
Older Adults Who Maintained a Regular Physical Exercise Routine before the Pandemic Show Better Immune Response to Vaccination for COVID-19
 , ,
, ,  , ,
, ,  , , ,
, , ,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
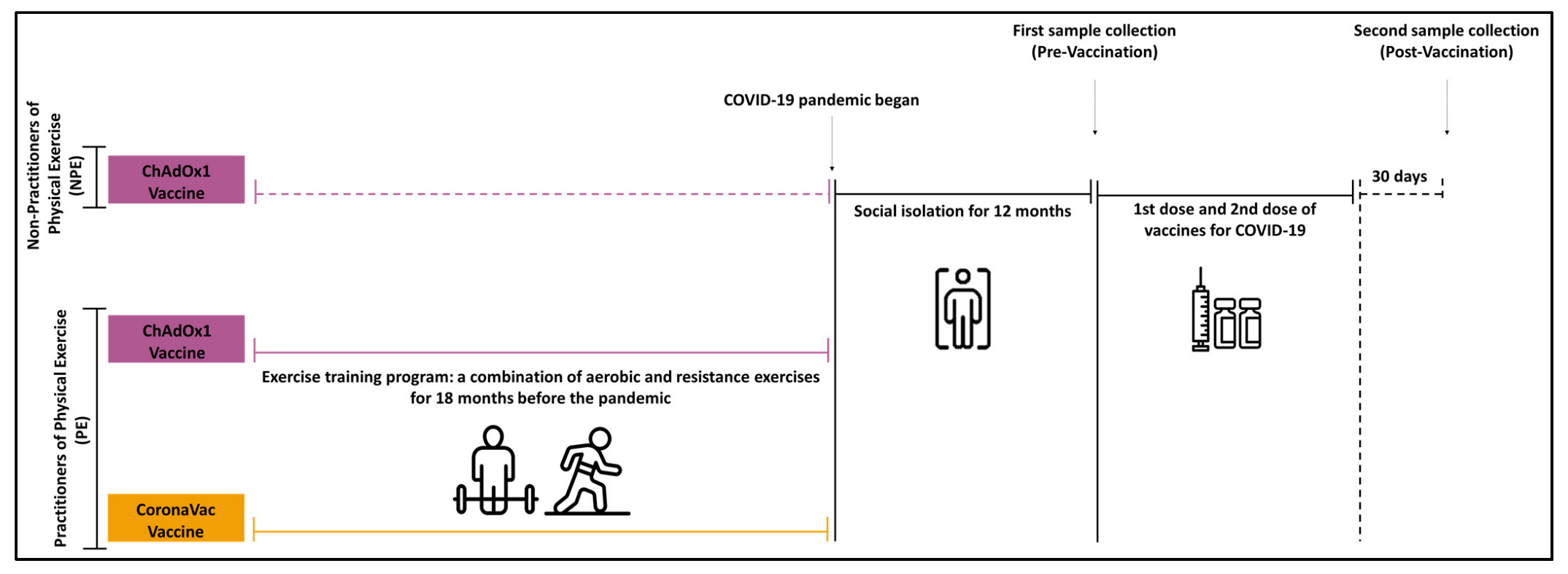
2.1. Study Design
2.2. Ethical Statement
2.3. Participants’ Selection Criteria
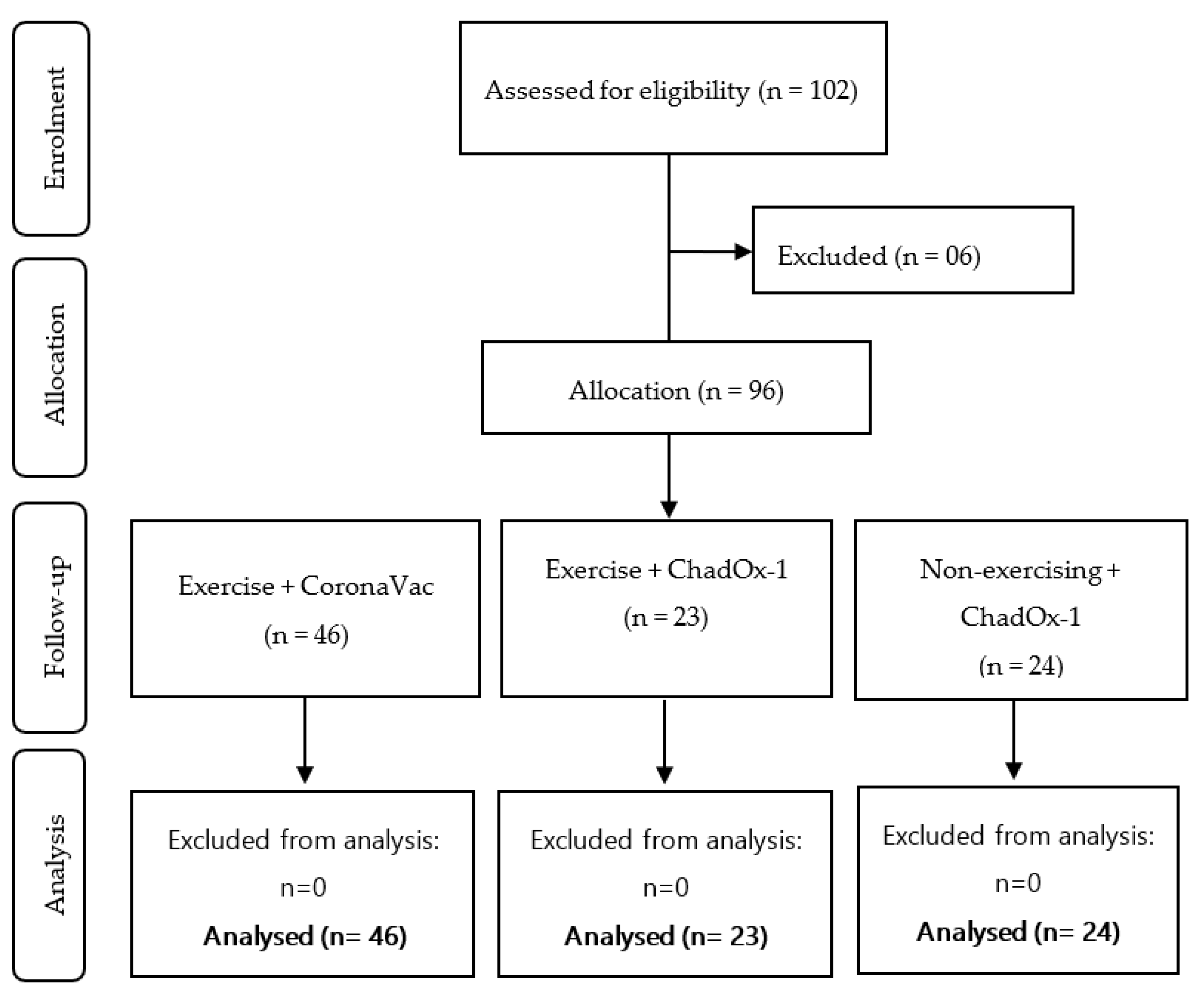
Sample Size Calculation and Experimental Groups
2.4. Exercise Intervention Protocol
2.5. Vaccination for COVID-19
2.6. Blood Sample Collection
2.7. Determination of Specific Antibodies (IgA and IgG) for the SARS-CoV-2 Antigens
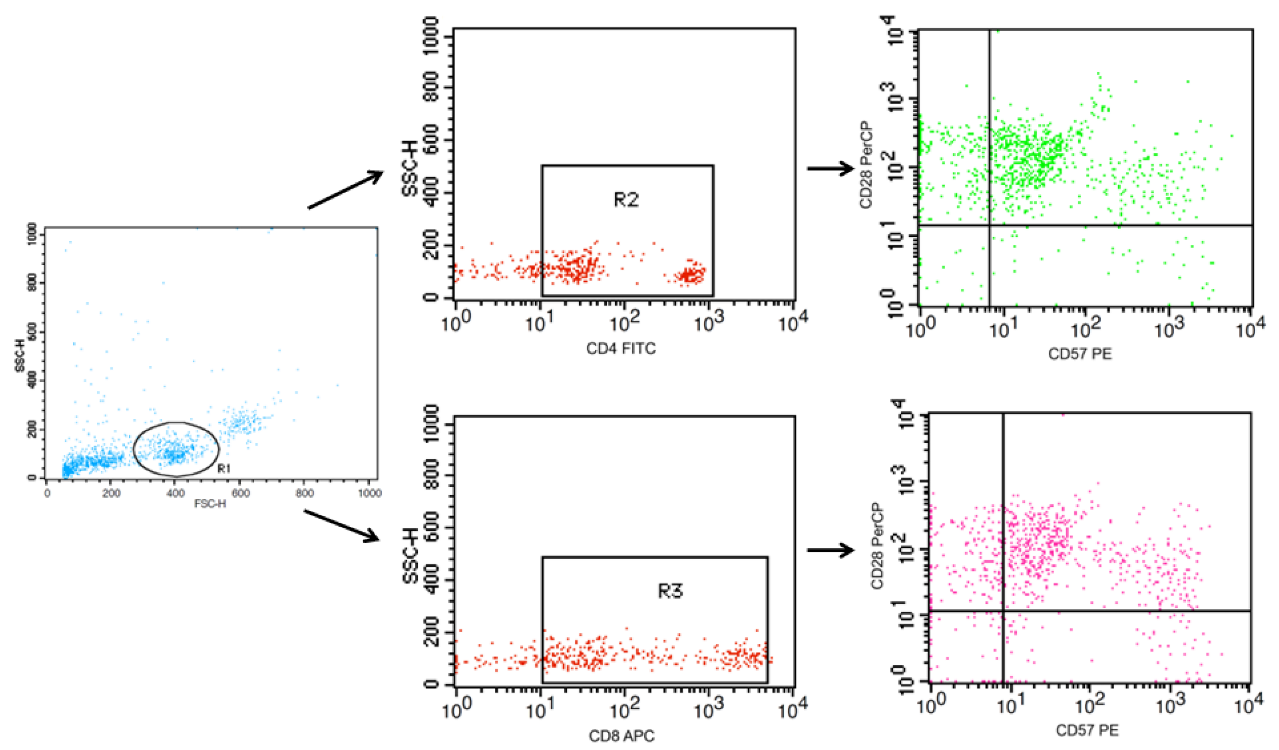
2.8. Immunophenotyping of T Cells
3. Statistical Analysis
4. Results
4.1. Sample Characterization
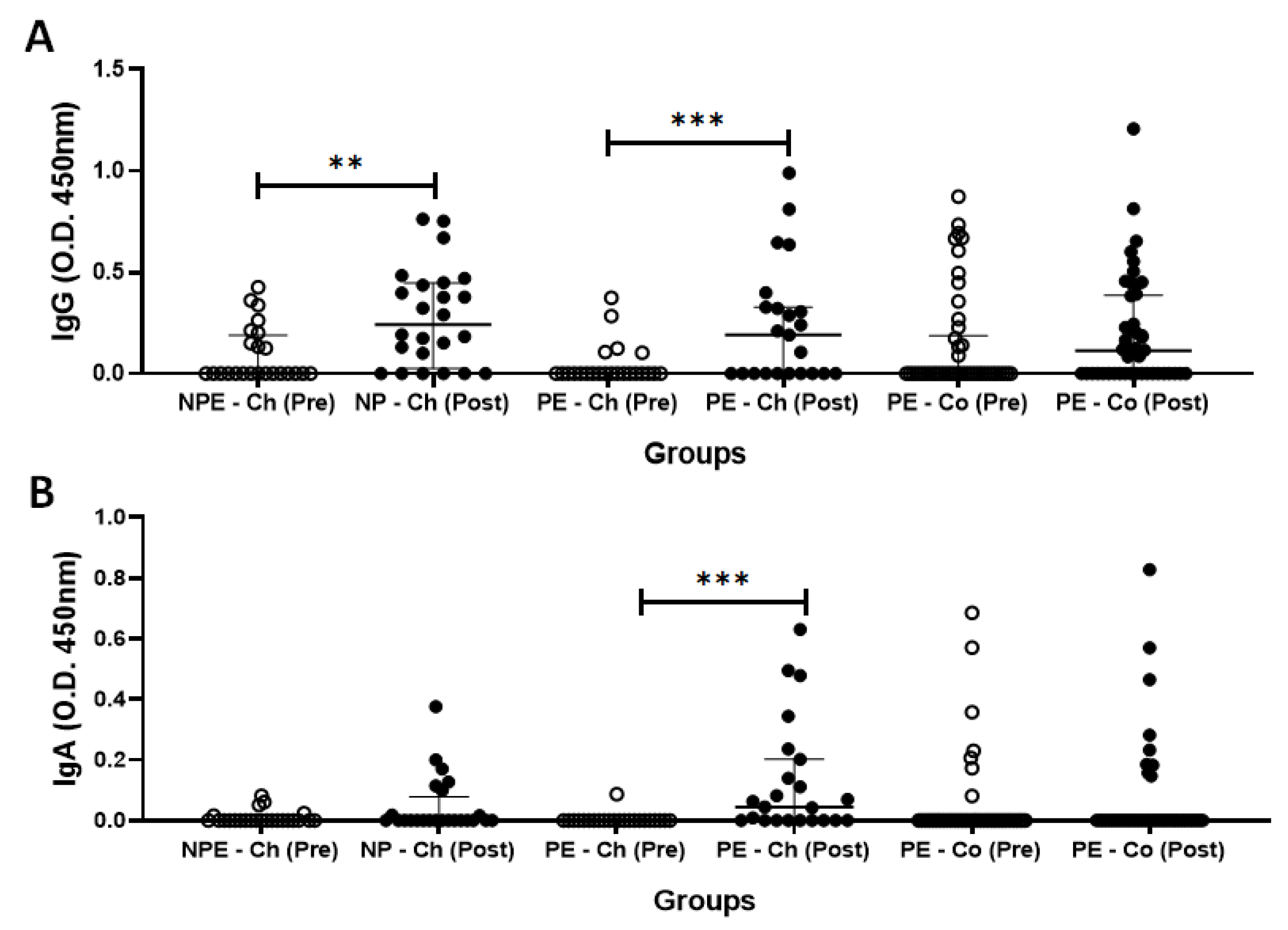
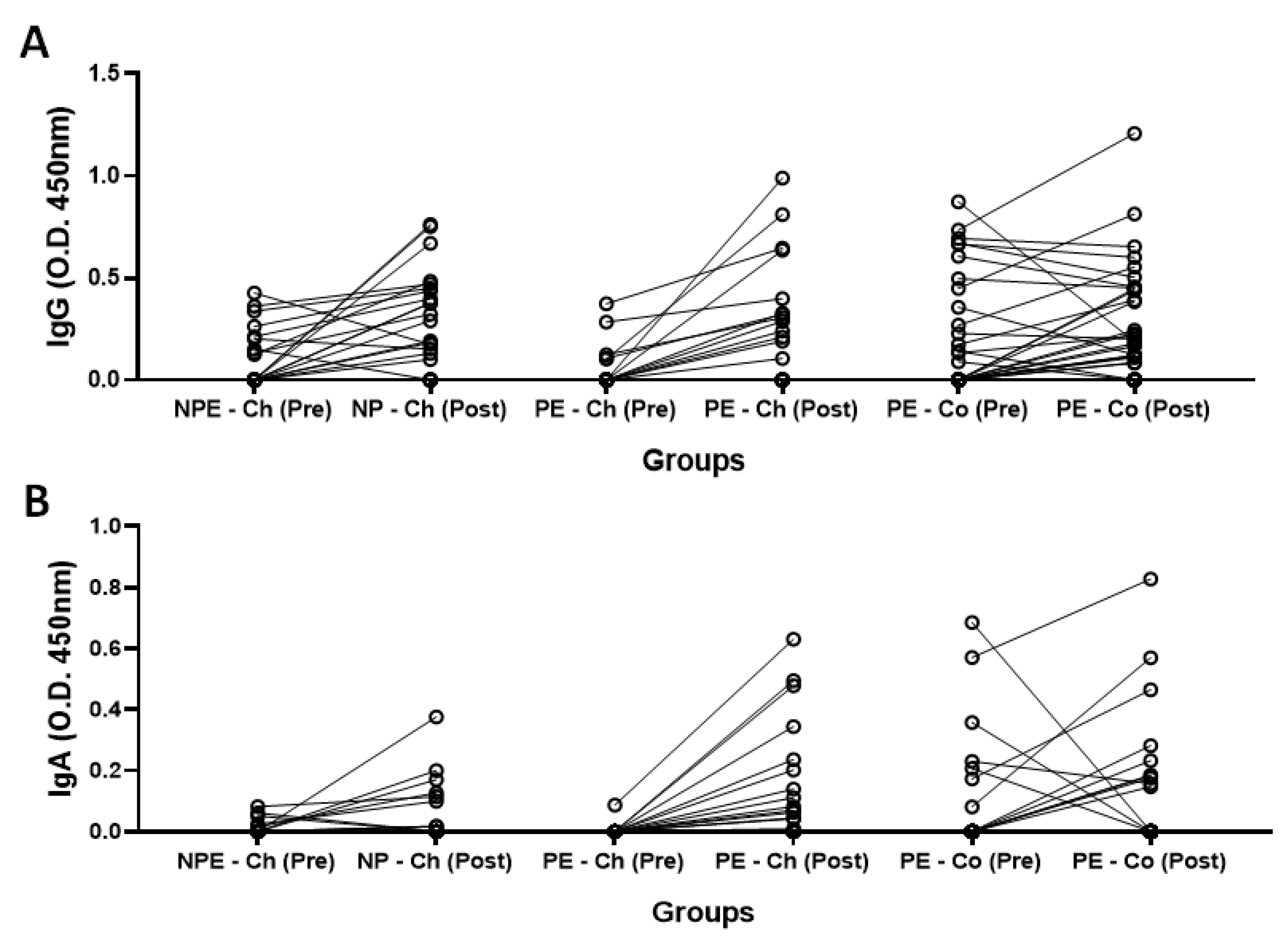
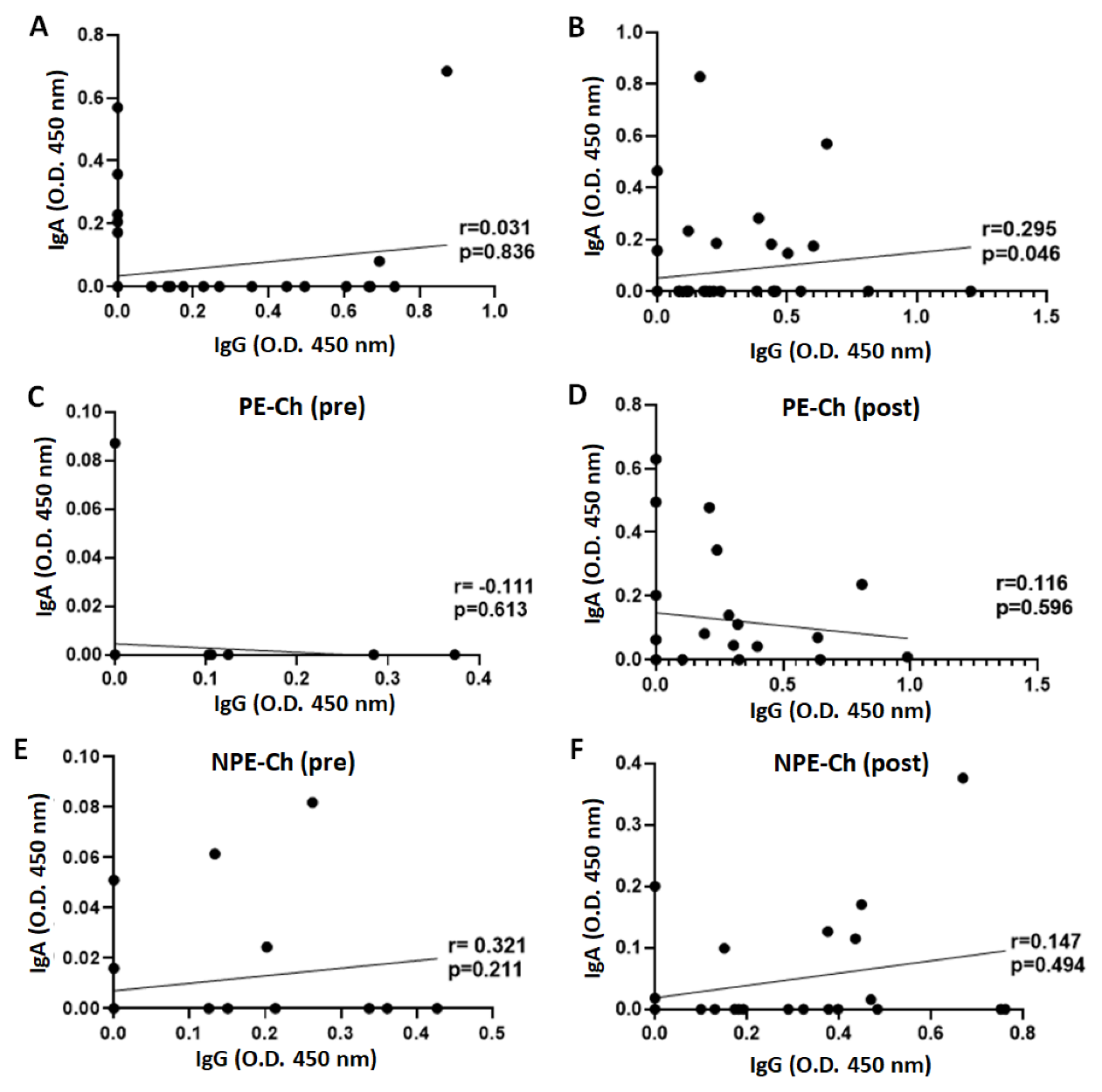
4.2. Specific Antibodies of (IgA and IgG) for the SARS-CoV-2 Antigens
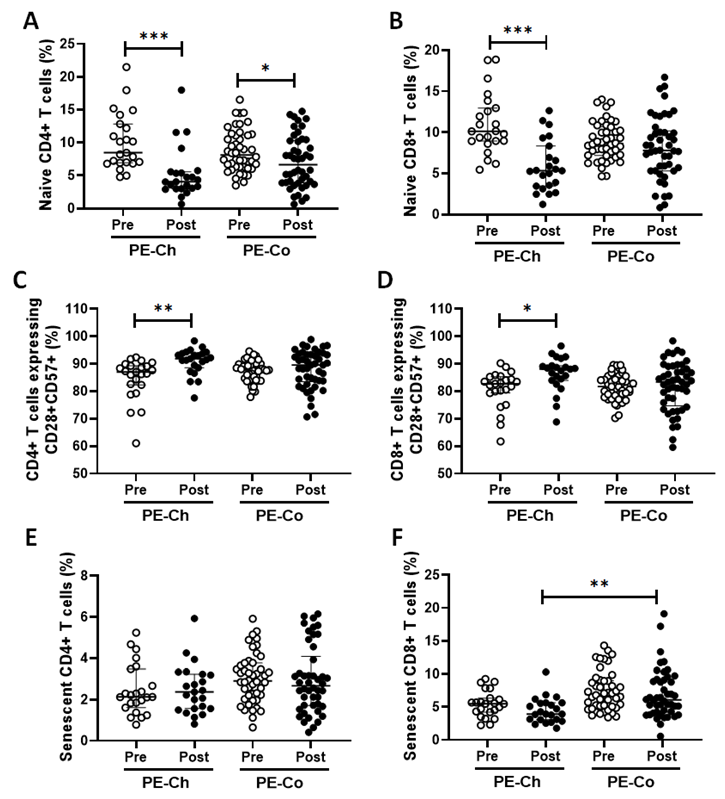
4.3. Immunophenotyping of T Cells
5. Discussion
6. Limitations of the Study
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, W.; Javed, S.; Bratty, M.A.; Alhazmi, H.A.; Najmi, A. Treatment of SARS-CoV-2: How far have we reached? Drug Discov. Ther. 2020, 14, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Khan, A.; Banjer, H.J.; Alzahrani, F.M.; Parvez, A.K.; Dey, S.K. Genomic surveillance, evolution and global transmission of SARS-CoV-2 during 2019–2022. PLoS One 2022, 17, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Bian, L.; Gao, Q.; Gao, F.; Wang, Q.; He, Q.; Wu, X.; Mao, Q.; Xu, M.; Liang, Z. Impact of the Delta variant on vaccine efficacy and response strategies. Expert Rev. Vaccines 2021, 201, 201–1209. [Google Scholar] [CrossRef] [PubMed]
- Joachim, L.; Schultze; Anna, C. Aschenbrenner COVID-19 and the human innate immune system. Cell 2021, 184, 19–21. [Google Scholar]
- Li, H.; Lu, W.; Li, Y.; Lu, Y.; Li, F. Reviewing immunopathology characteristics of SARS-CoV-2 for cancer entwisted with SARS-CoV-2. SAGE Open Med. 2021, 9, 205031212198950. [Google Scholar] [CrossRef]
- Abd El-Kader, S.M.; Al-Shreef, F.M. Inflammatory cytokines and immune system modulation by aerobic versus resisted exercise training for elderly. Afr. Health Sci. 2018, 18, 120–131. [Google Scholar] [CrossRef] [Green Version]
- Aw, D.; Silva, A.B.; Palmer, D.B. Immunosenescence: Emerging challenges for an ageing population. Immunology 2007, 120, 435–446. [Google Scholar] [CrossRef]
- Wong, G.C.L.; Strickland, M.C.; Larbi, A. Changes in T Cell Homeostasis and Vaccine Responses in Old Age. Interdiscip. Top. Gerontol. Geriatr. 2020, 43, 36–55. [Google Scholar] [CrossRef]
- Teissier, T.; Boulanger, E.; Cox, L.S. Interconnections between Inflammageing and Immunosenescence during Ageing. Cells 2022, 11, 359. [Google Scholar] [CrossRef]
- Shao, T.; Verma, H.K.; Pande, B.; Costanzo, V.; Ye, W.; Cai, Y.; Bhaskar, L.V.K.S. Physical Activity and Nutritional Influence on Immune Function: An Important Strategy to Improve Immunity and Health Status. Front. Physiol. 2021, 12, 751374. [Google Scholar] [CrossRef]
- Kohut, M.L.; Cooper, M.M.; Nickolaus, M.S.; Russell, D.R.; Cunnick, J.E. Exercise and psychosocial factors modulate immunity to influenza vaccine in elderly individuals. J. Gerontol.—Ser. A Biol. Sci. Med. Sci. 2002, 57, 557–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anjos, M.C.G.d.; Passos, L.F.d.S.; Malheiro, A. Efeitos do condicionamento físico sobre a imunossenescência. Geriatr. Gerontol. Aging 2013, 7, 60–67. [Google Scholar]
- Barrett, B.; Hayney, M.S.; Muller, D.; Rakel, D.; Ward, A.; Obasi, C.N.; Brown, R.; Zhang, Z.; Zgierska, A.; Gern, J.; et al. Meditation or exercise for preventing acute respiratory infection: A randomized controlled trial. Ann. Fam. Med. 2012, 10, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Chen, Y.; Yu, D.; Mao, D.; Wang, T.; Feng, D.; Li, T.; Yan, S.; Yu, Y. The effects of exercise on COVID-19 therapeutics: A protocol for systematic review and meta-analysis. Medicine 2020, 99, e22345. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C. Exercise Is Medicine for Immune Function: Implication for COVID-19. Curr. Sports Med. Rep. 2021, 20, 395–401. [Google Scholar] [CrossRef]
- Furtado, G.E.; Letieri, R.V.; Caldo-Silva, A.; Sardão, V.A.; Teixeira, A.M.; de Barros, M.P.; Vieira, R.P.; Bachi, A.L.L. Sustaining efficient immune functions with regular physical exercise in the COVID-19 era and beyond. Eur. J. Clin. Investig. 2021, 51, e13485. [Google Scholar] [CrossRef]
- Ranasinghe, C.; Ozemek, C.; Arena, R. Exercise and well-being during COVID 19—Time to boost your immunity. Expert Rev. Anti-Infective Ther. 2020, 18, 1195–1200. [Google Scholar] [CrossRef]
- Constandt, B.; Thibaut, E.; De Bosscher, V.; Scheerder, J.; Ricour, M.; Willem, A. Exercising in times of lockdown: An analysis of the impact of COVID-19 on levels and patterns of exercise among adults in Belgium. Int. J. Environ. Res. Public Health 2020, 17, 4144. [Google Scholar] [CrossRef]
- Hallam, J.; Jones, T.; Alley, J.; Kohut, M.L. Exercise after influenza or COVID-19 vaccination increases serum antibody without an increase in side effects. Brain Behav. Immun. 2022, 102, 1–10. [Google Scholar] [CrossRef]
- Scudiero, O.; Lombardo, B.; Brancaccio, M.; Mennitti, C.; Cesaro, A.; Fimiani, F.; Gentile, L.; Moscarella, E.; Amodio, F.; Ranieri, A.; et al. Exercise, Immune System, Nutrition, Respiratory and Cardiovascular Diseases during COVID-19: A Complex Combination. Int. J. Environ. Res. Public Health 2021, 18, 904. [Google Scholar] [CrossRef] [PubMed]
- Bohn-Goldbaum, E.; Owen, K.B.; Lee, V.Y.J.; Booy, R.; Edwards, K.M. Physical activity and acute exercise benefit influenza vaccination response: A systematic review with individual participant data metaanalysis. PLoS One 2022, 17, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 international online survey. Nutrients 2020, 12, 13. [Google Scholar] [CrossRef]
- Brancaccio, M.; Mennitti, C.; Gentile, A.; Correale, L.; Buzzachera, C.F.; Ferraris, C.; Montomoli, C.; Frisso, G.; Borrelli, P.; Scudiero, O. Effects of the COVID-19 Pandemic on Job Activity, Dietary Behaviours and Physical Activity Habits of University Population of Naples, Federico II-Italy. Int. J. Environ. Res. Public Health 2021, 18, 1502. [Google Scholar] [CrossRef] [PubMed]
- Woods, J.A.; Keylock, K.T.; Lowder, T.; Vieira, V.J.; Zelkovich, W.; Dumich, S.; Colantuano, K.; Lyons, K.; Leifheit, K.; Cook, M.; et al. Cardiovascular exercise training extends influenza vaccine seroprotection in sedentary older adults: The immune function intervention trial. J. Am. Geriatr. Soc. 2009, 57, 2183–2191. [Google Scholar] [CrossRef] [PubMed]
- Naik, S. Immunosenescence and Exercise-Mediated Modulation of the Innate Immune Response to Influenza Infection in Mice; Kinesiology, Iowa State University: Ames, IA, USA, 2013. [Google Scholar]
- Bachi, A.L.L.L.; Suguri, V.M.; Ramos, L.R.; Mariano, M.; Vaisberg, M.; Lopes, J.D. Increased production of autoantibodies and specific antibodies in response to influenza virus vaccination in physically active older individuals. Results Immunol. 2013, 3, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, F.R.; Roseira, T.; Amaral, J.B.; Paixão, V.; Almeida, E.B.; Foster, R.; Sperandio, A.; Rossi, M.; Amirato, G.R.; Apostólico, J.S.; et al. Combined Exercise Training and l-Glutamine Supplementation Enhances Both Humoral and Cellular Immune Responses after Influenza Virus Vaccination in Elderly Subjects. Vaccines 2020, 8, 685. [Google Scholar] [CrossRef]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing COVID-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zeng, H.; Gu, J.; Li, H.; Zheng, L.; Zou, Q. Progress and prospects on vaccine development against SARS-CoV-2. Vaccines 2020, 8, 153. [Google Scholar] [CrossRef] [Green Version]
- Zhou, D.; Borsa, M.; Simon, A.K. Hallmarks and detection techniques of cellular senescence and cellular ageing in immune cells. Aging Cell 2021, 20, e13316. [Google Scholar] [CrossRef]
- Lu, L.; Mok, B.W.Y.; Chen, L.L.; Chan, J.M.C.; Tsang, O.T.Y.; Lam, B.H.S.; Chuang, V.W.M.; Chu, A.W.H.; Chan, W.M.; Ip, J.D.; et al. Neutralization of Severe Acute Respiratory Syndrome Coronavirus 2 Omicron Variant by Sera From BNT162b2 or CoronaVac Vaccine Recipients. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 75, e822–e826. [Google Scholar] [CrossRef] [PubMed]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: The TREND statement. Am. J. Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef] [PubMed]
- de Lima, S.G.; de Lima, T.A.G.; de Macedo, L.A.; Sá, M.P.; Vidal, M.L.; Gomes, A.F.; Oliveira, L.C.; Santos, A.M. Ethics in Research with Human Beings: From Knowledge to Practice. Arq. Bras. Cardiol. 2010, 95, 289–294. [Google Scholar]
- Shephard, R.J. Ethics in exercise science research. Sports Med. 2002, 32, 169–183. [Google Scholar] [CrossRef]
- Petrini, C. Helsinki 50 years on. Clin. Ter. 2014, 165, 179–181. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Picorelli, A.M.A.; Pereira, L.S.M.; Pereira, D.S.; Felício, D.; Sherrington, C. Adherence to exercise programs for older people is influenced by program characteristics and personal factors: A systematic review. J. Physiother. 2014, 60, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Bachi, A.L.L.; Barros, M.P.; Vieira, R.P.; Rocha, G.A.; de Andrade, P.B.M.; Victorino, A.B.; Ramos, L.R.; Gravina, C.F.; Lopes, J.D.; Vaisberg, M.; et al. Combined Exercise Training Performed by Elderly Women Reduces Redox Indexes and Proinflammatory Cytokines Related to Atherogenesis. Oxid. Med. Cell Longev. 2019, 2019, 6469213. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, J.d.M.B.; do Amaral, J.B.; França, C.N.; Monteiro, F.R.; Alvares-Saraiva, A.M.; Kalil, S.; Durigon, E.L.; Oliveira, D.B.L.; Rodrigues, S.S.; Heller, D.; et al. Distinct Immunological Profiles Help in the Maintenance of Salivary Secretory IgA Production in Mild Symptoms COVID-19 Patients. Front. Immunol. 2022, 13, 890887. [Google Scholar] [CrossRef]
- Bektas, A.; Schurman, S.H.; Sen, R.; Ferrucci, L. Human T cell immunosenescence and inflammation in aging. J. Leukoc. Biol. 2017, 102, 977–988. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, K.; Viboud, C.; Simonsen, L. Antibody response to influenza vaccination in the elderly: A quantitative review. Vaccine 2006, 24, 1159–1169. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Renzo, L.; Gualtieri, P.; Cinelli, G.; Bigioni, G.; Soldati, L.; Attinà, A.; Bianco, F.F.; Caparello, G.; Camodeca, V.; Carrano, E.; et al. Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients 2020, 12, 2152. [Google Scholar] [CrossRef] [PubMed]
- McDowell, C.P.; Herring, M.P.; Lansing, J.; Brower, C.; Meyer, J.D. Working From Home and Job Loss Due to the COVID-19 Pandemic Are Associated with Greater Time in Sedentary Behaviors. Front. Public Health 2020, 8, 597619. [Google Scholar] [CrossRef] [PubMed]
- Malley, R.; Trzcinski, K.; Srivastava, A.; Thompson, C.M.; Anderson, P.W.; Lipsitch, M. CD4+ T cells mediate antibody-independent acquired immunity to pneumococcal colonization. Proc. Natl. Acad. Sci. USA 2005, 102, 4848–4853. [Google Scholar] [CrossRef] [Green Version]
- Weidinger, C.; Hegazy, A.N.; Glauben, R.; Siegmund, B. COVID-19—From Mucosal. Immunol.ogy to IBD patients. Mucosal. Immunol. 2021, 14, 566–573. [Google Scholar] [CrossRef]
- Torow, N.; Marsland, B.J.; Hornef, M.W.; Gollwitzer, E.S. Neonatal Mucosal. Immunol.ogy. Mucosal. Immunol. 2017, 10, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Romero-Pinedo, S.; Quesada, M.; Horndler, L.; Álvarez-Fernández, S.; Olmo, A.; Abia, D.; Alarcón, B.; Delgado, P. Vaccine Type-, Age- and Past Infection-Dependence of the Humoral Response to SARS-CoV-2 Spike S Protein. Front. Immunol. 2022, 13, 1–11. [Google Scholar] [CrossRef]
- Schijns, V.; Lavelle, E.C. Prevention and treatment of COVID-19 disease by controlled modulation of innate immunity. Eur. J. Immunol. 2020, 50, 932–938. [Google Scholar] [CrossRef]
- Cezário, K.; Santos, C.A.F.d.; Filho, C.d.M.A.; Amirato, G.R.; Paixão, V.D.; Almeida, E.B.; Amaral, J.B.D.; Caldo-Silva, A.; Pimenta, N.; Sampaio, A.R.; et al. Older Women Who Practiced Physical Exercises before the COVID-19 Pandemic Present Metabolic Alterations and Worsened Functional Physical Capacity after One Year of Social Isolation. Healthcare 2022, 10, 1736. [Google Scholar] [CrossRef]
- Bueno, S.M.; Abarca, K.; González, P.A.; Gálvez, N.M.S.; Soto, J.A.; Duarte, L.F.; Schultz, B.M.; Pacheco, G.A.; González, L.A.; Vázquez, Y.; et al. Safety and Immunogenicity of an Inactivated Severe Acute Respiratory Syndrome Coronavirus 2 Vaccine in a Subgroup of Healthy Adults in Chile. Clin. Infect. Dis. 2022, 75, e792–e804. [Google Scholar] [CrossRef]
- McElhaney, J.E. Influenza vaccine responses in older adults. Ageing Res. Rev. 2011, 10, 379–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcelhaney, J.E.; Coler, R.N.; Baldwin, S.L. Immunologic correlates of protection and potential role for adjuvants to improve influenza vaccines in older adults. Expert Rev. Vaccines 2013, 12, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Shahid, Z.; Kleppinger, A.; Gentleman, B.; Falsey, A.R.; McElhaney, J.E. Clinical and immunologic predictors of influenza illness among vaccinated older adults. Vaccine 2010, 28, 6145–6151. [Google Scholar] [CrossRef]
- Wilkinson, T.M.; Li, C.K.F.; Chui, C.S.C.; Huang, A.K.; Perkins, M.; Liebner, J.C.; Lambkin-Williams, R.; Gilbert, A.; Oxford, J.; Nicholas, B.; et al. Preexisting influenza-specific CD4 + T cells correlate with disease protection against influenza challenge in humans. Nat. Med. 2012, 18, 274–280. [Google Scholar] [CrossRef]
- Sridhar, S.; Begom, S.; Bermingham, A.; Hoschler, K.; Adamson, W.; Carman, W.; Bean, T.; Barclay, W.; Deeks, J.J.; Lalvani, A.; et al. Cellular immune correlates of protection against symptomatic pandemic influenza. Nat. Med. 2013, 19, 1305–1312. [Google Scholar] [CrossRef]
- Haq, K.; McElhaney, J.E. Immunosenescence: Influenza vaccination and the elderly. Curr. Opin. Immunol. 2014, 29, 38–42. [Google Scholar] [CrossRef]
- Flaxman, A.; Marchevsky, N.G.; Jenkin, D.; Aboagye, J.; Aley, P.K.; Angus, B.; Belij-Rammerstorfer, S.; Bibi, S.; Bittaye, M.; Cappuccini, F.; et al. Reactogenicity and immunogenicity after a late second dose or a third dose of ChAdOx1 nCoV-19 in the UK: A substudy of two randomised controlled trials (COV001 and COV002). Lancet 2021, 398, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.C.; Murthy, S.; Diaz, J. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- He, Q.; Mao, Q.; Zhang, J.; Bian, L.; Gao, F.; Wang, J.; Xu, M.; Liang, Z. COVID-19 Vaccines: Current Understanding on Immunogenicity, Safety, and Further Considerations. Front. Immunol. 2021, 12, 1–13. [Google Scholar] [CrossRef]
- Ritzau-Jost, J.; Hutloff, A. T cell/b cell interactions in the establishment of protective immunity. Vaccines 2021, 9, 1074. [Google Scholar] [CrossRef] [PubMed]
- Parker, D.C. T-cell Dependent B-Cell Activiation. Annu. Rev. lmmunol. 1993, 11, 331–360. [Google Scholar] [CrossRef] [PubMed]
- Olsen, I.; Sollid, L.M. Pitfalls in determining the cytokine profile of human T cells. J Immunol Methods. 2013, 390, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Pangrazzi, L.; Reidla, J.; Carmona Arana, J.A.; Naismith, E.; Miggitsch, C.; Meryk, A.; Keller, M.; Krause, A.A.N.; Melzer, F.L.; Trieb, K.; et al. CD28 and CD57 define four populations with distinct phenotypic properties within human CD8+ T cells. Eur. J. Immunol. 2020, 50, 363–379. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Bonafè, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann. N. Y. Acad. Sci. 2000, 908, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Garagnani, P.; Vitale, G.; Capri, M.; Salvioli, S. Inflammaging and ‘Garb-aging’. Trends Endocrinol. Metab. 2017, 28, 199–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martens, P.B.; Goronzy, J.J.; Schaid, D.; Weyand, C.M. Expansion of unusual CD4+ T cells in severe rheumatoid arthritis. Arthritis Rheum. 1997, 40, 1106–1114. [Google Scholar] [CrossRef]
- Rhee, J.W.; Sabatine, M.S.; Lilly, L.S. Acute coronary syndromes. In Lilly LS: Pathophysiology of Heart Disease: Acollaborative Project of Medical Students and Faculty, 5th ed.; LW&W: Baltimore, MD, USA, 2013; pp. 161–189. [Google Scholar]
- Goronzy, J.J.; Fulbright, J.W.; Crowson, C.S.; Poland, G.A.; O’Fallon, W.M.; Weyand, C.M. Value of Immunological Markers in Predicting Responsiveness to Influenza Vaccination in Elderly Individuals. J. Virol. 2001, 75, 12182–12187. [Google Scholar] [CrossRef] [Green Version]
- Goronzy, J.J.; Weyand, C.M. Mechanisms underlying T cell ageing. Nat. Rev. Immunol. 2019, 19, 573–583. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physical Exercise Group (PE) | Non-Physical Exercise Group (NPE) | |||
|---|---|---|---|---|
| CoronaVac Vaccine (n = 46) | ChadOx-1 Vaccine (n = 23) | ChadOx-1 Vaccine (n = 24) | p-Value | |
| Age (years) | 74.4 ± 3.9 | 75.3 ± 9.1 | 75.6 ± 7.9 | >0.05 |
| Women (n) | 34 | 18 | 06 | <0.0001 |
| Men (n) | 12 | 05 | 18 | <0.0265 |
| Height (m) | 1.57 ± 0.1 | 1.57 ± 0.08 | 1.56 ± 0.09 | >0.05 |
| Weight (kg) | 63.4 ± 12.2 | 65.9 ± 12.7 | 66.7 ± 16.6 | >0.05 |
| Body mass index | 25.9 ± 4.6 | 26.7 ± 5.3 | 27.4 ± 6.2 | >0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, B.R.; Monteiro, F.R.; Cezário, K.; Amaral, J.B.d.; Paixão, V.; Almeida, E.B.; Santos, C.A.F.d.; Amirato, G.R.; Oliveira, D.B.L.; Durigon, E.L.; et al. Older Adults Who Maintained a Regular Physical Exercise Routine before the Pandemic Show Better Immune Response to Vaccination for COVID-19. Int. J. Environ. Res. Public Health 2023, 20, 1939. https://doi.org/10.3390/ijerph20031939
Silva BR, Monteiro FR, Cezário K, Amaral JBd, Paixão V, Almeida EB, Santos CAFd, Amirato GR, Oliveira DBL, Durigon EL, et al. Older Adults Who Maintained a Regular Physical Exercise Routine before the Pandemic Show Better Immune Response to Vaccination for COVID-19. International Journal of Environmental Research and Public Health. 2023; 20(3):1939. https://doi.org/10.3390/ijerph20031939
Chicago/Turabian StyleSilva, Brenda Rodrigues, Fernanda Rodrigues Monteiro, Kizzy Cezário, Jônatas Bussador do Amaral, Vitória Paixão, Ewin Barbosa Almeida, Carlos André Freitas dos Santos, Gislene Rocha Amirato, Danielle Bruna Leal Oliveira, Edison Luiz Durigon, and et al. 2023. "Older Adults Who Maintained a Regular Physical Exercise Routine before the Pandemic Show Better Immune Response to Vaccination for COVID-19" International Journal of Environmental Research and Public Health 20, no. 3: 1939. https://doi.org/10.3390/ijerph20031939