to genitourinary and reproductive system Structure related to movement (ex: shoulder, pelvis, lower extremity) Skin and related structures |
| 27. Multiple Choice | You selected you ‘never’ complete at least one or more of the tasks from the previous section. Please tell us why. Do not know what to do (1) Do not know how to do it (2) Did not know I should be doing it (3) Restricted from doing it (4) Will not do it (5) |
| 28. Likert Scale | In terms of your patient load, how often do you elicit and/or document information on the functioning and disability of a patient specific to Activity Limitations and Participation? (Never, Some Patients, About, Half the Patients, Most of the patients, and Always) Learning and Applying Knowledge (ex: listening, watching, solving problems) General Tasks and Demands (ex: single tasks, multiple tasks) Communication (ex: spoken message, non-verbal message, conversation) Mobility (ex: lifting, carrying, grasping, driving) Self Care (ex: washing, toileting, dressing, eating, drinking) Domestic Life (ex: shopping, cooking, cleaning, assisting others) Interpersonal interactions and relationships (ex: basic, complex, strangers, social, family, intimate) Major life areas (ex: school, higher education, employment, economic self-sufficiency) Community, social, and civic life (ex: recreation, leisure, religion, spirituality, political life) |
| 29. Multiple Choice | You selected you ‘never’ complete at least one or more of the tasks from the previous section. Please tell us why. Do not know what to do (1) Do not know how to do it (2) Did not know I should be doing it (3) Restricted from doing it (4) Will not do it (5) |
| 30. Likert Scale | In terms of your patient load, how often do you elicit and/or document information on the functioning and disability of a patient specific to Environmental Factors? (Never, Some Patients, About, Half the Patients, Most of the patients, and Always) Products and technology (ex: food, medicine, transportation) Natural environment and human made changes to environment (ex: climate, light, sound) Support and relationships (ex: immediate family, friends, neighbors, health professionals) Attitudes (ex: individual attitudes of friends, societal attitudes, social norms, ideologies) Services, systems, and policies (ex: housing, transportation, education, health services, legal, social security) |
| 31. Multiple Choice | You selected you ‘never’ complete at least one or more of the tasks from the previous section. Please tell us why. Do not know what to do (1) Do not know how to do it (2) Did not know I should be doing it (3) Restricted from doing it (4) Will not do it (5) |
| 32. Likert Scale | In terms of your patient load, how often do you elicit and/or document information on the functioning and disability of a patient specific to Personal Factors? (Never, Some Patients, About, Half the Patients, Most of the patients, and Always) Lifestyle Habits Social Background Education Life Events Race/ethnicity Sexual orientation Individual psychological assets Age Gender Upbringing Food Preferences Fitness Coping Style |
| 33. Multiple Choice | You selected you ‘never’ complete at least one or more of the tasks from the previous section. Please tell us why. Do not know what to do (1) Do not know how to do it (2) Did not know I should be doing it (3) Restricted from doing it (4) Will not do it (5) |
References
- Commission on Accreditation of Athletic Training Education. Implementation and Guide to the CAATE 2020 Professional Standards; Commission on Accreditation of Athletic Training Education: Austin, TX, USA, 2018. [Google Scholar]
- Snyder Valier, A.R.; Bacon, C.E.W.; Lam, K.C. Disablement Model and Health-Related Quality of Life Classification for Patient-Reported Outcomes Measurement Information System (PROMIS) Instruments. J. Athl. Train. 2018, 53, 1206–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vela, L.I.; Denegar, C. Transient Disablement in the Physically Active with Musculoskeletal Injuries, Part I: A Descriptive Model. J. Athl. Train. 2010, 45, 615–629. [Google Scholar] [CrossRef] [Green Version]
- Sitzler, B. ICF Model: A Framework for Athletic Training Practice NATA News. 2016. Available online: https://www.nata.org/blog/beth-sitzler/icf-model-framework-athletic-training-practice (accessed on 23 February 2022).
- Parsons, J.T.; McLeod, T.C.V.; Snyder, A.R.; Sauers, E.L. Change Is Hard: Adopting a Disablement Model for Athletic Training. J. Athl. Train. 2008, 43, 446–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nottingham, S.L. Assessing Professional Students’ Application of the International Classification of Functioning, Health, and Disability Model and Patient-Reported Outcome Measures During Patient Care. Athl. Train. Educ. J. 2021, 16, 316–320. [Google Scholar] [CrossRef]
- Atkinson, H.L.; Nixon-Cave, K. A Tool for Clinical Reasoning and Reflection Using the International Classification of Functioning, Disability and Health (ICF) Framework and Patient Management Model. Phys. Ther. 2011, 91, 416–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snyder, A.R.; Parsons, J.T.; Valovich McLeod, T.C.; Curtis Bay, R.; Michener, L.A.; Sauers, E.L. Using disablement models and clinical outcomes assessment to enable evidence-based athletic training practice, part I: Disablement models. J. Athl. Train. 2008, 43, 428–436. [Google Scholar] [CrossRef] [Green Version]
- Bacon, C.E.W.; Van Lunen, B.L.; Hankemeier, D.A. Postprofessional Athletic Training Students’ Perceptions Concerning the Health Care Competencies. Athl. Train. Educ. J. 2018, 13, 309–323. [Google Scholar] [CrossRef] [Green Version]
- Lam, K.C.; Harrington, K.M.; Cameron, K.L.; Valier, A.R.S. Use of Patient-Reported Outcome Measures in Athletic Training: Common Measures, Selection Considerations, and Practical Barriers. J. Athl. Train. 2019, 54, 449–458. [Google Scholar] [CrossRef] [Green Version]
- Lam, K.C.; Marshall, A.N.; Valier, A.R.S. Patient-Reported Outcome Measures in Sports Medicine: A Concise Resource for Clinicians and Researchers. J. Athl. Train. 2020, 55, 390–408. [Google Scholar] [CrossRef] [Green Version]
- Wilson, C.J.; Eberman, L.E.; Redinger, A.S.; Neil, E.R.; Winkelmann, Z.K. Athletic trainers’ viewpoints of patient-centered care: Preliminary findings. PLoS ONE 2022, 17, e0274577. [Google Scholar] [CrossRef]
- World Health Organization. ICF Checklist Version 2.1 a, Clinician Form. 2007. Available online: http://who.int/classifications/icf/site/checklist/ictchecklist.pdf (accessed on 23 February 2022).
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Tzelepis, F.; Sanson-Fisher, R.W.; Zucca, A.C.; Fradgley, E.A. Measuring the quality of patient-centered care: Why patient-reported measures are critical to reliable assessment. Patient Prefer. Adherence 2015, 2015, 831–835. [Google Scholar] [CrossRef] [Green Version]
- Hankemeier, D.A.; Popp, J.K.; Walker, S.E. Familiarity with and Use of Clinical Prediction Rules and Patient-Rated Outcome Measures. Athl. Train. Sports Health Care 2017, 9, 108–123. [Google Scholar] [CrossRef]
- Landon, T.J.; Nay, A.; Connor, A.; Phillips, B.N.; Reyes, A.R.; Leavitt, J. Exploring the Relationship Between Familiarity with the ICF and Rehabilitation Counselor Confidence in Facilitating Workplace Accommodations. Rehabil. Res. Policy Educ. 2021, 35, 129–142. [Google Scholar] [CrossRef]
- Williams, R.M.; Welch, C.E.; Parsons, J.T.; McLeod, T.C.V. Athletic Trainers’ Familiarity with and Perceptions of Academic Accommodations in Secondary School Athletes After Sport-Related Concussion. J. Athl. Train. 2015, 50, 262–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pernambuco, A.P.; Lana, R.D.C.; Polese, J.C. Knowledge and use of the ICF in clinical practice by physiotherapists and occupational therapists of Minas Gerais. Fisioter. E Pesqui. 2018, 25, 134–142. [Google Scholar] [CrossRef] [Green Version]
- Jafri, S.K.; Camargo, O.K.d. Knowledge and use of the international classification of functioning, disability and health (ICF) among health professionals in a developing country. Pak. J. Neurol. Sci. PJNS 2020, 15, 23–25. [Google Scholar]
- Choudhry, N.K.; Fletcher, R.H.; Soumerai, S.B. Systematic Review: The Relationship between Clinical Experience and Quality of Health Care. Ann. Intern. Med. 2005, 142, 260–273. [Google Scholar] [CrossRef]
- Board of Certification. Continuing Professional Certification 2022. Available online: https://bocatc.org/newsroom/cpc?category_key=at (accessed on 7 February 2023).
- World Health Organization. ICF Browser 2017 English Version. Available online: https://apps.who.int/classifications/icfbrowser/ (accessed on 7 February 2023).
- Towards a Common Language for Functioning, Disability and Health: ICF, the International Classification of Functioning, Disability and Health [Internet]. The Organization. 2002. Available online: https://books.google.com/books?id=XWFUAQAACAAJ (accessed on 7 February 2023).
- Horn, K.K.; Jennings, S.; Richardson, G.; van Vliet, D.; Hefford, C.; Abbott, J.H. The Patient-Specific Functional Scale: Psychometrics, Clinimetrics, and Application as a Clinical Outcome Measure. J. Orthop. Sports Phys. Ther. 2012, 42, 30–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, R.T.; Burton, D.; Pickering, M.A.; Start, A. Confirmatory Factor Analysis of the Disablement in the Physically Active Scale and Preliminary Testing of Short-Form Versions: A Calibration and Validation Study. J. Athl. Train. 2019, 54, 302–318. [Google Scholar] [CrossRef] [Green Version]
- Nye, E.A.; Crossway, A.; Rogers, S.M.; Games, K.E.; Eberman, L.E. Lesbian, Gay, Bisexual, Transgender, and Queer Patients: Collegiate Athletic Trainers’ Perceptions. J. Athl. Train. 2019, 54, 334–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkman, L.F. Assessing the physical health effects of social networks and social support. Annu. Rev. Public Health 1984, 5, 413–432. [Google Scholar] [CrossRef] [PubMed]
- Diez Roux, A.V. Investigating neighborhood and area effects on health. Am. J. Public Health 2001, 91, 1783–1789. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | n, % |
|---|---|
| Gender | |
| Woman | 122, 65.9% |
| Man | 60, 32.4% |
| Transgender Man | 1, 0.5% |
| Prefer to Self-Describe | 2, 1.1% |
| Ethnicity | |
| White/Caucasian | 159, 85.9% |
| American Indian/Alaskan Native/Indigenous | 1, 0.5% |
| Asian/Asian American | 1, 0.5% |
| Black/African American | 5, 2.7% |
| Hispanic/Latinx | 5, 2.7% |
| Native Hawaiian/Pacific Islander | 1, 0.5% |
| 2 or more races | 9, 4.9% |
| Another option not listed | 1, 0.5% |
| Prefer not to say | 3, 1.6% |
| Job Setting | |
| Amateur, Recreation or Youth Sports | 2, 1.1% |
| Clinicand Physician Practice | 15, 8.1% |
| College/University | 77, 41.6% |
| Health/Fitness/Sports/Performance Enhancement Hospital | 2, 1.1% |
| Independent Contractor | 1, 0.5% |
| Military, Law Enforcement and Government | 1, 0.5% |
| Occupational Health and Industrial | 9, 4.9% |
| Performing Arts | 12, 6.5% |
| Professional Sports | 3, 1.6% |
| Secondary School | 5, 2.7% |
| 58, 31.4% |
| Learning Method | n, % |
|---|---|
| I have not learned about it | 96/185, 51.9% |
| I have learned about it (Select all that apply) | 89/185, 48.1% |
| During my Professional Athletic Training Program | 24 |
| During my Post-Professional Athletic Training Program | 24 |
| Informally by a colleague | 18 |
| Informally through self-education | 18 |
| Continuing education session by an athletic trainer | 17 |
| Reading journal articles | 14 |
| Continuing education session by a different healthcare provider | 8 |
| Required/Mandated in-service by employer | 6 |
| Other | 5 |
| Question stem: What Component of the ICF Framework Does the Following Example Describe? | Correct Answer | Participants Answering Correctly (n, %) |
|---|---|---|
| Physiological functions of body systems | Body Function | 106, 57.3% |
| The execution of a task or action by an individual | Activity | 97, 52.4% |
| Problems an individual may experience during involvement in life situations | Participation Restrictions | 28, 15.1% |
| Problems in body structure such as significant deviation or loss | Body Structure Impairments | 112, 60.5% |
| Anatomical parts of the body such as organs, limbs, and their components | Body Structures | 133, 71.9% |
| The physical, social, and attitudinal environment in which people live and conduct their lives | Environmental Factors | 111, 60.0% |
| Difficulties an individual may have in executing tasks like lifting weights or combing hair | Activity Limitations | 117, 63.2% |
| Involvement in a life situation | Participation | 91, 49.2% |
| ICF Framework Component | Correct ICF Framework Major Category | Correctly Sorted (n, %) |
|---|---|---|
| Regulation of emotion | Body function | 44, 23.8% |
| Managing diet and fitness | Activity | 85, 45.9% |
| Individual attitudes of friends | Environmental | 86, 46.5% |
| Muscles of shoulder region | Body structure | 141, 76.2% |
| Generalized anxiety disorder | Health condition | 122, 65.9% |
| Abuse of addictive drugs | Personal | 42, 22.7% |
| Heart rate | Body function | 131, 70.8% |
| Bursitis related to use, overuse, and pressure | Health condition | 119, 64.3% |
| Cornea | Body structure | 141, 76.2% |
| Population density | Environmental | 141, 76.2% |
| Living with family | Personal | 26, 14.1% |
| Managing daily routine | Activity | 115, 62.2% |
| Acute Sinusitis | Health condition | 141, 76.2% |
| Social cues in relationships | Activity | 20, 10.8% |
| Immediate family | Environmental | 74, 40.0% |
| Female biological sex | Personal | 52, 28.1% |
| Power of muscles in lower half of body | Body function | 121, 65.4% |
| Kidney | Body structure | 140, 75.7% |
| Impairments | Never Elicited | Some Patients | About Half of My Patients | Most of My Patients | Always Elicited | Did Not Answer |
|---|---|---|---|---|---|---|
| Mental (ex: sleep, orientation, emotion) | 19, 10.3% | 70, 37.8% | 26, 14.1% | 30, 16.2% | 11, 5.9% | 29, 15.7% |
| Sensory (ex: seeing, hearing, pain) | 25, 13.5% | 39, 21.1% | 12, 6.5% | 44, 23.8% | 36, 19.5% | 29, 15.7% |
| Voice and Speech | 77, 41.6% | 55, 29.7% | 2, 1.1% | 16, 8.6% | 5, 2.7% | 30, 16.2% |
| Cardiovascular, Hematological, Immunological, and Respiratory Systems (ex: heart, blood pressure, breathing, allergies) | 20, 10.8% | 70, 37.8% | 22, 11.9% | 29, 15.7% | 14, 7.6% | 30, 16.2% |
| Digestive, Metabolic, and Endocrine Systems (ex: weight, hormones, defecation) | 41, 22.2% | 75, 40.5% | 19, 10.3% | 14, 7.6% | 6, 3.2% | 30, 16.2% |
| Genitourinary and Reproductive (ex: urinary, sexual) | 67, 36.2% | 67, 36.2% | 10, 5.4% | 9, 4.9% | 1, 0.5% | 31, 16.8% |
| Neuromusculoskeletal and Movement (ex: mobility, power, tone) | 9, 4.9% | 20, 10.8% | 7, 3.8% | 54, 29.2% | 65, 35.1% | 30, 16.2% |
| Skin and Related Structures | 19, 10.3% | 55, 29.7% | 32, 17.3% | 37, 20% | 12, 6.5% | 30, 16.2% |
| Impairments | Never Elicited | Some Patients | About Half of My Patients | Most of My Patients | Always Elicited | Did Not Answer |
|---|---|---|---|---|---|---|
| Nervous System structures (ex: brain, spinal cord, nerves) | 11, 5.9% | 56, 30.3% | 24, 13% | 29, 15.7% | 24, 13% | 41, 22.2% |
| Eye, ear, and related structures | 14, 7.6% | 78, 42.2% | 20, 10.8% | 19, 10.3% | 14, 7.6% | 40, 21.6% |
| Structures involved in voice and speech | 49, 26.5% | 72, 38.9% | 3, 1.6% | 11, 5.9% | 10, 5.4% | 40, 21.6% |
| Structure of the cardiovascular, immunological, and respiratory systems | 20, 10.8% | 75, 40.5% | 19, 10.3% | 17, 9.2% | 14, 7.6% | 40, 21.6% |
| Structures related to the digestive, metabolism, and endocrine systems | 37, 20% | 73, 39.5% | 14, 7.6% | 13, 7% | 8, 4.3% | 40, 21.6% |
| Structures related to genitourinary and reproductive system | 51, 27.6% | 73, 39.5% | 6, 3.2% | 8, 4.3% | 7, 3.8% | 40, 21.6% |
| Structure related to movement (ex: shoulder, pelvis, lower extremity) | 8, 4.3% | 18, 19.7% | 8, 4.3% | 48, 25.9% | 63, 34.1% | 40, 21.6% |
| Skin and related structures | 13, 7% | 62, 33.5% | 20, 10.8% | 32, 17.3% | 18, 9.7% | 40, 21.6% |
| Limitation | Never Elicited | Some Patients | About Half of My Patients | Most of My Patients | Always Elicited | Did Not Answer |
|---|---|---|---|---|---|---|
| Learning and Applying Knowledge (ex: listening, watching, solving problems) | 27, 14.6% | 56, 30.3% | 17, 9.2% | 21, 11.4% | 18, 9.7% | 46, 24.9% |
| General Tasks and Demands (ex: single tasks, multiple tasks) | 26, 14.1% | 46, 24.9% | 21, 11.4% | 28, 15.1% | 19, 10.3% | 45, 24.3% |
| Communication (ex: spoken message, non-verbal message, conversation) | 28, 15.1% | 50, 27% | 19, 10.3% | 29, 15.7% | 14, 7.6% | 45, 24.3% |
| Mobility (ex: lifting, carrying, grasping, driving) | 9, 4.9% | 21, 11.4% | 18, 9.7% | 47, 25.4% | 45, 24.3% | 45, 24.3% |
| Self Care (ex: washing, toileting, dressing, eating, drinking) | 28, 15.1% | 57, 30.8% | 15, 8.1% | 24, 13% | 14, 7.6% | 47, 25.4% |
| Domestic Life (ex: shopping, cooking, cleaning, assisting others) | 42, 22.7% | 46, 24.9% | 18,9.7% | 26, 14.1% | 8, 4.3% | 45, 24.3% |
| Interpersonal interactions and relationships (ex: basic, complex, strangers, social, family, intimate) | 40, 21.6% | 63, 34.1% | 19, 10.3% | 11, 5.9% | 6, 3.2% | 46, 24.9% |
| Major life areas (ex: school, higher education, employment, economic self-sufficiency) | 28, 15.1% | 53, 28.6% | 17, 9.2% | 30, 16.2% | 11, 5.9% | 46, 24.9% |
| Community, social, and civic life (ex: recreation, leisure, religion, spirituality, political life) | 44, 23.8% | 47, 25.4% | 18, 9.7% | 22, 11.9% | 8, 4.3% | 46, 24.9% |
| Factor | Never Elicited | Some Patients | About Half of My Patients | Most of My Patients | Always Elicited | Did Not Answer |
|---|---|---|---|---|---|---|
| Products and technology (ex: food, medicine, transportation) | 22, 11.9% | 55, 29.7% | 21, 11.4% | 34, 18.4% | 4, 2.2% | 49, 26.5% |
| Natural environment and human made changes to environment (ex: climate, light, sound) | 31, 16.8% | 66, 35.7% | 19, 10.3% | 18, 19.7% | 2, 1.1% | 49, 26.5% |
| Support and relationships (ex: immediate family, friends, neighbors, health professionals) | 19, 10.3% | 63, 34.1% | 23, 12.4% | 27, 14.6% | 4, 2.2% | 49, 26.5% |
| Attitudes (ex: individual attitudes of friends, societal attitudes, social norms, ideologies) | 23, 12.4% | 61, 33.0% | 27, 14.6% | 22, 11.9% | 3, 1.6% | 49, 26.5% |
| Services, systems, and policies (ex: housing, transportation, education, health services, legal, social security) | 30, 16.2% | 69, 37.3% | 18, 9.7% | 16, 8.6% | 3, 1.6% | 49, 26.5% |
| Factor | Never Elicited | Some Patients | About Half of My Patients | Most of My Patients | Always Elicited | Did Not Answer |
|---|---|---|---|---|---|---|
| Lifestyle | 21, 11.4% | 56, 30.3% | 20, 10.8% | 28, 15.1% | 9, 4.9% | 51, 27.6% |
| Habits | 21, 11.4% | 53, 28.6% | 24, 13.0% | 28, 15.1% | 8, 4.3% | 51, 27.6% |
| Social Background | 32, 17.3% | 70, 37.8% | 12, 6.5% | 15, 8.1% | 5, 2.7% | 51, 27.6% |
| Education | 43, 23.2% | 54, 29.2% | 8, 4.3% | 23, 12.4% | 6, 3.2% | 51, 27.6% |
| Life Events | 16, 8.6% | 65, 35.1% | 20, 10.8% | 26, 14.1% | 7, 3.8% | 51, 27.6% |
| Race/ethnicity | 59, 31.9% | 48, 25.9% | 5, 2.7% | 16, 8.6% | 6, 3.2% | 51, 27.6% |
| Sexual orientation | 71, 38.4% | 51, 27.6% | 4, 2.2% | 7, 3.8% | 1, 0.5% | 51, 27.6% |
| Individual psychological assets | 31, 16.8% | 68, 36.8% | 15, 8.1% | 17, 9.2% | 3, 1.6% | 51, 27.6% |
| Age | 27, 14.6% | 45, 24.3% | 12, 6.5% | 18, 9.7% | 32, 17.3% | 51, 27.6% |
| Gender | 37, 20.0% | 42, 22.7% | 7, 3.8% | 21, 11.4% | 27, 14.6% | 51, 27.6% |
| Upbringing | 55, 29.7% | 56, 30.3% | 12, 6.5% | 11, 5.9% | 0, 0.0% | 51, 27.6% |
| Food Preferences | 40, 21.6% | 59, 31.9% | 13, 7.0% | 20, 10.8% | 2, 1.1% | 51, 27.6% |
| Fitness | 11, 5.9% | 41, 22.2% | 18, 9.7% | 39, 21.1% | 25, 13.5% | 51, 27.6% |
| Coping Style | 36, 19.5% | 48, 25.9% | 28, 15.1% | 18, 9.7% | 4, 2.2% | 51, 27.6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Millet, N.J.; Snyder Valier, A.R.; Eberman, L.E.; Rivera, M.J.; Winkelmann, Z.K. The Knowledge and Use of the International Classification of Functioning, Disability and Health (ICF) Framework in Athletic Training. Int. J. Environ. Res. Public Health 2023, 20, 5401. https://doi.org/10.3390/ijerph20075401
Millet NJ, Snyder Valier AR, Eberman LE, Rivera MJ, Winkelmann ZK. The Knowledge and Use of the International Classification of Functioning, Disability and Health (ICF) Framework in Athletic Training. International Journal of Environmental Research and Public Health. 2023; 20(7):5401. https://doi.org/10.3390/ijerph20075401
Chicago/Turabian StyleMillet, Nathaniel J., Alison R. Snyder Valier, Lindsey E. Eberman, Matthew J. Rivera, and Zachary K. Winkelmann. 2023. "The Knowledge and Use of the International Classification of Functioning, Disability and Health (ICF) Framework in Athletic Training" International Journal of Environmental Research and Public Health 20, no. 7: 5401. https://doi.org/10.3390/ijerph20075401