
Participation in Population Health Interventions by Older Adults in Poland: Barriers and Enablers
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
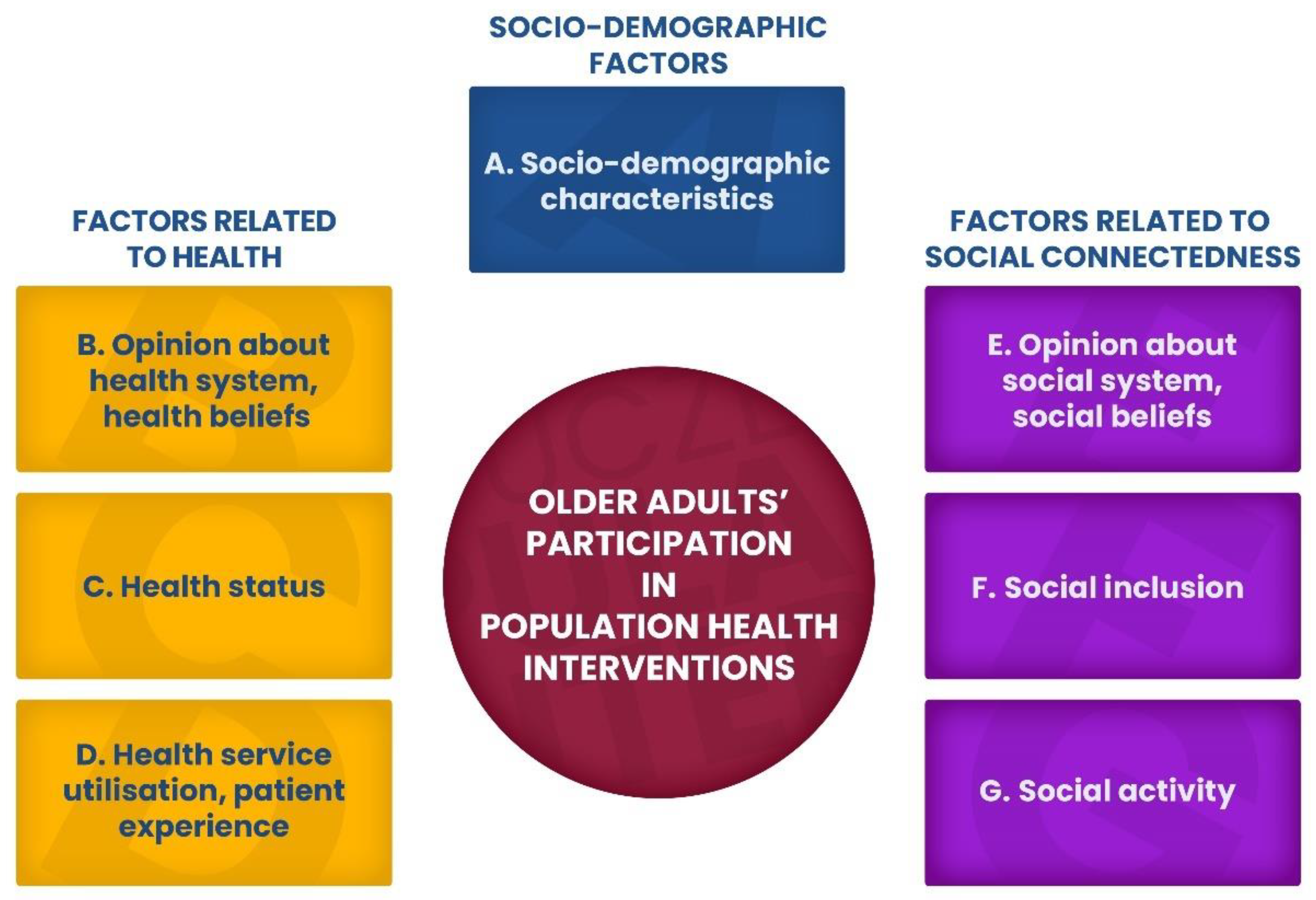
2.1. Conceptual Framework
- An undertaking (work);
- Organised by public healthcare and/or educational facilities, non-governmental organisations, enterprises or other entities;
- Promoted as the following:
- o
- Free-of-charge and available for specific groups of people (e.g., age, gender) within a particular period, beneficiaries inhabiting a particular place;
- o
- With the purpose to improve or maintain health.
2.2. Methods
2.3. Statistical Analysis
2.4. Material
3. Results
3.1. Scope of Participation in Health Programmes
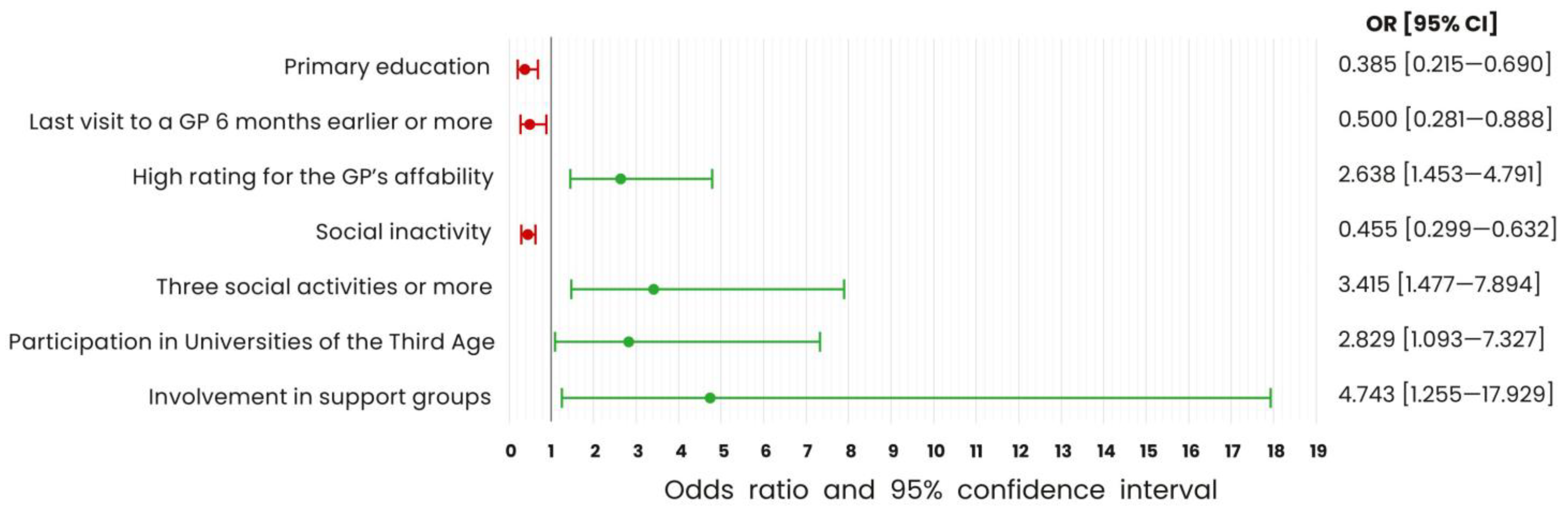
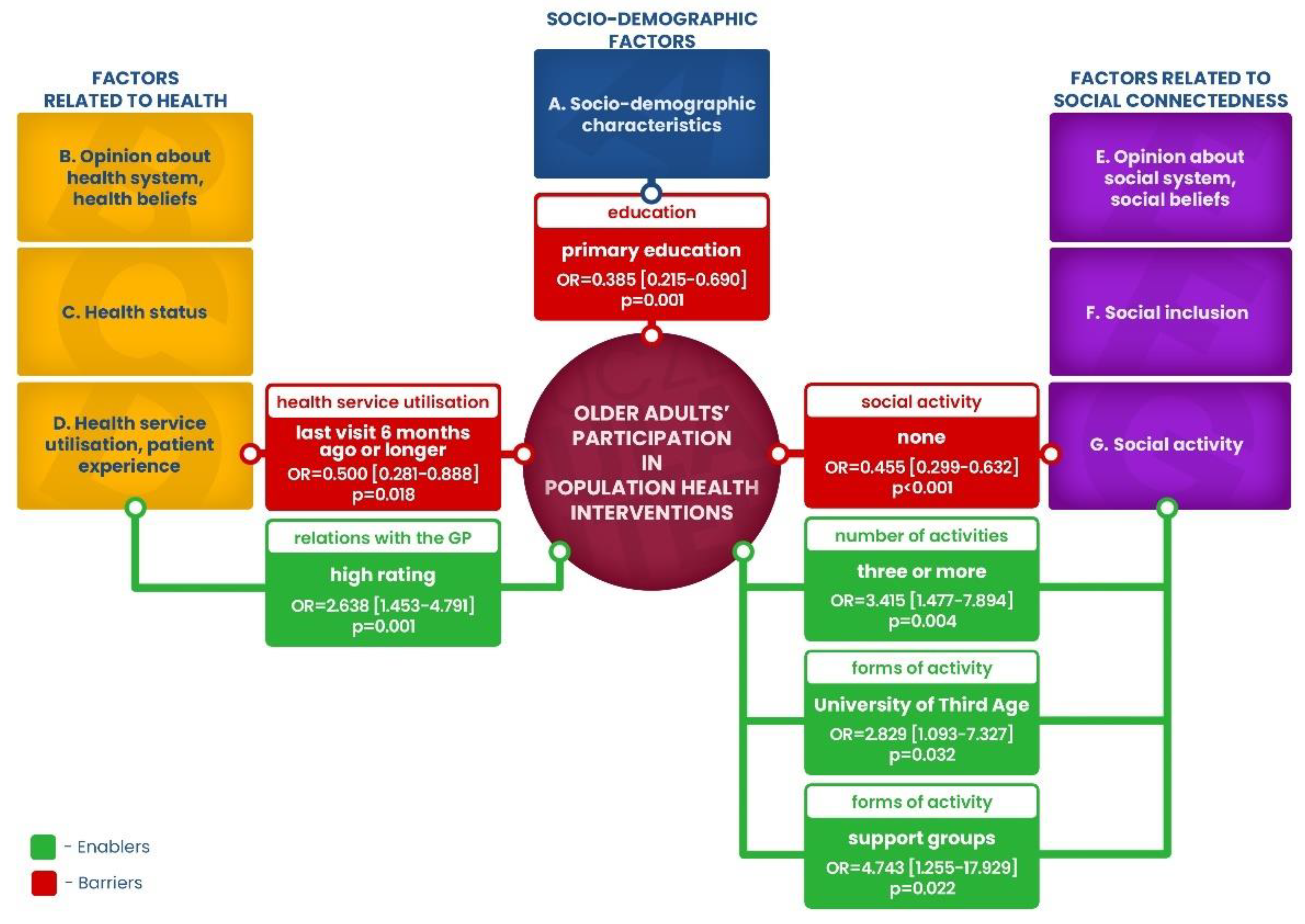
3.2. Enablers and Barriers to Older Adults’ Participation in Health Programmes
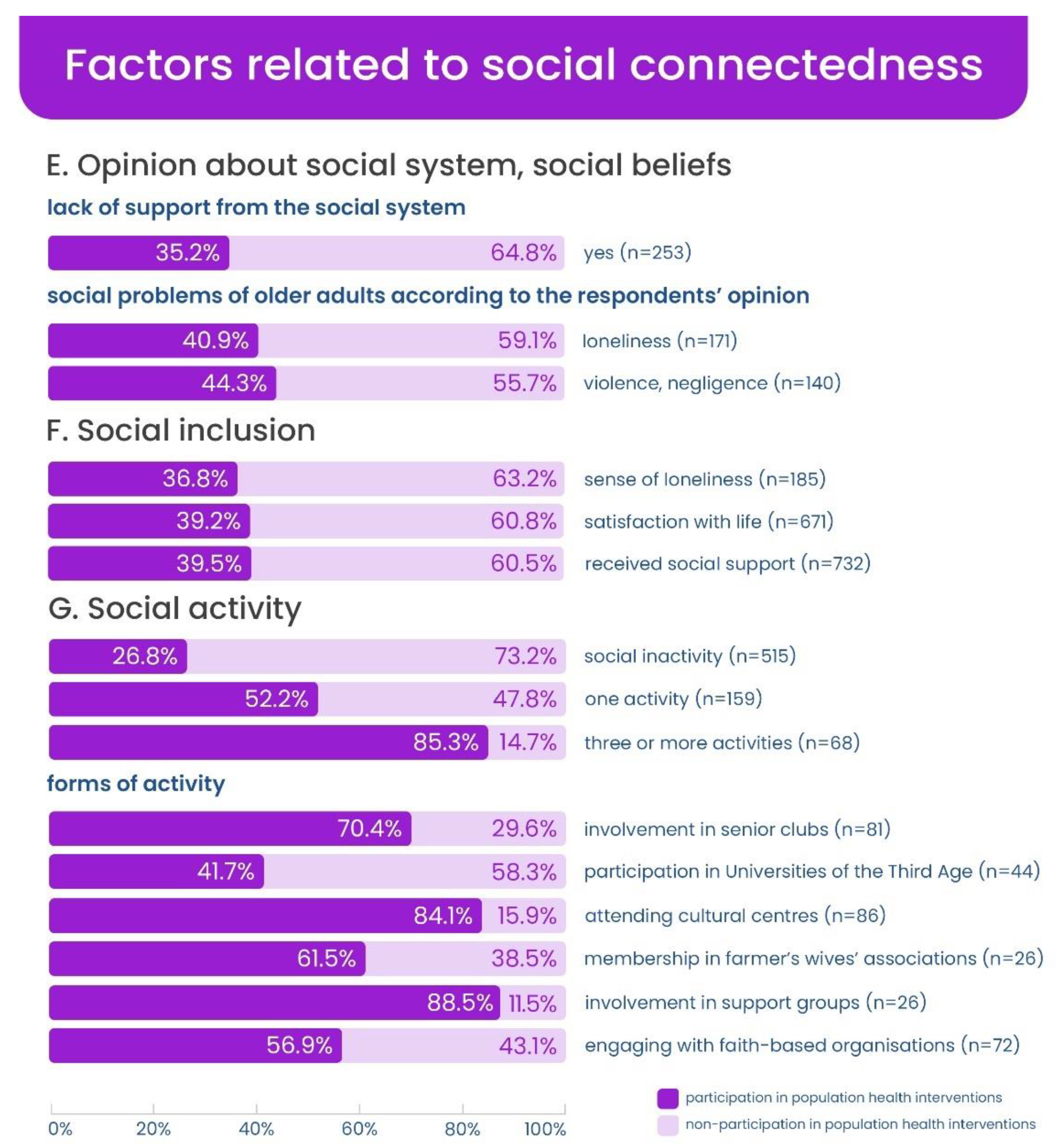
- Number of social activities: the chance of participation had increased more than threefold on the condition of participation in several forms of social activity. In the case of three or more social activities, the OR was 3.415 [1.477–7.894], (p = 0.004).
- Forms of social activities: engagement in support groups increased the chance of participation in health programmes as much as five times (OR = 4.743 [1.255–17.929], p = 0.022). A particularly important factor proved to be involvement in the University of the Third Age educational activities, which almost tripled the chance of using health programmes (OR = 2.829 [1.093–7.327], p = 0.032).
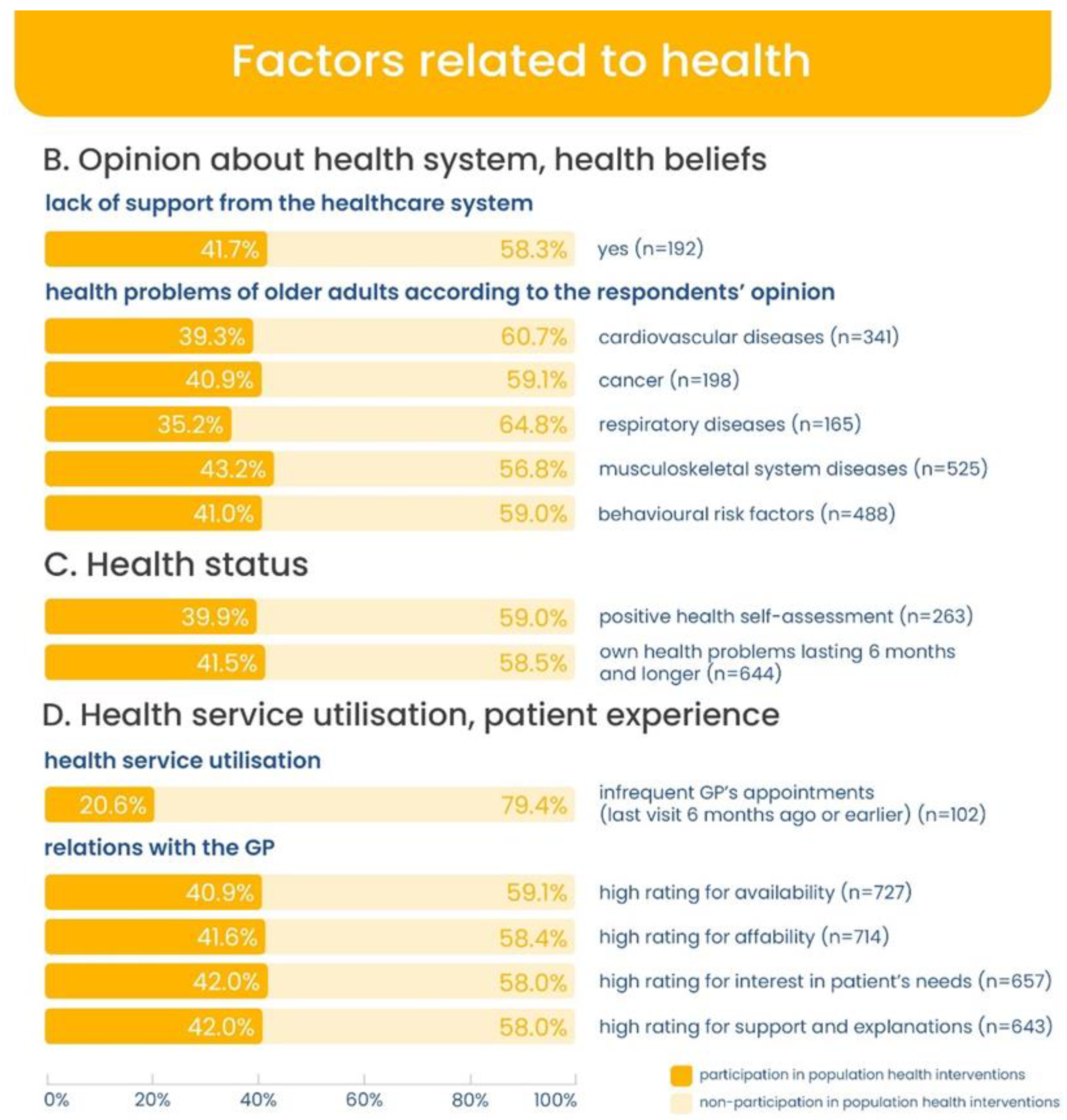
- Relation with the general practitioner (GP): his/her affability increased the chance of participation in population health interventions by 2.6 times (OR = 2.638 [1.453–4.791], p = 0.001).
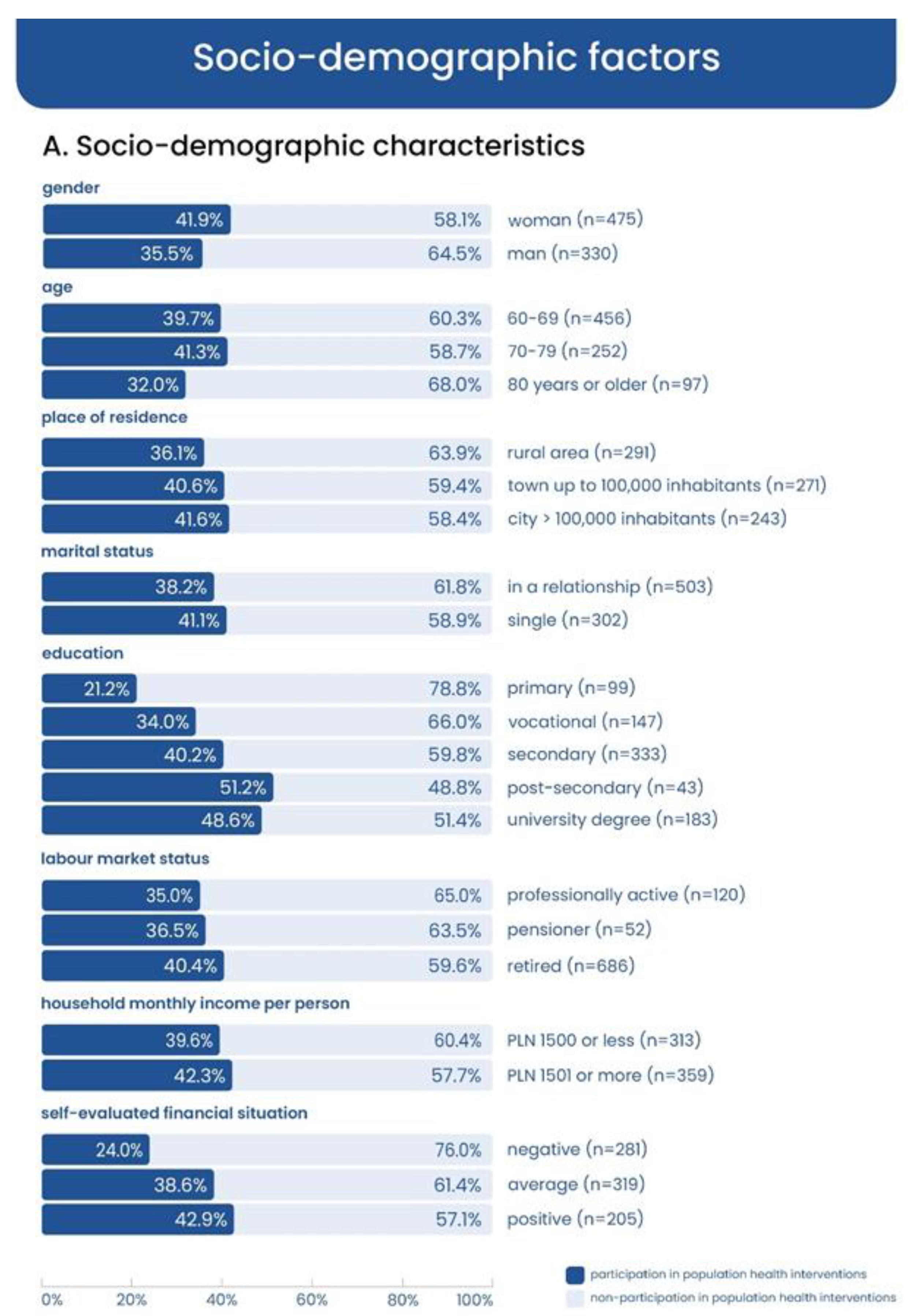
- Education: primary level (OR = 0.385 [0.215–0.690], p = 0.001) decreased the chance of participation by 61.5% in relation to people with higher education.
- Social activity: lack of social activity reduced the chance of participation by 54.5% (OR = 0.455 [0.299–0.632], p < 0.001).
- Health service utilisation: infrequent GP’s appointments halved the chance of participating (OR = 0.500 [0.281–0.888], p = 0.018).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistics Poland. Demographic Yearbook of Poland. 2019. Available online: https://stat.gov.pl/en/topics/statistical-yearbooks/statistical-yearbooks/demographic-yearbook-of-poland-2019,3,13.html (accessed on 10 July 2022).
- Eurostat. Population Structure Indicators at National Level. Available online: https://ec.europa.eu/eurostat/databrowser/view/DEMO_PJANIND__custom_4546345/default/table?lang=en (accessed on 15 August 2022).
- Statistics Poland. The Situation of Older People in Poland in 2020. Available online: https://stat.gov.pl/en/topics/older-people/older-people/the-situation-of-older-people-in-poland-in-2020,1,3.html?fbclid=IwAR0SIzFCUvmzazA4q4IvC9m8ZE6dQw4zjWNXgjjc-1aUT-l41FOtkk6p9Uc (accessed on 10 July 2022).
- World Health Organization. World Report on Ageing and Health. Geneva. 2015. Available online: https://apps.who.int/iris/handle/10665/186463 (accessed on 11 August 2022).
- Canadian Institutes of Health Research. Population Health Intervention Research Initiative for Canada. Available online: https://cihr-irsc.gc.ca/e/38731.html (accessed on 12 August 2022).
- Hawe, P.; Potvin, L. What is population health intervention research? Can. J. Public Health 2009, 100, I8–I14. [Google Scholar] [CrossRef]
- Moore, G.; Cambon, L.; Michie, S.; Arwidson, P.; Ninot, G.; Ferron, C.; Potvin, L.; Kellou, N.; Charlesworth, J.; Alla, F.; et al. Population health intervention research: The place of theories. Trials 2019, 20, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minary, L.; Alla, F.; Cambon, L.; Kivits, J.; Potvin, L. Addressing complexity in population health intervention research: The context/intervention interface. J. Epidemiol. Community Health 2018, 72, 319–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wodchis, W.P.; Dixon, A.; Anderson, G.M.; Goodwin, N. Integrating care for older people with complex needs: Key insights and lessons from a seven-country cross-case analysis. Int. J. Integr. Care 2015, 23, e021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duplaga, M.; Grysztar, M.; Rodzinka, M.; Kopec, A. Scoping review of health promotion and disease prevention interventions addressed to elderly people. BMC Health Serv. Res. 2016, 16 (Suppl. S5), 278. [Google Scholar] [CrossRef] [Green Version]
- Chiu, C.J.; Hu, J.C.; Lo, Y.H.; Chang, E.Y. Health Promotion and Disease Prevention Interventions for the Elderly: A Scoping Review from 2015–2019. Int. J. Environ. Res. Public Health 2020, 17, 5335. [Google Scholar] [CrossRef]
- Mah, J.; Rockwood, K.; Stevens, S.; Keefe, J.; Andrew, M.K. Do Interventions Reducing Social Vulnerability Improve Health in Community Dwelling Older Adults? A Systematic Review. Clin. Interv. Aging 2022, 17, 447–465. [Google Scholar] [CrossRef]
- Ministry of Health and Care Services. The Norwegian Public Health Act. Available online: https://app.uio.no/ub/ujur/oversatte-lover/data/lov-20110624-029-eng.pdf (accessed on 12 August 2022).
- Patyna, M.; Płusa, A.; Ziębińska, A. Kluczowe zagadnienia dotyczące projektowania i realizacji programów polityki zdrowotnej. Zdr. Publiczne Zarządzanie 2019, 17, 203–216. [Google Scholar] [CrossRef]
- Cybulski, M.; Krajewska-Kułak, E. Edukacja Prozdrowotna Seniorów jako Szansa na Pomyślne Starzenie się na Przykładzie Miasta Białegostoku. Uniwersytet Medyczny w Białymstoku. 2016. Available online: https://www.umb.edu.pl/photo/pliki/Dziekanat-WNOZ/monografie/12-2016/edukacja_prozdrowotna_seniorow.pdf (accessed on 12 August 2022).
- Levesque, J.F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [Green Version]
- Eurostat. NUTS—Nomenclature of Territorial Units for Statistics. Available online: https://ec.europa.eu/eurostat/web/nuts/background (accessed on 12 August 2022).
- Statistics Poland. Statistical Yearbook of the Republic of Poland. 2017. Available online: https://stat.gov.pl/en/topics/statistical-yearbooks/statistical-yearbooks/statistical-yearbook-of-the-republic-of-poland-2017,2,17.html (accessed on 15 August 2022).
- Czapiński, J.; Błędowski, P. Aktywność Społeczna Osób Starszych w Kontekście Percepcji Polaków; Diagnoza Społeczna 2013. Raport Tematyczny; Ministerstwo Pracy i Polityki Społecznej i Centrum Rozwoju Zasobów Ludzkich: Warszawa, Poland, 2014. [Google Scholar]
- Bunn, F.; Dickinson, A.; Barnett-Page, E.; McInnes, E.; Horton, K. A systematic review of older people’s perceptions of facilitators and barriers to participation in falls-prevention interventions. Ageing Soc. 2008, 28, 449–472. [Google Scholar] [CrossRef] [Green Version]
- Harden, A.; Sheridan, K.; McKeown, A.; Dan-Ogosi, I.; Bagnall, A.M. Evidence Review of Barriers to, and Facilitators of, Community Engagement Approaches and Practices in the UK; Institute for Health and Human Development, University of East London: London, UK, 2015; Available online: https://www.nice.org.uk/guidance/ng44/evidence/evidence-review-5-community-engagement-barriers-and-facilitators-pdf-2368403681 (accessed on 12 August 2022).
- Higuchi, M.; Narumoto, K.; Goto, T.; Inoue, M. Correlation between family physician’s direct advice and pneumococcal vaccination intention and behavior among the elderly in Japan: A cross-sectional study. BMC Fam. Pract. 2018, 19, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Wang, H.H.X.; Ma, E.S.K.; Wong, M.C.S. Contributions of physicians to government-subsidised disease prevention programmes: An appeal for active participation. Hong Kong Med. J. 2020, 26, 364–366. [Google Scholar] [CrossRef]
- Sandlund, M.; Skelton, D.A.; Pohl, P.; Ahlgren, C.; Melander-Wikman, A.; Lundin-Olsson, L. Gender perspectives on views and preferences of older people on exercise to prevent falls: A systematic mixed studies review. BMC Geriatr. 2017, 17, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petter, J.; Reitsma-van Rooijen, M.M.; Korevaar, J.C.; Nielen, M.M. Willingness to participate in prevention programs for cardiometabolic diseases. BMC Public Health 2015, 15, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gyulai, A.; Nagy, A.; Pataki, V.; Tonté, D.; Ádány, R.; Vokó, Z. General practitioners can increase participation in cervical cancer screening—A model program in Hungary. BMC Fam. Pract. 2018, 19, 67. [Google Scholar] [CrossRef] [Green Version]
- Chow, S.K.; Wong, F.K. A randomized controlled trial of a nurse-led case management programme for hospital-discharged older adults with co-morbidities. J. Adv. Nurs. 2014, 70, 2257–2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, Y.I.; Lin, T.F. Social capital and preventive care use among the elderly under Taiwan’s National Health Insurance. Arch. Gerontol. Geriatr. 2018, 75, 28–36. [Google Scholar] [CrossRef]
- Vozikaki, M.; Linardakis, M.; Philalithis, A. Preventive health services utilization in relation to social isolation in older adults. J. Public Health 2017, 25, 545–556. [Google Scholar] [CrossRef]
- Stafford, M.; von Wagner, C.; Perman, S.; Taylor, J.; Kuh, D.; Sheringham, J. Social connectedness and engagement in preventive health services: An analysis of data from a prospective cohort study. Lancet Public Health 2018, 3, e438–e446. [Google Scholar] [CrossRef] [Green Version]
- Leinonen, M.K.; Campbell, S.; Klungsøyr, O.; Lönnberg, S.; Hansen, B.T.; Nygård, M. Personal and provider level factors influence participation to cervical cancer screening: A retrospective register-based study of 1.3 million women in Norway. Prev. Med. 2017, 94, 31–39. [Google Scholar] [CrossRef]
- Broberg, G.; Wang, J.; Östberg, A.L.; Adolfsson, A.; Nemes, S.; Sparen, P.; Stander, B. Socio-economic and demographic determinants affecting participation in the Swedish cervical screening program: A population-based case-control study. PLoS ONE 2018, 13, e0190171. [Google Scholar] [CrossRef] [Green Version]
- Kristensson, J.H.; Sander, B.B.; von Euler-Chelpin, M.; Lynge, E. Predictors of non-participation in cervical screening in Denmark. Cancer Epidemiol. 2014, 38, 174–180. [Google Scholar] [CrossRef]
- Bobitt, J.; Aguayo, L.; Payne, L.; Jansen, T.; Schwingel, A. Geographic and Social Factors Associated with Chronic Disease Self-Management Program Participation: Going the “Extra-Mile” for Disease Prevention. Prev. Chronic Dis. 2019, 16, E25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucyk, K.; Simmonds, K.A.; Lorenzetti, D.L.; Drews, S.J.; Svenson, L.W.; Russell, M.L. The association between influenza vaccination and socioeconomic status in high income countries varies by the measure used: A systematic review. BMC Med. Res. Methodol. 2019, 19, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, L.; Flowers, P.; McLeod, J.; Young, D.; Rollins, L. The Catalyst Project Team. Social Patterning and Stability of Intention to Accept a COVID-19 Vaccine in Scotland: Will Those Most at Risk Accept a Vaccine? Vaccines 2021, 9, 17. [Google Scholar] [CrossRef]
- Syan, S.K.; Gohari, M.R.; Levitt, E.E.; Belisario, K.; Gillard, J.; DeJesus, J.; MacKillop, J. COVID-19 Vaccine Perceptions and Differences by Sex, Age, and Education in 1367 Community Adults in Ontario. Front. Public Health. 2021, 9, 719665. [Google Scholar] [CrossRef] [PubMed]
- CBOS (Centrum Badania Opinii Społecznej). Korzystanie ze Świadczeń i Ubezpieczeń Zdrowotnych. Available online: https://www.cbos.pl/SPISKOM.POL/2020/K_098_20.PDF (accessed on 15 August 2022).
- CBOS (Centrum Badania Opinii Społecznej). Opinie na Temat Funkcjonowania Systemu Opieki Zdrowotnej. Available online: https://www.cbos.pl/SPISKOM.POL/2021/K_125_21.PDF (accessed on 15 August 2022).
- Aktywność Osób Starszych Opracowania Tematyczne OT–672. Kancelaria Senatu. Biuro Analiz, Dokumentacji i Korespondencji. Warszawa. 2019. Available online: https://www.senat.gov.pl/gfx/senat/pl/senatopracowania/170/plik/ot-672.pdf (accessed on 15 August 2022).
- Behawioralnie o Polityce Aktywizacji Seniorów. Polski Instytut Ekonomiczny. Warszawa. 2020. Available online: https://pie.net.pl/wp-content/uploads/2021/06/PIE-Raport-Behawioralnie-o-polityce-aktywizacji-seniorow.pdf (accessed on 15 August 2022).
- Uniwersytety Trzeciego Wieku w Roku Akademickim 2017/2018. GUS, Warszawa, Gdańsk. 2019. Available online: https://stat.gov.pl/files/gfx/portalinformacyjny/pl/defaultaktualnosci/5488/11/2/1/uniwersytety_trzeciego_wieku_w_roku_akademickim_2017-2018.pdf (accessed on 15 August 2022).
- Badanie Ewaluacyjne Realizacji Rządowego Programu na Rzecz Aktywności Osób Starszych na Lata 2014–2020. Edycje 2016–2019. Instytut Pracy i Spraw Socjalnych. Available online: https://das.mpips.gov.pl/source/2020/Badanie%20ewaluacyjne%20realizacji%20Rzdowego%20Programu%20na%20rzecz%20Aktywnosci%20Osob%20Starszych%20na%20lata%202014-2020%20Edycje%202016-2019.pdf (accessed on 16 August 2022).
- Badanie Ewaluacyjne z Realizacji Programu Wieloletniego ”Senior+” na Lata 2015–2020. Edycje 2016–2019. Raport Końcowy. Instytut Pracy i Spraw Socjalnych. Available online: https://das.mpips.gov.pl/source/2020/1_Badanie%20ewaluacyjne%20realizacji%20programu%20wieloletniego%20Senior%20na%20lata%202015-2020%20Edycje%202016-2019.pdf (accessed on 17 August 2022).
- Craveiro, D. The role of personal social networks on health inequalities across European regions. Health Place 2017, 45, 24–31. [Google Scholar] [CrossRef]
- Theory at a glance: A Guide for Health Promotion Practice. Department of Health and Human Services, National Institutes of Health, National Cancer Institute: Bethesda, MD, USA. 2020. Available online: https://cancercontrol.cancer.gov/sites/default/files/2020-06/theory.pdf (accessed on 18 August 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristcs | n | % of Total | |
|---|---|---|---|
| Socio-Demographic Factors | |||
| A. Socio-Demographic Characteristics | |||
| Gender | Woman | 475 | 59.0 |
| Man | 330 | 41.0 | |
| Age | 60–69 | 456 | 56.6 |
| 70–79 | 252 | 31.3 | |
| 80 years or older | 97 | 12.1 | |
| Place of residence | Rural area | 291 | 36.1 |
| Town up to 100,000 inhabitants | 271 | 33.7 | |
| City >100,000 inhabitants | 243 | 30.2 | |
| Marital status | In a relationship | 503 | 62.5 |
| Single | 302 | 37.5 | |
| Education | Primary | 99 | 12.3 |
| Vocational | 147 | 18.3 | |
| Secondary | 333 | 41.4 | |
| Post-secondary | 43 | 5.3 | |
| University degree | 183 | 22.7 | |
| Labour market status * | Professionally active | 120 | 14.9 |
| Pensioner | 52 | 6.5 | |
| Retired | 686 | 85.2 | |
| Household monthly income per person | PLN 1500 or less ** | 313 | 38.9 |
| PLN 1501 or more ** | 359 | 44.6 | |
| Self-evaluated financial situation | Negative | 281 | 34.9 |
| Average | 319 | 39.6 | |
| Positive | 205 | 25.5 | |
| FactorsRelatedto Health | |||
| B. Opinion about Health System, Health Beliefs | |||
| Lack of support from the healthcare system | 192 | 23.9 | |
| Health problems of older adults according to the respondents’ opinion | Cardiovascular diseases | 341 | 42.4 |
| Cancer | 198 | 24.6 | |
| Respiratory diseases | 165 | 20.5 | |
| Musculoskeletal system diseases | 525 | 65.2 | |
| Behavioural risk factors | 488 | 60.6 | |
| C. Health Status | |||
| Positive health self-assessment | 263 | 32.7 | |
| Duration of health problems | Lasting 6 months and more | 644 | 80.0 |
| D. Health Service Utilisation, Patient Experience | |||
| Health service utilisation | Infrequent general practitioner’s (gp’s) appointments (last visit 6 months ago or earlier) | 102 | 12.7 |
| Relations with the general practitioner | High rating for availability | 727 | 90.3 |
| High rating for affability | 714 | 88.7 | |
| High rating for interest in patient’s needs | 657 | 81.6 | |
| High rating for support and explanations | 643 | 79.9 | |
| Factors Related to Social Connectedness | |||
| E. Opinion about Social System, Social Beliefs | |||
| Lack of support from the social system | 253 | 31.4 | |
| Social problems of older adults according to the respondents’ opinion | Loneliness | 171 | 21.2 |
| Violence, negligence | 140 | 17.4 | |
| F. Social Inclusion | |||
| Sense of loneliness | 185 | 23.0 | |
| Satisfaction with life | 671 | 83.4 | |
| Received social support | 732 | 90.9 | |
| G. Social Activity | |||
| Social inactivity | 515 | 64.0 | |
| Number of activities | One | 159 | 19.8 |
| Three or more | 68 | 8.4 | |
| Forms of activity * | Involvement in senior clubs | 81 | 10.1 |
| Participation in Universities of the Third Age | 44 | 5.5 | |
| Attending cultural centres | 86 | 10.7 | |
| Membership in farmer’s wives’ associations | 26 | 3.2 | |
| Involvement in support groups | 26 | 3.2 | |
| Engaging with faith-based organisations | 72 | 8.9 | |
| Variable | Odds Ratio for Participation in Health Programmes (OR) | 95% Confidence Interval Limits for OR | Significance (p-Value) |
|---|---|---|---|
| Socio-Demographic Factors | |||
| A. Socio-Demographic Characteristics | |||
| Woman | 1.313 | 0.982–1.754 | NS |
| Age of 60–69 | 1.043 | 0.784–1.388 | NS |
| Age of 80 and more | 0.697 | 0.443–1.096 | NS |
| Place of residence—rural area | 0.811 | 0.602–1.091 | NS |
| Place of residence—city >100,000 inhabitants | 1.148 | 0.845–1.560 | NS |
| Marital status—in a relationship | 0.886 | 0.662–1.186 | NS |
| Primary education | 0.375 | 0.226–0.621 | <0.001 |
| University degree | 1.648 | 1.181–2.298 | 0.003 |
| Professionally active | 0.808 | 0.539–1.211 | NS |
| Retired | 1.389 | 0.920–2.098 | NS |
| Household monthly income per person below PLN 1500 | 1.025 | 0.767–1.370 | NS |
| Negative self-evaluated financial situation | 0.668 | 0.493–0.904 | 0.009 |
| FactorsRelatedto Health | |||
| B. Opinion about Health System, Health Beliefs | |||
| Lack of support from the healthcare system | 1.141 | 0.820–1.587 | NS |
| Cardiovascular disease as a health problem of the population of older adults | 1.003 | 0.753–1.335 | NS |
| Cancer as a health problem | 1.096 | 0.790–1.520 | NS |
| Respiratory diseases as a health problem | 0.803 | 0.562–1.146 | NS |
| Musculoskeletal system diseases as a health problem | 1.635 | 1.205–2.218 | 0.002 |
| Behavioural risk factors as a health problem | 1.203 | 0.899–1.610 | NS |
| C. Health Status | |||
| Positive self-assessment of health | 1.043 | 0.771–1.409 | NS |
| Own health problems lasting 6 months and longer | 1.619 | 1.118–2.345 | 0.011 |
| D. Health Service Utilisation, Patient Experience | |||
| Visit to a GP 6 months earlier or more | 0.359 | 0.217–0.593 | <0.001 |
| High rating for GP’s availability | 2.145 | 1.253–3.672 | 0.005 |
| High rating for GP’s affability | 2.699 | 1.593–4.571 | <0.001 |
| High rating for GP’s interest in patient’s needs | 1.956 | 1.318–2.902 | <0.001 |
| High rating for GP’s support, Explanations | 1.825 | 1.254–2.658 | 0.002 |
| Factors Related to Social Connectedness | |||
| E. Opinion about Social System, Social Beliefs | |||
| Lack of support from the Social system | 0.707 | 0.571–1.058 | NS |
| Loneliness as a social problem | 1.093 | 0.775–1.542 | NS |
| Violence, negligence as a social problem | 1.286 | 0.890–1.859 | NS |
| F. Social Inclusion | |||
| Sense of loneliness | 0.872 | 0.621–1.224 | NS |
| Satisfaction with life | 0.985 | 0.674–1.440 | NS |
| Received social support | 1.111 | 0.676–1.828 | NS |
| G. Social Activity | |||
| Social inactivity | 0.230 | 0.169–0.313 | <0.001 |
| One social activity | 1.936 | 1.364–2.747 | <0.001 |
| Three or more social activities | 10.768 | 5.412–21.425 | <0.001 |
| Involvement in senior clubs | 4.264 | 2.585–7.034 | <0.001 |
| Participation in Universities of the Third Age | 9.132 | 4.017–20.758 | <0.001 |
| Attending cultural centres | 6.656 | 3.910–11.332 | <0.001 |
| Membership in farmer’s wives’ associations | 2.555 | 1.144–5.703 | 0.022 |
| Involvement in support groups | 12.717 | 3.785–42.723 | <0.001 |
| Engaging with faith-based Organisations | 2.203 | 1.350–3.595 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cianciara, D.; Lewtak, K.; Poznańska, A.; Piotrowicz, M.; Gajewska, M.; Urban, E.; Sugay, L.; Rutyna, A. Participation in Population Health Interventions by Older Adults in Poland: Barriers and Enablers. Int. J. Environ. Res. Public Health 2023, 20, 2284. https://doi.org/10.3390/ijerph20032284
Cianciara D, Lewtak K, Poznańska A, Piotrowicz M, Gajewska M, Urban E, Sugay L, Rutyna A. Participation in Population Health Interventions by Older Adults in Poland: Barriers and Enablers. International Journal of Environmental Research and Public Health. 2023; 20(3):2284. https://doi.org/10.3390/ijerph20032284
Chicago/Turabian StyleCianciara, Dorota, Katarzyna Lewtak, Anna Poznańska, Maria Piotrowicz, Małgorzata Gajewska, Ewa Urban, Larysa Sugay, and Anna Rutyna. 2023. "Participation in Population Health Interventions by Older Adults in Poland: Barriers and Enablers" International Journal of Environmental Research and Public Health 20, no. 3: 2284. https://doi.org/10.3390/ijerph20032284