

Management of Hypoplastic or Hypomineralized Defects with Resin Infiltration at Pediatric Ages: Systematic Review

Abstract
:1. Introduction
2. Materials and Methods

{kind=link}
| Author. Year | Study | Methodology | Material Used | Statistical Treatment |
|---|---|---|---|---|
| Hasmun, N. 2020 [7] | Experimental longitudinal intervention study. | Adapted survey. | Child Oral Health Impact Profile Short Form 19 questionnaire. | (SPSS v24.0, IBM Corp., Chicago, IL, EE. UU.) |
| Moradi, S. 2021 [8] | Observational cross-sectional study | Original survey on dental procedures in dental and postgraduate students. | Adapted thanks to the International Caries Consensus Collaboration (ICCC) | Frequencies and percentages. |
| Memis B. 2015 [9] | Experimental “in vitro” study | Power analysis (Power and Precision software ver. 4, Biostat, Englewood, NJ, USA | Stereomicroscope (Leica MZ12, Leica Microsystems, Wetzlar, Germany | SPSS software (ver. 20; Chicago, IL, USA). Mann–Whitney U test. Kruskal–Wallis |
| Swamy, D. 2017 [10] | Experimental “in vitro” study | Extracted and treated teeth to assess penetration | Stereomicroscope (20x, Stemi SV 11, Carl Zeiss, Oberkochen, Germany) | SPSS (SPSS Inc., Released 2009. PASW Statistics for Windows, Version 18.0. Chicago, IL, USA |
| Bhandari, R. 2019 [11] | RCT “in vivo” | Randomized clinical trial | CIELAB method | ANOVA and post hoc Tukey’s test |
| Mattos-Silveira, J. 2015 [12] | RCT | Parallel groups | Wong-Baker faces scale | SPSS software (ver. 20; Chicago, IL, USA |
| Hasmun, N. 2018 [13] | Experimental prospective intervention study | Survey | Child Oral Health Impact Profile Short Form 19 questionnaire | (SPSS) v24.0 (IBM Corp., Chicago, IL, USA |
| Bagher, S.M 2018 [14] | RCT Split mouth | Test—control Temporary molars. | NaF alone in the control group or combined with resins. | NA |
| Turska-Szybka A 2014 [15] | Experimental “in vitro” study | Extracted primary molars shoving white spots on smooth surfaces | Vickers micro-hardness test. Depth of infiltration and microhardness were evaluated. | NA |
| Kabaktchieva, R. 2014 [16] | Experimental “in vivo” study | Light-induced fluorescence (SoploLife chamber) | NA | |
| Muñoz M. 2012 [17] | Case report | NA | Dean’s classification7 system | NA |
| Ammari, MM 2017 [18] | RCT Split mouth | CliniView | Facial Image Scale Cariogram model | SPSS software (SPSS Inc., Chicago, USA-version 22) |
| Studies | Significance Level | Conclusions |
|---|---|---|
| Hasmun, N. 2020 [7] | p < 0.001 | Quality of life is significantly improved. |
| Memis B. 2015 [9] | p ≤ 0.05 | Fluoride varnish + resin infiltration significantly inhibited the progression of the lesion in deciduous teeth. |
| Bhandari, R. 2019 [11] | p ≤ 0.001 | Microabrassion CPP-ACFP, bring better esthetic results. |
| Hasmun, N. 2018 [13] | p ≤ 0.05 | Stain removal, positive impact on children’s well-being. |
| Bagher, S.M 2018 [14] | p = 0.04 | Resin infiltration + NaF, better results. |
| Turska-Szybka A 2014 [15] | - | Icon® infiltrates at least half the depth of enamel lesions in deciduous teeth. |
| Title and Abstract | 1 |  |
| Introduction Context/basics | 2 | |
| Objective | 3 | |
| Methods Study design | 4 | |
| Context | 5 | |
| Participants | 6 | - |
| Variables | 7 | |
| Data sources | 8 |  |
| Biases | 9 | |
| Sample size | 10 | |
| Quantitative variables | 11 | |
| Statistical methods | 12 | |
| Results Participants | 13 |  |
| Descriptive data | 14 | |
| Data of the results variables | 15 | |
| Participants results | 16 | |
| Other analysis | 17 | |
| Discussion Key results | 18 | |
| Limitations | 19 | |
| Interpretation | 20 | |
| Generalizability | 21 | |
| Other information Financing | 22 | |
| Total | - | 13/22 |
| Items | Hasmun, N. 2020 [7] | Bhandari, R. 2019 [11] | Hasmun, N. 2018 [13] | Bagher, S.M. 2018 [14] | Swamy, D.F. 2017 [10] | Ammari, MM 2017 [18] | Mattos-Silveira, J. 2015 [12] | Memis B. 2015 [9] | Turska- A 2014 [15] | Kabaktchieva, R. 2014 [16] |
|---|---|---|---|---|---|---|---|---|---|---|
| The selection criteria were specified | pg.7 | pg.2 | pg.3 | pg.4 | pg.1 | pg.2 | pg.2 | v pg.2 | v pg.2 | v pg.2 |
| Subjects were randomly assigned to groups | pg.7 | | v pg.5 | v pg.6 | v pg.2 | pg.6 | | v pg.2 | v pg.2 | v pg.2 |
| The allocation was hidden | pg.7 | | pg.5 | pg.6 | v pg.2 | pg.6 | | v pg.2 | v pg.2 | v pg.2 |
| The groups were similar at baseline with respect to the most important prognostic indicators. | pg.7 y 10 | pg.4 | pg.4 | pg.5 | pg.2 | pg.3 | pg.3 | pg.2-3 | pg.2-3 | pg.3 |
| All subjects were blinded. | pg.8 | | pg.5 | pg.6 | pg.2 | pg pg.6 | | v pg.2 | v pg.2 | v pg.3 |
| All therapists were blinded. | pg.8 | | pg.5 | pg.6 | pg.2 | pg.2 | pg.2 | v pg.2 | v pg.2 | v pg.3 |
| All assessors were blinded. | pg.8 | | pg.5 | pg.6 | pg.2 | pg pg.2 | pg.2 | v pg.2 | v pg.2 | v pg.3 |
| Means were obtained from more than 85% subjects. | pg.10 | pg.4 | pg.6 | pg.7 | pg.3 | pg.4 | pg.4 | pg.4 | pg.4 | pg.3 |
| Results from all subjects were presented. | pg.10 | pg.4 | pg.6 | pg.7 | pg.3 | pg.4 | pg.4 | pg.4 | pg.4 | pg.3 |
| Statistical comparison results between groups were reported for at least one key outcome. | pg.9 | pg.4 | pg.7 | pg.8 | pg.2 | pg.2 | pg.3 | pg.4 | pg.4 | pg.3 |
| The study provides point and variability measures for at least one key outcome | pg.9 | | pg.7 | pg.8 | pg.3 | pg.2 | | pg.4 | pg.4 | pg.3 |
| Total: | 6/11 | 5/11 | 6/11 | 6/11 | 6/11 | 11/11 | 7/11 | 5/11 | 5/11 | 4/11 |
| 1.Clinical History | |
| 2.Target behaviors | |
| 3.Desing | |
| 4.Baseline | |
| 5.Treatment behavior | |
| 6.Raw data | |
| 7.Interrater reliability | |
| 8.Independence of assessors | |
| 9.Statistical analysis | |
| 10.Replication | |
| 11.Generalizatino | |
| Total | 5/11 |
3. Results
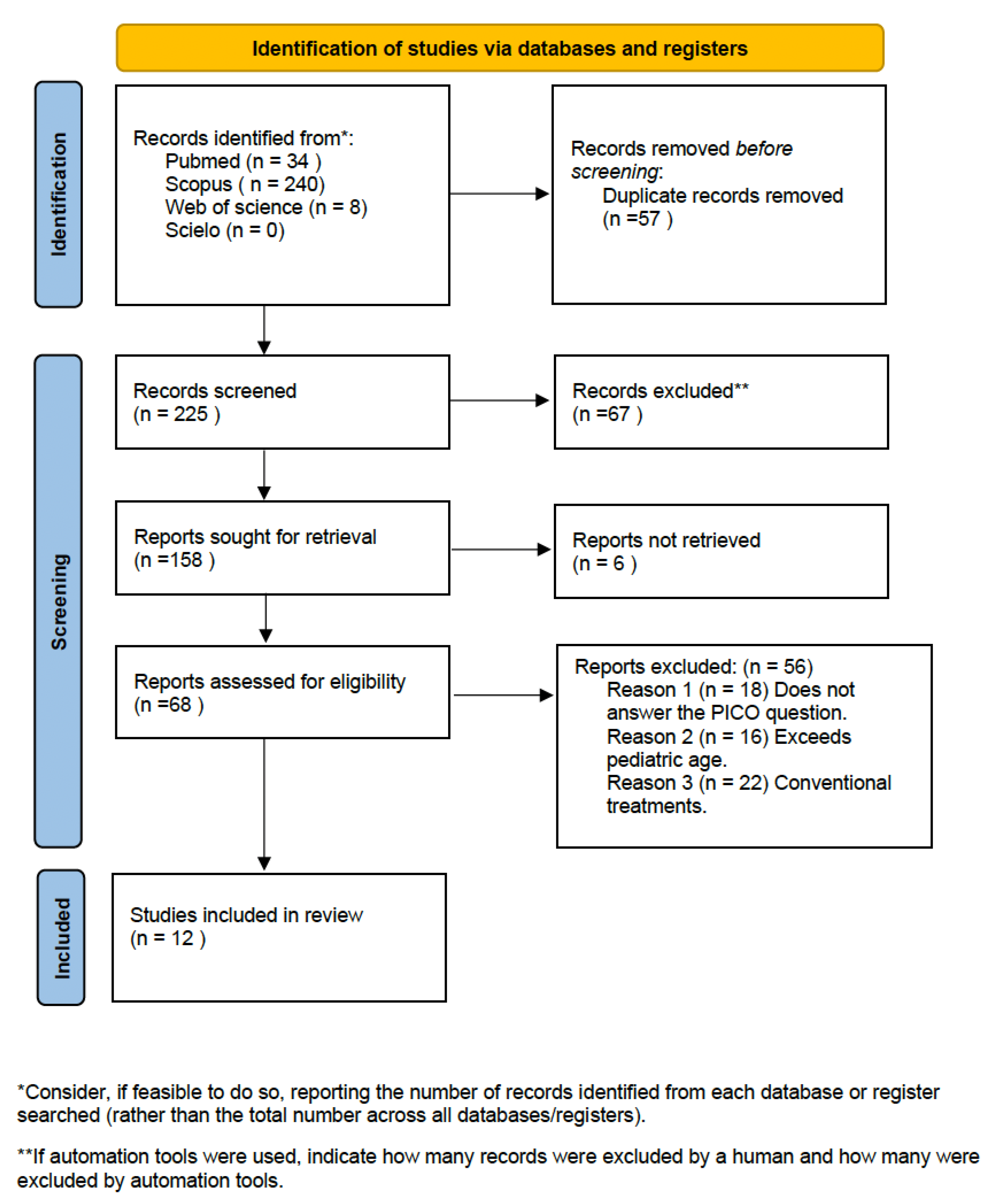
3.1. Study Selection and Flow Diagram—Study Results
3.2. Results of Individual Studies, Meta-Analysis and Additional Analyses
3.3. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Acosta, M.G.; Natera, A. Level of knowledge concerning enamel defects and their treatment among pediatric dentists. ALOP 2021, 7, 25–34. [Google Scholar]
- Meyer-Lueckel, H.; Paris, S. Improved resin infiltration of natural caries lesions. J. Dent. Res. 2008, 87, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Masri, A.A.b.H.A.; Khang, K.K.Y.; Shen, L.L.W.; Ekambaram, M.; Loch, C. Knowledge of dental enamel defects amongst undergraduate dental students—A cross-sectional survey. Eur. J. Dent. Educ. 2021, 25, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Bourouni, S.; Dritsas, K.; Kloukos, D.; Wierichs, R.J. Efficacy of resin infiltration to mask post-orthodontic or non-post-orthodontic white spot lesions or fluorosis–a systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 4711–4719. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Bren, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 89, 105906. [Google Scholar]
- Buela, G. Evaluation of the quality of articles and scientific journals: Proposal for the weighted impact factor and a quality index. Psicothema 2003, 15, 23–25. [Google Scholar]
- Hasmun, N.; Vettore, M.V.; Lawson, J.A.; Elcock, C.; Zaitoun, H.; Rodd, H.D. Determinants of children’s oral health-related quality of life following aesthetic treatment of enamel opacities. J. Dent. 2020, 98, 103372. [Google Scholar] [CrossRef] [PubMed]
- Moradi, S.; Sabbagh, S.; Timms, L.; Ravaghi, V. Teaching Minimally Invasive Interventions in Paediatric Dentistry: A Cross-Sectional Survey of Dental Schools in Iran. BMC Oral Health 2021, 23, 368. [Google Scholar] [CrossRef] [PubMed]
- Ozgul, B.M.; Orhan, K.; Oz, F.T. Micro-computed tomographic analysis of progression of artificial enamel lesions in primary and permanent teeth after resin infiltration. J. Oral Sci. 2015, 57, 177–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swamy, D.F.; Barretto, E.S.; Mallikarjun, S.B.; Dessai, S.S.R. In vitro Evaluation of Resin Infiltrant Penetration into White Spot Lesions of Deciduous Molars. J. Clin. Diagn. Res. 2017, 11, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, R.; Thakur, S.; Singhal, P.; Chauhan, D.; Jayam, C.; Jain, T. In vivo Comparative Evaluation of Esthetics after Microabrasion and Microabrasion followed by Casein Phosphopeptide-Amorphous Calcium Fluoride Phosphate on Molar Incisor Hypomineralization-Affected Incisors. Contemp. Clin. Dent. 2019, 10, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Mattos-Silveira, J.; Floriano, I.; Ferreira, F.R.; Viganó, M.E.; Mendes, F.M.; Braga, M.M. Children′s discomfort may vary among different treatments for initial approximal caries lesions: Preliminary findings of a randomized controlled clinical trial. Int. J. Paediatr. Dent. 2015, 25, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Hasmun, N.; Lawson, J.; Vettore, M.V.; Elcock, C.; Zaitoun, H.; Rodd, H. Change in Oral Health-Related Quality of Life Following Minimally Invasive Aesthetic Treatment for Children with Molar Incisor Hypomineralisation: A Prospective Study. Dent. J. 2018, 6, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagher, S.M.; Hegazi, F.M.; Finkelman, M.; Ramesh, A.; Gowharji, N.; Swee, G.; Felemban, O.; Loo, C.Y. Radiographic Effectiveness of Resin Infiltration in Arresting Incipient Proximal Enamel Lesions in Primary Molars. Pediatr. Dent. 2018, 40, 95–200. [Google Scholar]
- Turska-Szybka, A. Resin infiltration of natural caries lesions on smooth surfaces of primary teeth–In vitro studies. Dent. Med. Probl. 2014, 53, 308–317. [Google Scholar]
- Kabaktchieva, R. The role of light-induced fluorescence in the treatment of smooth surface carious lesions with icon infiltration and the results after 1 year. Acta Medica Bulg. 2014, 41, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, M.A.; Arana-Gordillo, L.A.; Gomes, G.M.; Gomes, O.M.; Bombarda, N.H.; Reis, A.; Loguercio, A.D. Alternative esthetic management of fluorosis and hypoplasia stains: Blending effect obtained with resin infiltration techniques. J. Esthet. Restor. Dent. 2013, 25, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Ammari, M.M.; Jorge, R.C.; Souza, I.P.R.; Soviero, V.M. Efficacy of resin infiltration of proximal caries in primary molars: 1-year follow-up of a split-mouth randomized controlled clinical trial. Clin. Oral Investig. 2018, 22, 1355–1362. [Google Scholar] [CrossRef] [PubMed]
- Leal, S.C. Minimal intervention dentistry in the management of the paediatric patient. Br. Dent. J. 2014, 216, 623–627. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casaña-Ruiz, M.D.; Marqués Martínez, L.; García Miralles, E. Management of Hypoplastic or Hypomineralized Defects with Resin Infiltration at Pediatric Ages: Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 5201. https://doi.org/10.3390/ijerph20065201
Casaña-Ruiz MD, Marqués Martínez L, García Miralles E. Management of Hypoplastic or Hypomineralized Defects with Resin Infiltration at Pediatric Ages: Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(6):5201. https://doi.org/10.3390/ijerph20065201
Chicago/Turabian StyleCasaña-Ruiz, María Dolores, Laura Marqués Martínez, and Esther García Miralles. 2023. "Management of Hypoplastic or Hypomineralized Defects with Resin Infiltration at Pediatric Ages: Systematic Review" International Journal of Environmental Research and Public Health 20, no. 6: 5201. https://doi.org/10.3390/ijerph20065201