
Increasing Physical Activity at School Improves Physical Fitness of Early Adolescents



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Procedure
2.4. Measurements
2.4.1. Anthropometric Measurements
2.4.2. Eurofit Tests
2.5. Statistical Analysis
3. Results
3.1. Description of the Group
3.2. Eurofit Tests
3.2.1. Core Strength
3.2.2. Long Jump
3.2.3. Shuttle Run 10 × 5 m
3.3. Averaged Results
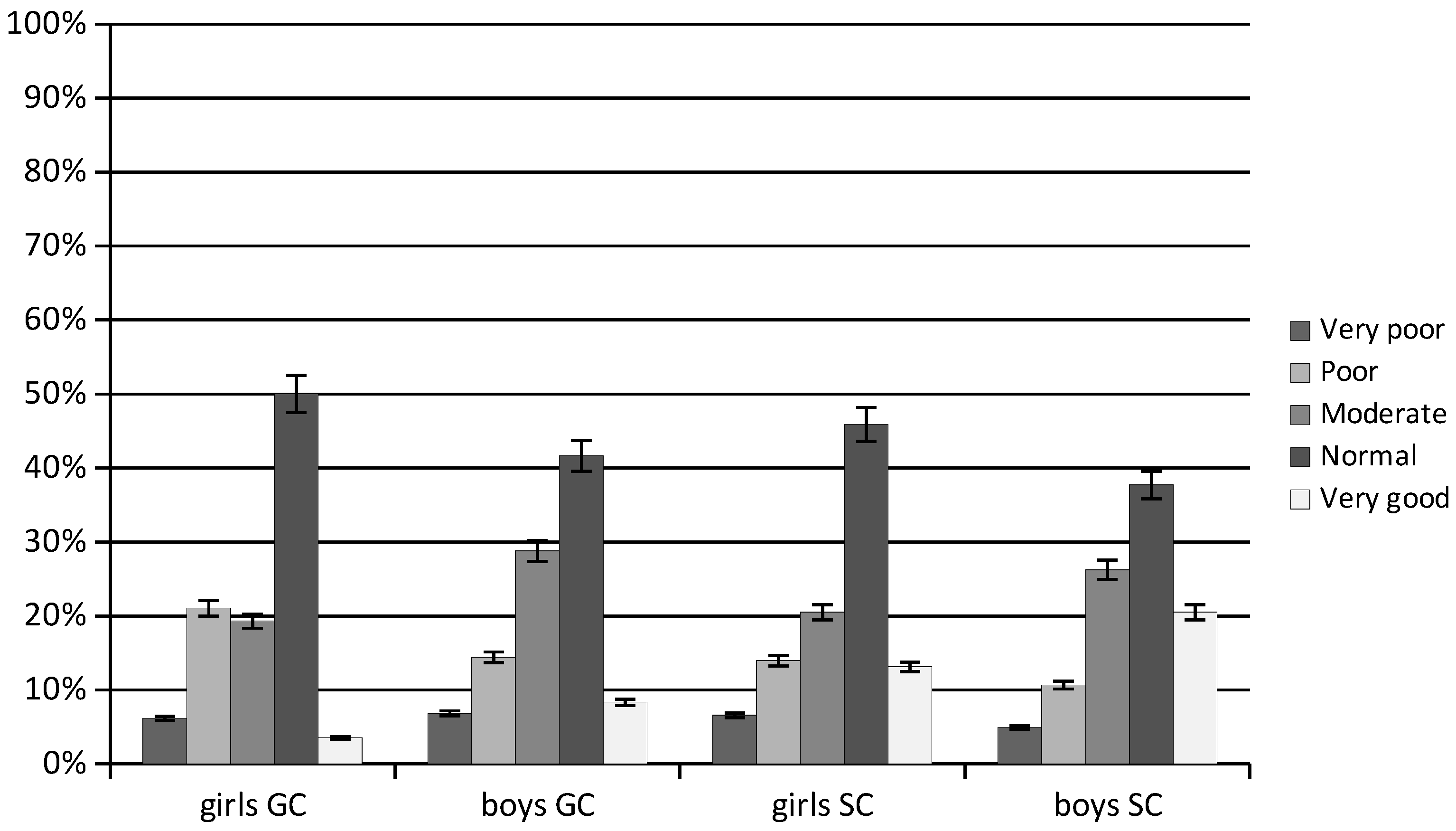
3.4. General Physical Fitness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oja, L.; Piksööt, J. Physical Activity and Sports Participation among Adolescents: Associations with Sports-Related Knowledge and Attitudes. Int. J. Environ. Res. Public Health 2022, 19, 6235. [Google Scholar] [CrossRef]
- Kolb, S.; Burchartz, A.; Oriwol, D.; Schmidt, S.C.E.; Woll, A.; Niessner, C. Indicators to Assess Physical Health of Children and Adolescents in Activity Research-A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 10711. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2007, 32, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020.
- Landry, B.W.; Driscoll, S.W. Physical activity in children and adolescents. PM R 2012, 4, 826–832. [Google Scholar] [CrossRef]
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; Department of Health and Human Services: Washington, DC, USA, 2018.
- Patton, G.C.; Sawyer, S.M.; Santelli, J.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Our future: A Lancet commission on adolescent health and wellbeing. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!): Guidance to Support Country Implementation; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- The Lancet. Join the Lancet 2020 Campaign on child and adolescent health. Lancet 2020, 395, 89. [Google Scholar] [CrossRef]
- Tremblay, M.; Barnes, J.D.; González, S.; Katzmarzyk, P.T.; Onywera, V.O.; Reilly, J.J.; Tomkinson, G.R. Global Matrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act. Health 2016, 13, S343–S366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ługowska, K.; Kolanowski, W.; Trafialek, J. Eating Behaviour and Physical Fitness in 10-Year-Old Children Attending General Education and Sports Classes. Int. J. Environ. Res. Public Health 2020, 17, 6467. [Google Scholar] [CrossRef] [PubMed]
- Kolanowski, W.; Ługowska, K.; Trafialek, J. Increased Physical Activity at School Benefits Arterial Blood Pressure in Children—A Prospective Follow-Up Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 4662. [Google Scholar] [CrossRef]
- Ługowska, K.; Kolanowski, W.; Trafialek, J. The Impact of Physical Activity at School on Children’s Body Mass during 2 Years of Observation. Int. J. Environ. Res. Public Health 2022, 19, 3287. [Google Scholar] [CrossRef]
- Gea-García, G.M.; González-Gálvez, N.; Espeso-García, A.; Marcos-Pardo, P.J.; González-Fernández, F.T.; Martínez-Aranda, L.M. Relationship Between the Practice of Physical Activity and Physical Fitness in Physical Education Students: The Integrated Regulation As a Mediating Variable. Front. Psychol. 2020, 11, 1910. [Google Scholar] [CrossRef]
- Sember, V.; Jurak, G.; Kovac, M.; Durić, S.; Starc, G. Decline of physical activity in early adolescence: A 3-year cohort study. PLoS ONE 2020, 15, e0229305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buja, A.; Grotto, G.; Brocadello, F.; Sperotto, M.; Baldo, V. Primary school children and nutrition: Lifestyles and behavioral traits associated with a poor-to-moderate adherence to the Mediterranean diet. A cross-sectional study. Eur. J. Pediatr. 2020, 179, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Clavel, I.; Gallardo, L.; Garcia-Unanue, J. Relationship between Adherence to the Mediterranean Diet and Body Composition with Physical Fitness Parameters in a Young Active Population. Int. J. Environ. Res. Public Health 2020, 17, 3337. [Google Scholar] [CrossRef]
- Drygas, W.; Gajewska, M.; Zdrojewski, T. Niedostateczny Poziom Aktywności Fizycznej w Polsce Jako Zagrożenie i Wyzwanie dla Zdrowia Publicznego—Raport Komitetu Zdrowia Publicznego Polskiej Akademii Nauk; Narodowy Instytut Zdrowia Publicznego—PZH: Warszawa, Poland, 2021; pp. 69–90. [Google Scholar]
- Woynarowska, B.; Mazur, J.; Oblacińska, A. Uczestnictwo uczniów w lekcjach wychowania fizycznego w szkołach w Polsce. Probl. Hig. Epidemiol. 2015, 50, 183–190. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Maszczak, T. Kondycja fizyczna młodzieży szkolnej w świetle badań populacyjnych. Akad. Aktywność Fiz. I Zdr. 2017, 12, 63–68. [Google Scholar]
- Mazur, J.; Małkowska-Szkutnik, A. Zdrowie Uczniów w 2018 Roku Na Tle Nowego Modelu Badań HBSC; Instytut Matki I Dziecka: Warszawa, Poland, 2018. [Google Scholar]
- Messing, S.; Rütten, A.; Abu-Omar, K.; Ungerer-Röhrich, U.; Goodwin, L.; Burlacu, I.; Gediga, G. How Can Physical Activity Be Promoted Among Children and Adolescents? A Systematic Review of Reviews Across Settings. Front. Public Health 2019, 7, 55. [Google Scholar] [CrossRef] [Green Version]
- Zembura, P.; Korcz, A.; Cieśla, E.; Gołdys, A.; Nałęcz, H. Results from Poland’s 2018 Report Card on Physical Activity for Children and Youth. J. Phys. Act. Health 2018, 15, S395–S397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zembura, P.; Korcz, A.; Nałęcz, H.; Cieśla, E. Results from Poland’s 2022 Report Card on Physical Activity for Children and Youth. Int. J. Environ. Res. Public Health 2022, 19, 4276. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Cvejic, D.; Pejovic, T.; Ostojic, S. Assessment of physical fitness in children and adolescents. Phys. Educ. Sport 2013, 11, 135–145. [Google Scholar]
- Bruggeman, B.S.; Vincent, H.K.; Chi, X.; Filipp, S.L.; Mercado, R.; Modave, F.; Guo, Y.; Gurka, M.J.; Bernier, A. Simple tests of cardiorespiratory fitness in a pediatric population. PLoS ONE 2020, 15, e0238863. [Google Scholar] [CrossRef] [PubMed]
- Pluim, C.; Gard, M. Physical education’s grand convergence: Fitnessgram, big-data and the digital commerce of children’s health. Crit. Stud. Educ. 2018, 3, 261–278. [Google Scholar] [CrossRef]
- Mekota, K.; Kovar, R. Unifittest (6–60): Test and Norms of Motor Performance and Physical Fitness in Youth and in Adult Age; Palacký University: Olomouc, Czech Republic, 1995. [Google Scholar]
- Council of Europe. Eurofit: Handbook for the Eurofit Tests of Physical Fitness; Council of Europe: Rome, Italy, 1988.
- Kemper, H.C.; Van Mechelen, W. Physical Fitness Testing of Children: A European Perspective. Pediatr. Exerc. Sci. 1996, 8, 201–214. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Olds, T.S.; Borms, J. Who are the Eurofittest? Med. Sport Sci. 2007, 50, 104–128. [Google Scholar]
- Lang, J.J.; Tremblay, M.S.; Ortega, F.B.; Ruiz, J.R.; Tomkinson, G.R. Review of criterion-referenced standards for cardiorespiratory fitness: What percentage of 1 142 026 international children and youth are apparently healthy? Br. J. Sports Med. 2017, 53, 953–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsigilis, N.; Douda, H.; Tokmakidis, S.P. Test-retest reliability of the Eurofit test battery administered to university students. Percept. Mot. Skills 2002, 95, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Tomkinson, G.R.; Carver, K.D.; Atkinson, F.; Daniell, N.D.; Lewis, L.K.; Fitzgerald, J.S.; Lang, J.J.; Ortega, F.B. European normative values for physical fitness in children and adolescents aged 9–17 years: Results from 2 779 165 Eurofit performances representing 30 countries. Br. J. Sports Med. 2018, 52, 1445–1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO European Regional Obesity Report 2022; WHO Regional Office for Europe: Copenhagen, Denmark, 2022.
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S.; Dale, M.; Leblanc, A.G.; Belanger, K.; Ortega, F.B.; Léger, L. International normative 20 m shuttle run values from 1 142 026 children and youth representing 50 countries. Br. J. Sports Med. 2016, 51, 1545–1554. [Google Scholar] [CrossRef] [Green Version]
- Lisinskiene, A.; Lochbaum, M. The Coach-Athlete-Parent Relationship: The Importance of the Sex, Sport Type, and Family Composition. Int. J. Environ. Res. Public Health 2022, 19, 4821. [Google Scholar] [CrossRef]
- Jarnig, G.; Jaunig, J.; Kerbl, R.; Lima, R.A.; van Poppel, M.N.M. A Novel Monitoring System (AUT FIT) for Anthropometrics and Physical Fitness in Primary School Children in Austria: A Cross-Sectional Pilot Study. Sports 2021, 10, 4. [Google Scholar] [CrossRef]
- Ługowska, K.; Kolanowski, W. The Impact of Physical Activity at School on Body Fat Content in School-Aged Children. Int. J. Environ. Res. Public Health 2022, 19, 12514. [Google Scholar] [CrossRef]
- Microsoft Excel. Available online: https://www.microsoft.com/pl-pl/microsoft-365/excel (accessed on 4 March 2022).
- StatSoft. Electronic Statistics Textbook. Kraków, 2006. Available online: https://www.statsoft.pl/textbook/stathome.html (accessed on 4 March 2022).
- Sullivan, G.M.; Feinn, R. Using Effect Size—Or Why the p Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, J.; Marques, A.; Gouveia, É.R.; Carvalho, F.; Sarmento, H.; Valeiro, M.G. Participation in Physical Education Classes and Health-Related Behaviours among Adolescents from 67 Countries. Int. J. Environ. Res. Public Health 2022, 19, 955. [Google Scholar] [CrossRef] [PubMed]
- Puchalska-Sarna, A.; Baran, R.; Kustra, M.; Pop, T.; Herbert, J.; Baran, J. The Level and Factors Differentiating the Physical Fitness of Adolescents Passively and Actively Resting in South-Eastern Poland-A Pilot Study. Children 2022, 9, 1341. [Google Scholar] [CrossRef] [PubMed]
- Abdelkarim, O.; Ammar, A.; Trabelsi, K.; Cthourou, H.; Jekauc, D.; Irandoust, K.; Taheri, M.; Bös, K.; Woll, A.; Bragazzi, N.L.; et al. Prevalence of Underweight and Overweight and Its Association with Physical Fitness in Egyptian Schoolchildren. Int. J. Environ. Res. Public Health 2019, 17, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierra-Diaz, M.J.; González-Víllora, S.; Pastor-Vicedo, J.C.; López-Sánchez, G.F. Can we motivate students to practice physical activities and sports through models-based practice? A systematic review and meta-analysis of psychosocial factors related to physical education. Front. Psychol. 2019, 10, 2115. [Google Scholar]
- Fiori, F.; Bravo, G.; Parpinel, M.; Messina, G.; Malavolta, R.; Lazzer, S. Relationship between body mass index and physical fitness in Italian prepubertal schoolchildren. PLoS ONE 2020, 15, e0233362. [Google Scholar] [CrossRef]
- Palou, P.; Muntaner-Mas, A.; Cantallops, J.; Borràs, P.A.; Labayen, I.; Jiménez-Pavón, D.; García, C.D.; Moliner-Urdiales, D.; Pérez, M.A.R.; Rojo-Tirado, M.A.; et al. A Single Question of Parent-Reported Physical Activity Levels Estimates Objectively Measured Physical Fitness and Body Composition in Preschool Children: The PREFIT Project. Front. Psychol. 2019, 10, 1585. [Google Scholar] [CrossRef]
- Weedon, B.D.; Liu, F.; Mahmoud, W.; Burden, S.J.; Whaymand, L.; Esser, P.; Collett, J.; Izadi, H.; Joshi, S.; Meaney, A.; et al. Declining fitness and physical education lessons in UK adolescents. BMJ Open Sport Exerc. Med. 2022, 8, e001165. [Google Scholar] [CrossRef]
- Handelsman, D.J.; Hirschberg, A.L.; Bermon, S. Circulating Testosterone as the Hormonal Basis of Sex Differences in Athletic Performance. Endocr. Rev. 2018, 39, 803–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Negro, J.; Huertas-Delgado, F.J.; Yanci, J. Motor skills differences by gender in early elementary education students. Early Child Dev. Care 2021, 191, 281–291. [Google Scholar] [CrossRef]
- Malina, R.M.; Bouchard, C. Growth, Maturation, and Physical Activity; Human Kinetics Books: Champaign, IL, USA, 1991. [Google Scholar]
- Riddoch, C.J.; Andersen, L.B.; Wedderkopp, N.; Harro, M.; Klasson-Heggebø, L.; Sardinha, L.B.; Cooper, A.R.; Ekelund, U. Physical activity levels and patterns of 9- and 15-yr-old European children. Med. Sci. Sports Exerc. 2004, 36, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancini, A.; Martone, D.; Vitucci, D.; Capobianco, A.; Alfieri, A.; Buono, P.; Orrù, S. Influence of Sport Practice and Body Weight on Physical Fitness in Schoolchildren Living in the Campania Region. Int. J. Environ. Res. Public Health 2022, 19, 7412. [Google Scholar] [CrossRef] [PubMed]
- Vandoni, M.; Calcaterra, V.; Pellino, V.C.; De Silvestri, A.; Marin, L.; Zuccotti, G.V.; Tranfaglia, V.; Giuriato, M.; Codella, R.; Lovecchio, N. “Fitness and Fatness” in Children and Adolescents: An Italian Cross-Sectional Study. Children 2021, 8, 762. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.J.; Liao, C.D.; Tsai, M.W.; Chen, C.N. Effects of exercise and nutritional intervention on body composition, metabolic health, and physical performance in adults with sarcopenic obesity: A meta-analysis. Nutrients 2019, 11, 2163. [Google Scholar] [CrossRef] [Green Version]
- Ding, C.; Jiang, Y. The Relationship between Body Mass Index and Physical Fitness among Chinese University Students: Results of a Longitudinal Study. Healthcare 2020, 8, 570. [Google Scholar] [CrossRef]
- Morano, M.; Robazza, C.; Bortoli, L.; Rutigliano, I.; Ruiz, M.C.; Campanozzi, A. Physical Activity and Physical Competence in Overweight and Obese Children: An Intervention Study. Int. J. Environ. Res. Public Health 2020, 17, 6370. [Google Scholar] [CrossRef]
- Kwieciński, J.; Konarski, J.M.; Strzelczyk, R.; Krzykała, M.; Konarska, A.; Bartkowiak, S.; Lopes, V.; Malina, R.M. Non-linear relationships between the BMI and physical fitness in Polish adolescents. Ann. Hum. Biol. 2018, 45, 406–413. [Google Scholar] [CrossRef]
- Fransen, J.; Deprez, D.; Pion, J.; Tallir, I.B.; D’Hondt, E.; Vaeyens, R.; Lenoir, M.; Philippaerts, R.M. Changes in physical fitness and sports participation among children with different levels of motor competence: A 2-year longitudinal study. Pediatr. Exerc. Sci. 2014, 26, 11–21. [Google Scholar] [CrossRef]
- Korcz, A.; Monyeki, M.A. Association Between Sport Participation, Body Composition, Physical Fitness, and Social Correlates Among Adolescents: The PAHL Study. Int. J. Environ. Res. Public. Health 2018, 15, 2793. [Google Scholar]
- Dobosz, J.; Mayorga-Vega, D.; Viciana, J. Percentile values of physical fitness levels among polish children aged 7 to 19 years-a population-based study. Cent. Eur. J. Public Health 2015, 23, 340–351. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Bi, C.; Yin, X.; Chen, Q.; Li, Y.; Liu, Y.; Zhang, T.; Li, M.; Sun, Y.; Yang, X. Physical fitness reference standards for Chinese children and adolescents. Sci. Rep. 2021, 11, 4991. [Google Scholar] [CrossRef]
- Martinez-de-Quel, O.; Alegre, L.M.; Castillo-García, A.; Ayan, C. Anthropometric and fitness normative values for young karatekas. Biol. Sport 2021, 38, 351–357. [Google Scholar] [CrossRef]
- Ørntoft, C.; Larsen, M.N.; Madsen, M.; Sandager, L.; Lundager, I.; Møller, A.; Hansen, L.; Madsen, E.E.; Elbe, A.-M.; Ottesen, L.; et al. Physical Fitness and Body Composition in 10–12-Year-Old Danish Children in Relation to Leisure-Time Club-Based Sporting Activities. BioMed Res. Int. 2018, 2018, 9807569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riso, E.M.; Toplaan, L.; Viira, P.; Vaiksaar, S.; Jürimäe, J. Physical fitness and physical activity of 6-7-year-old children according to weight status and sports participation. PLoS ONE 2019, 14, e0218901. [Google Scholar] [CrossRef] [PubMed]
- Kolanowski, W.; Ługowska, K.; Trafialek, J. The Impact of Physical Activity at School on Eating Behaviour and Leisure Time of Early Adolescents. Int. J. Environ. Res. Public Health 2022, 19, 16490. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurement Session | Average Age (y/o) | Total Average (n/30 s) | Group | ESs | p * | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GC | SC | |||||||||||||||
| Average | Median | Min. | Max. | SD | 95% CI | Average | Median | Min. | Max. | SD | 95% CI | |||||
| Mean | ||||||||||||||||
| I | 10.90 | 18.67 | 18.00 | 19.00 | 2.00 | 24.00 | 3.53 | 3.14–4.04 | 19.35 | 20.00 | 9.00 | 27.00 | 3.86 | 3.42–4.41 | 0.250 | <0.001 |
| II | 11.90 | 20.62 | 19.90 | 21.00 | 4.00 | 26.00 | 3.50 | 3.11–4.00 | 21.34 | 22.00 | 13.00 | 29.00 | 3.67 | 3.26–4.20 | 0.614 | 0.010 |
| Girls | ||||||||||||||||
| I | 10.90 | 17.63 | 17.01 | 17.00 | 8.00 | 22.00 | 2.75 | 2.32–3.37 | 18.26 | 20.00 | 9.00 | 25.00 | 3.88 | 3.50–4.52 | 0.340 | 0.040 |
| II | 11.90 | 19.55 | 18.91 | 19.00 | 10.00 | 24.00 | 2.83 | 2.39–3.47 | 20.19 | 21.00 | 13.00 | 27.00 | 3.42 | 3.05–3.93 | 0.510 | 0.030 |
| Boys | ||||||||||||||||
| I | 10.90 | 19.70 | 18.96 | 20.00 | 2.00 | 24.00 | 3.88 | 3.31–4.69 | 20.44 | 22.00 | 12.00 | 27.00 | 3.53 | 3.00–4.30 | 0.560 | 0.020 |
| II | 11.90 | 21.68 | 20.87 | 22.00 | 4.00 | 26.00 | 3.78 | 3.23–4.56 | 22.50 | 23.00 | 14.00 | 29.00 | 3.48 | 2.95–4.24 | 0.240 | 0.060 |
| Measurement Session | Average Age (y/o) | Total Average (cm) | Group | ESs | p * | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GC | SC | |||||||||||||||
| Average | Median | Min. | Max. | SD | 95% CI | Average | Median | Min. | Max. | SD | 95% CI | |||||
| Mean | ||||||||||||||||
| I | 10.90 | 139.44 | 137.16 | 140.00 | 98.00 | 179.00 | 14.70 | 13.07–16.81 | 141.72 | 145.00 | 100.00 | 195.00 | 18.25 | 15.48–22.21 | 0.140 | 0.030 |
| II | 11.90 | 149.36 | 146.60 | 148.00 | 110.00 | 184.00 | 13.84 | 12.30–15.82 | 152.13 | 152.00 | 115.00 | 215.00 | 19.20 | 16.29–23.37 | 0.550 | 0.010 |
| Girls | ||||||||||||||||
| I | 10.90 | 134.14 | 132.17 | 137.00 | 100.00 | 156.00 | 12.86 | 10.86–15.78 | 136.11 | 140.00 | 100.00 | 165.00 | 13.81 | 11.72–16.81 | 0.170 | 0.110 |
| II | 11.90 | 143.36 | 141.38 | 145.00 | 115.00 | 161.00 | 11.29 | 9.53–13.85 | 145.34 | 147.00 | 115.00 | 193.00 | 14.90 | 12.64–18.14 | 0.541 | 0.200 |
| Boys | ||||||||||||||||
| I | 10.90 | 144.74 | 142.16 | 145.00 | 98.00 | 179.00 | 14.71 | 12.55–17.75 | 147.32 | 147.00 | 105.00 | 195.00 | 15.70 | 13.33–19.21 | 0.301 | 0.050 |
| II | 11.90 | 155.37 | 151.83 | 153.00 | 110.00 | 184.00 | 14.08 | 12.02–16.99 | 158.91 | 155.00 | 115.00 | 215.00 | 19.22 | 16.32–23.41 | 0.610 | 0.020 |
| Measurement Session | Average Age (y/o) | Total Average (sec.) | Group | ESs | p * | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GC | SC | |||||||||||||||
| Average | Median | Min. | Max. | SD | 95% CI | Average | Median | Min. | Max. | SD | 95% CI | |||||
| I | 10.90 | 22.37 | 22.58 | 21.88 | 19.05 | 32.00 | 1.83 | 1.63–2.09 | 22.16 | 21.82 | 18.30 | 29.03 | 1.79 | 1.59–2.04 | 0.235 | 0.090 |
| II | 11.90 | 21.26 | 21.56 | 21.05 | 18.73 | 28.99 | 1.75 | 1.55–2.00 | 20.96 | 20.90 | 18.01 | 28.02 | 1.67 | 1.48–1.91 | 0.621 | 0.024 |
| Girls | ||||||||||||||||
| I | 10.90 | 22.83 | 23.03 | 22.60 | 20.50 | 30.35 | 1.70 | 1.44–2.09 | 22.64 | 22.00 | 19.59 | 29.03 | 1.74 | 1.56–2.24 | 0.410 | 0.230 |
| II | 11.90 | 21.78 | 22.02 | 21.89 | 18.82 | 28.02 | 1.85 | 1.56–2.28 | 21.55 | 21.50 | 18.05 | 25.92 | 1.82 | 1.54–2.21 | 0.580 | 0.300 |
| Boys | ||||||||||||||||
| I | 10.90 | 21.90 | 22.13 | 21.74 | 19.05 | 32.00 | 1.91 | 1.58–2.23 | 21.68 | 21.60 | 18.30 | 24.98 | 1.60 | 1.36–1.95 | 0.371 | 0.140 |
| II | 11.90 | 20.73 | 21.10 | 20.73 | 18.73 | 28.99 | 1.54 | 1.31–1.86 | 20.36 | 20.65 | 18.01 | 24.16 | 1.42 | 1.20–1.73 | 0.617 | 0.390 |
| Eurofit Tests | Group | Average | Median | Min. | Max. | SD | 95% CI | p * | p ** |
|---|---|---|---|---|---|---|---|---|---|
| 10 × 5 m shuttle run (sec.) | SC | 21.72 | 21.50 | 18.01 | 29.03 | 1.78 | 1.64–1.96 | 0.024 | 0.631 |
| GC | 22.04 | 21.68 | 18.72 | 32.00 | 1.86 | 1.71–2.04 | |||
| standing long jump (cm) | SC | 146.92 | 147.00 | 100.00 | 215.00 | 17.89 | 16.43–19.64 | 0.001 | 0.148 |
| GC | 142.26 | 145.00 | 98.00 | 184.00 | 15.01 | 13.79–16.47 | |||
| sit-ups in 30 s (n/30 s) | SC | 20.25 | 21.00 | 9.00 | 29.00 | 3.86 | 3.55–4.24 | 0.003 | 0.064 |
| Variable | Class | Referenced | Average | Median | Min. | Max. | SD | 95% CI | p * | p ** |
|---|---|---|---|---|---|---|---|---|---|---|
| 10 × 5 m shuttle run (sec.) | Girls | ≥22.63 | 22.34 | 21.99 | 18.05 | 30.35 | 1.87 | 1.72–2.08 | 0.025 | 0.127 |
| Boys | ≥21.78 | 21.45 | 21.30 | 18.01 | 32.00 | 1.68 | 1.54–1.84 | |||
| standing long jump (cm) | Girls | ≥137.50 | 138.82 | 140.00 | 100.00 | 193.00 | 14.16 | 12.98–15.56 | <0.001 | 0.521 |
| Boys | ≥147.70 | 149.94 | 150.00 | 98.00 | 215.00 | 17.04 | 15.68–18.67 | |||
| sit-ups in 30 s (n/30 s) | Girls | ≥17 | 18.61 | 19.00 | 8.00 | 27.00 | 3.50 | 3.21–3.85 | <0.001 | 0.875 |
| Boys | ≥18 | 20.57 | 21.00 | 2.00 | 29.00 | 3.83 | 3.52–4.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ługowska, K.; Kolanowski, W.; Trafialek, J. Increasing Physical Activity at School Improves Physical Fitness of Early Adolescents. Int. J. Environ. Res. Public Health 2023, 20, 2348. https://doi.org/10.3390/ijerph20032348
Ługowska K, Kolanowski W, Trafialek J. Increasing Physical Activity at School Improves Physical Fitness of Early Adolescents. International Journal of Environmental Research and Public Health. 2023; 20(3):2348. https://doi.org/10.3390/ijerph20032348
Chicago/Turabian StyleŁugowska, Katarzyna, Wojciech Kolanowski, and Joanna Trafialek. 2023. "Increasing Physical Activity at School Improves Physical Fitness of Early Adolescents" International Journal of Environmental Research and Public Health 20, no. 3: 2348. https://doi.org/10.3390/ijerph20032348