
Relationships between Self-Efficacy and Post-Stroke Activity Limitations, Locomotor Ability, Physical Activity, and Community Reintegration in Sub-Saharan Africa: A Cross-Sectional Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Recruitment
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. Participants’ Recovery Profiles
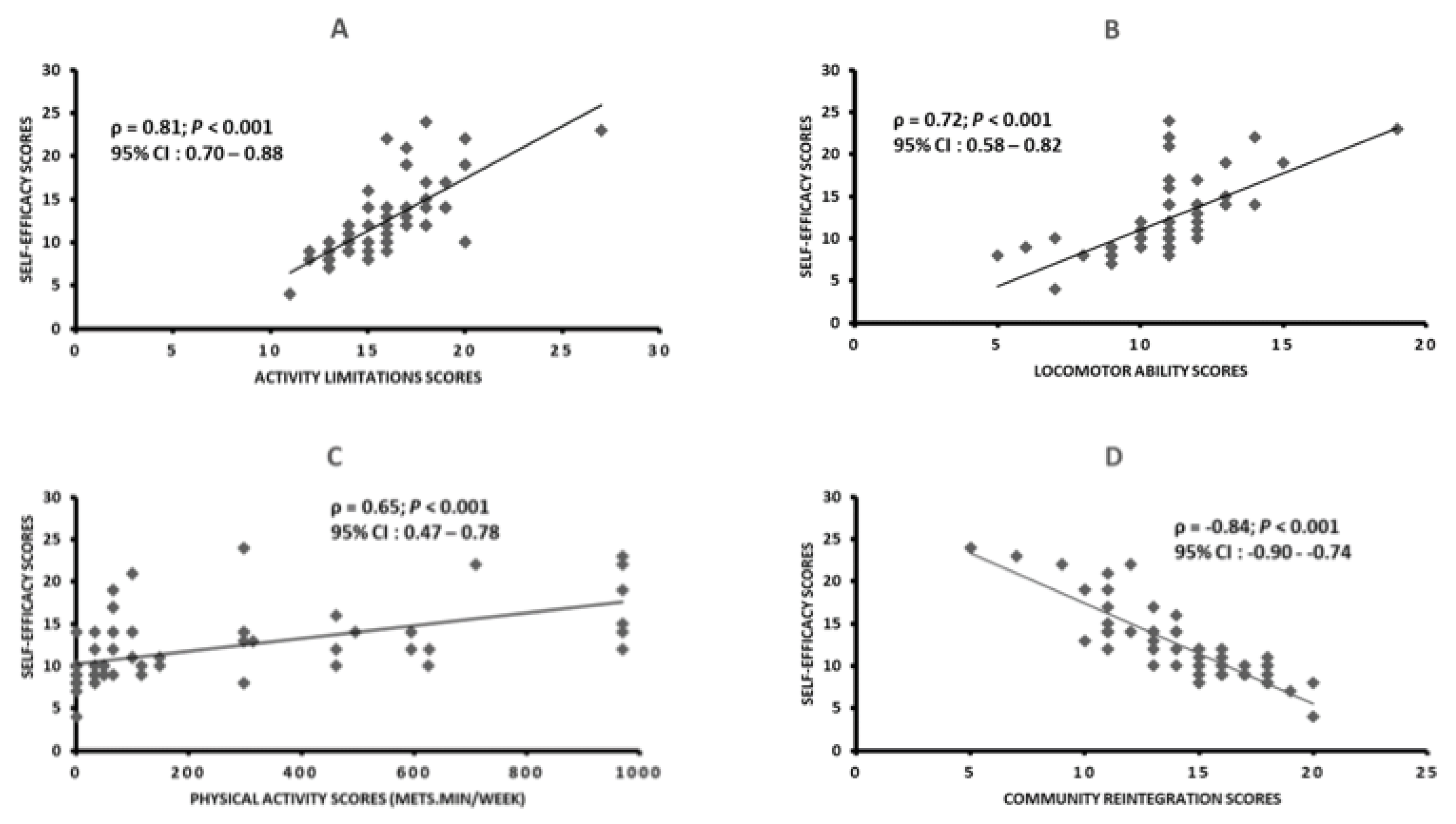
3.3. Relationships between Self-Efficacy and Activity Limitations, Locomotor Ability, Physical Activity, and Community Reintegration Scores in Stroke Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Stages | Assignments | Responsible People | Results Obtained |
|---|---|---|---|
| Stage 1: Initial translation. | Assignment: To translate the original English version of the SSEQ into Beninese French. | 02 people: -1 physiotherapist (PhD degree) [informed translator TR1] -1 linguist (Master’s degree) [naive or uninformed translator TR2]. | Production of two independent French versions of the SSEQ named T1 & T2 respectively. |
| Stage 2: Synthesis of the translations. | Assignments: To work together, to resolve any discrepancies, and to obtain a consensual French version of the SSEQ (SSEQ-F). | 02 people: - TR1 - TR2 | Production of the first experimental version of the SSEQ-F (T1-2) from T1 & T2 |
| Stage 3: Back translation. | Assignments: To work from T1-2 version and to create two back translations BT1 & BT2 totally blind to the original version of the SSEQ. | 02 people: Individuals whose mother tongue is English, without medical background and self-efficacy study background (BTR1 & BTR2) | Production of two independent English versions of the SSEQ from T1-2 version. |
| Stage 4: Expert committee review. | Assignment: To work together using all reports, all the translated and original versions of SSEQ to produce the prefinal version of the SSEQ-F. | 11 people: -TR1 -TR2 -BTR1 -BTR2 -1 Doctor specialist in physical and rehabilitation medicine -1 physiotherapist specialist in stroke rehabilitation -1 Doctor in neurology -1 Doctor in psychology -2 stroke survivors -The principal researcher (ASH) | Production of the prefinal version of SSEQ-F. |
| Stage 5: Test of the prefinal version | Assignment: To administer the prefinal version of the SSEQ-F to the Beninese stroke patients. | 30 Beninese stroke survivors | Stroke survivors understood and answered the items of SSEQ-F without difficulty. |
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [PubMed]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Hutton-Johnson, I. Stroke Survivors’ Perceptions of Social Participation After Stroke. Perspect. Gerontol. 2011, 16, 56–63. [Google Scholar] [CrossRef]
- De Souza, F.H.N.; Silva Filho, E.; Cezarino, L.; de Melo, E.L.A.; Cacho, Ê.W.A. Social Participation as a goal of the post-stroke rehabilitation program: A literature review. Man. Ther. Posturology Rehabil. J. 2017, 15, 503. [Google Scholar] [CrossRef]
- Chino, N.; Sonoda, S.; Domen, K.; Saitoh, E.; Kimura, A. Stroke impairment assessment set (SIAS) a new evaluation instrument for stroke patients. Jpn. J. Rehabil. Med. 1994, 31, 119–125. [Google Scholar] [CrossRef]
- Batcho, C.S.; Tennant, A.; Thonnard, J.L. ACTIVLIM-Stroke: A crosscultural Rasch-built scale of activity limitations in patients with stroke. Stroke 2012, 43, 815–823. [Google Scholar] [CrossRef]
- Salter, K.L.; Foley, N.C.; Jutai, J.W.; Teasell, R.W. Assessment of participation outcomes in randomized controlled trials of stroke rehabilitation interventions. Int. J. Rehabil. Res. 2007, 30, 339–342. [Google Scholar] [CrossRef]
- Schiavi, M.; Costi, S.; Pellegrini, M.; Formisano, D.; Borghi, S.; Fugazzaro, S. Occupational therapy for complex inpatients with stroke: Identification of occupational needs in post-acute rehabilitation setting. Disabil. Rehabil. 2018, 40, 1026–1032. [Google Scholar] [CrossRef]
- Jones, F.; Riazi, A. Self-efficacy and self-management after stroke: A systematic review. Disabil. Rehabil. 2011, 33, 797–810. [Google Scholar] [CrossRef]
- Jones, F.; Partridge, C.; Reid, F. The Stroke Self-Efficacy Questionnaire: Measuring individual confidence in functional performance after stroke. J. Clin. Nurs. 2008, 17, 244–252. [Google Scholar] [CrossRef]
- Riazi, A.; Aspden, T.; Jones, F. Stroke Self-efficacy Questionnaire. J. Rehabil. Med. 2014, 46, 406–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostanjsek, N. Use of The International Classification of Functioning, Disability and Health (ICF) as a Conceptual Framework and Common Language for Disability Statistics and Health Information Systems. In BMC Public Health: 2011; BioMed Central: Geneva, Switzerland, 2011. [Google Scholar]
- Pearson, O.R.; Busse, M.; Van Deursen, R.W.M.; Wiles, C.M. Quantification of walking mobility in neurological disorders. QJM 2004, 97, 463–475. [Google Scholar] [CrossRef] [Green Version]
- Pajalic, Z.; Karlsson, S.; Westergren, A. Functioning and subjective health among stroke survivors after discharge from hospital. J. Adv. Nurs. 2006, 54, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Van De Port, I.G.; Kwakkel, G.; Van Wijk, I.; Lindeman, E. Susceptibility to deterioration of mobility long-term after stroke: A prospective cohort study. Stroke 2006, 37, 167–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urimubenshi, G. Activity limitations and participation restrictions experienced by people with stroke in Musanze district in Rwanda. Afr. Health Sci. 2015, 15, 917–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sogbossi, E.S.; Thonnard, J.-L.; Batcho, C.S. Assessing locomotion ability in West African stroke patients: Validation of ABILOCO-Benin scale. Arch. Phys. Med. Rehabil. 2014, 95, 1470–1476, e1473. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.E.; Eng, J.J. Goal Priorities Identified through Client-Centred Measurement in Individuals with Chronic Stroke. Physiother. Can. 2004, 56, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Törnbom, K.; Sunnerhagen, K.S.; Danielsson, A. Perceptions of physical activity and walking in an early stage after stroke or acquired brain injury. PLoS One 2017, 12, e0173463. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.H. The recovery of walking in stroke patients: A review. Int. J. Rehabil. Res. 2010, 33, 285–289. [Google Scholar] [CrossRef]
- English, C.; Manns., P.J.; Tucak, C.; Bernhardt, J. Physical activity and sedentary behaviors in people with stroke living in the community: A systematic review. Phys. Ther. 2014, 94, 185–196. [Google Scholar] [CrossRef]
- Aguiar, L.T.; Martins, J.C.; Nadeau, S.; Britto, R.R.; Teixeira-Salmela, L.F.; Faria, C.D. Efficacy of interventions to improve physical activity levels in individuals with stroke: A systematic review protocol. BMJ Open 2017, 7, e012479. [Google Scholar] [CrossRef]
- O’Donnell, M.J.; Xavier, D.; Liu, L.; Zhang, H.; Chin, S.L.; Rao-Melacini, P.; Rangarajan, S.; Islam, S.; Pais, P.; McQueen, M.J.; et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. Lancet 2010, 376, 112–123. [Google Scholar] [CrossRef]
- Gallanagh, S.; Quinn, T.J.; Alexander, J.; Walters, M.R. Physical activity in the prevention and treatment of stroke. ISRN Neurol. 2011, 2011, 953818. [Google Scholar] [CrossRef] [Green Version]
- Obembe, A.; Mapayi, B.; Johnson, O.; Agunbiade, T.; Emechete, A. Community reintegration in stroke survivors: Relationship with. motor function and depression. Hong Kong Physiother. J. 2013, 31, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Wood-Dauphinee, S.; Williams, J.I. Reintegration to normal living as a proxy to quality of life. J. Chronic Dis. 1987, 40, 491–499. [Google Scholar] [CrossRef]
- Olaoye, O.A.; Adejumobi, A.S.; Olasusi, A.O.; Aladesuyi, O.B.; Emechete, A.A. Relationship between community integration and life satisfaction among stroke survivors dwelling in rural communities of southwest, Nigeria. J. Environ. Occup. Health 2017, 6, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Crum, R.M.; Anthony, J.C.; Bassett, S.S.; Folstein, M.F. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef]
- Honado, A.S.; Roy, J.-S.; Daneault, J.-F.; Atigossou, O.L.G.; Batcho, C.S. Test-retest reliability of an adapted version of the International Physical Activity Questionnaire for healthy individuals and stroke survivors. Ann. Phys. Rehabil. Med. 2020, 63, 581–583. [Google Scholar] [CrossRef]
- Honado, A.S.; Atigossou, O.L.G.; Daneault, J.-F.; Roy, J.-S.; Batcho, C.S. Relationships between overall physical activity and step counts in able-bodied adults and stroke survivors in developing countries: A cross-sectional study. Disabil. Rehabil. 2022. [Google Scholar] [CrossRef] [PubMed]
- Bourget, N.; Deblock-Bellamy, A.; Blanchette, A.K.; Batcho, C.S. Use and psychometric properties of the Reintegration to Normal Living Index in rehabilitation: A systematic review. Ann. Phys. Rehabil. Med. 2018, 61, 262–269. [Google Scholar] [CrossRef] [PubMed]
- International Physical Activity Questionnaire. Available online: http://www.ipaq.ki.se (accessed on 15 November 2022).
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillemin, F.; Bombardier, C.; Beaton, D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J. Clin. Epidemiol. 1993, 46, 1417–1432. [Google Scholar] [CrossRef]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar] [PubMed]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation coefficients: Appropriate use and interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Olawale, O.A.; Usman, J.S.; Oke, K.I.; Osundiya, O.C. Evaluation of predictive factors influencing community reintegration in adult patients with stroke. J. Neurosci. Rural. Pract. 2018, 9, 006–010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einstad, M.S.; Saltvedt, I.; Lydersen, S.; Ursin, M.H.; Munthe-Kaas, R.; Ihle-Hansen, H.; Knapskog, A.-B.; Askim, T.; Beyer, M.K.; Næss, H. Associations between post-stroke motor and cognitive function: A cross-sectional study. BMC Geriatr. 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Vincent-Onabajo, G.; Musa, H.Y.; Joseph, E. Prevalence of balance impairment among stroke survivors undergoing neurorehabilitation in nigeria. J. Stroke Cerebrovasc. Dis. 2018, 27, 3487–3492. [Google Scholar] [CrossRef]
- Sarfo, F.S.; Berchie, P.; Singh, A.; Nichols, M.; Agyei-Frimpong, M.; Jenkins, C.; Ovbiagele, B.; Investigators, P.S. Prevalence, trajectory, and predictors of poststroke fatigue among Ghanaians. J. Stroke Cerebrovasc. Dis. 2019, 28, 1353–1361. [Google Scholar] [CrossRef]
- Akinyemi, R.O.; Ovbiagele, B.; Adeniji, O.A.; Sarfo, F.S.; Abd-Allah, F.; Adoukonou, T.; Ogah, O.S.; Naidoo, P.; Damasceno, A.; Walker, R.W. Stroke in Africa: Profile, progress, prospects and priorities. Nat. Rev. Neurol. 2021, 17, 634–656. [Google Scholar] [CrossRef] [PubMed]
- Atigossou, O.L.G.; Ouédraogo, F.; Honado, A.S.; Alagnidé, E.; Kpadonou, T.G.; Batcho, C.S. Association between post-stroke psychological disorders, activity limitations and health-related quality of life in chronic stroke survivors in Benin. Disabil. Rehabil. 2022. [Google Scholar] [CrossRef] [PubMed]
- Suwandewi, N.K.; Dewi, N.L.P.T.; Sukadarma, I.G.N.K.; Wati, N.M.N. The Relationship Between Self efficacy With The Ability Of Daily Living Activity Of Post-Stroke Patients. Caring: J. Keperawatan 2021, 10, 211–219. [Google Scholar]
- Korpershoek, C.; Van der Bijl, J. Hafsteinsdóttir TB: Self-efficacy and its influence on recovery of patients with stroke: A systematic review. J. Adv. Nurs. 2011, 67, 1876–1894. [Google Scholar] [CrossRef] [PubMed]
- Szczepańska-Gieracha, J.; Mazurek, J. The role of self-efficacy in the recovery process of stroke survivors. Psychol. Res. Behav. Manag. 2020, 13, 897. [Google Scholar] [CrossRef]
- Volz, M.; Möbus, J.; Letsch, C.; Werheid, K. The influence of early depressive symptoms, social support and decreasing self-efficacy on depression 6 months post-stroke. J. Affect. Disord. 2016, 206, 252–255. [Google Scholar] [CrossRef] [Green Version]
- French, M.A.; Moore, M.F.; Pohlig, R.; Reisman, D. Self-efficacy mediates the relationship between balance/walking performance, activity, and participation after stroke. Top. Stroke Rehabil. 2016, 23, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-M.; Moon, H.-H.; Lee, S.-K.; Lee, H.-L.; Park, Y.-J. The effects of a community-based walking program on walking ability and fall-related self-efficacy of chronic stroke patients. J. Exerc. Rehabil. 2019, 15, 20. [Google Scholar] [CrossRef] [Green Version]
- Thilarajah, S.; Mentiplay, B.F.; Bower, K.J.; Tan, D.; Pua, Y.H.; Williams, G.; Koh, G.; Clark, R.A. Factors associated with post-stroke physical activity: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2018, 99, 1876–1889. [Google Scholar] [CrossRef]
- Salbach, N.M.; Mayo, N.E.; Robichaud-Ekstrand, S.; Hanley, J.A.; Richards, C.L.; Wood-Dauphinee, S. Balance self-efficacy and its relevance to physical function and perceived health status after stroke. Arch. Phys. Med. Rehabil. 2006, 87, 364–370. [Google Scholar] [CrossRef]
- Pang, M.Y.; Eng, J.J.; Miller, W.C. Determinants of satisfaction with community reintegration in older adults with chronic stroke: Role of balance self-efficacy. Phys. Ther. 2007, 87, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Tito Vincent-Onabajo, G.; Kime Lawan, A.; Yoonus Oyeyemi, A.; Kolapo Hamzat, T. Functional self-efficacy and its determinants in Nigerian stroke survivors. Top. Stroke Rehabil. 2012, 19, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-Efficacy. In Encyclopedia of Human Behavior; Ramachaudran, V., Ed.; Academic Press: New York, NY, USA, 1994; Volume 4, pp. 71–81. [Google Scholar]
- Robinson-Smith, G. Self-efficacy and quality of life after stroke. J. Neurosci. Nurs. 2002, 34, 91. [Google Scholar] [CrossRef]
- Hamzat, T.K.; Agbomeji, O.; Peters, G. Relationship between functional abilities confidence level and performance of motor function after stroke. J. Niger. Soc. Physiother. 2009, 17, 7–10. [Google Scholar]
- Messina, R.; Dallolio, L.; Fugazzaro, S.; Rucci, P.; Iommi, M.; Bardelli, R.; Costi, S.; Denti, M.; Accogli, M.A.; Cavalli, E. The Look After Yourself (LAY) intervention to improve self-management in stroke survivors: Results from a quasi-experimental study. Patient Educ. Couns. 2020, 103, 1191–1200. [Google Scholar] [CrossRef]
- Lorig KR, Sobel DS, Ritter PL, Laurent D, Hobbs M: Effect of a self-management program on patients with chronic disease. Eff. Clin. Pract. ECP 2001, 4, 256–262.
- Fryer CE, Luker JA, McDonnell MN, Hillier SL: Self management programmes for quality of life in people with stroke. Cochrane Database Syst. Rev. 2016, 47, e266–e267.
- Sit, J.W.; Chair, S.Y.; Choi, K.C.; Chan, C.W.; Lee, D.T.; Chan, A.W.; Cheung, J.L.; Tang, S.W.; Chan, P.S.; Taylor-Piliae, R.E. Do empowered stroke patients perform better at self-management and functional recovery after a stroke? A randomized controlled trial. Clin. Interv. Aging 2016, 11, 1441. [Google Scholar] [CrossRef] [Green Version]
- Arkan, G.; Beser, A.; Haney, M.O.; Ozturk, V. Psychometric testing of the Turkish version of the Stroke Self-Efficacy Questionnaire. J. Nurs. Res. 2019, 27, e35. [Google Scholar] [CrossRef]
- Lo, S.H.S.; Chang, A.M.; Chau, J.P.C. Translation and validation of a Chinese version of the stroke self-efficacy questionnaire in community-dwelling stroke survivors. Top. Stroke Rehabil. 2016, 23, 163–169. [Google Scholar] [CrossRef]
- Makhoul, M.P.; Pinto, E.B.; Mazzini, N.A.; Winstein, C.; Torriani-Pasin, C. Translation and validation of the stroke self-efficacy questionnaire to a Portuguese version in stroke survivors. Top. Stroke Rehabil. 2020, 27, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.K.S.; Pallesen, H. Stroke self-efficacy questionnaire–Denmark (SSEQ-DK): Test–retest of the Danish version. Top. Stroke Rehabil. 2022. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Adamu, A.A.; Hassan, A.B.; Dominic, E.; Dada, O.; Abdullahi, A. Hausa translation, cross-cultural adaptation, and assessment of psychometric properties of the Stroke Self-Efficacy Questionnaire. Physiother. Theory Pract. 2021, 39, 174–181. [Google Scholar] [CrossRef] [PubMed]

| Variables | Values |
|---|---|
| Mean ± SD | |
| Age (years) | 56.7 ± 10.4 |
| Body mass index (kg/m²) | 26.4 ± 3.7 |
| n (%) | |
| Normal weight | 22 (36.7) |
| Overweight | 29 (48.3) |
| Obese | 9 (15) |
| Gender | |
| Male | 44 (73.3) |
| Female | 16 (26.7) |
| Educational level | |
| More than secondary | 9 (15) |
| Secondary | 35 (58.3) |
| Less than secondary | 16 (27.6) |
| Employment status | |
| White collar | 11 (18.3) |
| Blue collar | 23 (38.3) |
| Unemployed | 26 (43.3) |
| Time since stroke (month) | Median/interquartile range |
| 14.1/40.9 | |
| n (%) | |
| ≤6 months | 19 (31.7) |
| >6 months | 41 (68.3) |
| SCORES | |||||
|---|---|---|---|---|---|
| VARIABLES | Min (Min p) | 25th Centile | Median (IQR) | 75th Centile | Max (Max p) |
| Mean ± SD | |||||
| Self-efficacy | 4 (0) | 9 | 10.5 (5) | 14 | 24 (39) |
| 12 ± 4.3 | |||||
| Activity limitations | 11 (0) | 14 | 15 (3) | 17 | 27 (40) |
| 15.6 ± 2.6 | |||||
| Locomotor ability | 5 (0) | 10 | 11 (1.7) | 11.7 | 19 (30) |
| 10.7 ± 2.1 | |||||
| Community reintegration | 5 (0) | 12.2 | 15 (4.7) | 17 | 20 (22) |
| 14.4 ± 3.1 | |||||
| Physical activity (METS.min/week) | 0 (0) | 33 | 66 (391.8) | 424.8 | 970.5 (NA) |
| 235.9 ± 313.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Honado, A.S.; Atigossou, O.L.G.; Roy, J.-S.; Daneault, J.-F.; Batcho, C.S. Relationships between Self-Efficacy and Post-Stroke Activity Limitations, Locomotor Ability, Physical Activity, and Community Reintegration in Sub-Saharan Africa: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 2286. https://doi.org/10.3390/ijerph20032286
Honado AS, Atigossou OLG, Roy J-S, Daneault J-F, Batcho CS. Relationships between Self-Efficacy and Post-Stroke Activity Limitations, Locomotor Ability, Physical Activity, and Community Reintegration in Sub-Saharan Africa: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(3):2286. https://doi.org/10.3390/ijerph20032286
Chicago/Turabian StyleHonado, Aristide S., Orthelo Léonel Gbètoho Atigossou, Jean-Sébastien Roy, Jean-François Daneault, and Charles Sèbiyo Batcho. 2023. "Relationships between Self-Efficacy and Post-Stroke Activity Limitations, Locomotor Ability, Physical Activity, and Community Reintegration in Sub-Saharan Africa: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 3: 2286. https://doi.org/10.3390/ijerph20032286