
Dynamic Nomogram for Predicting Long-Term Survival in Terms of Preoperative and Postoperative Radiotherapy Benefits for Advanced Gastric Cancer

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Variables
2.3. Statistical Analysis
2.4. Dynamic Nomogram Construction
3. Results
3.1. Demographics and Clinical Characteristics of the Cohort
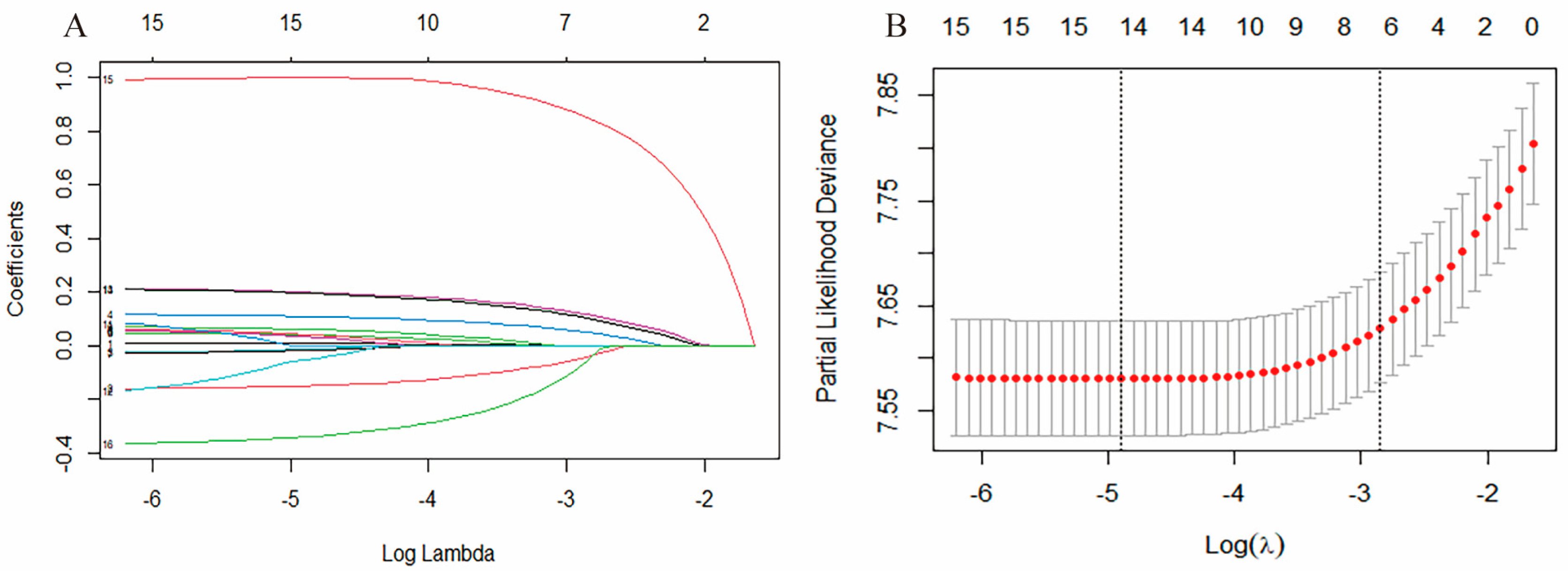
3.2. Feature Selection
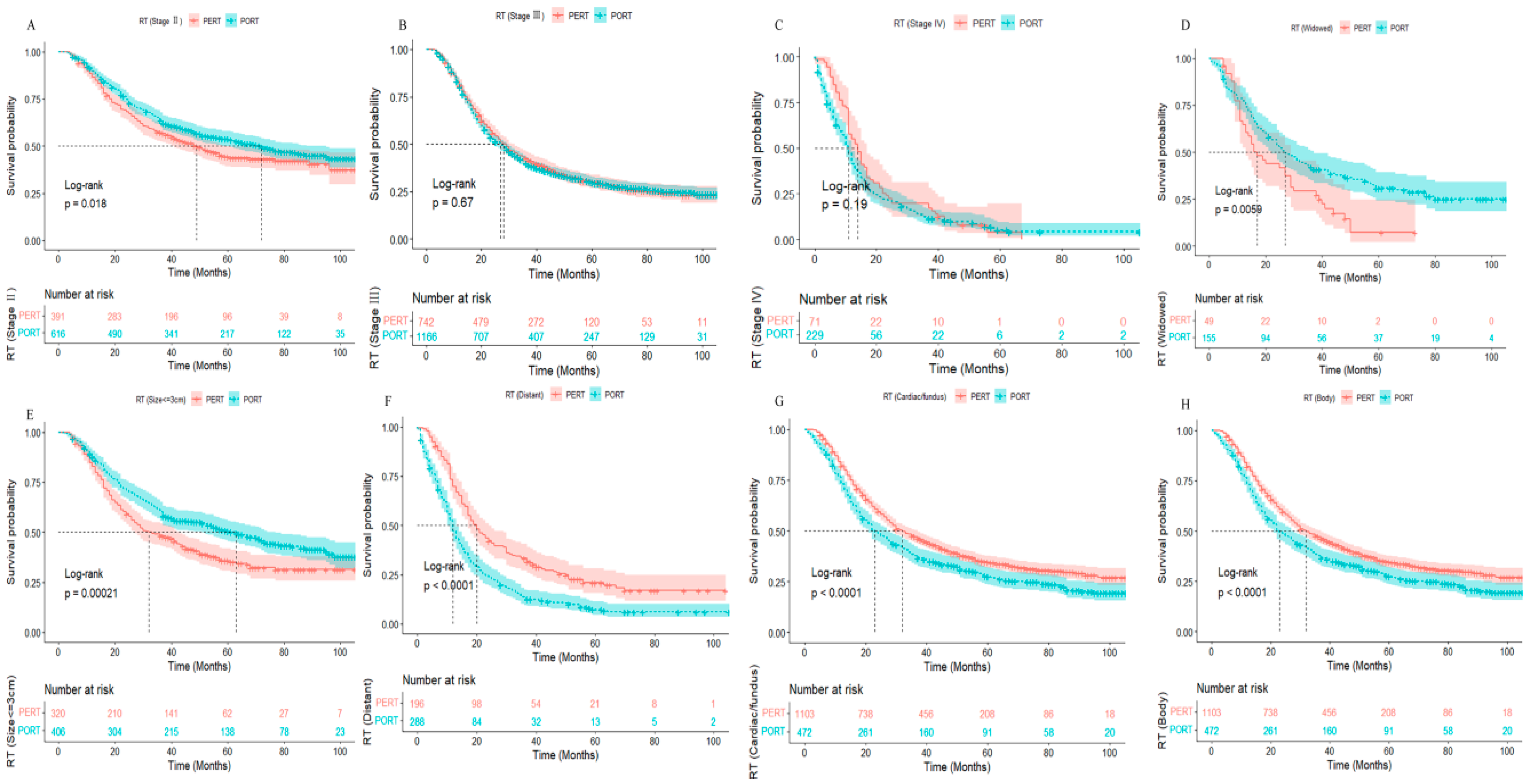
3.3. Survival Outcomes
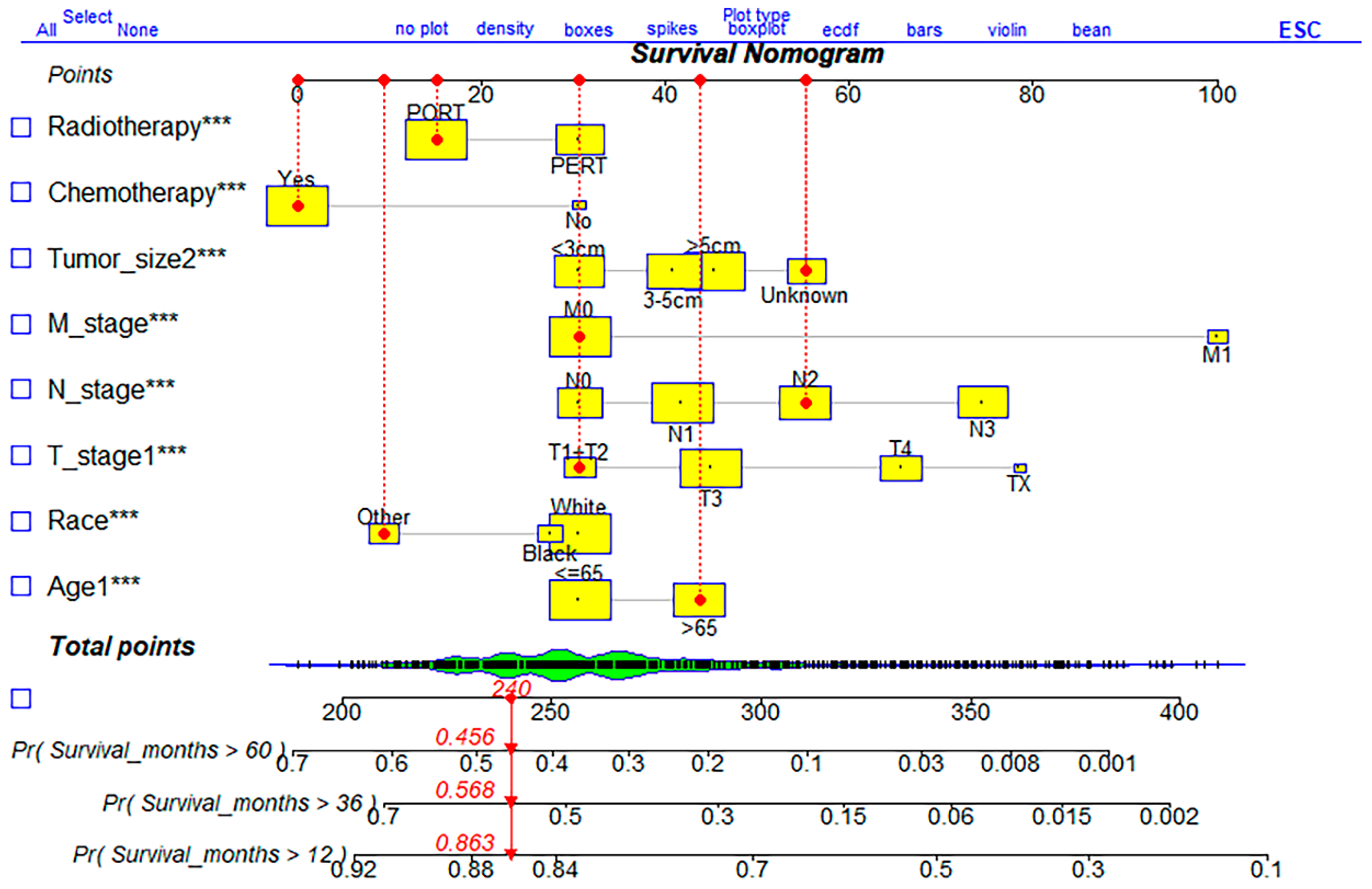
3.4. Nomogram Model Developed to Predict Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; D’Amico, T.A.; Almhanna, K.; Bentrem, D.J.; Chao, J.; Das, P.; Denlinger, C.S.; Fanta, P.; Farjah, F.; Fuchs, C.S.; et al. Gastric Cancer, Version 3.2016, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2016, 14, 1286–1312. [Google Scholar] [CrossRef]
- Brenner, H.; Rothenbacher, D.; Arndt, V. Epidemiology of stomach cancer. Methods Mol. Biol. 2009, 472, 467–477. [Google Scholar]
- Tan, H.L.; Chia, C.S.; Tan, G.H.C.; Choo, S.P.; Tai, D.W.; Chua, C.W.L.; Ng, M.C.H.; Soo, K.C.; Teo, M.C.C. Metastatic gastric cancer: Does the site of metastasis make a difference? Asia Pac. J. Clin. Oncol. 2019, 15, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Songun, I.; Putter, H.; Kranenbarg, E.M.; Sasako, M.; van de Velde, C.J. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010, 11, 439–449. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Macdonald, J.S.; Smalley, S.R.; Benedetti, J.; Hundahl, S.A.; Estes, N.C.; Stemmermann, G.N.; Haller, D.G.; Ajani, J.A.; Gunderson, L.L.; Jessup, J.M.; et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N. Engl. J. Med. 2001, 345, 725–730. [Google Scholar] [CrossRef]
- Gotze, T.O.; Piso, P.; Lorenzen, S.; Bankstahl, U.S.; Pauligk, C.; Elshafei, M.; Amato, G.; Reim, D.; Bechstein, W.O.; Konigsrainer, A.; et al. Preventive HIPEC in combination with perioperative FLOT versus FLOT alone for resectable diffuse type gastric and gastroesophageal junction type II/III adenocarcinoma—The phase III “PREVENT”-(FLOT9) trial of the AIO/CAOGI/ACO. BMC Cancer 2021, 21, 1158. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lim, D.H.; Kim, S.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Choi, M.G.; Sohn, T.S.; Noh, J.H.; et al. Phase III trial comparing capecitabine plus cisplatin versus capecitabine plus cisplatin with concurrent capecitabine radiotherapy in completely resected gastric cancer with D2 lymph node dissection: The ARTIST trial. J. Clin. Oncol. 2012, 30, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Caulfield, S.; Menezes, G.; Marignol, L.; Poole, C. Nomograms are key decision-making tools in prostate cancer radiation therapy. Urol. Oncol. 2018, 36, 283–292. [Google Scholar] [CrossRef]
- Nieder, C.; Mehta, M.P.; Geinitz, H.; Grosu, A.L. Prognostic and predictive factors in patients with brain metastases from solid tumors: A review of published nomograms. Crit. Rev. Oncol. Hematol. 2018, 126, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Qiu, M.Z.; Shi, S.M.; Chen, Z.H.; Yu, H.E.; Sheng, H.; Jin, Y.; Wang, D.S.; Wang, F.H.; Li, Y.H.; Xie, D.; et al. Frequency and clinicopathological features of metastasis to liver, lung, bone, and brain from gastric cancer: A SEER-based study. Cancer Med. 2018, 7, 3662–3672. [Google Scholar] [CrossRef]
- Li, Y.; Cao, Y.; Zheng, M.; Hu, J.; Yan, W.; Liu, X.; Liao, A.; Yang, W.; Li, J.; Wang, H. Nomogram Model for Dynamic and Individual Prediction of Cardiac Response and Survival for Light Chain Amyloidosis in 737 Patients with Cardiac Involvement. Front. Oncol. 2021, 11, 758502. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Huang, X.; Yang, W.; Li, C.; Li, Z.; Zhang, C.; Chen, S.; Wu, G.; Xie, W.; Wei, C.; et al. Nomogram for predicting overall survival in stage II-III colorectal cancer. Cancer Med. 2020, 9, 2363–2371. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Kim, Y.; Jeong, K.; Jeong, H.; Kim, J. Logistic LASSO regression for the diagnosis of breast cancer using clinical demographic data and the BI-RADS lexicon for ultrasonography. Ultrasonography 2018, 37, 36–42. [Google Scholar] [CrossRef]
- Joshi, S.S.; Badgwell, B.D. Current treatment and recent progress in gastric cancer. CA Cancer J. Clin. 2021, 71, 264–279. [Google Scholar] [CrossRef]
- Li, S.S.; Klempner, S.J.; Costantino, C.L.; Parikh, A.; Clark, J.W.; Wo, J.Y.; Hong, T.S.; Mullen, J.T. Impact of Treatment Sequencing on Survival for Patients with Locally Advanced Gastric Cancer. Ann. Surg. Oncol. 2021, 28, 2856–2865. [Google Scholar] [CrossRef]
- Zhang, Y.; Yu, J. The role of MRI in the diagnosis and treatment of gastric cancer. Diagn. Interv. Radiol. 2020, 26, 176–182. [Google Scholar] [CrossRef]
- Chon, H.J.; Hyung, W.J.; Kim, C.; Park, S.; Kim, J.H.; Park, C.H.; Ahn, J.B.; Kim, H.; Chung, H.C.; Rha, S.Y.; et al. Differential Prognostic Implications of Gastric Signet Ring Cell Carcinoma: Stage Adjusted Analysis from a Single High-volume Center in Asia. Ann. Surg. 2017, 265, 946–953. [Google Scholar] [CrossRef]
- Lin, S.J.; Gagnon-Bartsch, J.A.; Tan, I.B.; Earle, S.; Ruff, L.; Pettinger, K.; Ylstra, B.; van Grieken, N.; Rha, S.Y.; Chung, H.C.; et al. Signatures of tumour immunity distinguish Asian and non-Asian gastric adenocarcinomas. Gut 2015, 64, 1721–1731. [Google Scholar] [CrossRef]
- Coit, D.G.; Andtbacka, R.; Anker, C.J.; Bichakjian, C.K.; Carson, W.E., 3rd; Daud, A.; Dimaio, D.; Fleming, M.D.; Guild, V.; Halpern, A.C.; et al. Melanoma, version 2.2013: Featured updates to the NCCN guidelines. J. Natl. Compr. Canc. Netw. 2013, 11, 395–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noh, S.H.; Park, S.R.; Yang, H.K.; Chung, H.C.; Chung, I.J.; Kim, S.W.; Kim, H.H.; Choi, J.H.; Kim, H.K.; Yu, W.; et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1389–1396. [Google Scholar] [CrossRef] [PubMed]
- de Steur, W.O.; van Amelsfoort, R.M.; Hartgrink, H.H.; Putter, H.; Kranenbarg, E.M.-K.; van Grieken, N.C.T.; van Sandick, J.W.; Claassen, Y.H.M.; Braak, J.; Jansen, E.P.M.; et al. Adjuvant chemotherapy is superior to chemoradiation after D2 surgery for gastric cancer in the per-protocol analysis of the randomized CRITICS trial. Ann. Oncol. 2021, 32, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Lim, D.H.; Sohn, T.S.; Lee, J.; Zang, D.Y.; Kim, S.T.; Kang, J.H.; Oh, S.Y.; Hwang, I.G.; Ji, J.H.; et al. A randomized phase III trial comparing adjuvant single-agent S1, S-1 with oxaliplatin, and postoperative chemoradiation with S-1 and oxaliplatin in patients with node-positive gastric cancer after D2 resection: The ARTIST 2 trial(). Ann. Oncol. 2021, 32, 368–374. [Google Scholar] [CrossRef]
- Zhang, Z.X.; Gu, X.Z.; Yin, W.B.; Huang, G.J.; Zhang, D.W.; Zhang, R.G. Randomized clinical trial on the combination of preoperative irradiation and surgery in the treatment of adenocarcinoma of gastric cardia (AGC)--report on 370 patients. Int. J. Radiat. Oncol. Biol. Phys. 1998, 42, 929–934. [Google Scholar] [CrossRef]
- Stahl, M.; Walz, M.K.; Stuschke, M.; Lehmann, N.; Meyer, H.J.; Riera-Knorrenschild, J.; Langer, P.; Engenhart-Cabillic, R.; Bitzer, M.; Konigsrainer, A.; et al. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J. Clin. Oncol. 2009, 27, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Ke, J.; Zhang, D.; Zhang, Y.; Fu, Y.; Cao, B.; Zhao, D. A dynamic nomogram for predicting diabetic macular edema in type 2 diabetes patients based on plasma cytokines. Aging 2021, 13, 8369–8379. [Google Scholar] [CrossRef]
- Deng, H.; Yu, X.; Gao, K.; Liu, Y.; Tong, Z.; Liu, Y.; Li, W. Dynamic Nomogram for Predicting Thrombocytopenia in Adults with Acute Pancreatitis. J. Inflamm. Res. 2021, 14, 6657–6667. [Google Scholar] [CrossRef]
- Wakatsuki, K.; Matsumoto, S.; Migita, K.; Kunishige, T.; Nakade, H.; Miyao, S.; Sho, M. Risk Factors and Risk Scores for Predicting Early Recurrence After Curative Gastrectomy in Patients with Stage III Gastric Cancer. J. Gastrointest. Surg. 2020, 24, 1758–1769. [Google Scholar] [CrossRef]
- Mikami, J.; Kimura, Y.; Makari, Y.; Fujita, J.; Kishimoto, T.; Sawada, G.; Nakahira, S.; Nakata, K.; Tsujie, M.; Ohzato, H. Clinical outcomes and prognostic factors for gastric cancer patients with bone metastasis. World J. Surg. Oncol. 2017, 15, 8. [Google Scholar] [CrossRef]
- Ma, J.; Shen, H.; Kapesa, L.; Zeng, S. Lauren classification and individualized chemotherapy in gastric cancer. Oncol. Lett. 2016, 11, 2959–2964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, L.Y.; Zhang, W.H.; Chen, X.Z.; Yang, K.; Chen, X.L.; Liu, K.; Zhang, B.; Chen, Z.X.; Chen, J.P.; Zhou, Z.G.; et al. Prognostic Significance of Tumor Size in 2405 Patients with Gastric Cancer: A Retrospective Cohort Study. Medicine 2015, 94, e2288. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total (n = 3215) | PERT (n = 1204) | PORT (n = 2011) | p |
|---|---|---|---|---|
| Age | 0.309 | |||
| ≤65 | 1902 (59.2) | 726 (60.3) | 1176 (58.5) | |
| >65 | 1313 (40.8) | 478 (39.7) | 835 (41.5) | |
| Sex | <0.001 | |||
| Male | 2271 (70.6) | 1002 (83.2) | 1269 (63.1) | |
| Female | 944 (29.4) | 202 (16.8) | 742 (36.9) | |
| Race | <0.001 | |||
| White | 2278 (70.9) | 1062 (88.2) | 1216 (60.5) | |
| Black | 377 (11.7) | 50 (4.2) | 327 (16.3) | |
| Other | 560 (17.4) | 92 (7.6) | 468 (23.3) | |
| Marital status | <0.001 | |||
| Married | 2097 (65.2) | 822 (68.3) | 1275 (63.4) | |
| Divorced/Separated | 313 (9.7) | 128 (10.6) | 185 (9.2) | |
| Single | 460 (14.3) | 166 (13.8) | 294 (14.6) | |
| Widowed | 204 (6.3) | 49 (4.1) | 155 (7.7) | |
| Unknown | 141 (4.4) | 39 (3.2) | 102 (5.1) | |
| Primary site | <0.001 | |||
| Cardiac/fundus | 1575 (49.0) | 1103 (91.6) | 472 (23.5) | |
| Body | 219 (6.8) | 15 (1.2) | 204 (10.1) | |
| Antrum/pylorus | 703 (21.9) | 16 (1.3) | 687 (34.2) | |
| Lesser/greater curvature | 356 (11.1) | 30 (2.5) | 326 (16.2) | |
| Other | 362 (11.3) | 40 (3.3) | 322 (16.0) | |
| Histology | <0.001 | |||
| Adenocarcinoma | 2896 (90.1) | 1151 (95.6) | 1745 (86.8) | |
| Other | 319 (9.9) | 53 (4.4) | 266 (13.2) | |
| TNM Stage | <0.001 | |||
| II | 1007 (31.3) | 391 (32.5) | 616 (30.6) | |
| III | 1908 (59.3) | 742 (61.6) | 1166 (58.0) | |
| IV | 300 (9.3) | 71 (5.9) | 229 (11.4) | |
| T stage | <0.001 | |||
| T1-2 | 478 (14.9) | 178 (14.8) | 300 (14.9) | |
| T3 | 1857 (57.8) | 926 (76.9) | 931 (46.3) | |
| T4 | 817 (25.4) | 95 (7.9) | 722 (35.9) | |
| Tx | 63 (2.0) | 5 (0.4) | 58 (2.9) | |
| N stage | <0.001 | |||
| N0 | 623 (19.4) | 284 (23.6) | 339 (16.9) | |
| N1 | 1105 (34.4) | 570 (47.3) | 535 (26.6) | |
| N2 | 773 (24.0) | 265 (22.0) | 508 (25.3) | |
| N3 | 714 (22.2) | 85 (7.1) | 629 (31.3) | |
| M stage | <0.001 | |||
| M0 | 2915 (90.7) | 1133 (94.1) | 1782 (88.6) | |
| M1 | 300 (9.3) | 71 (5.9) | 229 (11.4) | |
| Differentiation | <0.0001 | |||
| Poorly | 2041 (63.5) | 638 (53.0) | 1403 (69.8) | |
| Moderately | 783 (24.4) | 382 (31.7) | 401 (19.9) | |
| Well | 82 (2.6) | 43 (3.6) | 39 (1.9) | |
| Undifferentiated | 309 (9.6) | 141 (11.7) | 168 (8.4) | |
| Summary stage | 0.010 | |||
| Localized | 241 (7.5) | 108 (9.0) | 133 (6.6) | |
| Regional | 2490 (77.4) | 900 (74.8) | 1590 (79.1) | |
| Distant | 484 (15.1) | 196 (16.3) | 288 (14.3) | |
| Lauren type | <0.001 | |||
| Intestinal | 333 (10.4) | 60 (5.0) | 273 (13.6) | |
| Diffuse | 252 (7.8) | 28 (2.3) | 224 (11.1) | |
| Mixed | 100 (3.1) | 21 (1.7) | 79 (3.9) | |
| Unknown | 2530 (78.7) | 1095 (90.9) | 1435 (71.4) | |
| Tumor size | <0.001 | |||
| ≤3 cm | 726 (22.6) | 320 (26.6) | 406 (20.2) | |
| 3–5 cm | 919 (28.6) | 347 (28.8) | 572 (28.4) | |
| >5 cm | 1113 (34.6) | 288 (23.9) | 825 (41.0) | |
| Unknown | 457 (14.2) | 249 (20.7) | 208 (10.3) | |
| Bone metastases | <0.153 | |||
| Yes | 129 (4.0) | 56 (4.7) | 73 (3.6) | |
| No/Unknown | 3086 (96.0) | 1148 (95.3) | 1938 (96.4) | |
| Brain metastases | <0.001 | |||
| Yes | 39 (1.2) | 4 (0.3) | 35 (1.7) | |
| No/Unknown | 3176 (98.8) | 1200 (99.7) | 1976 (98.3) | |
| liver metastases | 0.142 | |||
| Yes | 72 (2.2) | 21 (1.7) | 51 (2.5) | |
| No/Unknown | 3143 (97.8) | 1183 (98.3) | 1960 (97.5) | |
| lung metastases | 0.820 | |||
| Yes | 31 (1.0) | 11 (0.9) | 20 (1.0) | |
| No/Unknown | 3184 (99.0) | 1193 (99.1) | 1991 (99.0) | |
| Chemotherapy | <0.001 | |||
| Yes | 3061 (95.2) | 1193 (99.1) | 1868 (92.9) | |
| No/Unknown | 154 (4.8) | 11 (0.9) | 143 (7.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Yu, Y.; Zheng, C.; Zhang, Y.; Shi, C.; Zhang, L.; Qiao, H. Dynamic Nomogram for Predicting Long-Term Survival in Terms of Preoperative and Postoperative Radiotherapy Benefits for Advanced Gastric Cancer. Int. J. Environ. Res. Public Health 2023, 20, 2747. https://doi.org/10.3390/ijerph20032747
Li X, Yu Y, Zheng C, Zhang Y, Shi C, Zhang L, Qiao H. Dynamic Nomogram for Predicting Long-Term Survival in Terms of Preoperative and Postoperative Radiotherapy Benefits for Advanced Gastric Cancer. International Journal of Environmental Research and Public Health. 2023; 20(3):2747. https://doi.org/10.3390/ijerph20032747
Chicago/Turabian StyleLi, Xinghui, Yang Yu, Cheng Zheng, Yue Zhang, Chuandao Shi, Lei Zhang, and Hui Qiao. 2023. "Dynamic Nomogram for Predicting Long-Term Survival in Terms of Preoperative and Postoperative Radiotherapy Benefits for Advanced Gastric Cancer" International Journal of Environmental Research and Public Health 20, no. 3: 2747. https://doi.org/10.3390/ijerph20032747