
Sleep Quality and Cognitive Function after Stroke: The Mediating Roles of Depression and Anxiety Symptoms

Abstract
:1. Introduction
2. Materials and Methods
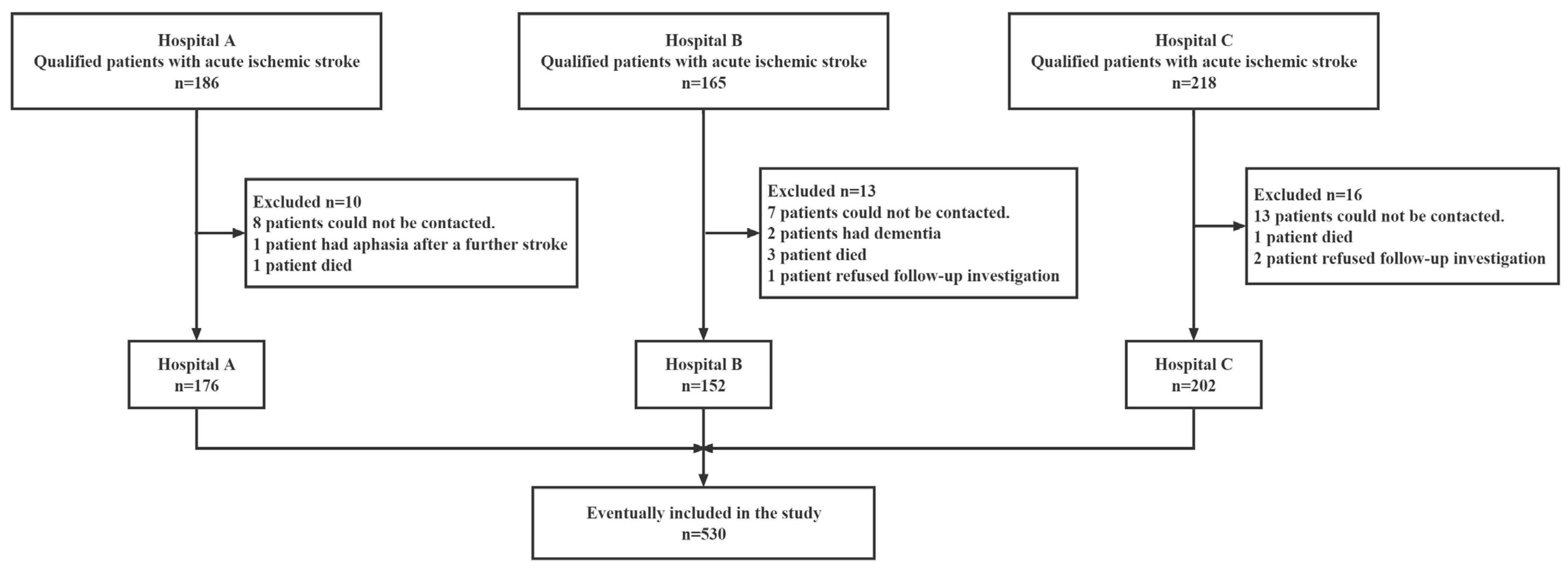
2.1. Subjects
- (1)
- transient ischemic attack (TIA) diagnosed by neurologists;
- (2)
- unable to give appropriate responses to the questions on the questionnaires (altered consciousness, confusion, or aphasia);
- (3)
- diagnosed with dementia of any type or another neurodegenerative or neurological condition.
2.2. Measures
2.2.1. Basic Information Collection and Functional Assessment
2.2.2. Assessment of Sleep Quality
2.2.3. Assessment of Cognitive Function
2.2.4. Assessment of Post-Stroke Anxiety and Depression
2.3. Data Analysis
2.4. Patient and Public Involvement
3. Results
3.1. Baseline Characteristics of Patients in the Two Sleep Quality Groups
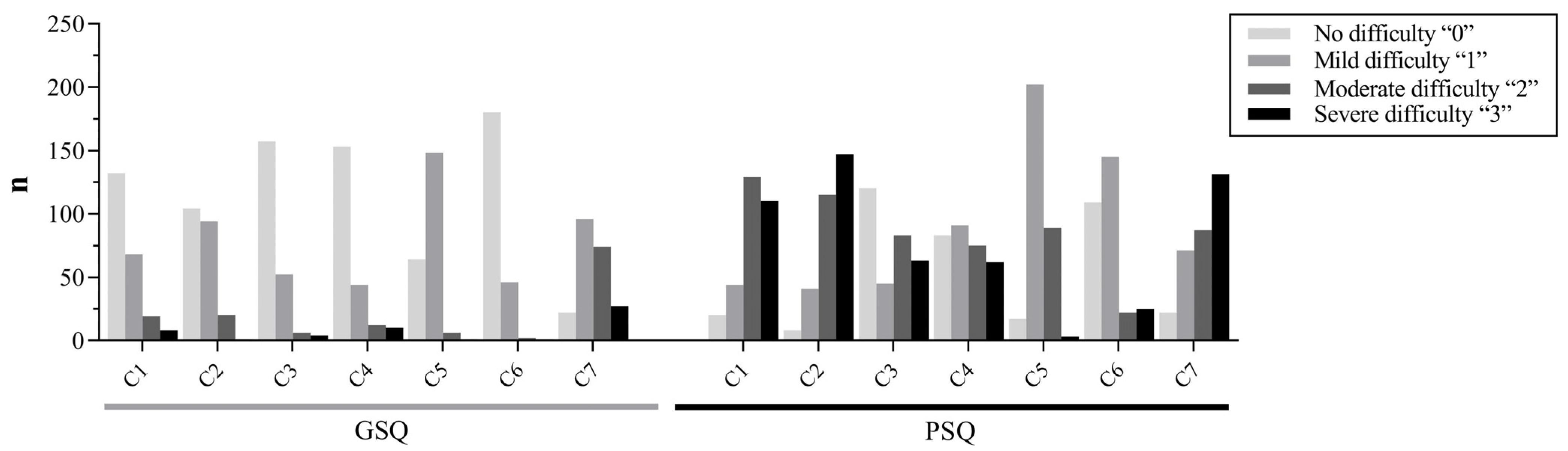
3.2. Assessment of Patients’ Sleep Condition
3.3. Association between Sleep Quality and Related Influencing Factors in Is Patients
3.4. The Mediation Role of Depression (SDS) between MoCA, SAS, and PSQI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sierra, C.; Coca, A.; Schiffrin, E.L. Vascular mechanisms in the pathogenesis of stroke. Curr. Hypertens. Rep. 2011, 13, 200–207. [Google Scholar] [CrossRef]
- Wang, Y.; Cui, L.; Ji, X.; Dong, Q.; Zeng, J.; Wang, Y.; Zhou, Y.; Zhao, X.; Wang, C.; Liu, L.; et al. The China National Stroke Registry for patients with acute cerebrovascular events: Design, rationale, and baseline patient characteristics. Int. J. Stroke 2011, 6, 355–361. [Google Scholar] [CrossRef]
- Wang, W.; Jiang, B.; Sun, H.; Ru, X.; Sun, D.; Wang, L.; Wang, L.; Jiang, Y.; Li, Y.; Wang, Y.; et al. Prevalence, incidence, and mortality of stroke in China: Results from a nationwide population-based survey of 480 687 adults. Circulation 2017, 135, 759–771. [Google Scholar] [CrossRef]
- Chinese Society of Neurology Cerebrovascular Group. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018. Chin. J. Neurol. 2018, 51, 662–683. [Google Scholar]
- Thrift, A.G.; Thayabaranathan, T.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.L.; Norrving, B.; Donnan, G.A.; Cadilhac, D.A. Global stroke statistics. Int. J. Stroke 2017, 12, 13–32. [Google Scholar] [CrossRef]
- Pasic, Z.; Smajlovic, D.; Dostovic, Z.; Kojic, B.; Selmanovic, S. Incidence and types of sleep disorders in patients with stroke. Med. Arh. 2011, 65, 225–227. [Google Scholar] [CrossRef] [Green Version]
- Al-Dughmi, M.; Al-Sharman, A.; Stevens, S.; Siengsukon, C.F. Sleep characteristics of individuals with chronic stroke: A pilot study. Nat. Sci. Sleep 2015, 7, 139–145. [Google Scholar]
- Joa, K.L.; Kim, W.H.; Choi, H.Y.; Park, C.H.; Kim, E.S.; Lee, S.J.; Kim, S.Y.; Ko, S.H.; Jung, H.Y. The effect of sleep disturbances on the functional recovery of rehabilitation inpatients following mild and moderate stroke. Am. J. Phys. Med. Rehab. 2017, 96, 734–740. [Google Scholar] [CrossRef]
- Kim, K.T.; Moom, H.J.; Yang, J.G.; Sohn, S.I.; Hong, J.H.; Cho, Y.W. The prevalence and clinical significance of sleep disorders in acute ischemic stroke patients-a questionnaire study. Sleep Breath. 2017, 21, 759–765. [Google Scholar] [CrossRef]
- Sahlin, C.; Sandberg, O.; Gustafson, Y.; Bucht, G.; Carlberg, B.; Stenlund, H.; Franklin, K.A. Obstructive sleep apnea is a risk factor for death in patients with stroke: A 10-year follow-up. Arch. Intern. Med. 2008, 168, 268–297. [Google Scholar] [CrossRef] [Green Version]
- Wallace, D.M.; Ramos, A.R.; Rundek, T. Sleep disorders and stroke. Int. J. Stroke 2012, 7, 231–242. [Google Scholar] [CrossRef] [Green Version]
- Raven, F.; Meerlo, P.; Havekes, R. The role of sleep in regulating structural plasticity and synaptic strength: Implications for memory and cognitive function. Sleep Med. Rev. 2018, 39, 3–11. [Google Scholar] [CrossRef]
- Dzierzewski, J.M.; Dautovich, N.; Ravyts, S. Sleep and cognition in older adults. Sleep Med. Clin. 2018, 13, 93–106. [Google Scholar] [CrossRef]
- Mattery, P.P.; Nelson, E.J. Sleep disturbances, obesity, and cognitive function in childhood: A mediation analysis. Curr. Dev. Nutr. 2021, 5, 119–126. [Google Scholar]
- Guan, Q.; Hu, X.; Ma, N.; He, H.; Duan, F.; Li, X.; Luo, Y.; Zhang, H. Sleep quality, depression, and cognitive function in non-demented older adults. J. Alzheimer’s Dis. 2020, 76, 1637–1650. [Google Scholar] [CrossRef]
- Xu, Y.; Wen, H.; Li, J.; Yang, J.; Luo, K.; Chang, L. The relationship between sleep disorders, anxiety, depression, and cognitive function with restless legs syndrome (RLS) in the elderly. Sleep Breath. 2022, 26, 1309–1318. [Google Scholar] [CrossRef]
- Mason, G.M.; Lokhandwala, S.; Riggins, T.; Spencer, R.M.C. Sleep and human cognitive development. Sleep Med. Rev. 2021, 57, 101472. [Google Scholar] [CrossRef]
- Quinn, T.J.; Dawson, J.; Walters, M.R.; Lees, K.R. Functional outcome measures in contemporary stroke trials. Int. J. Stroke 2010, 4, 200–205. [Google Scholar] [CrossRef]
- Quinn, T.J.; McArthur, K.; Ellis, G.; Stott, D.J. Functional assessment in older people. BMJ Clin. Res. 2011, 343, d4681. [Google Scholar] [CrossRef] [Green Version]
- Quinn, T.J.; Langhorne, P.; Stott, D.J. Barthel index for stroke trials: Development, properties, and application. Stroke 2011, 42, 1146–1151. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.C.; Tang, M.Q. Reliability and validity of the Pittsburgh sleep quality index. Chin. J. Psychiatry 1996, 2, 103–107. [Google Scholar]
- Zhai, S.; Tao, S.; Wu, X.; Zou, L.; Yang, Y.; Xie, Y.; Li, T.; Zhang, D.; Qu, Y.; Tao, F. Associations of sleep insufficiency and chronotype with inflammatory cytokines in college students. Nat. Sci. Sleep 2021, 13, 1675–1685. [Google Scholar] [CrossRef]
- Ren, Z.; Xin, Y.; Wang, Z.; Liu, D.; Ho, R.C.M.; Ho, C.S.H. What factors are most closely associated with mood disorders in adolescents during the COVID-19 pandemic? A cross-sectional study based on 1,771 adolescents in Shandong Province, China. Front. Psychiatry 2021, 12, 728278. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Ji, X.; Zhou, W.; Liu, J. Sleep problems in shift nurses: A brief review and recommendations at both individual and institutional levels. J. Nurs. Manag. 2019, 27, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Qin, K.; Zou, C.; Wang, H.H.; Lu, C.; Chen, W.; Guo, V.Y. The association of nighttime sleep duration and quality with chronic kidney disease in middle-aged and older Chinese: A cohort study. Sleep Med. 2021, 86, 25–31. [Google Scholar] [CrossRef]
- Li, Y.L.; Qiu, D.; Hu, C.; Ouyang, F.Y.; He, J.; Zang, D.F.; Luo, D.; Xiao, S.Y. Stressful life events and poor sleep quality: A cross-sectional survey in the Chinese governmental employees. Sleep Med. 2021, 85, 123–130. [Google Scholar] [CrossRef]
- Wen, H.; Zhang, Z.; Niu, F.; Li, L. The application of Montreal cognitive assessment in urban Chinese residents of Beijing. J. Gen. Intern. Med. 2008, 47, 36–39. [Google Scholar]
- Razali, R.; Jean-Li, L.; Jaffar, A.; Ahmad, M.; Shah, S.A.; Ibrahim, N.; Din, N.C.; Nik Jaafar, N.R.; Midin, M.; Sidi, H.; et al. Is the Bahasa Malaysia version of the Montreal Cognitive Assessment (MoCA-BM) a better instrument than the Malay version of the Mini Mental State Examination (M-MMSE) in screening for mild cognitive impairment (MCI) in the elderly? Compr. Psychiatry 2014, 55, 70–75. [Google Scholar] [CrossRef]
- Zung, W.W.; Coppedge, H.M. The Evaluation of Depressive Symptomatology. A Triadic Approach. Psychother. Psychosom. 1974, 24, 170–174. [Google Scholar] [CrossRef]
- Chen, X.; Bi, H.; Zhang, M.; Liu, H.; Wang, X.; Zu, R. Research of Sleep Disorders in Patients with Acute Cerebral Infarction. J. Stroke Cerebrovasc. Dis. 2015, 24, 2508–2513. [Google Scholar] [CrossRef]
- Sterr, A.; Herron, K.; Dijk, D.J.; Ellis, J. Time to wake-up: Sleep problems and daytime sleepiness in long-term stroke survivors. Brain Inj. 2008, 22, 575–579. [Google Scholar] [CrossRef] [Green Version]
- Alfinito, P.D.; Chen, X.; Mastroeni, R.; Pawlyk, A.C.; Deecher, D.C. Estradiol increases catecholamine levels in the hypothalamus of ovariectomized rats during the dark-phase. Eur. J. Pharmacol. 2009, 616, 334–339. [Google Scholar] [CrossRef]
- Gervais, N.J.; Mong, J.A.; Lacreuse, A. Ovarian hormones, sleep and cognition across the adult female lifespan: An integrated perspective. Front Neuroendocrin. 2017, 47, 134–153. [Google Scholar] [CrossRef]
- Khazaei, S.; Ayubi, E.; Khazaei, M. Sleep quality and related determinants among stroke patients: A cross-sectional study. Iran. J. Psychiatry 2022, 17, 84–90. [Google Scholar] [CrossRef]
- Yaffe, K.; Blackwell, T.; Barnes, D.E.; Ancoli-Israel, S.; Stone, K.L. Preclinical cognitive decline and subsequent sleep disturbance in older women. Neurology 2007, 69, 237–242. [Google Scholar] [CrossRef]
- Lowe, C.J.; Safati, A.; Hall, P.A. The neurocognitive consequences of sleep restriction: A meta-analytic review. Neurosci. Biobehav. R. 2017, 80, 586–604. [Google Scholar] [CrossRef]
- Killgore, W.D. Effects of sleep deprivation on cognition. Prog. Brain Res. 2010, 185, 105–129. [Google Scholar]
- Gerstner, J.R.; Yin, J.C. Circadian rhythms and memory formation. Nat. Rev. Neurosci. 2010, 11, 577–588. [Google Scholar] [CrossRef]
- Guarnieri, B.; Sorbi, S. Sleep and cognitive decline: A strong bidirectional relationship. It is time for specific recommendations on routine assess-ment and the management of sleep disorders in patients with mild cognitive impairment and dementia. Eur. Neurol. 2015, 74, 43–48. [Google Scholar] [CrossRef]
- Karaca, B. Factors Affecting Poststroke Sleep Disorders. J. Stroke Cerebrovasc. Dis. 2016, 25, 727–732. [Google Scholar] [CrossRef]
- Saper, C.B.; Scammell, T.E.; Lu, J. Hypothalamic regulation of sleep and circadian rhythms. Nature 2005, 437, 1257–1263. [Google Scholar] [CrossRef]
- Drake, C.L.; Pillai, V.; Roth, T. Stress and sleep reactivity: A prospective investigation of the stress-diathesis model of insomnia. Sleep 2014, 37, 1295–1304. [Google Scholar] [CrossRef] [Green Version]
- Hackett, M.L.; Pickles, K. Part I: Frequency of depression after stroke: An updated systematic review and meta-analysis of observational studies. Int. J. Stroke 2014, 9, 1017–1125. [Google Scholar] [CrossRef]
- Sonmez, I.; Karasel, S. Poor sleep quality i related to impaired functional status following stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 104349. [Google Scholar] [CrossRef]
- Davis, J.C.; Falck, R.S.; Best, J.R.; Chan, P.; Doherty, S.; Liu-Ambrose, T. Examining the Inter-relations of Depression, Physical Function, and Cognition with Subjective Sleep Parameters among Stroke Survivors: A Cross-sectional Analysis. J. Stroke Cerebrovasc. Dis. 2019, 28, 2115–2123. [Google Scholar] [CrossRef]
- Srivastava, A.; Taly, A.B.; Gupta, A.; Murali, T. Post-stroke depression: Prevalence and relationship with disability in chronic stroke survivors. Ann. Indian Acad. Neur. 2010, 13, 123–127. [Google Scholar] [CrossRef]
- Kutlubaev, M.A.; Hackett, M.L. Part II: Predictors of depression after stroke and impact of depression on stroke outcome: An updated systematic review of observational studies. Int. J. Stroke 2014, 9, 1026–1036. [Google Scholar] [CrossRef]
- Van Someren, E. Brain mechanisms of insomnia: New perspectives on causes and consequences. Physiol. Rev. 2021, 101, 995–1046. [Google Scholar] [CrossRef] [PubMed]
- McKinley, J.; McCarthy, A.; Lynch, T. Don’t lose sleep over neurodegeneration-it helps clear amyloid Beta. Front. Neurol. 2013, 4, 206. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Good Sleep Quality (n = 219) | Poor Sleep Quality (n = 311) | Statistics | p |
|---|---|---|---|---|
| Age | 62.15 ± 10.63 | 64.31 ± 9.99 | 5.706 | 0.017 |
| BMI | 24.06 ± 2.96 | 24.52 ± 2.96 | 3.132 | 0.077 |
| Sex, n (%) | ||||
| Male | 172 (78.5) | 205 (65.9) | 9.971 | 0.002 |
| Female | 47 (21.5) | 106 (34.1) | ||
| Marriage, n (%) | ||||
| Married | 200 (91.3) | 279 (89.7) | 0.385 | 0.535 |
| Unmarried/divorced/Widowed | 19 (8.7) | 32 (10.3) | ||
| Education years, n (%) | ||||
| Under primary school (≤6) | 17 (7.8) | 41 (13.2) | 5.368 | 0.147 |
| Primary school (7–9) | 86 (39.3) | 130 (41.8) | ||
| High school (10–12) | 60 (27.4) | 74 (23.8) | ||
| University and above (≥13) | 56 (25.6) | 66 (21.2) | ||
| Working status, n (%) | ||||
| Employed | 62 (28.3) | 83 (26.7) | 0.170 | 0.680 |
| Retired | 157 (71.7) | 228 (73.3) | ||
| Medical insurance, n (%) | ||||
| Yes | 191 (87.2) | 276 (88.7) | 0.288 | 0.592 |
| No | 28 (12.8) | 35 (11.3) | ||
| Vascular risk factors, n (%) | ||||
| Drink | 77 (35.2) | 140 (45.0) | 5.163 | 0.023 |
| Smoke | 73 (33.3) | 131 (42.1) | 4.193 | 0.041 |
| Hypertension | 120 (54.8) | 205 (65.9) | 6.702 | 0.010 |
| Diabetes | 87 (39.7) | 154 (49.5) | 4.969 | 0.026 |
| Coronary heart disease | 26 (11.9) | 38 (12.2) | 0.015 | 0.904 |
| Atrial fibrillation | 12 (5.5) | 15 (4.8) | 0.114 | 0.735 |
| Hyperlipidemia | 45 (20.5) | 66 (21.2) | 0.035 | 0.851 |
| Hyperuricemia | 13 (5.9) | 21 (6.8) | 0.143 | 0.706 |
| Thyroid disease | 17 (7.8) | 26 (8.4) | 0.062 | 0.804 |
| TIA history | 14 (6.4) | 28 (9.0) | 1.200 | 0.273 |
| NIHSS (M, IQR) | 3 (3) | 3 (3) | −0.313 | 0.754 |
| BI (M, IQR) | 55 (30) | 55 (25) | −0.479 | 0.632 |
| SAS | 32.50 ± 6.25 | 35.26 ± 8.34 | 17.208 | *** |
| SDS | 36.14 ± 7.53 | 43.29 ± 11.51 | 64.778 | *** |
| MoCA (M, IQR) | 22 (5) | 21 (8) | −4.901 | *** |
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | ||||
|---|---|---|---|---|---|---|---|---|
| β | SE | β | SE | β | SE | β | SE | |
| Constant | 6.873 *** | 1.271 | 5.615 *** | 1.457 | 9.300 *** | 1.569 | 6.519 *** | 1.647 |
| Age | 0.055 *** | 0.016 | 0.054 *** | 0.016 | 0.036 * | 0.016 | 0.015 | 0.014 |
| Sex | −1.335 *** | 0.361 | −1.321 *** | 0.258 | −1.249 *** | 0.350 | −0.775 * | 0.308 |
| Marriage | −0.604 | 0.551 | −0.629 | 0.545 | −0.381 | 0.535 | −0.507 | 0.468 |
| EDU | −0.065 | 0.171 | −0.037 | 0.169 | 0.321 | 0.174 | 0.113 | 0.153 |
| BMI | 0.125 | 0.176 | 0.136 | 0.174 | 0.234 | 0.174 | 0.121 | 0.154 |
| Work | −0.170 | 0.119 | −0.186 | 0.119 | 0.125 | 0.146 | 0.027 | 0.128 |
| Insurance | 0.067 | 0.188 | 0.141 | 0.187 | 0.159 | 0.199 | 0.128 | 0.245 |
| NIHSS | 0.258 | 0.071 | 0.219 ** | 0.070 | 0.101 | 0.062 | ||
| BI | −0.249 * | 0.103 | −0.260 * | 0.102 | −0.120 | 0.106 | ||
| MoCA | −0.204 *** | 0.040 | −0.111 ** | 0.037 | ||||
| SAS | 0.087 *** | 0.018 | ||||||
| SDS | 0.167 *** | 0.015 | ||||||
| R2 | 0.056 | 0.079 | 0.123 | 0.333 | ||||
| Adj R2 | 0.049 | 0.069 | 0.111 | 0.322 | ||||
| ΔR2 | 0.023 | 0.044 | 0.210 | |||||
| ΔF | 7.765 *** | 6.710 *** | 25.939 *** | 81.969 *** | ||||
| Items | Estimate | S.E. | t | p | Standardized Estimate |
|---|---|---|---|---|---|
| SDS←MoCA | 0.918 | 0.092 | −9.973 | *** | −0.395 |
| SDS←SAS | 0.152 | 0.055 | 2.758 | 0.006 | −0.109 |
| PSQI←MoCA | −0.080 | 0.033 | −2.438 | 0.015 | −0.097 |
| PSQI←SDS | 0.161 | 0.014 | 11.241 | *** | 0.449 |
| PSQI←SAS | 0.093 | 0.018 | 5.066 | *** | 0.186 |
| Items | β | S.E. | 95%CI | p | Variance (%) |
|---|---|---|---|---|---|
| Total effect | - | ||||
| PSQI←MoCA | −0.274 | 0.036 | (−0.334, −0.215) | *** | - |
| PSQI←SAS | 0.235 | 0.040 | (0.165, 0.297) | *** | - |
| Direct effect | - | ||||
| PSQI←MoCA | −0.097 | 0.038 | (−0.160, −0.034) | *** | 35.4 a |
| PSQI←SAS | 0.186 | 0.037 | (0.120, 0.245) | 0.015 | 79.1 b |
| Indirect effect | - | ||||
| PSQI←SDS←MoCA | −0.177 | 0.023 | (−0.214, −0.139) | *** | 64.6 a |
| PSQI←SDS←SAS | 0.049 | 0.017 | (0.021, 0.079) | 0.004 | 20.9 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niu, S.; Liu, X.; Wu, Q.; Ma, J.; Wu, S.; Zeng, L.; Shi, Y. Sleep Quality and Cognitive Function after Stroke: The Mediating Roles of Depression and Anxiety Symptoms. Int. J. Environ. Res. Public Health 2023, 20, 2410. https://doi.org/10.3390/ijerph20032410
Niu S, Liu X, Wu Q, Ma J, Wu S, Zeng L, Shi Y. Sleep Quality and Cognitive Function after Stroke: The Mediating Roles of Depression and Anxiety Symptoms. International Journal of Environmental Research and Public Health. 2023; 20(3):2410. https://doi.org/10.3390/ijerph20032410
Chicago/Turabian StyleNiu, Shuzhen, Xianliang Liu, Qian Wu, Jiajia Ma, Songqi Wu, Li Zeng, and Yan Shi. 2023. "Sleep Quality and Cognitive Function after Stroke: The Mediating Roles of Depression and Anxiety Symptoms" International Journal of Environmental Research and Public Health 20, no. 3: 2410. https://doi.org/10.3390/ijerph20032410