
Participation in the Global Corporate Challenge®, a Four-Month Workplace Pedometer Program, Reduces Psychological Distress

Abstract
:1. Introduction
2. Materials and Methods
2.1. Global Corporate Challenge®
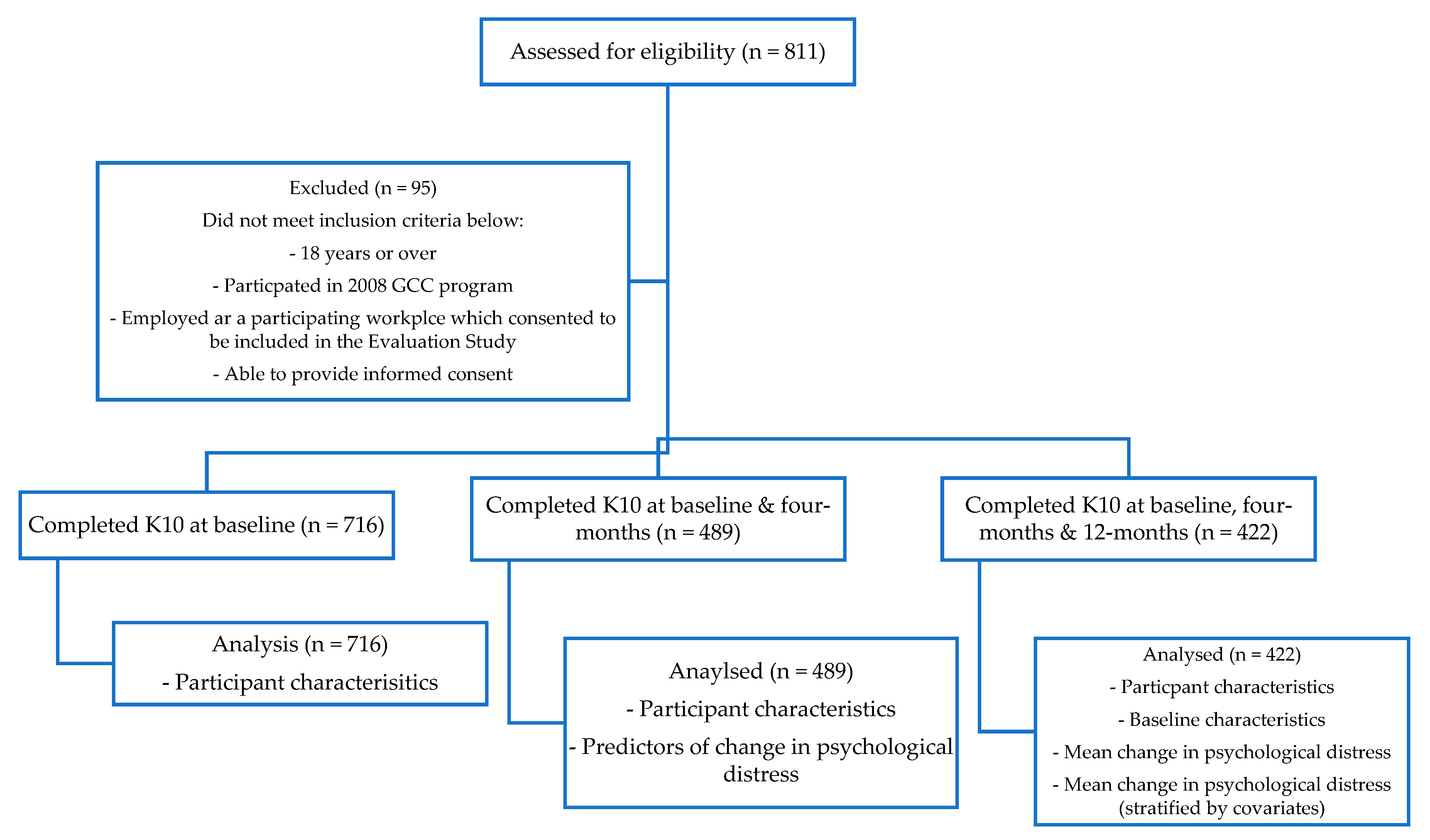
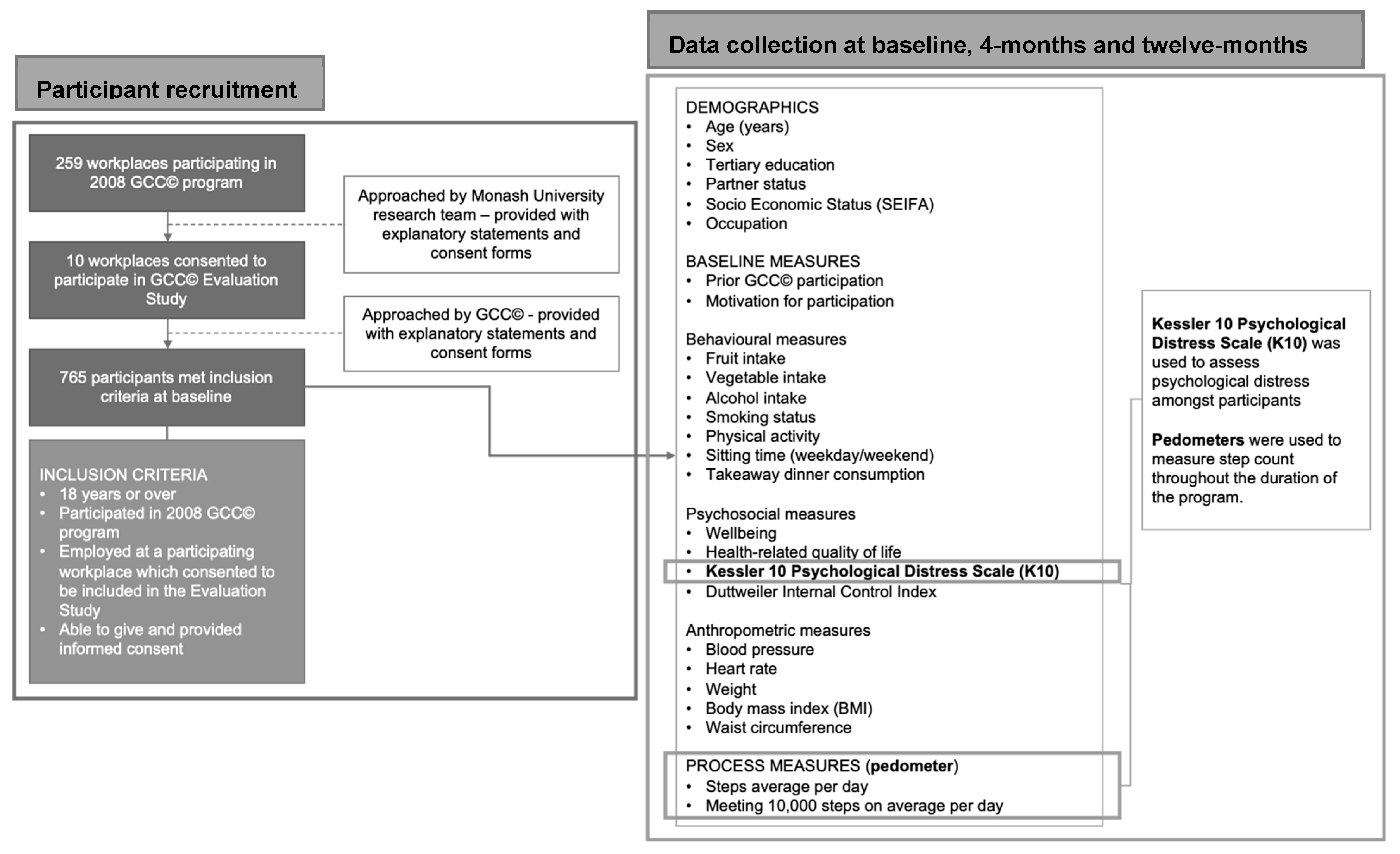
2.2. Recruitment and Participation
2.3. Psychological Distress
2.4. Measures
2.5. Data Analysis
3. Results
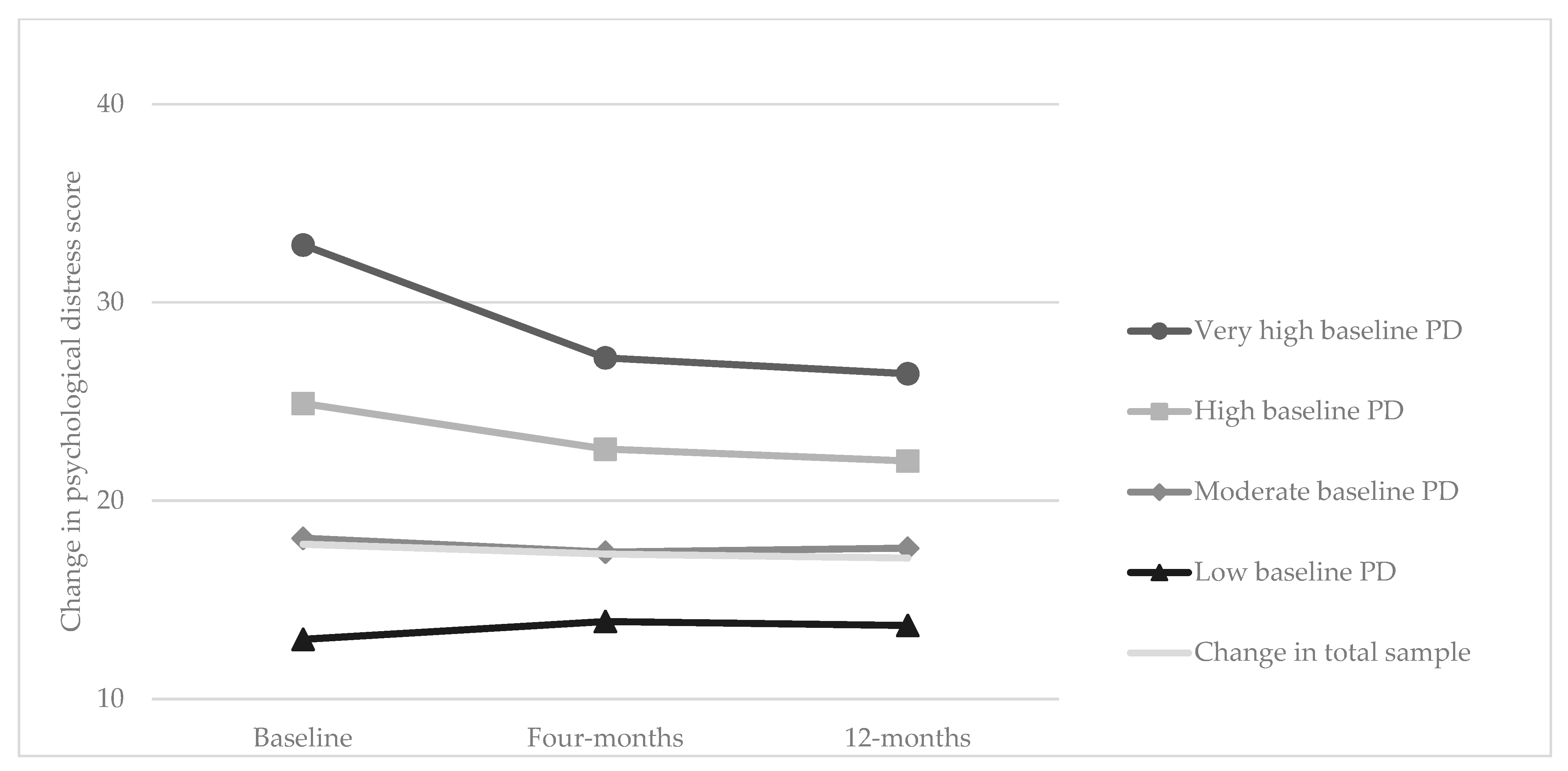
3.1. Immediate and Long-Term Changes in Psychological Distress
3.2. Predictors of a Reduction in Psychological Distress
4. Discussion
4.1. Immediate and Long-Term Changes in Psychological Distress
4.2. Predictors of a Reduction in Psychological Distress
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Psychological Distress | ||||
|---|---|---|---|---|
| N = 422 | Low Mean ± SD or n (%) | Moderate Mean ± SD or n (%) | High Mean ± SD or n (%) | Very High Mean ± SD or n (%) |
| n | 117 | 215 | 71 | 19 |
| DEMOGRAPHICS | ||||
| Age (year) | ||||
| Male | ||||
| Completed teritary education c | ||||
| Partner status | ||||
| Married or de facto | ||||
| Widowed, separated or divorced | ||||
| Never married | ||||
| Socio Economic Status (by SEIFA) d | 1 (<1%) | |||
| Occupation | 8 (6.8%) | 14 (6.5%) | 4 (5.6%) | 2 (10.5%) |
| BASELINE MEASURES | ||||
| Prior GCC® Participation c | ||||
| Motivation for participation | ||||
| Health c | ||||
| To look my best c | ||||
| Fitness c | ||||
| Colleagues c | ||||
| Friends or family c | ||||
| BEHAVIOURAL MEASURES | ||||
| Fruit intake c | ||||
| Vegetable intake c | ||||
| Alcohol c | ||||
| Non smoker c | ||||
| Physical activity c | ||||
| Sitting time | ||||
| Weekday | ||||
| Weekend | ||||
| Takeaway Dinner | ||||
| Once or less per month | ||||
| About once a week | ||||
| More than once a week | ||||
| PSYCHOSOCIAL MEASURES | ||||
| Well-being | ||||
| Well-being c (positive category) | ||||
| Health related quality of life (SF-12) | ||||
| Mental health component | 1 (<1%) | 1 (<1%) | ||
| Physical health component | ||||
| Duttweiler Internal Control Index score | ||||
| ANTHROPOMETRIC MEASURES | ||||
| Systolic blood pressure (mmHg) | ||||
| Diastolic blood pressure (mmHg) | 12 (5.6%) | 5 (7%) | ||
| Heart rate (beats per minute) | 12 (5.6%) | 5 (7%) | ||
| Weight (kg) | 6 (2.8%) | 3 (4.2%) | 1 (5.3%) | |
| Body mass index (kg/m2) | 2 (1.7%) | 6 (2.8%) | 3 (4.2%) | 1 (5.3%) |
| Waist circumference | 2 (1.7%) | 6 (2.8%) | 3 (4.2%) | 1 (5.3%) |
| PROCESS MEASURES | ||||
| STEP DATA | ||||
| Steps average (per day) | 1 (1.4%) | |||
| Meeting 10,000 on average (per day) | 1 (1.4%) | |||
| Meeting 7500 on average (per day) | 63 (153.8%) | 63 (29.3%) | 1 (1.4%) | |
Appendix C. The Kessler 10 Psychological Distress Scale (K10) [40]
- Answer Scale
- Scoring
- The following questions are about your feelings in the past 4 weeks.
- In the past 4 weeks, about how often did you feel tired out for no good reason?
- (In the past 4 weeks,) about how often did you feel nervous?
- (In the past 4 weeks,) about how often did you feel so nervous that nothing could calm you down?
- (In the past 4 weeks,) about how often did you feel hopeless?
- (In the past 4 weeks,) about how often did you feel restless or fidgety?
- (In the past 4 weeks,) about how often did you feel so restless you could not sit still?
- (In the past 4 weeks,) about how often did you feel depressed?
- (In the past 4 weeks,) about how often did you feel that everything was an effort?
- (In the past 4 weeks,) about how often did you feel so sad that nothing could cheer you up?
- (In the past 4 weeks,) about how often did you feel worthless?
Appendix D

Appendix E
| Baseline Only Mean + SD or n (%) | Baseline and 4-Months Mean + SD or n (%) | Baseline, 4-Months and 12-Months Mean + SD or n (%) | p-Value | |
|---|---|---|---|---|
| n | 716 | 489 | 422 | |
| DEMOGRAPHICS | ||||
| Age (year) | 40 ± 10 | 41 ± 10 | 41 ± 10 | <0.001 |
| Male | 284 (39.7%) | 200 (40.9%) | 178 (42.2%) | <0.001 |
| Completed tertiary education a | 572 (79.9%) | 394 (80.6%) | 394 (80.6%) | <0.001 |
| Partner status | ||||
| Married or de facto | 501 (70%) | 351 (71.8%) | 300 (71.1%) | <0.001 |
| Widowed, separated or divorced | 63 (8.8%) | 47 (9.6%) | 42 (10%) | |
| Never married | 152 (21.2%) | 91 (18.6%) | 80 (19%) | |
| Socio Economic Status (by SEIFA) b | ||||
| Most Advantaged | 176 (24.6%) | 119 (24.4%) | 101 (24%) | <0.001 |
| Advantaged | 165 (23.1%) | 126 (25.8%) | 110 (26.1%) | |
| Disadvantaged | 195 (27.3%) | 125 (25.6%) | 108 (25.7%) | |
| Most Disadvantaged | 179 (25%) | 118 (24.2%) | 102 (24.2%) | |
| Occupation | ||||
| Professional | 294 (44%) | 213 (46.8%) | 186 (47.2%) | <0.001 |
| Associate professional | 122 (18.2%) | 90 (19.8%) | 78 (19.8%) | |
| Manager | 147 (22%) | 88 (19.3%) | 76 (19.3%) | |
| Clerical or Service | 106 (15.8%) | 64 (14.1%) | 54 (13.7%) | |
| BASELINE MEASURES | ||||
| Prior GCC® Participation a | 157 (21.9%) | 106 (21.7%) | 97 (23%) | <0.001 |
| Motivation for participation | ||||
| Health a | 484 (67.7%) | 337 (68.9%) | 289 (68.5%) | <0.001 |
| To look my best a | 418 (58.5%) | 289 (59.1%) | 259 (61.4%) | <0.001 |
| Fitness a | 475 (66.4%) | 324 (66.3%) | 284 (67.3%) | <0.001 |
| Colleagues a | 700 (97.8%) | 478 (97.8%) | 413 (97.9%) | <0.001 |
| Friends or family a | 95 (13.3%) | 66 (13.5%) | 50 (11.9%) | <0.001 |
| BEHAVIOURAL MEASURES | ||||
| Fruit intake (meeting guidelines) a | 216 (30.2%) | 181 (37%) | 155 (37.6%) | <0.001 |
| Vegetable intake (meeting guidelines) a | 103 (14.4%) | 90 (18.4%) | 82 (19.4%) | <0.001 |
| Alcohol (meeting guidelines)a | 311 (43.4%) | 209 (42.7%) | 215 (51%) | <0.001 |
| Non smoker a | 642 (89.7%) | 452 (92.4%) | 401 (95%) | <0.001 |
| Physical activity (meeting guidelines) a | 274 (38.3%) | 230 (47%) | 193 (45.7%) | <0.001 |
| Sitting time (hours per day) | ||||
| Weekday | 8.1 ± 3.6 | 7.6 ± 3.6 | 7.4 ± 3.7 | <0.001 |
| Weekend | (715) 5.3 ± 3.0 | 4.8 ± 3.0 | 4.9 ± 2.8 | <0.001 |
| Takeaway Dinner | ||||
| Once or less per month | 321 (44.8%) | 236 (48.3%) | 210 (49.8%) | <0.001 |
| About once a week | 298 (41.6%) | 209 (42.7%) | 177 (41.9%) | |
| More than once a week | 97 (13.6%) | 44 (9%) | 35 (8.3%) | |
| PSYCHOSOCIAL MEASURES | ||||
| Well-being | 60 ± 19.1 | 63.5 ± 18.8 | 63.6 ± 18.7 | <0.001 |
| Well-being (positive category) a | 521 (72.77%) | 395 (80.78%) | 327 (77.5%) | <0.001 |
| Health related quality of life (SF-12) | ||||
| Mental health component | (713) 49.4 ± 10 | 50.5 ± 9.1 | (421) 43.1 ± 5.3 | <0.001 |
| Physical health component | (713) 50.5 ± 7.3 | 50.5 ± 7.8 | (421) 48.5 ± 4.9 | <0.001 |
| K10 Scores | ||||
| Low | 209 (29.2%) | 224 (45.8%) | 205 (48.6%) | <0.001 |
| Moderate | 347 (48.5%) | 173 (35.4%) | 143 (33.9%) | |
| High | 129 (18%) | 61 (12.5%) | 49 (11.6%) | |
| Very high | 31 (4.3%) | 31 (6.3%) | 25 (5.9%) | |
| Duttweiler Internal Control Index score | 106 ± 11.1 | 105 ± 11.9 | 105 ± 12.4 | <0.001 |
| ANTHROPOMETRIC MEASURES | ||||
| Systolic blood pressure (mmHg) | (646) 118.6 ± 15 | (457) 116.9 ± 13.7 | (386) 115.6 ± 13.2 | <0.001 |
| Diastolic blood pressure (mmHg) | (646) 79.7 ± 10.4 | (457) 78 ± 9.8 | (386) 78.2 ± 9.9 | <0.001 |
| Heart rate (beats per minute) | (646) 68.6 ± 10 | (457) 68.8 ± 10.8 | (377) 68.3 ± 10.8 | <0.001 |
| Weight (kg) | (657) 76.8 ± 16.2 | (458) 76.8 ± 15.5 | (387) 77.6 ± 15.8 | <0.001 |
| Body mass index (kg/m2) | (657) 26.7 ± 4.8 | (446) 26.6 ± 4.6 | (387) 26.9 ± 4.8 | <0.001 |
| Waist circumference | (656) 87.8 ± 12.6 | (458) 86.1 ± 12.1 | (387) 88 ± 12.6 | <0.001 |
| PROCESS MEASURES | ||||
| STEP DATA | ||||
| Steps average (per day) | (706) 11,481.1 ± 3720.8 | (488) 11,691.5 ± 3700.1 | (421) 11,778.2 ± 3755.7 | <0.001 |
| Meeting 10,000 on average (per day) a | ||||
| Yes | 450 (63.7%) | 329 (67.4%) | 289 (68.7%) | <0.001 |
| No | 256 (36.3%) | 159 (32.6%) | 132 (31.4%) | |
Appendix F
| Baseline to 4-Months | Baseline to 12-Months | |||||||
|---|---|---|---|---|---|---|---|---|
| n | Baseline | 4-Months | 12-Months | Mean Change B (95% CI) | p-Value | Mean Change B (95% CI) | p-Value | |
| Change in K10 score in total sample | 422 | 17.8 ± 5.6 | 17.3 ± 5.6 | 17.1 ± 5.8 | −0.5 (−0.9, −0.04) | 0.035 | −0.7 (−1.1, −0.3) | 0.005 |
| Low baseline K10 score | 180 | 13.0 ± 1.5 | 13.9 ± 3.4 | 13.7 ± 3.2 | 0.9 (0.3, 1.0) | 0.007 | 0.6 (0.2, 1.0) | 0.015 |
| Moderate baseline K10 score | 152 | 18.1 ± 1.7 | 17.4 ± 4.1 | 17.6 ± 4.4 | −0.7 (−1.4, 0.01) | 0.052 | −0.5 (−1.1, 0.1) | 0.097 |
| High baseline K10 score | 71 | 24.9 ± 2.2 | 22.6 ± 5.3 | 22.0 ± 6.3 | −2.3 (−4.8, 0.3) | 0.074 | −2.9 (−4.5, −1.2) | 0.003 |
| Very high baseline K10 score | 19 | 32.9 ± 3.3 | 27.2 ± 6.9 | 26.4 ± 7.1 | −5.7 (−9.5, −1.0) | 0.01 | −6.5 (−12.8, −0.4) | 0.041 |
Appendix G
| Baseline to 4-Months | Baseline to 12-Months | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Baseline | 4-Months | 12-Months | Mean Change | (95% CI) Min | (95% CI) Max | p-Value | Mean Change | (95% CI) Min | (95% CI) Max | p-Value | ||
| Total sample | 422 | 17.8 ± 5.6 | 17.3 ± 5.6 | 17.1 ± 5.8 | −0.5 | −0.9 | −0.04 | 0.035 | −0.7 | −1.1 | −0.3 | 0.005 | |
| DEMOGRAPHICS | |||||||||||||
| Age | 20–30 | 65 | 20 ± 5.1 | 20.1 ± 6.7 | 19.7 ± 6.8 | 0.5 | −1.2 | 2.3 | 0.508 | 0.2 | −1.9 | 2.3 | 0.83 |
| 30–40 | 130 | 19.4 ± 5.3 | 17.8 ± 5.6 | 17 ± 5.1 | −0.9 | −1.8 | −0.1 | 0.039 | −1.8 | −2.9 | −0.6 | 0.008 | |
| 40–50 | 135 | 18 ± 4 | 16.2 ± 5.1 | 16.6 ± 6.1 | −0.6 | −1.1 | −0.1 | 0.022 | −0.2 | −0.8 | 0.5 | 0.541 | |
| 50–60 | 80 | 17.9 ± 4.6 | 16.4 ± 4.7 | 16.1 ± 4.4 | −0.3 | −1.0 | 0.4 | 0.421 | −0.6 | −1.1 | −0.1 | 0.017 | |
| 60–70 | 12 | 17.3 ± 3.2 | 14.7 ± 3.8 | 16.3 ± 6.6 | −1.4 | −2.7 | −0.1 | 0.037 | 0.2 | −1.3 | 1.7 | 0.774 | |
| Sex | Females | 244 | 18.9 ± 5.1 | 17.5 ± 5.8 | 17.4 ± 5.6 | −0.6 | −1.0 | −0.3 | 0.003 | −0.8 | −1.5 | −0.1 | 0.026 |
| Males | 178 | 18.4 ± 4.3 | 16.9 ± 5.4 | 16.7 ± 5.9 | −0.3 | −1.4 | 0.8 | 0.559 | −0.5 | −1.3 | 0.3 | 0.214 | |
| Tertiary education | Completed tertiary education | 340 | 18.7 ± 4.9 | 17.2 ± 5.6 | 17.2 ± 5.8 | −0.6 | −1.0 | −0.2 | 0.005 | −0.6 | −1.1 | −0.2 | 0.008 |
| Did not complete tertiary education | 82 | 17.6 ± 5 | 17.5 ± 5.5 | 16.8 ± 5.4 | −0.05 | −1.9 | 1.8 | 0.952 | −0.8 | −2.2 | 0.5 | 0.206 | |
| Partner status | Married or de facto | 300 | 18.2 ± 4.3 | 16.8 ± 5.3 | 16.9 ± 5.8 | −0.5 | −0.8 | −0.1 | 0.025 | −0.3 | −0.8 | 0.1 | 0.125 |
| Widowed, separated or divorced | 42 | 20.9 ± 5.7 | 17.7 ± 5.2 | 17.3 ± 5 | −2.0 | −4.2 | 0.1 | 0.057 | −2.5 | −4.3 | −0.7 | 0.012 | |
| Never married | 80 | 19.5 ± 5.5 | 18.9 ± 6.7 | 17.7 ± 5.9 | 0.2 | −1.0 | 1.3 | 0.771 | −1.0 | −1.6 | −0.4 | 0.005 | |
| Socio Economic Status (by SEIFA) | Most Advantaged | 101 | 18.6 ± 4.9 | 17 ± 5.8 | 16.9 ± 5.4 | −0.7 | −2.4 | 1.0 | 0.358 | −0.9 | −1.6 | −0.2 | 0.017 |
| Advantaged | 110 | 18.3 ± 4.5 | 16.1 ± 4.7 | 16.1 ± 4.7 | −0.9 | −1.5 | −0.3 | 0.007 | −0.9 | −2.2 | 0.4 | 0.149 | |
| Disadvantaged | 108 | 19.1 ± 5.3 | 18.2 ± 5.8 | 17.8 ± 6.4 | −0.1 | −0.9 | 0.7 | 0.776 | −0.5 | −1.0 | −0.04 | 0.038 | |
| Most Disadvantaged | 102 | 18.9 ± 4.3 | 17.8 ± 5.9 | 17.6 ± 6.4 | −0.2 | −1.0 | 0.6 | 0.564 | −0.4 | −1.4 | 0.5 | 0.346 | |
| Occupation | Professional | 186 | 18.8 ± 4.9 | 17.4 ± 6.1 | 17.2 ± 5.9 | −0.3 | −1.1 | 0.5 | 0.384 | −0.5 | −1.1 | 0.1 | 0.090 |
| Associate professional | 78 | 18.7 ± 4.6 | 16.7 ± 4.7 | 16.7 ± 5.5 | −1.2 | −1.7 | −0.6 | 0.002 | −1.2 | −2.2 | −0.2 | 0.023 | |
| Manager | 76 | 18.6 ± 4.5 | 17 ± 4.5 | 17.2 ± 5.8 | −0.9 | −1.7 | −0.1 | 0.029 | −0.7 | −1.7 | 0.4 | 0.178 | |
| Clerical or Service | 54 | 18.4 ± 4.2 | 18.1 ± 5.9 | 17 ± 5.5 | 0.5 | −0.8 | 1.8 | 0.387 | −0.6 | −2.3 | 1.0 | 0.403 | |
| BASELINE MEASURES | |||||||||||||
| Motivation for participation | Health (yes) | 289 | 19 ± 4.9 | 17.6 ± 5.8 | 17.1 ± 5.6 | −0.6 | −1.1 | −0.03 | 0.040 | −1.1 | −1.5 | −0.6 | <0.001 |
| To look my best (yes) | 259 | 18.9 ± 4.9 | 17.6 ± 5.9 | 17.5 ± 5.8 | −0.5 | −1.0 | −0.1 | 0.026 | −0.7 | −1.2 | −0.1 | 0.024 | |
| Fitness (yes) | 284 | 18.9 ± 4.8 | 17.3 ± 5.8 | 17.3 ± 5.8 | −0.7 | −1.3 | −0.2 | 0.016 | −0.9 | −1.5 | −0.3 | 0.009 | |
| Colleagues (yes) | 413 | 18.6 ± 4.7 | 17.3 ± 5.6 | 17 ± 5.8 | −0.5 | −0.9 | −0.04 | 0.034 | −0.7 | −1.1 | −0.3 | 0.005 | |
| Friends or family (yes) | 50 | 19.8 ± 5.6 | 18.3 ± 6.8 | 18.7 ± 7.4 | −0.6 | −2.0 | 0.8 | 0.386 | −0.2 | −1.2 | 0.8 | 0.630 | |
| PSYCHOSOCIAL MEASURES | |||||||||||||
| Duttweiler | 422 | 18.7 ± 4.8 | 17.3 ± 5.6 | 17.1 ± 5.8 | 0.2 | −4.8 | 5.1 | 0.933 | −4.8 | −9.8 | 0.2 | 0.059 | |
| PROCESS MEASURES | |||||||||||||
| Steps average per day (per 10,000 steps) | 422 | 17.8 ± 5.6 | 17.3 ± 5.6 | 17.1 ± 5.8 | 0.3 | −0.8 | 1.3 | 0.565 | −0.4 | −2.1 | 1.2 | 0.574 | |
| Program compliance | |||||||||||||
| Yes | 289 | 17.5 ± 5.4 | 16.8 ± 5.2 | 16.6 ± 5.4 | −0.7 | −1.3 | −0.02 | b | −0.9 | −1.4 | −0.3 | 0.009 | |
| No | 132 | 18.4 ± 6 | 18.3 ± 6.4 | 18.1 ± 6.4 | −0.1 | −0.9 | 0.7 | 0.83 | −0.2 | −0.9 | 0.5 | 0.466 | |
Appendix H

References
- Kessler, R.C.; Demler, O.; Frank, R.G.; Olfson, M.; Pincus, H.A.; Walters, E.E.; Wang, P.; Wells, K.B.; Zaslavsky, A.M. Prevalence and Treatment of Mental Disorders, 1990 to 2003. N. Engl. J. Med. 2005, 352, 2515–2523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenzie, S.H.; Harris, M. Understanding the relationship between stress, distress and healthy lifestyle behaviour: A qualitative study of patients and general practitioners. BMC Fam. Pract. 2013, 14, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viertiö, S.; Kiviruusu, O.; Piirtola, M.; Kaprio, J.; Korhonen, T.; Marttunen, M.; Suvisaari, J. Factors contributing to psychological distress in the working population, with a special reference to gender difference. BMC Public Health 2021, 21, 611. [Google Scholar] [CrossRef]
- McLachlan, K.J.J.; Gale, C. The effects of psychological distress and its interaction with socioeconomic position on risk of developing four chronic diseases. J. Psychosom. Res. 2018, 109, 79–85. [Google Scholar] [CrossRef]
- Vigo, D.; Thornicroft, G.; Atun, R. Estimating the true global burden of mental illness. Lancet Psychiatry 2016, 3, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Enticott, J.C.; Lin, E.; Shawyer, F.; Russell, G.; Inder, B.; Patten, S.; Meadows, G. Prevalence of psychological distress: How do Australia and Canada compare? Aust. N. Z. J. Psychiatry 2018, 52, 227–238. [Google Scholar] [CrossRef]
- Drapeau, A.; Marchand, A.; Beaulieu-Prévost, D. Epidemiology of Psychological Distress. In Mental Illnesses: Understanding, Prediction and Control; InTech Open: London, UK, 2012. [Google Scholar]
- Mental Health. Available online: https://www.safeworkaustralia.gov.au/topic/mental-health (accessed on 12 May 2021).
- Available online: https://osha.europa.eu/en/themes/psychosocial-risks-and-stress (accessed on 12 May 2021).
- He, Y.; Yatsuya, H.; Chiang, C.; Ota, A.; Okubo, R.; Ishimaru, T.; Tabuchi, T. 1503 The association of work-related stress with aggravation of pre-existing disease during COVID-19 emergency in Japan. Int. J. Epidemiol. 2021, 50 (Suppl. S1), dyab168.273. [Google Scholar] [CrossRef]
- Sørensen, J.K.; Framke, E.; Pedersen, J.; Alexanderson, K.; Bonde, J.P.; Farrants, K.; Flachs, E.M.; Magnusson Hanson, L.L.; Nyborg, S.T.; Kivimäki, M.; et al. 1175 Work stress and loss of years lived without chronic disease; an 18-year prospective cohort study. Int. J. Epidemiol. 2021, 50, dyab168.624. [Google Scholar] [CrossRef]
- Harding, J.; Freak-Poli, R.L.; Backholer, K.; Peeters, A. Change in Health-Related Quality of Life Amongst Participants in a 4-Month Pedometer-Based Workplace Health Program. J. Phys. Act. Health 2013, 10, 533–543. [Google Scholar] [CrossRef]
- Brown, W.J.; Bauman, A.E.; Bull, F.; Burton, N.W. Development of Evidence-Based Physical Activity Recommendations for Adults (18–64 Years); Australian Government Department of Health: Woden Town Centre, Austraila, 2012.
- Freak-Poli, R.L.; Wolfe, R.; Wong, E.; Peeters, A. Change in well-being amongst participants in a four-month pedometer-based workplace health program. BMC Public Health 2014, 14, 953. [Google Scholar] [CrossRef] [Green Version]
- Warburton, D.; Nicol, C.W.; Bredin, S. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Physical Acitvity. World Health Organisation. 23 February 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 27 October 2020).
- Mikkelsen, K.; Stojanovska, L.; Polenakovic, M.; Bosevski, M.; Apostolopoulos, V. Exercise and mental health. Maturitas 2017, 106, 48–56. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services. Physical Activity Guidelines Advisory Committee Report Part G. Section 8: Mental Health; US Department of Health and Human Services: Washington, DC, USA, 2008.
- Teychenne, M.; Costigan, S.A.; Parker, K. The association between sedentary behaviour and risk of anxiety: A systematic review. BMC Public Health 2015, 15, 513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perales, F.; Pozo-Cruz, J.D.; Pozo-Cruz, B.D. Impact of physical activity on psychological distress: A prospective analysis of an Australian national sample. Am. J. Public Health 2014, 104, e91. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics (ABS). 4364.0.55.001—National Health Survey: First Results, 2017–2018 in Physical activity; Australian Bureau of Statistics: Canberra, Australia, 2018.
- WHO. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010.
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- WHO. Preventing Noncommunicable Diseases in the Workplace through Diet and Physical Activity: WHO/World Economic Forum Report of a Joint Event; World Health Organization/World Economic Forum: Geneva, Switzerland, 2008; pp. 1–52.
- Eurostat. Sit at Work? You Are One of 39%; Eurostat: Luxembourg, 2019. [Google Scholar]
- Gilson, N.D.; Suppini, A.; Ryde, G.C.; Brown, H.E.; Brown, W.J. Does the use of standing ‘hot’ desks change sedentary work time in an open plan office? Prev. Med. 2012, 54, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, M.; Sanderson, K.; Blizzard, L.; Teale, B.; Venn, A. Cross-sectional associations between sitting at work and psychological distress: Reducing sitting time may benefit mental health. Ment. Health Phys. Act. 2013, 6, 103–109. [Google Scholar] [CrossRef]
- Parry, S.; Straker, L.; Gilson, N.D.; Smith, A.J. Participatory workplace interventions can reduce sedentary time for office workers—A randomised controlled trial. PloS ONE 2013, 8, e78957. [Google Scholar] [CrossRef]
- Tew, G.A.; Posso, M.C.; Arundel, C.E.; McDaid, C.M. Systematic review: Height-adjustable workstations to reduce sedentary behaviour in office-based workers. Occup. Med. 2015, 65, 357–366. [Google Scholar] [CrossRef] [Green Version]
- Torbeyns, T.; Bailey, S.; Bos, I.; Meeusen, R. Active Workstations to Fight Sedentary Behaviour. Sport. Med. 2014, 44, 1261–1273. [Google Scholar] [CrossRef]
- Kohl, H.W.; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croteau, K.A. Using Pedometers to Increase the Non-Workday Steps of Hospital Nursing and Support Staff: A Pilot Study. Workplace Health Saf. 2017, 65, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Freak-Poli, R.L.; Cumpston, M.; Albarqouni, L.; Clemes, S.A.; Peeters, A. Workplace pedometer interventions for increasing physical activity. Cochrane Database Syst. Rev. 2020, 7, CD009209. [Google Scholar] [PubMed]
- Blake, H.; Batt, M.E. Employee perceptions of a pedometer walking intervention in a hospital workplace. Int. J. Health Promot. Educ. 2015, 53, 257–270. [Google Scholar] [CrossRef]
- Caperchione, C.M.; Vandelanotte, C.; Corry, K.; Power, D.; Gill, N.; Duncan, M.J. Qualitative Exploration of the Feasibility and Acceptability of Workplace-Based Microgrants to Improve Physical Activity: The 10,000 Steps Pedometer Microgrant Scheme. J. Occup. Environ. Med. 2018, 60, e406–e411. [Google Scholar] [CrossRef]
- Macniven, R.; Engelen, L.; Kacen, M.J.; Bauman, A. Does a corporate worksite physical activity program reach those who are inactive? Findings from an evaluation of the Global Corporate Challenge. Health Promot. J. Aust. 2015, 26, 142–145. [Google Scholar] [CrossRef]
- Freak-Poli, R.; Wolfe, R.; Backholer, K.; De Courten, M.; Peeters, A. Impact of a pedometer-based workplace health program on cardiovascular and diabetes risk profile. Prev. Med. 2011, 53, 162–171. [Google Scholar] [CrossRef]
- Freak-Poli, R.; Wolfe, R.; Brand, M.; de Courten, M.; Peeters, A. Eight-month postprogram completion: Change in risk factors for chronic disease amongst participants in a 4-month pedometer-based workplace health program. Obesity 2013, 21, E360–E368. [Google Scholar] [CrossRef]
- Freak-Poli, R.L.; Wolfe, R.; Walls, H.; Backholer, K.; Peeters, A. Participant characteristics associated with greater reductions in waist circumference during a four-month, pedometer-based, workplace health program. BMC Public Health 2011, 11, 824. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics (ABS). 4364.0.55.001—National Health Survey: First Results, 2017–2018, in Psychological Distress; Australian Bureau of Statistics: Canberra, Australia, 2018.
- Coombs, T. Australian Mental Health Outcomes and Classification Network. Kessler-10 Training Manual; NSW Insititute of Psychiatry: Sydney, Australia, 2005.
- Slade, T.; Grove, R.; Burgess, P. Kessler Psychological Distress Scale: Normative Data from the 2007 Australian National Survey of Mental Health and Wellbeing. Aust. N. Z. J. Psychiatry 2011, 45, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Hides, L.; Lubman, D.I.; Devlin, H.; Cotton, S.; Aitken, C.; Gibbie, T.; Hellard, M. Reliability and validity of the Kessler 10 and Patient Health Questionnaire among injecting drug users. Aust. N. Z. J. Psychiatry 2007, 41, 166–168. [Google Scholar] [CrossRef] [PubMed]
- Spies, G.; Kader, K.; Kidd, M.; Smit, J.; Myer, L.; Stein, D.J.; Seedat, S. Validity of the K-10 in detecting DSM-IV-defined depression and anxiety disorders among HIV-infected individuals. AIDS Care 2009, 21, 1163–1168. [Google Scholar] [CrossRef]
- Donker, T.; Comijs, H.; Cuijpers, P.; Terluin, B.; Nolen, W.; Zitman, F.; Penninx, B. The validity of the Dutch K10 and extended K10 screening scales for depressive and anxiety disorders. Psychiatry Res. 2009, 176, 45–50. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Baillie, A.J. Predictive gender and education bias in Kessler’s psychological distress Scale (K10). Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 743–748. [Google Scholar] [CrossRef]
- Spies, G.; Stein, D.J.; Roos, A.; Faure, S.C.; Mostert, J.; Seedat, S.; Vythilingum, B. Validity of the Kessler 10 (K-10) in detecting DSM-IV defined mood and anxiety disorders among pregnant women. Arch. Women’s Ment. Health 2009, 12, 69–74. [Google Scholar] [CrossRef]
- Arnaud, B.; Malet, L.; Teissedre, F.; Izaute, M.; Moustafa, F.; Geneste, J.; Schmidt, J.; Llorca, P.M.; Brousse, G. Validity study of Kessler’s Psychological Distress Scales conducted among patients admitted to French emergency departments for alcohol consumption-related disorders. Alcohol Clin. Exp. Res. 2010, 34, 1235–1245. [Google Scholar] [CrossRef]
- Wittchen, H.-U. Screening for serious mental illness: Methodological studies of the K6 screening scale. Int. J. Methods Psychiatr. Res. 2010, 19 (Suppl. S1), 1–3. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Bassett, D.R., Jr. How many steps/day are enough? Preliminary pedometer indices for public health. Sports Med. 2004, 34, 1–8. [Google Scholar] [CrossRef]
- Clayton, D.; Hill, M. Statistical Models in Epidemiology; Oxford University Press: New York, NY, USA, 1993; p. 273. [Google Scholar]
- WHO. The WHO STEPwise Approach. Surveillence of Risk Factors for Noncommunicable Diseases: Step 1, 2 & 3; World Health Organization (WHO): Geneva, Switzerland, 2002.
- WHO. The WHO Mini-STEP Questionnaire; World Health Organization: Geneva, Switzerland, 2002.
- Duttweiler, P.C. The Internal Control Index: A Newly Developed Measure of Locus of Control. Educ. Psychol. Meas. 1984, 44, 209–221. [Google Scholar] [CrossRef]
- Hallam, K.T.; Bilsborough, S.; de Courten, M. “Happy feet”: Evaluating the benefits of a 100-day 10,000 step challenge on mental health and wellbeing. BMC Psychiatry 2018, 18, 19. [Google Scholar] [CrossRef] [Green Version]
- del Pozo Cruz, B.; Gallardo-Gomez, D.; del Pozo-Cruz, J.; Ding, D. How many steps a day to reduce the risk of all-cause mortality? A dose–response meta-analysis. J. Intern. Med. 2022, 291, 519–521. [Google Scholar] [CrossRef] [PubMed]
- White, R.L.; Bennie, J.; Abbott, G.; Teychenne, M. Work-related physical activity and psychological distress among women in different occupations: A cross-sectional study. BMC Public Health 2020, 20, 1007. [Google Scholar] [CrossRef] [PubMed]
- Lally, P.; Van Jaarsveld, C.H.; Potts, H.W.; Wardle, J. How are habits formed: Modelling habit formation in the real world. Eur. J. Soc. Psychol 2010, 40, 998–1009. [Google Scholar] [CrossRef] [Green Version]
- Abdin, S.; Welch, R.K.; Byron-Daniel, J.; Meyrick, J. The effectiveness of physical activity interventions in improving well-being across office-based workplace settings: A systematic review. Public Health 2018, 160, 70–76. [Google Scholar] [CrossRef]
- Jindo, T.; Kai, Y.; Kitano, N.; Tsunoda, K.; Nagamatsu, T.; Arao, T. Relationship of workplace exercise with work engagement and psychological distress in employees: A cross-sectional study from the MYLS study. Prev. Med. Rep. 2020, 17, 101030. [Google Scholar] [CrossRef]
- Linden, A. Estimating the effect of regression to the mean in health management programs. Dis. Manag. Health Outcomes 2007, 15, 7–12. [Google Scholar] [CrossRef]
- Gucciardi, D.F.; Law, K.H.; Guerrero, M.D.; Quested, E.; Thøgersen-Ntoumani, C.; Ntoumanis, N.; Jackson, B. Longitudinal relations between psychological distress and moderate-to-vigorous physical activity: A latent change score approach. Psychol. Sport Exerc. 2020, 47, 101490. [Google Scholar] [CrossRef]
- Thøgersen-Ntoumani, C.; Loughren, E.A.; Taylor, I.M.; Duda, J.L.; Fox, K.R. A step in the right direction? Change in mental well-being and self-reported work performance among physically inactive university employees during a walking intervention. Ment. Health Phys. Act. 2014, 7, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Groeneveld, I.F.; Proper, K.I.; van der Beek, A.J.; Hildebrandt, V.H.; van Mechelen, W. Factors associated with non-participation and drop-out in a lifestyle intervention for workers with an elevated risk of cardiovascular disease. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stults-Kolehmainen, M.A.; Sinha, R. The Effects of Stress on Physical Activity and Exercise. Sport. Med. 2013, 44, 81–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson-Kozlow, M.F.; Sallis, J.F.; Calfas, K.J. Does life stress moderate the effects of a physical activity intervention? Psychol. Health 2004, 19, 479–489. [Google Scholar] [CrossRef]
- Lutz, R.S.; Stults-Kolehmainen, M.A.; Bartholomew, J.B. Exercise caution when stressed: Stages of change and the stress–exercise participation relationship. Psychol. Sport Exerc. 2010, 11, 560–567. [Google Scholar] [CrossRef]
- Brown, W.J.; Heesch, K.C.; Miller, Y.D. Life Events and Changing Physical Activity Patterns in Women at Different Life Stages. Ann. Behav. Med. 2009, 37, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Jorm, A.F.; Windsor, T.D.; Dear, K.B.; Anstey, K.J.; Christensen, H.; Rodgers, B. Age group differences in psychological distress: The role of psychosocial risk factors that vary with age. Psychol. Med. 2005, 35, 1253–1263. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Kondo, N. Organizational justice, psychological distress, and stress-related behaviors by occupational class in female Japanese employees. PLoS ONE 2019, 14, e0214393. [Google Scholar] [CrossRef]
- Bierman, A. Functional Limitations and Psychological Distress: Marital Status as Moderator. Soc. Ment. Health 2012, 2, 35–52. [Google Scholar] [CrossRef] [Green Version]
- Wagner, A.L.; Keusch, F.; Yan, T.; Clarke, P.J. The impact of weather on summer and winter exercise behaviors. J. Sport Health Sci. 2019, 8, 39–45. [Google Scholar] [CrossRef]
- Johnsen, M.T.; Wynn, R.; Bratlid, T. Is there a negative impact of winter on mental distress and sleeping problems in the subarctic: The Tromsø Study. BMC Psychiatry 2012, 12, 225. [Google Scholar] [CrossRef] [Green Version]
- Tudor-Locke, C.; Williams, J.E.; Reis, J.P.; Pluto, D. Utility of pedometers for assessing physical activity: Convergent validity. Sports Med. 2002, 32, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Shimura, A.; Masuya, J.; Yokoi, K.; Morishita, C.; Kikkawa, M.; Nakajima, K.; Chen, C.; Nakagawa, S.; Inoue, T. Too much is too little: Estimating the optimal physical activity level for a healthy mental state. Front. Psychol. 2023, 13, 1044988. [Google Scholar] [CrossRef] [PubMed]
- Sandoval-Reyes, J.; Restrepo-Castro, J.C.; Duque-Oliva, J. Work Intensification and Psychological Detachment: The Mediating Role of Job Resources in Health Service Workers. Int. J. Environ. Res. Public Health. 2021, 18, 12228. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A. End ‘Fat-Shaming’ Employee Wellness Programs. HuffPost, 11 December 2015. Available online: https://www.huffpost.com/entry/end-fat-shaming-employee-wellness-programs_b_8738540(accessed on 12 February 2023).
- Australian Institute of Health and Welfare. Insufficient Physical Activity; AIHW: Canberra, Australia, 2020.
- Heath, A. Skills, Technology and the Future of Work; Reserve Bank of Australia: Sydney, Australia, 2020.
- Barankay, I. Why Employee Wellness Programs Don’t Work. Knowledge at Wharton Podcast. 7 March 2022. Available online: https://knowledge.wharton.upenn.edu/podcast/knowledge-at-wharton-podcast/why-employee-wellness-programs-dont-work/ (accessed on 12 February 2023).
- Platts, K.; Breckon, J.; Marshall, E. Enforced home-working under lockdown and its impact on employee wellbeing: A cross-sectional study. BMC Public Health 2022, 22, 199. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.E.; Dennerlein, J.T.; Wagner, G.R.; Sorensen, G. Work and worker health in the post-pandemic world: A public health perspective. Lancet Public Health 2022, 7, e188–e194. [Google Scholar] [CrossRef]


| Psychological Distress | |||||
|---|---|---|---|---|---|
| N = 422 | Low Mean ± SD or n (%) | Moderate Mean ± SD or n (%) | High Mean ± SD or n (%) | Very High Mean ± SD or n (%) | p-Value b |
| n | 117 | 215 | 71 | 19 | |
| DEMOGRAPHICS | |||||
| Age (year) | 42.6 ± 10 | 41.7 ± 10 | 39.4 ± 10.7 | 37.8 ± 8.8 | <0.001 |
| Male | 46 (39.3%) | 96 (44.7%) | 29 (40.9%) | 7 (36.8%) | 0.366 |
| Completed tertiary education c | 97 (82.9%) | 169 (78.6%) | 56 (78.9%) | 18 (94.7%) | 0.778 |
| Partner status | |||||
| Married or de facto | 86 (73.5%) | 162 (75.4%) | 41 (57.8%) | 11 (57.9%) | 0.164 |
| Widowed, separated or divorced | 9 (7.7%) | 18 (8.4%) | 11 (15.5%) | 4 (21.1%) | |
| Never married | 22 (18.8%) | 35 (16.3%) | 19 (26.8%) | 4 (21.1%) | |
| Socio Economic Status by residential postcode (SEIFA) d | |||||
| Most Advantaged | 32 (27.4%) | 49 (22.9%) | 15 (21.1%) | 5 (26.3%) | 0.363 |
| Advantaged | 28 (23.9%) | 63 (29.4%) | 16 (22.5%) | 3 (15.8%) | |
| Disadvantaged | 32 (27.4%) | 49 (22.9%) | 18 (25.4%) | 9 (47.4%) | |
| Most Disadvantaged | 25 (21.4%) | 53 (24.8%) | 22 (31%) | 2 (10.5%) | |
| Occupation | |||||
| Professional | 49 (45%) | 97 (48.3%) | 29 (43.3%) | 11 (64.7%) | 0.768 |
| Associate professional | 24 (22%) | 36 (17.9%) | 16 (23.9%) | 2 (11.8%) | |
| Manager | 19 (17.4%) | 42 (20.9%) | 13 (19.4%) | 2 (11.8%) | |
| Clerical or Service | 17 (15.6%) | 26 (12.9%) | 9 (13.4%) | 2 (11.8%) | |
| BASELINE MEASURES | |||||
| Prior GCC® Participation c | 32 (27.4%) | 49 (22.8%) | 13 (18.3%) | 3 (15.8%) | 0.314 |
| Motivation for participation | |||||
| Health c | 73 (62.4%) | 146 (67.9%) | 57 (80.3%) | 13 (68.4%) | 0.006 |
| To look my best c | 67 (57.3%) | 132 (61.4%) | 47 (66.2%) | 13 (68.4%) | 0.066 |
| Fitness c | 76 (65%) | 144 (67%) | 50 (70.4%) | 14 (73.7%) | 0.103 |
| Colleagues c | 117 (100%) | 209 (97.2%) | 69 (97.2%) | 18 (94.7%) | 0.336 |
| Friends or family c | 13 (11.1%) | 23 (10.7%) | 10 (14.1%) | 4 (21.1%) | 0.351 |
| BEHAVIOURAL MEASURES | |||||
| Fruit intake (meeting guidelines) c | 36 (30.8%) | 73 (34%) | 27 (38%) | 4 (21.1%) | 0.274 |
| Vegetable intake (meeting guidelines) c | 16 (13.7%) | 38 (17.7%) | 11 (15.5%) | 2 (10.5%) | 0.91 |
| Alcohol (meeting guidelines) c | 57 (48.7%) | 90 (41.9%) | 22 (31%) | 10 (52.6%) | 0.676 |
| Non smoker c | 109 (93.2%) | 198 (92.1%) | 68 (95.8%) | 14 (73.7%) | 0.284 |
| Physical activity (meeting guidelines) c | 48 (41%) | 95 (44.2%) | 27 (38%) | 6 (31.6%) | 0.003 |
| Sitting time (hours per day) | |||||
| Weekday | 8.6 ± 3.5 | 8 ± 3.5 | 8.5 ± 3.9 | 8.6 ± 4.4 | 0.991 |
| Weekend | 5.7 ± 3 | 5.3 ± 2.9 | 4.7 ± 2.2 | 5.8 ± 3.8 | 0.437 |
| Takeaway Dinner | |||||
| Once or less per month | 57 (48.7%) | 98 (45.6%) | 32 (45.1%) | 8 (42.1%) | 0.026 |
| About once a week | 46 (39.3%) | 95 (44.2%) | 25 (35.2%) | 10 (52.6%) | |
| More than once a week | 14 (12%) | 22 (10.2%) | 14 (19.7%) | 1 (5.3%) | |
| PSYCHOSOCIAL MEASURES | |||||
| Well-being | 69.2 ± 12 | 63.3 ± 15.3 | 44.1 ± 20.2 | 27.8 ± 17.4 | <0.001 |
| Well-being c (positive category) | 108 (92.3%) | 175 (81.4%) | 31 (43.7%) | 3 (15.8%) | <0.001 |
| Health related quality of life (SF-12) | |||||
| Mental health component | 54.8 ± 3.6 | 51.4 ± 7.2 | 39.2 ± 11.2 | 31.1 ± 10.8 | <0.001 |
| Physical health component | 50.7 ± 6.9 | 51 ± 7.2 | 51 ± 8.9 | 52.4 ± 7.8 | 0.676 |
| Duttweiler Internal Control Index score | 110.5 ± 10.7 | 106.4 ± 10.2 | 100.6 ± 11 | 97.3 ± 13.5 | <0.001 |
| ANTHROPOMETRIC MEASURES | |||||
| Systolic blood pressure (mmHg) | 120.1 ± 12.9 | 117.9 ± 14.6 | 120.6 ± 14.9 | 115.5 ± 14.3 | 0.053 |
| Diastolic blood pressure (mmHg) | 82.1 ± 9.8 | (203) 79.1 ± 10.4 | (66) 79.6 ± 9.3 | 78 ± 10.8 | 0.011 |
| Heart rate (beats per minute) | 70.2 ± 11.3 | (203) 68.1 ± 10.1 | (66) 67.9 ± 8.5 | 68.1 ± 9.7 | 0.868 |
| Weight (kg) | 77.1 ± 15.5 | (209) 77.6 ± 16 | (68) 76.8 ± 16 | (18) 81 ± 16.3 | 0.811 |
| Body mass index (kg/m2) | (115) 26.8 ± 5 | (209) 26.8 ± 4.6 | (68) 26.7 ± 5 | (18) 28 ± 5.8 | 0.524 |
| Waist circumference | (115) 88.1 ± 12.3 | (209) 88.6 ± 12.7 | (68) 87.4 ± 13.1 | (18) 91.9 ± 11.6 | 0.973 |
| PROCESS MEASURES | |||||
| STEP DATA | |||||
| Steps average (per day) | 11,718.5 ± 4318.3 | 11,839.6 ± 3368.2 | (70) 11,975.9 ± 4154.3 e | 10,722 ± 2555.2 | 0.135 |
| Meeting 10,000 on average (per day) | |||||
| Yes | 77 (65.8%) | 154 (71.6%) | 46 (65.7%) | 12 (63.2%) | 0.168 |
| No | 40 (34.2%) | 61 (28.4%) | 24 (34.3%) | 7 (36.8%) | |
| Meeting 7500 on average (per day) | |||||
| Yes | 159 (88.3%) | 141 (92.8%) | 62 (88.6%) | 16 (84.2%) | 0.909 |
| No | 21 (11.7%) | 11 (7.2%) | 8 (11.4%) | 3 (15.8%) | |
| Univariable Model | Multivariable Model b | |||||
|---|---|---|---|---|---|---|
| Predictor Variable | n | Crude Psychological Distress Change (Units) | Psychological Distress Change B (95% CI) | p-Value | Psychological Distress Change B (95% CI) | p-Value |
| Age (years) | 489 | −1.4 | −0.1 (−0.1, −0.01) | 0.024 | −0.02 (−0.1, 0.05) | 0.549 |
| Sex | ||||||
| Female | 200 | −1.4 | REFERENCE | REFERENCE | ||
| Male | 289 | −1.5 | 0.4 (−0.7, 1.6) | 0.428 | −0.5 (−2.1, 1.1) | 0.477 |
| Tertiary education | ||||||
| Not completed | 95 | −1.1 | REFERENCE | REFERENCE | ||
| Completed | 394 | −1.5 | −0.4 (−2.0, 1.1) | 0.539 | −0.7 (−2.4, 1.0) | 0.367 |
| Partner Status | ||||||
| Married/de facto | 351 | −1.4 | REFERENCE | REFERENCE | ||
| Widowed, separated or divorced | 47 | −3.1 | −2.2 (−3.8, −0.6) | 0.012 | −2.0 (−4.3, 0.3) | 0.081 |
| Never married | 91 | −0.6 | 0.8 (−0.2, 1.7) | 0.105 | 0.7 (−0.3, 1.7) | 0.162 |
| Socio Economic Status by residential postcode (SEIFA) | ||||||
| Most Advantaged | 29 | −1.6 | −0.9 (−2.0, 0.1) | 0.078 | −0.3 (−2.0, 1.4) | 0.671 |
| Advantaged | 213 | −2.2 | −0.4 (−2.6, 1.7) | 0.659 | 0.1 (−1.2, 1.4) | 0.884 |
| Disadvantaged | 80 | −0.9 | 0.2(−1.5, 1.9) | 0.807 | 0.3 (−1.0, 1.7) | 0.585 |
| Most Disadvantaged | 29 | −1.0 | REFERENCE | REFERENCE | ||
| Occupation | ||||||
| Professional | 213 | −1.4 | REFERENCE | REFERENCE | ||
| Associate professional | 90 | −2.0 | −0.7 (−1.0, −0.3) | 0.004 | −1.1 (−1.8, −0.4) | 0.005 |
| Manager | 88 | −1.7 | −0.7 (−1.8, 0.5) | 0.226 | −0.7 (−1.7, 0.3) | 0.142 |
| Clerical or Service | 64 | −0.3 | 1.1 (−0.5, 2.8) | 0.162 | 0.7 (−0.2, 1.7) | 0.123 |
| Steps average per day (per 10,000 steps) | 488 | −1.4 | −0.0001 (−0.0003, −0.00001) | 0.032 | * | |
| Meeting 10,000 daily step goal | ||||||
| Yes | 329 | −1.8 | −1.1 (−2.0, −0.2) | 0.024 | −0.6 (−1.6, 0.5) | 0.272 |
| No | 159 | −0.7 | REFERENCE | REFERENCE | ||
| Meeting 7500 steps (on average) c | ||||||
| Yes | 440 | −0.6 | −1.0 (−2.6, 0.6) | 0.200 | −0.9 (−2.5, 0.7) | 0.228 |
| No | 48 | 0.4 | REFERENCE | REFERENCE | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stone, J.; Barker, S.F.; Gasevic, D.; Freak-Poli, R. Participation in the Global Corporate Challenge®, a Four-Month Workplace Pedometer Program, Reduces Psychological Distress. Int. J. Environ. Res. Public Health 2023, 20, 4514. https://doi.org/10.3390/ijerph20054514
Stone J, Barker SF, Gasevic D, Freak-Poli R. Participation in the Global Corporate Challenge®, a Four-Month Workplace Pedometer Program, Reduces Psychological Distress. International Journal of Environmental Research and Public Health. 2023; 20(5):4514. https://doi.org/10.3390/ijerph20054514
Chicago/Turabian StyleStone, Jessica, S. Fiona Barker, Danijela Gasevic, and Rosanne Freak-Poli. 2023. "Participation in the Global Corporate Challenge®, a Four-Month Workplace Pedometer Program, Reduces Psychological Distress" International Journal of Environmental Research and Public Health 20, no. 5: 4514. https://doi.org/10.3390/ijerph20054514