
Multi-Component Intervention to Promote Physical Activity in Japanese Office Workers: A Single-Arm Feasibility Study


Abstract
:1. Introduction
2. Materials and Methods
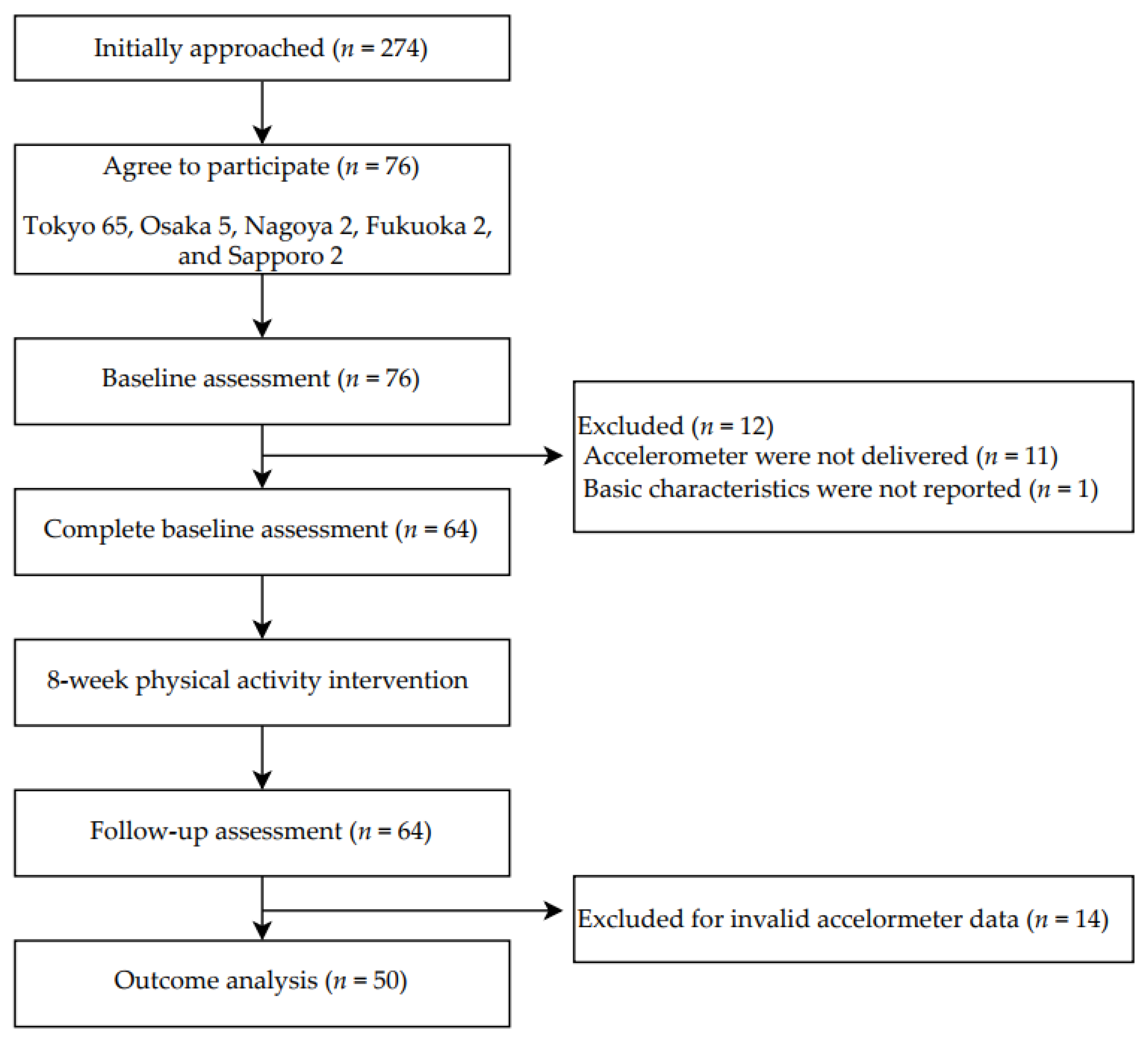
2.1. Design and Participants
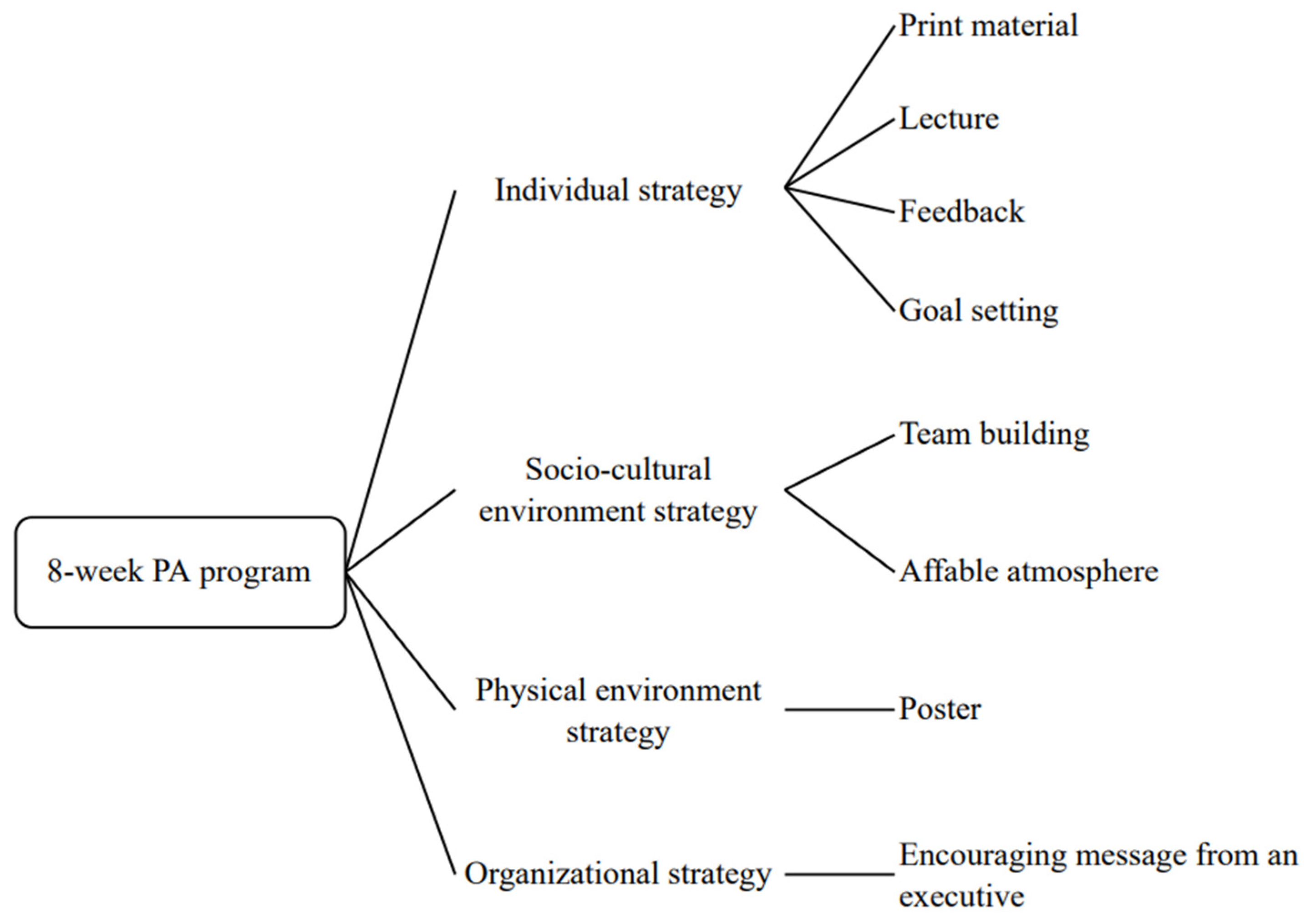
2.2. Intervention Program
2.2.1. Individual Strategy
2.2.2. Socio-Cultural Environment Strategy
2.2.3. Physical Environment Strategy
2.2.4. Organizational Strategy
2.3. Measurements
2.3.1. Baseline Characteristics
2.3.2. Primary and Secondary Outcomes
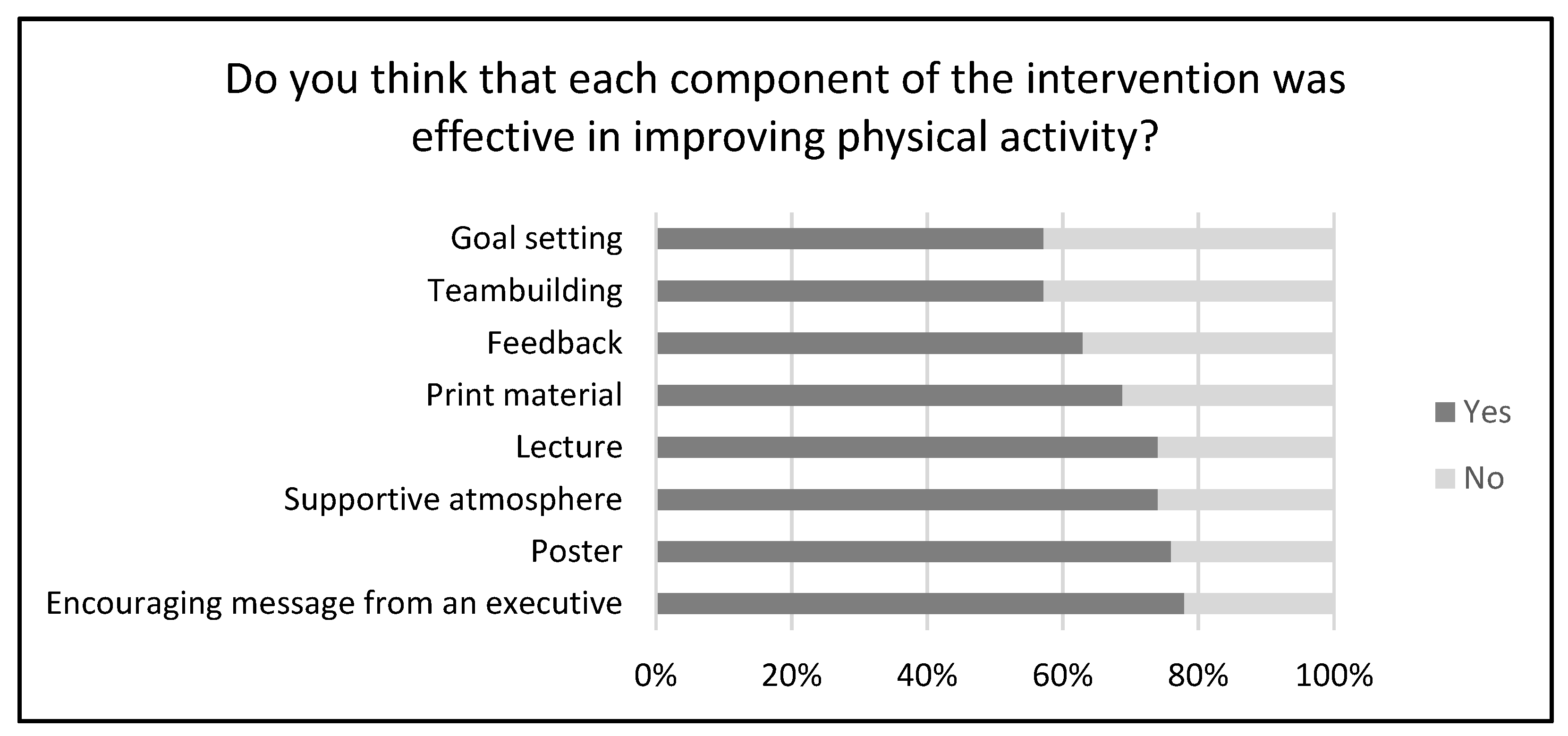
2.3.3. Post-Intervention Survey
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Fact Sheets of Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 28 April 2022).
- Galper, D.I.; Trivedi, M.H.; Barlow, C.E.; Dunn, A.L.; Kampert, J.B. Inverse Association between Physical Inactivity and Mental Health in Men and Women. Med. Sci. Sport. Exerc. 2006, 38, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M.; Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sport. Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Active Guide—Japanese Official Physical Activity Guidelines for Health Promotion. Available online: https://www.nibiohn.go.jp/eiken/programs/pdf/active2013-e.pdf (accessed on 28 April 2022).
- Ross, R.; Chaput, J.-P.; Giangregorio, L.M.; Janssen, I.; Saunders, T.J.; Kho, M.E.; Poitras, V.J.; Tomasone, J.R.; El-Kotob, R.; McLaughlin, E.C.; et al. Canadian 24-Hour Movement Guidelines for Adults aged 18–64 years and Adults aged 65 years or older: An integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 2020, 45, S57–S102. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, B.; Schnall, P.L.; Yang, H.; Dobson, M.; Landsbergis, P.; Israel, L.; Karasek, R.; Baker, D. Sedentary work, low physical job demand, and obesity in US workers. Am. J. Ind. Med. 2010, 53, 1088–1101. [Google Scholar] [CrossRef]
- Van Dongen, J.M.; Proper, K.I.; Van Wier, M.F.; Van Der Beek, A.J.; Bongers, P.M.; Van Mechelen, W.; Van Tulder, M.W. A systematic review of the cost-effectiveness of worksite physical activity and/or nutrition programs. Scand. J. Work. Environ. Health 2012, 38, 393–408. [Google Scholar] [CrossRef] [Green Version]
- van Uffelen, J.G.; Wong, J.; Chau, J.Y.; van der Ploeg, H.P.; Riphagen, I.; Gilson, N.D.; Burton, N.W.; Healy, G.N.; Thorp, A.A.; Clark, B.K.; et al. Occupational Sitting and Health Risks: A Systematic Review. Am. J. Prev. Med. 2010, 39, 379–388. [Google Scholar] [CrossRef] [Green Version]
- Prince, S.A.; Elliott, C.G.; Scott, K.; Visintini, S.; Reed, J.L. Device-measured physical activity, sedentary behaviour and cardiometabolic health and fitness across occupational groups: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 30. [Google Scholar] [CrossRef]
- Ishii, K.; Shibata, A.; Oka, K. Work Engagement, Productivity, and Self-Reported Work-Related Sedentary Behavior Among Japanese Adults. J. Occup. Environ. Med. 2018, 60, e173–e177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munir, F.; Houdmont, J.; Clemes, S.; Wilson, K.; Kerr, R.; Addley, K. Work engagement and its association with occupational sitting time: Results from the Stormont study. BMC Public Health 2015, 15, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, T.J.; Tullar, J.M.; Diamond, P.M.; Kohl, H.W.; Amick, B.C. The longitudinal relation between self-reported physical activity and presenteeism. Prev. Med. 2017, 102, 120–126. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. 2018. Available online: https://apps.who.int/iris/handle/10665/272722 (accessed on 28 April 2022).
- Watanabe, K.; Kawakami, N. Effects of a Multi-Component Workplace Intervention Program with Environmental Changes on Physical Activity among Japanese White-Collar Employees: A Cluster-Randomized Controlled Trial. Int. J. Behav. Med. 2018, 25, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Brakenridge, C.L.; Fjeldsoe, B.S.; Young, D.C.; Winkler, E.A.H.; Dunstan, D.W.; Straker, L.M.; Healy, G.N. Evaluating the effectiveness of organisational-level strategies with or without an activity tracker to reduce office workers’ sitting time: A cluster-randomised trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 115. [Google Scholar] [CrossRef] [Green Version]
- Bergman, F.; Wahlström, V.; Stomby, A.; Otten, J.; Lanthén, E.; Renklint, R.; Waling, M.; Sörlin, A.; Boraxbekk, C.-J.; Wennberg, P.; et al. Treadmill workstations in office workers who are overweight or obese: A randomised controlled trial. Lancet Public Health 2018, 3, e523–e535. [Google Scholar] [CrossRef] [Green Version]
- Gremaud, A.L.; Carr, L.J.; Simmering, J.E.; Evans, N.J.; Cremer, J.F.; Segre, A.M.; Polgreen, L.A.; Polgreen, P.M. Gamifying Accelerometer Use Increases Physical Activity Levels of Sedentary Office Workers. J. Am. Heart Assoc. 2018, 7, e007735. [Google Scholar] [CrossRef] [Green Version]
- Jirathananuwat, A.; Pongpirul, K. Promoting physical activity in the workplace: A systematic meta-review. J. Occup. Health 2017, 59, 385–393. [Google Scholar] [CrossRef]
- Bredahl, T.V.G.; Særvoll, C.A.; Kirkelund, L.; Sjøgaard, G.; Andersen, L.L. When Intervention Meets Organisation, a Qualitative Study of Motivation and Barriers to Physical Exercise at the Workplace. Sci. World J. 2015, 2015, 518561. [Google Scholar] [CrossRef] [Green Version]
- Stankevitz, K.; Dement, J.; Schoenfisch, A.; Joyner, J.; Clancy, S.M.; Stroo, M.; Østbye, T. Perceived Barriers to Healthy Eating and Physical Activity Among Participants in a Workplace Obesity Intervention. J. Occup. Environ. Med. 2017, 59, 746–751. [Google Scholar] [CrossRef]
- Morris, A.; Murphy, R.; Shepherd, S.; Graves, L. Multi-Stakeholder Perspectives of Factors That Influence Contact Centre Call Agents’ Workplace Physical Activity and Sedentary Behaviour. Int. J. Environ. Res. Public Health 2018, 15, 1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amini, H.; Habibi, S.; Islamoglu, A.H.; Isanejad, E.; Uz, C.; Daniyari, H. COVID-19 pandemic-induced physical inactivity: The necessity of updating the Global Action Plan on Physical Activity 2018-2030. Environ. Health Prev. Med. 2021, 26, 32. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, N.; Kuroda, R.; Tsuno, K.; Kawakami, N. Workplace responses to COVID-19 associated with mental health and work performance of employees in Japan. J. Occup. Health 2020, 62, e12134. [Google Scholar] [CrossRef]
- Okawara, M.; Ishimaru, T.; Tateishi, S.; Hino, A.; Tsuji, M.; Ikegami, K.; Nagata, M.; Matsuda, S.; Fujino, Y. Association Between the Physical Work Environment and Work Functioning Impairment While Working From Home Under the COVID-19 Pandemic in Japanese Workers. J. Occup. Environ. Med. 2021, 63, e565–e570. [Google Scholar] [CrossRef]
- Kim, J.; Mizushima, R.; Nishida, K.; Morimoto, M.; Nakata, Y. Proposal of a Comprehensive and Multi-Component Approach to Promote Physical Activity among Japanese Office Workers: A Qualitative Focus Group Interview Study. Int. J. Environ. Res. Public Health 2022, 19, 2172. [Google Scholar] [CrossRef]
- Miyachi, M.; Tripette, J.; Kawakami, R.; Murakami, H. “+10 min of Physical Activity per Day”: Japan Is Looking for Efficient but Feasible Recommendations for Its Population. J. Nutr. Sci. Vitaminol. 2015, 61, S7–S9. [Google Scholar] [CrossRef] [Green Version]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Diaz, K.; Howard, V.J.; Hutto, B.; Colabianchi, N.; Vena, J.E.; Safford, M.M.; Blair, S.N.; Hooker, S.P. Patterns of Sedentary Behavior and Mortality in U.S. Middle-Aged and Older Adults. Ann. Intern. Med. 2017, 167, 465–475. [Google Scholar] [CrossRef]
- Ohkawara, K.; Oshima, Y.; Hikihara, Y.; Ishikawa-Takata, K.; Tabata, I.; Tanaka, S. Real-time estimation of daily physical activity intensity by a triaxial accelerometer and a gravity-removal classification algorithm. Br. J. Nutr. 2011, 105, 1681–1691. [Google Scholar] [CrossRef]
- Oshima, Y.; Kawaguchi, K.; Tanaka, S.; Ohkawara, K.; Hikihara, Y.; Ishikawa-Takata, K.; Tabata, I. Classifying household and locomotive activities using a triaxial accelerometer. Gait Posture 2010, 31, 370–374. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Mâsse, L.C.; Tilert, T.; Mcdowell, M. Physical Activity in the United States Measured by Accelerometer. Med. Sci. Sport. Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Mâsse, L.; Fuemmeler, B.; Anderson, C.B.; Matthews, C.; Trost, S.; Catellier, D.J.; Treuth, M. Accelerometer Data Reduction: A Comparison of Four Reduction Algorithms on Select Outcome Variables. Med. Sci. Sport. Exerc. 2005, 37, S544–S554. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Blom, V.; Nooijen, C.F.J.; Kallings, L.V.; Ekblom, M.M. The Role of Executive Function in the Effectiveness of Multi-Component Interventions Targeting Physical Activity Behavior in Office Workers. Int. J. Environ. Res. Public Health 2021, 19, 266. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.; Straker, L.; Gilson, N.; Smith, A.J. Participatory Workplace Interventions Can Reduce Sedentary Time for Office Workers—A Randomised Controlled Trial. PLoS ONE 2013, 8, e78957. [Google Scholar] [CrossRef] [PubMed]
- Carr, L.J.; Leonhard, C.; Tucker, S.; Fethke, N.; Benzo, R.; Gerr, F. Total Worker Health Intervention Increases Activity of Sedentary Workers. Am. J. Prev. Med. 2015, 50, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Buja, A.; Rabensteiner, A.; Sperotto, M.; Grotto, G.; Bertoncello, C.; Cocchio, S.; Baldovin, T.; Contu, P.; Lorini, C.; Baldo, V. Health Literacy and Physical Activity: A Systematic Review. J. Phys. Act. Health 2020, 17, 1259–1274. [Google Scholar] [CrossRef]
- Ding, D.; Cheng, M.; Cruz, B.D.P.; Lin, T.; Sun, S.; Zhang, L.; Yang, Q.; Ma, Z.; Wang, J.; Jia, Y.; et al. How COVID-19 lockdown and reopening affected daily steps: Evidence based on 164,630 person-days of prospectively collected data from Shanghai, China. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 40. [Google Scholar] [CrossRef]
- Fukushima, N.; Machida, M.; Kikuchi, H.; Amagasa, S.; Hayashi, T.; Odagiri, Y.; Takamiya, T.; Inoue, S. Associations of working from home with occupational physical activity and sedentary behavior under the COVID-19 pandemic. J. Occup. Health 2021, 63, e12212. [Google Scholar] [CrossRef]
- Public Health England. 10 Minutes Brisk Walking Each Day in Mid-Life for Health Benefits and towards Achieving Physical Activity Recommendations: Evidence Summary. 24 August 2017. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/639030/Health_benefits_of_10_mins_brisk_walking_evidence_summary.pdf (accessed on 11 May 2022).
- Sarkar, S.; Taylor, W.C.; Lai, D.; Shegog, R.; Paxton, R.J. Social support for physical activity: Comparison of family, friends, and coworkers. Work 2016, 55, 893–899. [Google Scholar] [CrossRef]
- Tabak, R.G.; Hipp, J.A.; Marx, C.M.; Brownson, R.C. Workplace Social and Organizational Environments and Healthy-Weight Behaviors. PLoS ONE 2015, 10, e0125424. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.R. Clinical trial structures. J. Exp. Stroke Transl. Med. 2010, 3, 8–18. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Participants (n = 64) |
|---|---|
| Age, years | 49.6 (9.3) |
| Women, n (%) | 10 (16) |
| Height, cm | 171.9 (7.4) |
| Weight, kg; n = 61 * | 69.8 (12.9) |
| Body mass index, kg/m2; n = 61 * | 23.3 (3.3) |
| Current smoker, n (%); n = 59 * | 6 (10) |
| Four-year college graduate, n (%) | 61 (95) |
| Continuous years of service, years; n = 59 * | 10 (0, 37) |
| Living with one or other people, n (%); n = 59 * | 55 (93) |
| Currently married, n (%); n = 59 * | 52 (89) |
| Week 0 | Week 8 | Change (95% CI) | p-Value | |
|---|---|---|---|---|
| Characteristic | ||||
| Age, years | 49.6 (9.8) | |||
| Women, n (%) | 10 (20) | |||
| BMI, kg/m2; n = 47 * | 22.8 (3.1) | |||
| Physical activity outcomes | ||||
| MVPA, min/day | 50.0 (27.1) | 57.3 (29.8) | 7.3 (0.8 to 13.8) | 0.028 |
| LPA, min/day | 196.1 (64.6) | 197.8 (67.9) | 1.7 (−10.8 to 14.3) | 0.786 |
| MPA, min/day | 48.9 (26.8) | 55.5 (29.5) | 6.6 (0.3 to 13.0) | 0.042 |
| VPA, min/day | 1.1 (3.2) | 1.8 (4.8) | 0.7 (−0.1 to 1.4) | 0.071 |
| Steps, steps/day | 6701 (2859) | 7574 (3003) | 873 (169 to 1576) | 0.016 |
| ST, min/day | 573.4 (85.2) | 566.6 (89.2) | −6.9 (−27.9 to 14.2) | 0.515 |
| Valid day | 6.9 (1.7) | 6.8 (1.4) | −0.1 (−0.7 to 0.4) | 0.654 |
| Week 0 | Week 8 | Change (95% CI) | p-Value | |
|---|---|---|---|---|
| Characteristic | ||||
| Age, years | 51.1 (8.9) | |||
| Women, n (%) | 8 (20) | |||
| BMI, kg/m2; n = 38 * | 22.5 (2.9) | |||
| Physical activity outcomes on working day | ||||
| MVPA, min/day | 45.8 (27.4) | 55.7 (28.8) | 10.0 (3.7 to 16.3) | 0.003 |
| LPA, min/day | 186.3 (65.3) | 193.1 (69.2) | 6.8 (−5.6 to 19.2) | 0.272 |
| MPA, min/day | 45.1 (27.2) | 54.1 (28.3) | 9.0 (2.8 to 15.1) | 0.005 |
| VPA, min/day | 0.6 (1.7) | 1.7 (3.5) | 1.0 (0.01 to 2.1) | 0.047 |
| Steps, steps/day | 6212 (2860) | 7384 (2985) | 1172 (365 to 1979) | 0.006 |
| ST, min/day | 620.8 (92.0) | 607.1 (94.9) | −13.7 (−34.0 to 6.6) | 0.180 |
| Valid day | 4.4 (1.1) | 4.8 (1.2) | 0.4 (−0.1 to 0.9) | 0.081 |
| Physical activity outcomes on non-working day | ||||
| MVPA, min/day | 63.7 (41.5) | 77.4 (51.0) | 13.7 (−2.0 to 29.5) | 0.086 |
| LPA, min/day | 252.0 (90.0) | 249.4 (93.9) | −2.6 (−33.8 to 28.6) | 0.866 |
| MPA, min/day | 60.8 (41.4) | 74.4 (51.7) | 13.6 (−2.0 to 29.2) | 0.086 |
| VPA, min/day | 3.0 (9.0) | 3.1 (12.1) | 0.1 (−1.5 to 1.7) | 0.885 |
| Steps, steps/day | 8244 (4461) | 9553 (4451) | 1310 (63 to 2557) | 0.040 |
| ST, min/day | 466.1 (108.4) | 461.3 (121.2) | −4.8 (−49.2 to 39.6) | 0.828 |
| Valid day | 2.9 (0.9) | 2.2 (0.8) | −0.7 (−1.0 to −0.4) | <0.001 |
| Week 0 | Week 8 | Change (95% CI) | p-Value | |
|---|---|---|---|---|
| Characteristic | ||||
| Age, years | 49.6 (9.4) | |||
| Women, n (%) | 8 (24) | |||
| BMI, kg/m2; n = 31 * | 23.0 (3.0) | |||
| Physical activity outcomes on commuting working day | ||||
| MVPA, min/day | 58.5 (27.5) | 62.0 (25.3) | 3.5 (−2.8 to 9.9) | 0.263 |
| LPA, min/day | 179.7 (72.8) | 189.3 (80.4) | 9.6 (−9.2 to 28.4) | 0.307 |
| MPA, min/day | 58.1 (27.6) | 61.4 (25.0) | 3.3 (−3.0 to 9.5) | 0.292 |
| VPA, min/day | 0.4 (0.8) | 0.6 (1.0) | 0.2 (−0.02 to 0.5) | 0.068 |
| Steps, steps/day | 8215 (2681) | 8755 (2674) | 540 (−274 to 1355) | 0.186 |
| ST, min/day | 627.8 (98.8) | 618.4 (87.8) | −9.4 (−32.9 to 14.0) | 0.420 |
| Valid day | 2.1 (1.0) | 2.4 (1.0) | 0.3 (−0.1 to 0.8) | 0.133 |
| Physical activity outcomes on remote working day | ||||
| MVPA, min/day | 34.1 (33.9) | 41.5 (35.9) | 7.1 (0.4 to 13.7) | 0.037 |
| LPA, min/day | 175.9 (68.6) | 170.7 (67.1) | −5.2 (−19.4 to 9.0) | 0.460 |
| MPA, min/day | 32.9 (33.7) | 40.2 (35.6) | 7.3 (0.8 to 13.7) | 0.028 |
| VPA, min/day | 1.5 (5.5) | 1.3 (3.4) | −0.2 (−1.3 to 1.0) | 0.758 |
| Steps, steps/day | 4261 (3526) | 5087 (3498) | 826 (46 to 1606) | 0.039 |
| ST, min/day | 610.0 (104.6) | 612.7 (95.1) | 2.7 (−21.8 to 27.2) | 0.823 |
| Valid day | 2.4 (1.3) | 2.6 (1.2) | 0.2 (−0.3 to 0.7) | 0.439 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Mizushima, R.; Nishida, K.; Morimoto, M.; Nakata, Y. Multi-Component Intervention to Promote Physical Activity in Japanese Office Workers: A Single-Arm Feasibility Study. Int. J. Environ. Res. Public Health 2022, 19, 16859. https://doi.org/10.3390/ijerph192416859
Kim J, Mizushima R, Nishida K, Morimoto M, Nakata Y. Multi-Component Intervention to Promote Physical Activity in Japanese Office Workers: A Single-Arm Feasibility Study. International Journal of Environmental Research and Public Health. 2022; 19(24):16859. https://doi.org/10.3390/ijerph192416859
Chicago/Turabian StyleKim, Jihoon, Ryoko Mizushima, Kotaro Nishida, Masahiro Morimoto, and Yoshio Nakata. 2022. "Multi-Component Intervention to Promote Physical Activity in Japanese Office Workers: A Single-Arm Feasibility Study" International Journal of Environmental Research and Public Health 19, no. 24: 16859. https://doi.org/10.3390/ijerph192416859