
The Lived Self-Care Experiences of Patients Undergoing Long-Term Haemodialysis: A Phenomenological Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
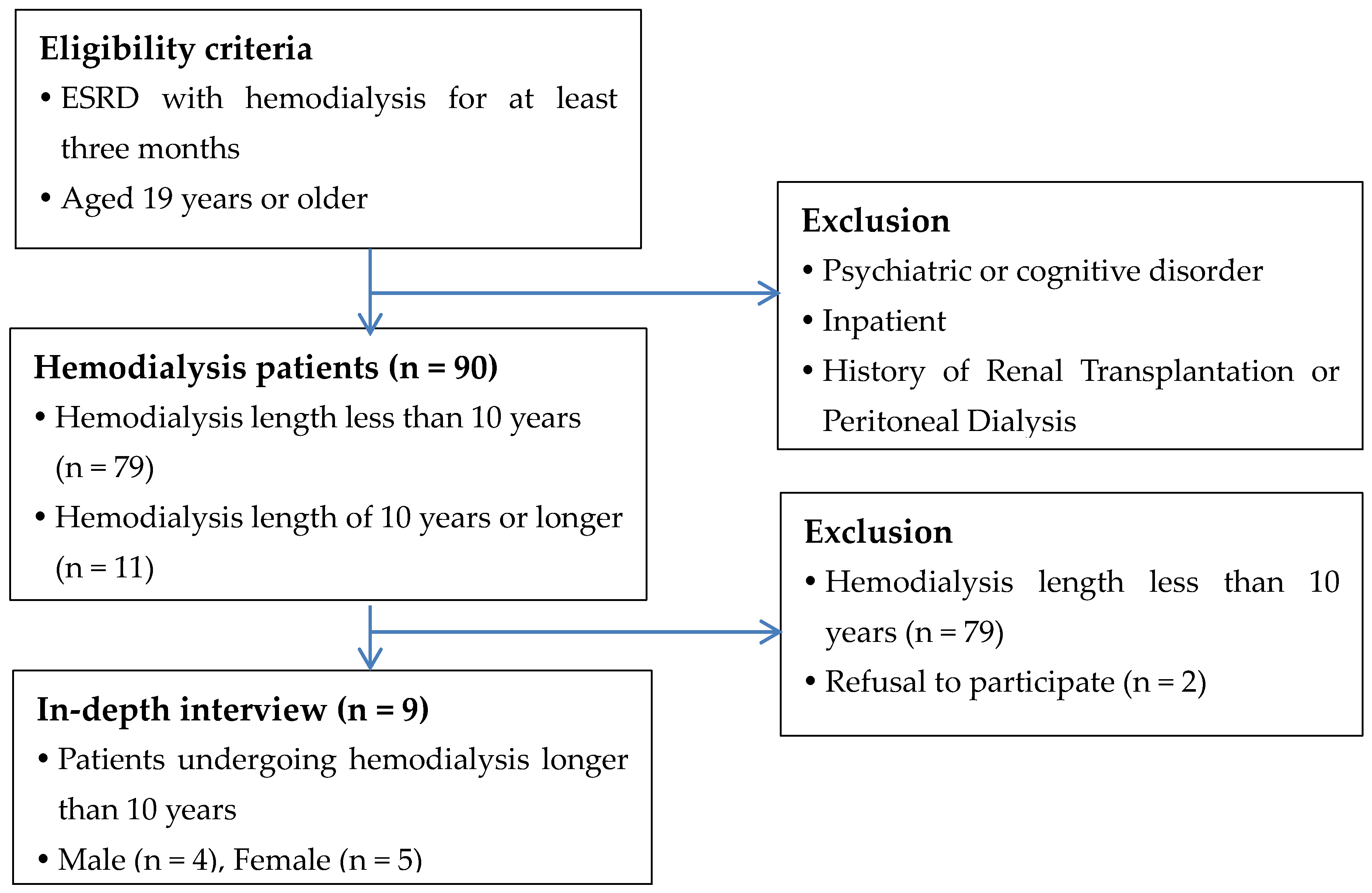
2.2. Participants
2.3. Data Collection
2.4. Data Analysis


{kind=link}
| Participant ID | Gender | Age (Years) | Hemodialysis Period | Causes of Disease | Family Living Together with Participant |
|---|---|---|---|---|---|
| P1 | Female | 74 | 10 year 7 month | Diabetes Mellitus | Son, granddaughters |
| P2 | Female | 72 | 11 year 5 month | Hypertension | Husband |
| P3 | Male | 75 | 10 year 4 month | Unknown | Wife |
| P4 | Male | 60 | 18 year 10 month | Hypertension | None |
| P5 | Male | 69 | 13 year 6 month | Hypertension | Wife, son, daughter |
| P6 | Male | 62 | 10 year 8 month | Hypertension | Wife |
| P7 | Female | 66 | 10 year 5 month | Diabetes Mellitus | None |
| P8 | Female | 51 | 16 year 7 month | Hypertension | Husband |
| P9 | Female | 62 | 16 year 4 month | Unknown | Daughter |
| Participant | First Step | Second Step | Third Step |
|---|---|---|---|
| P8 | “…[During hemodialysis] as I watch television, close my eyes, and think this and that…. those thoughts of “Why should I live like this?” and “What did I do wrong?” come to mind. Sometimes, I lie down and cry. But rather than people suffering from cancer and chemotherapy, it’s still possible to live on hemodialysis, so I got this kind of comfort…Let’s just be grateful that I can live on dialysis like this.” | “…[During haemodialysis] As I watch television, close my eyes, and think this and that…./ Those thoughts of “Why should I live like this?” and “What did I do wrong?” come to mind./ Sometimes, I lie down and cry./ But rather than people suffering from cancer, chemotherapy, it’s still possible to live on hemodialysis, so I got this kind of comfort…/ Let’s just be grateful that I can live on dialysis like this.” |
|
2.5. Validity and Reliability
2.6. Ethical Considerations
3. Results
3.1. Participants’ Characteristics
3.2. Themes
3.2.1. Theme 1. The Desire to Keep Living despite Challenges
‘I have more thoughts of living now…I have to live 80 years old, don’t I? But I do not even know if I am 100 years old (laughing). When we are all at the clinic, oh, no, we are all gathered again to live like this (laughing). We say this: as we receive a bundle of medicine, tons of medicine, we say that we have a lot of precious medicine that is good for the body.’(Participant 1)
3.2.2. Theme 2. Creating One’s Own Dietary Principles
‘I used to mostly eat at restaurants on my way home after haemodialysis; however, this was not very good for me. (After eating out) I craved water. My blood pressure increased, and then I needed to take pills to control my blood pressure. So, I decided to cook and eat at home as much as I can, even if it is hard.’(Participant 8)
3.2.3. Theme 3. Moving One’s Body with Remaining Strength
‘I’ve been exercising ever since I’ve been sick… for my body. I do not overexert myself, and I feel better little by little doing it like that. I feel a certain amount of lively energy.’(Participant 6)
3.2.4. Theme 4. Moving toward Independence
‘This is not a curable disease. I am just maintaining life. If I do not get haemodialysis, my body swells up, and it is hard. As I have experienced, I try to overcome that… I can do it with my own strength. I try to do things myself. Even though I get support from others, [being dependent] is not going to help me or cure my disease.’(Participant 3)
4. Discussion
- Physical self-care
- Emotional self-care
5. Conclusions
6. Strengths and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Orem, D.E.; Taylor, S.G.; Renpenning, K.M. Nursing: Concepts of Practice, 5th ed.; Library of Congress: St. Louis, MO, USA, 1995. [Google Scholar]
- Denyes, M.J.; Orem, D.E.; Bekel, G. Self-care: A foundational science. Nurs. Sci. Q. 2001, 14, 48–54. [Google Scholar] [CrossRef]
- Curtin, R.B.; Sitter, D.C.; Schatell, D.; Chewning, B.A. Self-management, knowledge, and functioning and well-being of patients on hemodialysis. Nephrol. Nurs. J. 2004, 31, 378–386, 396. [Google Scholar] [PubMed]
- Siregar, C.T.; Nasution, S.Z.; Ariga, R.A.; Harahap, I.A.; Tanjung, D.; Rasmita, D.; Ariadni, D.K. Self-care of patients during hemodialysis: A qualitative study. Enferm. Clín. 2021, 31, 588–592. [Google Scholar] [CrossRef]
- Reid, C.; Seymour, J.; Jones, C. A thematic synthesis of the experiences of adults living with hemodialysis. Clin. J. Am. Soc. Nephrol. CJASN 2016, 11, 1206–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biruete, A.; Jeong, J.H.; Barnes, J.L.; Wilund, K.R. Modified nutritional recommendations to improve dietary patterns and outcomes in hemodialysis patients. J. Ren. Nutr. 2017, 27, 62–70. [Google Scholar] [CrossRef]
- Logan, A.G.; Mente, A. Diet Patterns—A Neglected Aspect of Hemodialysis Care. J. Am. Soc. Nephrol. 2018, 29, 1581–1582. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.M.; Reston, J.D.; Bieraugel, R.; Da Silva Gane, M.; Wellsted, D.; Offredy, M.; Farrington, K. You cannot choose your family: Sociological ambivalence in the hemodialysis unit. Qual. Health Res. 2015, 25, 27–39. [Google Scholar] [CrossRef] [Green Version]
- Griva, K.; Mooppil, N.; Seet, P.; Krishnan, D.S.P.; James, H.; Newman, S.P. The NKF-NUS hemodialysis trial protocol—A randomized controlled trial to determine the effectiveness of a self management intervention for hemodialysis patients. BMC Nephrol. 2011, 12, 4. [Google Scholar] [CrossRef] [Green Version]
- Clark-Cutaia, M.N.; Sevick, M.A.; Thurheimer-Cacciotti, J.; Hoffman, L.A.; Snetselaar, L.; Burke, L.E.; Zickmund, S.L. Perceived Barriers to Adherence to Hemodialysis Dietary Recommendations. Clin. Nurs. Res. 2019, 28, 1009–1029. [Google Scholar] [CrossRef]
- Lee, E.J.; Chang, A.K.; Chung, Y.C. Socioecological factors affecting fluid restriction adherence among korean patients receiving hemodialysis: A qualitative study. J. Transcult. Nurs. 2021, 32, 239–247. [Google Scholar] [CrossRef]
- Pio, T.M.T.; Prihanto, J.B.; Jahan, Y.; Hirose, N.; Kazawa, K.; Moriyama, M. Assessing Burden, Anxiety, Depression, and Quality of Life among Caregivers of Hemodialysis Patients in Indonesia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 4544. [Google Scholar] [CrossRef] [PubMed]
- Sass, R.; Finlay, J.; Rossum, K.; Soroka, K.V.; McCormick, M.; Desjarlais, A.; Bohm, C. Patient, caregiver, and provider perspectives on challenges and solutions to individualization of care in hemodialysis: A qualitative study. Can. J. Kidney Health Dis. 2020, 7, 2054358120970715. [Google Scholar] [CrossRef]
- Hejazi, S.S.; Hosseini, M.; Ebadi, A.; Alavi Majd, H. Components of quality of life in hemodialysis patients from family caregivers’ perspective: A qualitative study. BMC Nephrol. 2021, 22, 379. [Google Scholar] [CrossRef] [PubMed]
- Hooker, C. Understanding empathy: Why phenomenology and hermeneutics can help medical education and practice. Med. Health Care Philos. 2015, 18, 541–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giorgi, A. The descriptive phenomenological psychological method. J. Phenomenol. Psychol. 2012, 43, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Salehi, F.; Dehghan, M.; Mangolian Shahrbabaki, P.; Ebadzadeh, M.R. Effectiveness of exercise on fatigue in hemodialysis patients: A randomized controlled trial. BMC Sport. Sci. Med. Rehabil. 2020, 12, 19. [Google Scholar] [CrossRef] [PubMed]
- Alkhaqani, A.L.; Ali DK, A. Improving physical performance through resistance exercise training on patients undergoing hemodialysis: A randomized clinical trial. Ann. Rom. Soc. Cell Biol. 2021, 25, 13639–13653. [Google Scholar]
- Jiménez MD, A.; García, M.N.; Reina, E.S.; Álvarez-Ude, F. Disability in instrumental activities of daily living in hemodialysis patients: Influence on quality of life related to health. Nefrología 2019, 39, 531–538. [Google Scholar] [CrossRef]
- Ghaffari, M.; Morowatisharifabad, M.A.; Mehrabi, Y.; Zare, S.; Askari, J.; Alizadeh, S. What are the hemodialysis patients’ style in coping with stress? A directed content analysis. Int. J. Community Based Nurs. Midwifery 2019, 7, 309. [Google Scholar]
- Sheshadri, A.; Kittiskulnam, P.; Johansen, K.L. Higher Physical Activity Is Associated With Less Fatigue and Insomnia among Patients on Hemodialysis. Kidney Int. Rep. 2019, 4, 285–292. [Google Scholar] [CrossRef] [Green Version]
- Sakkas, G.; Karatzaferi, C. Hemodialysis Fatigue: Just “Simple” Fatigue or a Syndrome on Its Own Right? Front. Physiol. 2012, 3, 306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldeira, S.; Timmins, F. Resilience: Synthesis of concept analyses and contribution to nursing classifications. Int. Nurs. Rev. 2016, 63, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Ng, H.J.; Nandakumar, M.; Griva, K. The management of food cravings and thirst in hemodialysis patients: A qualitative study. J. Health Psychol. 2016, 21, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Han, C.Y.; Pan, I.J. A qualitative approach of psychosocial adaptation process in patients undergoing long-term hemodialysis. Asian Nurs. Res. 2015, 9, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Jonasson, K.; Gustafsson, L.K. You Live as Much as You Have Time To: The Experience of Patients Living with Hemodialysis. Nephrol. Nurs. J. 2017, 44, 35–41. [Google Scholar]
- Chiaranai, C. The lived experience of patients receiving hemodialysis treatment for end-stage renal disease: A qualitative study. J. Nurs. Res. 2016, 24, 101–108. [Google Scholar] [CrossRef]
- Tavassoli, N.; Darvishpour, A.; Mansour-Ghanaei, R.; Atrkarroushan, Z. A correlational study of hope and its relationship with spiritual health on hemodialysis patients. J. Educ. Health Promot. 2019, 8, 146. [Google Scholar]
- Caboral, M.F.; Evangelista, L.S.; Whetsell, M.V. Hope in elderly adults with chronic heart failure. Concept analysis. Investig. Educ. Enferm. 2012, 30, 406–411. [Google Scholar]
- Ahmad, M.M.; Al Nazly, E.K. Hemodialysis: Stressors and coping strategies. Psychol. Health Med. 2015, 20, 477–487. [Google Scholar] [CrossRef]
- Sabouri, F.; Rambod, M.; Khademian, Z. The effect of positive thinking training on hope and adherence to treatment in hemodialysis patients: A randomized controlled trial. BMC Psychol. 2023, 11, 6. [Google Scholar]
| Main Themes | The Desire to Keep Living Despite Challenges | Creating One’s Own Dietary Principles | Moving One’s Body with Remaining Strength | Moving toward Independence |
|---|---|---|---|---|
| Meaning Unit |
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Lee, H.Z. The Lived Self-Care Experiences of Patients Undergoing Long-Term Haemodialysis: A Phenomenological Study. Int. J. Environ. Res. Public Health 2023, 20, 4690. https://doi.org/10.3390/ijerph20064690
Kim S, Lee HZ. The Lived Self-Care Experiences of Patients Undergoing Long-Term Haemodialysis: A Phenomenological Study. International Journal of Environmental Research and Public Health. 2023; 20(6):4690. https://doi.org/10.3390/ijerph20064690
Chicago/Turabian StyleKim, Sisook, and Hyunsook Zin Lee. 2023. "The Lived Self-Care Experiences of Patients Undergoing Long-Term Haemodialysis: A Phenomenological Study" International Journal of Environmental Research and Public Health 20, no. 6: 4690. https://doi.org/10.3390/ijerph20064690