
Correlation between UV Index, Temperature and Humidity with Respect to Incidence and Severity of COVID 19 in Spain
 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
3. Results
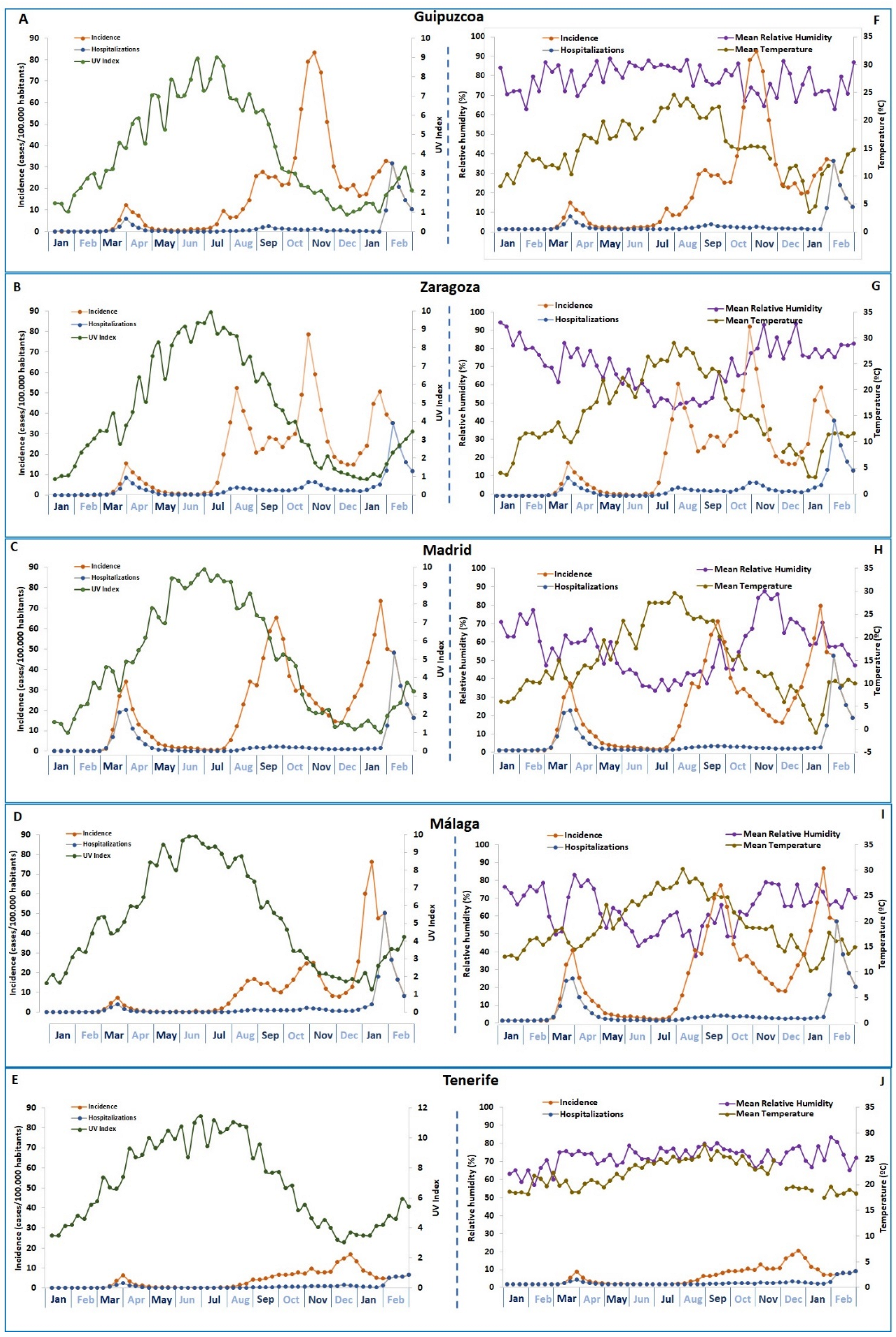
3.1. Description of Meteorological and COVID-19 Variables
3.2. Correlation between COVID-19 and UVI
3.3. Correlation between COVID-19 and Temperature
3.4. Correlation between COVID-19 and Relative Humidity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.-H.; Lai, W.-Y.; Lin, Y.-Y.; Luo, Y.-H.; Chen, H.-K.; Chen, Y.-M.; Lai, Y.-C.; Kuo, L.-C.; Chen, S.-D.; Chang, K.-J.; et al. Clinical manifestation and disease progression in COVID-19 infection. J. Chin. Med. Assoc. 2021, 84, 3–8. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Map-Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 1 November 2020).
- Meselson, M. Droplets and Aerosols in the Transmission of SARS-CoV-2. N. Engl. J. Med. 2020, 382, 2063. [Google Scholar] [CrossRef] [PubMed]
- Stadnytskyi, V.; Bax, C.E.; Bax, A.; Anfinrud, P. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc. Natl. Acad. Sci. USA 2020, 117, 11875–11877. [Google Scholar] [CrossRef] [PubMed]
- Mead, M.N. Benefits of sunlight: A bright spot for human health. Environ. Health Perspect. 2018, 116, 160–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef]
- Mercola, J.; Grant, W.B.; Wagner, C.L. Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity. Nutrients 2020, 12, 3361. [Google Scholar] [CrossRef]
- Corrêa, T.Q.; Blanco, K.C.; Vollet-Filho, J.D.; Moais, V.S.; Trevelin, W.R.; Pratavieira, S.; Bagnato, V.S. Efficiency of an air circulation decontamination device for micro-organisms using ultraviolet radiation. J. Hosp. Infect. 2021, 115, 32–43. [Google Scholar] [CrossRef]
- Herman, J.; Biegel, B.; Huang, L. Inactivation times from 290 to 315 nm UVB in sunlight for SARS coronaviruses CoV and CoV-2 using OMI satellite data for the sunlit Earth. Air Qual. Atmos Health 2021, 14, 217–233. [Google Scholar] [CrossRef]
- Hobday, R.; Collignon, P. An Old Defence Against New Infections: The Open-Air Factor and COVID-19. Cureus 2022, 14, E26133. [Google Scholar] [CrossRef]
- Tang, L.; Liu, M.; Ren, B.; Wu, Z.; Yu, X.; Peng, C.; Tian, J. Sunlight ultraviolet radiation dose is negatively correlated with the percent positive of SARS-CoV-2 and four other common human coronaviruses in the U.S. Sci. Total Environ. 2021, 751, 141816. [Google Scholar] [CrossRef] [PubMed]
- Isaia, G.; Diémoz, H.; Maluta, F.; Fountoulakis, I.; Ceccon, D.; di Sarra, A.; Facta, S.; Fedele, F.; Lorenzetto, G.; Siani, A.M.; et al. Does solar ultraviolet radiation play a role in COVID-19 infection and deaths? An environmental ecological study in Italy. Sci. Total Environ. 2021, 757, 143757. [Google Scholar] [CrossRef]
- Lansiaux, É.; Pébaÿ, P.P.; Picard, J.L.; Forget, J. COVID-19 and vit-d: Disease mortality negatively correlates with sunlight exposure. Spat. Spatio Temporal Epidemiol. 2020, 35, 100362. [Google Scholar] [CrossRef] [PubMed]
- Nicastro, F.; Sironi, G.; Antonello, E.; Bianco, A.; Biasin, M.; Brucato, J.R.; Ermolli, I.; Pareschi, G.; Salvati, M.; Tozzi, P.; et al. Solar UV-B/A radiation is highly effective in inactivating SARS-CoV-2. Sci. Rep. 2021, 11, 14805. [Google Scholar] [CrossRef]
- Biasin, M.; Strizzi, S.; Bianco, A.; Macchi, A.; Utyro, O.; Pareschi, G.; Loffreda, A.; Cavalleri, A.; Lualdi, M.; Trabattoni, D.; et al. UV and violet light can Neutralize SARS-CoV-2 Infectivity. J. Photochem. Photobiol. 2022, 10, 100107. [Google Scholar] [CrossRef]
- Gies, P.; van Deventer, E.; Green, A.C.; Sinclair, C.; Tinker, R. Review of the Global Solar UV Index 2015 Workshop Report. Health Phys. 2018, 114, 84–90. [Google Scholar] [CrossRef] [Green Version]
- ISO/CIE 17166:2019; Erythema Reference Action Spectrum and Standard Erythema Dose. International Commission on Illumination: Vienna, Austria, 2019.
- Setlow, R.B. The wavelengths in sunlight effective in producing skin cancer: A theoretical analysis. Proc. Natl. Acad. Sci. USA 1974, 71, 3363–3366. [Google Scholar] [CrossRef] [Green Version]
- Bernhard, G.; Mayer, B.; Seckmeyer, G.; Moise, A. Measurements of spectral solar UV irradiance in tropical Australia. J. Geophys. Res. Atmos. 1997, 102, 8719–8730. [Google Scholar] [CrossRef]
- Gies, P.; Roy, C.; Javorniczky, J.; Henderson, S.; Lemus-Deschamps, L.; Driscoll, C. Global Solar UV Index: Australian measurements, forecasts and comparison with the UK. Photochem. Photobiol. 2004, 79, 32–39. [Google Scholar] [CrossRef]
- Herman, J.; Piacentini, R.D. UVB (290–315 nm) inactivation of the SARS-CoV-2 virus as a function of the standard UV index. Air Qual. Atmos. Health 2022, 15, 85–90. [Google Scholar] [CrossRef]
- Nandin de Carvalho, H. Latitude impact on pandemic Sars-CoV-2 2020 outbreaks and possible utility of UV indexes in predictions of regional daily infections and deaths. J. Photochem. Photobiol. 2022, 10, 100108. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Biological Effects of Sunlight, Ultraviolet Radiation, Visible Light, Infrared Radiation and Vitamin D for Health. Anticancer Res. 2016, 36, 1345–1356. [Google Scholar] [PubMed]
- Lv, Q.; Liu, M.; Qi, F.; Gong, S.; Zhou, S.; Zhan, S.; Bao, L. Sensitivity of SARS-CoV-2 to different temperatures. Anim. Model. Exp. Med. 2020, 3, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Jing, W.; Liu, J.; Ma, Q.; Yuan, J.; Wang, Y.; Du, M.; Liu, M. Effects of temperature and humidity on the daily new cases and new deaths of COVID-19 in 166 countries. Sci. Total Environ. 2020, 729, 139051. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwartencluded, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Linton, N.M.; Kobayashi, T.; Yang, Y.; Hayashi, K.; Akhmetzhanov, A.R.; Jung, S.M.; Yuan, B.; Kinoshita, R.; Nishiura, H. Incubation Period and Other Epidemiological Characteristics of 2019 Novel Coronavirus Infections with Right Truncation: A Statistical Analysis of Publicly Available Case Data. J. Clin. Med. 2020, 9, 538. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Walrand, S. Autumn COVID-19 surge dates in Europe correlated to latitudes, not to temperature-humidity, pointing to vitamin D as contributing factor. Sci. Rep. 2021, 11, 1981. [Google Scholar] [CrossRef]
- Ganasegeran, K.; Fadzly, M.F., 1st; wee Hock Ch’ng, A.S.; Looi, I.; Peariasamy, K.M. Influence of Population Density for COVID-19 Spread in Malaysia: An Ecological Study. Int. J. Environ. Res. Public Health 2021, 18, 9866. [Google Scholar] [CrossRef]
- Paez, A.; Lopez, F.A.; Menezes, T.; Cavalcanti, R.; Pitta, M.G.D.R. A Spatio-Temporal Analysis of the Environmental Correlates of COVID-19 Incidence in Spain. Geogr. Anal. 2020, 53, 397–421. [Google Scholar] [CrossRef]
- Xu, R.; Rahmandad, H.; Gupta, M.; DiGennaro, C.; Ghaffarzadegan, N.; Amini, H.; Jalali, M.S. Weather, air pollution, and SARS-CoV-2 transmission: A global analysis. Lancet Planet Health 2021, 5, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Cacho, P.M.; Hernánde, Z.J.L.; López-Hoyos, M.; Martínez-Taboada, V.M. Can meteorological factors explain the differences in COVID-19 incidence and severity across the Spanish regions? An ecological study. Environ. Health 2020, 19, 106. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Tang, K.; Feng, K.; Lin, X.; Lv, W.; Chen, K.; Wang, F. Impact of temperature and relative humidity on the transmission of COVID-19: A modelling study in China and the United States. BMJ Open 2021, 11, e043863. [Google Scholar] [CrossRef] [PubMed]
- Sharma, G.D.; Bansal, S.; Yadav, A.; Jain, M.; Garg, I. Meteorological factors, COVID-19 cases, and deaths in top 10 most affected countries: An econometric investigation. Environ. Sci. Pollut. Res. 2021, 28, 28624–28639. [Google Scholar] [CrossRef]
- He, Z.; Chin, Y.; Yu, S.; Huang, J.; Zhang, C.J.P.; Zhu, K.; Azarakhsh, N.; Sheng, J.; He, Y.; Jayavanth, P.; et al. The Influence of Average Temperature and Relative Humidity on New Cases of COVID-19: Time-Series Analysis. JMIR Public Health Surveill. 2021, 7, e20495. [Google Scholar] [CrossRef] [PubMed]
- Panigrahi, A.; Mohapatra, I.; Kanyari, S.S.; Maharana, S.; Panigrahi, M. Impact of environmental temperature and relative humidity on spread of COVID-19 infection in India: A cross-sectional time-series analysis. Arch. Environ. Occup. Health 2021, 77, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Mozumder, M.S.I.; Amin, M.S.A.; Uddin, M.R.; Talukder, M.J. Coronavirus COVID-19 outbreak and control: Effect of temperature, relative humidity, and lockdown implementation. Arch. Pediatr. 2021, 28, 111–116. [Google Scholar] [CrossRef]
- Jain, M.; Sharma, G.D.; Goyal, M.; Kaushal, R.M.; Sethi, M. Econometric analysis of COVID-19 cases, deaths, and meteorological factors in South Asia. Environ. Sci. Pollut. Res. 2021, 28, 28518–28534. [Google Scholar] [CrossRef]
- Schuit, M.; Ratnesar-Shumate, S.; Yolitz, J.; Williams, G.; Weaver, W.; Green, B.; Miller, D.; Krause, M.; Beck, K.; Wood, S.; et al. Airborne SARS-CoV-2 Is Rapidly Inactivated by Simulated Sunlight. J. Infect. Dis. 2020, 222, 564–571. [Google Scholar] [CrossRef]
- Biryukov, J.; Boydston, J.A.; Dunning, R.A.; Yeager, J.J.; Wood, S.; Reese, A.L.; Ferris, A.; Miller, D.; Weaver, W.; Zeitouni, N.E.; et al. Increasing Temperature and Relative Humidity Accelerates Inactivation of SARS-CoV-2 on Surfaces. mSphere 2020, 5, e00441-20. [Google Scholar] [CrossRef]
- Bruno, R.R.; Wernly, B.; Masyuk, M.; Muessig, J.M.; Schiffner, R.; Bäz, L.; Schulze, C.; Franz, M.; Kelm, M.; Jung, C. No impact of weather conditions on the outcome of intensive care unit patients. Wien. Med. Wochenschr. 2021, 172, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Li, S.; Yu, H.; Wang, P.; Zhang, Y.; Chen, Z.; Li, Y.; Cheng, L.; Li, W.; Jia, H.; et al. Epidemiological, comorbidity factors with severity and prognosis of COVID-19: A systematic review and meta-analysis. Aging 2020, 12, 12493–12503. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Xu, J. The association between COVID-19 deaths and short-term ambient air pollution/meteorological condition exposure: A retrospective study from Wuhan, China. Air Qual. Atmos. Health 2020, 14, 1–5. [Google Scholar] [CrossRef]
- Zaazouee, M.S.; Eleisawy, M.; Abdalalaziz, A.M.; Elhady, M.M.; Ali, O.A.; Abdelbari, T.M.; Hasan, S.M.; Almadhoon, H.W.; Ahmed, A.Y.; Fassad, A.S.; et al. Hospital and laboratory outcomes of patients with COVID-19 who received vitamin D supplementation: A systematic review and meta-analysis of randomized controlled trials. Naunyn Schmiedeberg’s Arch. Pharmacol. 2022, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Feiner Solís, Á.; Avedillo Salas, A.; Luesma Bartolomé, M.J.; Santander Ballestín, S. The Effects of Vitamin D Supplementation in COVID-19 Patients: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 12424. [Google Scholar] [CrossRef] [PubMed]
- Martineau, A.R. Vitamin D in the prevention or treatment of COVID-19. Proc. Nutr. Soc. 2022, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, N.; Rafiq, M.; Masooma; Tareen, S.; Ahmad, M.; Nawaz, F.; Khan, S.; Riaz, R.; Yang, T.; Fatima, A.; et al. The SARS-CoV-2 differential genomic adaptation in response to varying UVindex reveals potential genomic resources for better COVID-19 diagnosis and prevention. Front. Microbiol. 2022, 13, 922393. [Google Scholar] [CrossRef]


{kind=link}
| Guipuzcoa | Zaragoza | Madrid | Málaga | Tenerife | ||
|---|---|---|---|---|---|---|
| Mean UV Index | ||||||
| 2020 | Winter | 2.6 | 2.5 | 2.9 | 3.5 | 5.4 |
| Spring | 6.8 | 7.6 | 7.9 | 8.0 | 9.9 | |
| Summer | 6.5 | 7.3 | 7.7 | 7.9 | 9.6 | |
| Autumn | 1.8 | 2.0 | 2.4 | 2.9 | 4.6 | |
| 2021 | Winter | 2.0 | 2.0 | 2.2 | 2.8 | 4.5 |
| Mean (SD) | 4.0 (2.5) | 4.3 (2.9) | 4.6 (2.9) | 5.0 (2.7) | 5.0 (2.7) | |
| Mean temperature (°C) | ||||||
| 2020 | Winter | 11.5 | 9.7 | 9.8 | 15.4 | 19.7 |
| Spring | 17.6 | 19.3 | 18.4 | 20.8 | 21.9 | |
| Summer | 21.7 | 24.9 | 24.9 | 26.7 | 25.4 | |
| Autumn | 13.3 | 12.0 | 11.1 | 17.5 | 22.3 | |
| 2021 | Winter | 10.4 | 9.0 | 6.9 | 14.0 | 18.6 |
| Mean (SD) | 14.9 (4.7) | 15.0 (6.9) | 14.2 (7.3) | 18.9 (5.1) | 21.6 (2.6) | |
| Mean Relative Humidity (%) | ||||||
| 2020 | Winter | 76.9 | 79.4 | 63.1 | 69.2 | 67.1 |
| Spring | 81.9 | 67.3 | 50.4 | 59.9 | 72.1 | |
| Summer | 81.8 | 52.7 | 41.9 | 54.4 | 76.4 | |
| Autumn | 74.8 | 78.8 | 70.5 | 68.4 | 72.9 | |
| 2021 | Winter | 74.9 | 78.8 | 57.7 | 70.4 | 73.9 |
| Mean (SD) | 78.4 (3.6) | 71.4 (11.6) | 56.4 (11.1) | 64.5 (7.0) | 72.5 (3.4) | |
| COVID-19 Incidence (number of cases/100,000 habitants) | ||||||
| 2020 | Winter | 1.59 | 1.89 | 6.05 | 1.14 | 0.91 |
| Spring | 2.20 | 2.96 | 5.51 | 0.74 | 0.69 | |
| Summer | 14.86 | 25.91 | 27.91 | 8.37 | 2.57 | |
| Autumn | 42.44 | 33.09 | 24.61 | 15.07 | 9.97 | |
| 2021 | Winter | 22.57 | 30.60 | 42.89 | 38.91 | 6.12 |
| Mean (SD) | 16.73 (16.9) | 18.89 (15.3) | 21.39 (15.8) | 12.84 (15.7) | 4.05 (4.0) | |
| COVID-19 Hospitalizations (number cases/100,000 habitants) | ||||||
| 2020 | Winter | 0.75 | 1.05 | 4.07 | 0.67 | 0.42 |
| Spring | 0.52 | 1.18 | 2.11 | 0.24 | 0.26 | |
| Summer | 0.80 | 2.24 | 1.15 | 0.54 | 0.24 | |
| Autumn | 0.63 | 3.32 | 1.33 | 1.13 | 0.92 | |
| 2021 | Winter | 10.92 | 13.75 | 17.00 | 15.92 | 3.25 |
| Mean (SD) | 2.73 (4.6) | 4.31 (5.4) | 5.13 (6.7) | 3.70 (6.8) | 1.02 (1.3) | |
| COVID-19 Intensive Care Units patients (number cases/100,000 habitants) | ||||||
| 2020 | Winter | 0.07 | 0.16 | 0.33 | 0.08 | 0.08 |
| Spring | 0.02 | 0.13 | 0.17 | 0.02 | 0.03 | |
| Summer | 0.09 | 0.11 | 0.06 | 0.05 | 0.05 | |
| Autumn | 0.08 | 0.29 | 0.07 | 0.08 | 0.14 | |
| 2021 | Winter | 0.01 | 0.32 | 0.16 | 0.27 | 0.12 |
| Mean (SD) | 0.05 (0.04) | 0.20 (0.10) | 0.16 (0.11) | 0.10 (0.10) | 0.08 (0.05) | |
| COVID-19 Deaths (number cases/100,000 habitants) | ||||||
| 2020 | Winter | 0.08 | 0.15 | 0.55 | 0.07 | 0.04 |
| Spring | 0.38 | 0.65 | 0.81 | 0.11 | 0.08 | |
| Summer | 0.12 | 0.44 | 0.18 | 0.07 | 0.02 | |
| Autumn | 0.70 | 0.94 | 0.33 | 0.25 | 0.14 | |
| 2021 | Winter | 0.39 | 0.65 | 0.44 | 0.59 | 0.14 |
| Mean (SD) | 0.39 (0.29) | 0.56 (0.33) | 0.46 (0.27) | 0.22 (0.09) | 0.08 (0.05) | |
| Cases | Hospitalized | ICU-Admitted | Deaths | |
|---|---|---|---|---|
| /100,000 inh. | /100,000 inh. | /100,000 inh. | /100,000 inh. | |
| GUIPUZCOA | −0.242 p < 0.001 | N.S. | N.S. | −0.302 p < 0.001 |
| ZARAGOZA | −0.111 p = 0.02 | −0.201 p < 0.001 | −0.174 p < 0.001 | −0.219 p < 0.001 |
| MADRID | −0.188 p < 0.001 | −0.144 p = 0.005 | N.S. | N.S. |
| MÁLAGA | −0.362 p < 0.001 | −0.333 p < 0.001 | N.S. | −0.264 p < 0.001 |
| TENERIFE | −0.456 p < 0.001 | −0.374 p < 0.001 | N.S. | N.S. |
| Cases /100,000 inh. | Hospitalized /100,000 inh. | ICU-Admitted /100,000 inh. | Deaths /100,000 inh. | |
|---|---|---|---|---|
| GIPUZCOA | N.S. | 0.138 p = 0.007 | N.S. | −0.291 p < 0.001 |
| ZARAGOZA | 0.105 p = 0.031 | N.S. | −0.173 p < 0.001 | −0.116 p = 0.019 |
| MADRID | N.S. | N.S. | N.S. | N.S. |
| MÁLAGA | N.S. | −0.150 p = 0.003 | N.S. | −0.220 p < 0.001 |
| TENERIFE | N.S. | −0.110 p = 0.031 | N.S. | N.S. |
| Cases /100,000 inh. | Hospitalized /100,000 inh. | ICU-Admitted /100,000 inh. | Deaths /100,000 inh. | |
|---|---|---|---|---|
| GIPUZCOA | −0.163 p = 0.001 | N.S. | 0.138 p = 0.005 | −0.115 p = 0.02 |
| ZARAGOZA | −0.168 p = 0.01 | N.S. | 0.131 p = 0.008 | N.S. |
| MADRID | NS | N.S. | N.S. | N.S. |
| MÁLAGA | 0.118 p = 0.015 | N.S. | N.S. | N.S. |
| TENERIFE | 0.191 p < 0.001 | −0.159 p = 0.002 | N.S. | N.S. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Gilaberte, J.B.; Martín-Iranzo, N.; Aguilera, J.; Almenara-Blasco, M.; de Gálvez, M.V.; Gilaberte, Y. Correlation between UV Index, Temperature and Humidity with Respect to Incidence and Severity of COVID 19 in Spain. Int. J. Environ. Res. Public Health 2023, 20, 1973. https://doi.org/10.3390/ijerph20031973
Pérez-Gilaberte JB, Martín-Iranzo N, Aguilera J, Almenara-Blasco M, de Gálvez MV, Gilaberte Y. Correlation between UV Index, Temperature and Humidity with Respect to Incidence and Severity of COVID 19 in Spain. International Journal of Environmental Research and Public Health. 2023; 20(3):1973. https://doi.org/10.3390/ijerph20031973
Chicago/Turabian StylePérez-Gilaberte, Juan Blas, Natalia Martín-Iranzo, José Aguilera, Manuel Almenara-Blasco, María Victoria de Gálvez, and Yolanda Gilaberte. 2023. "Correlation between UV Index, Temperature and Humidity with Respect to Incidence and Severity of COVID 19 in Spain" International Journal of Environmental Research and Public Health 20, no. 3: 1973. https://doi.org/10.3390/ijerph20031973