

Knowledge, Perception and Consumption of Indigenous Foods in Gauteng Region, South Africa
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Site and Population
2.3. Sampling
2.4. Data Collection
2.5. Ethical Considerations
2.6. Data Analysis
3. Results
3.1. Sociodemographic Characteristics of the Studied Population
3.2. Knowledge and Consumption Level of Indigenous Foods
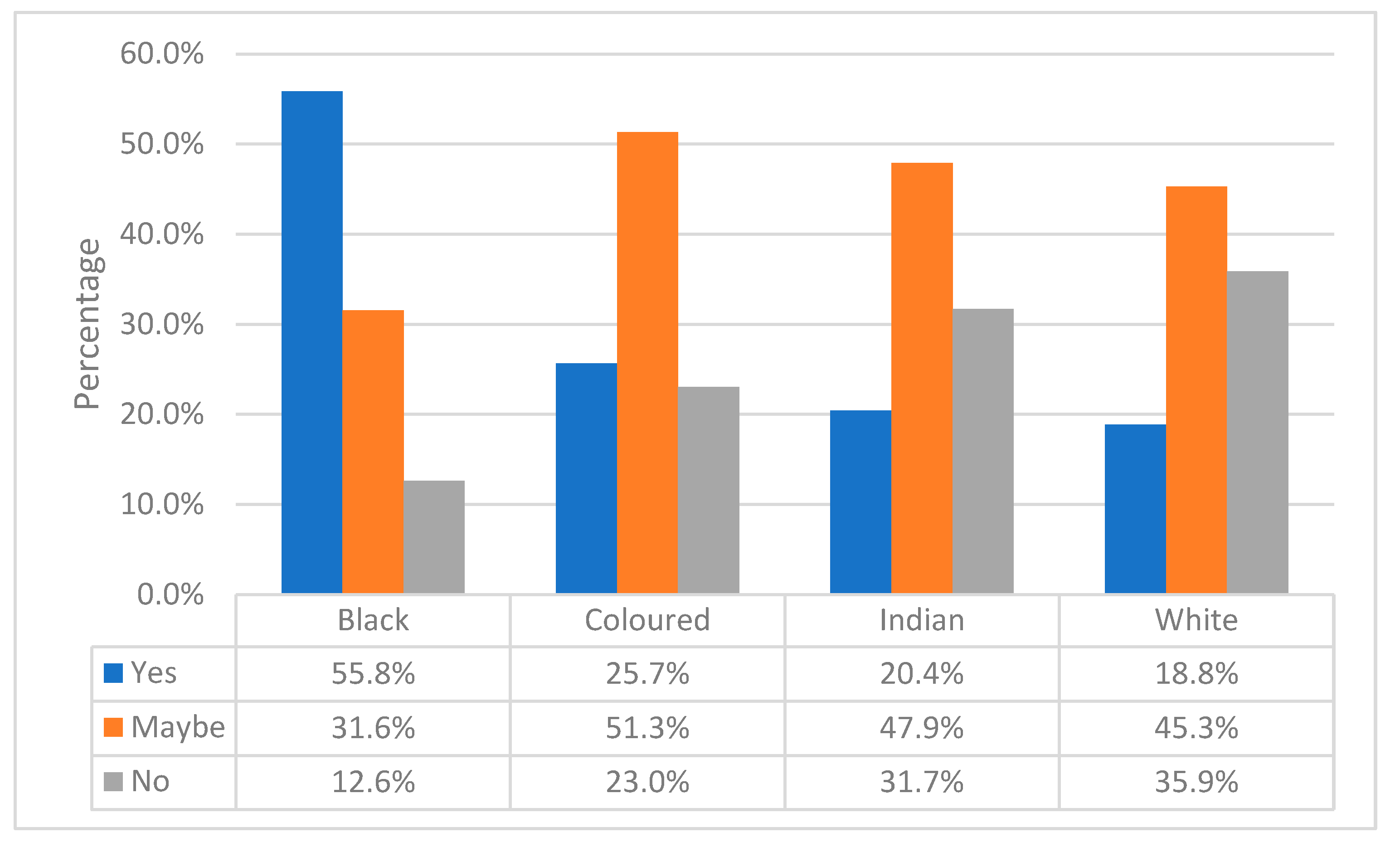
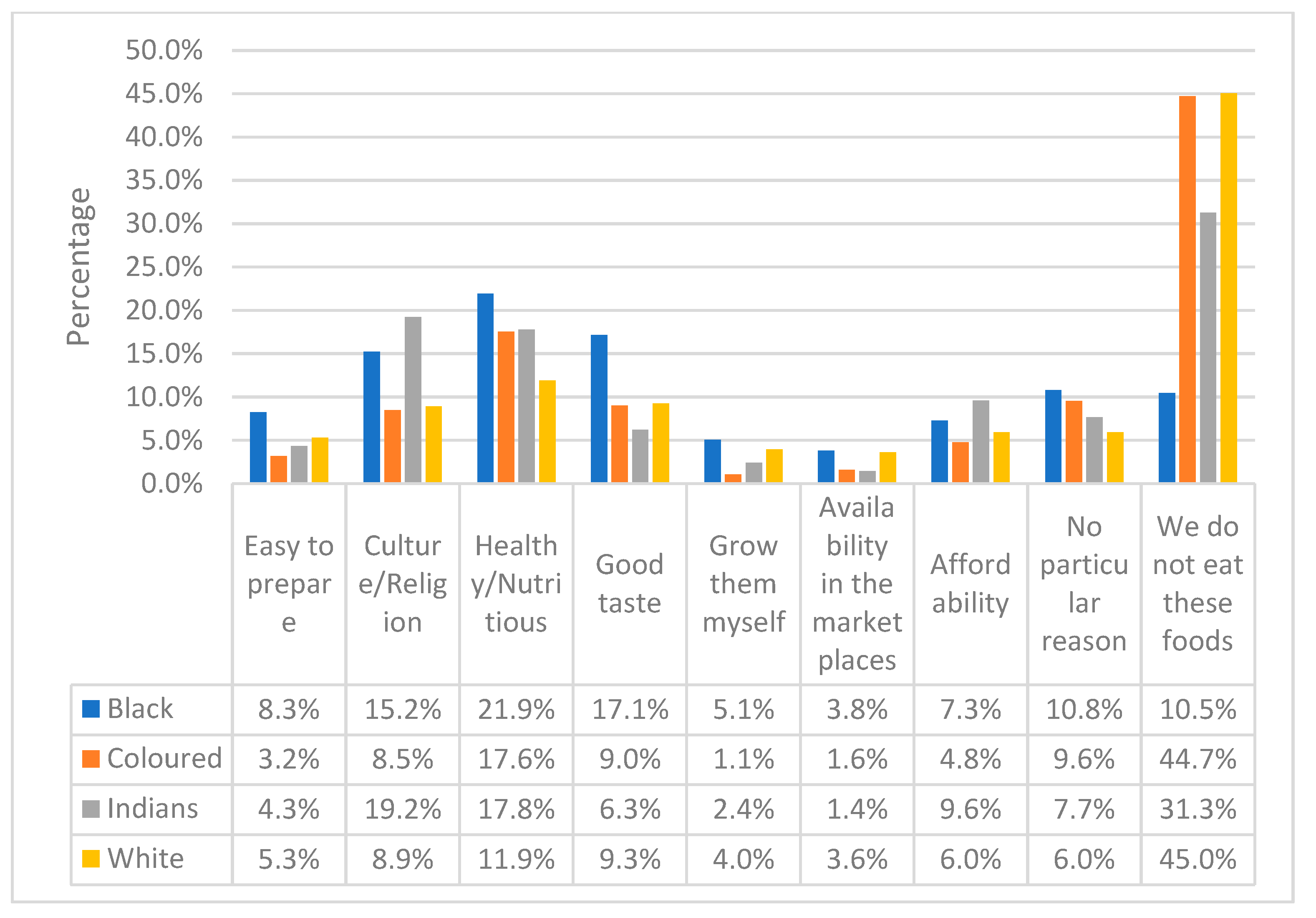
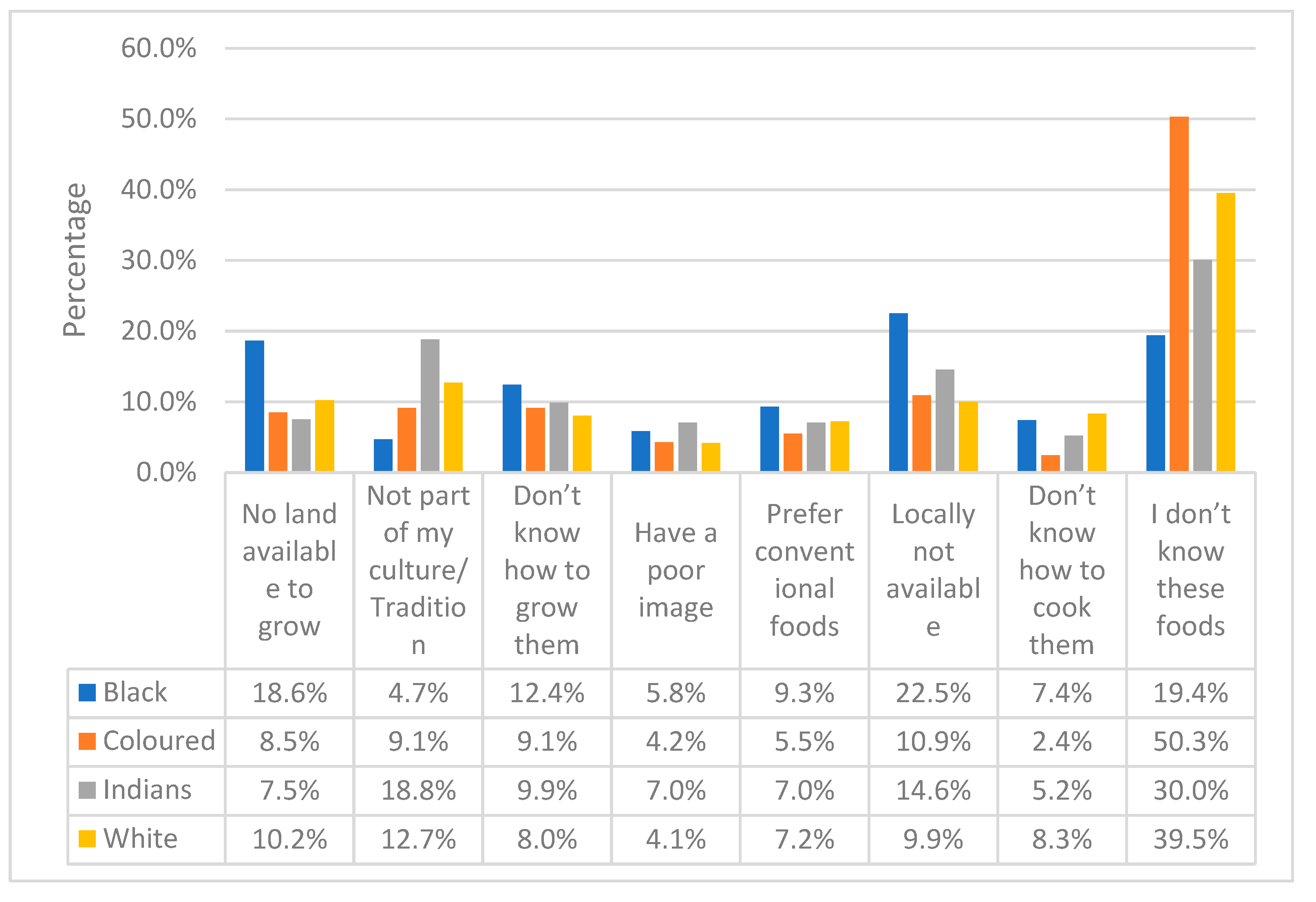
3.3. Perceptions and Reasons for Consuming Indigenous Foods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, K.R.; Patel, S.A.; Ali, M.K. Non-communicable diseases in South Asia: Contemporary Perspectives. Br. Med. Bull. 2014, 111, 31–44. [Google Scholar] [CrossRef]
- Reubi, D.; Herrick, C.; Brown, T. The politics of non-communicable diseases in the Global South. Health Place 2016, 39, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Bigna, J.J.; Noubiap, J.J. The rising burden of non-communicable diseases in sub-Saharan Africa. Lancet Glob. Health 2019, 7, e1295–e1296. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases. World Health Organization. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 7 August 2023).
- Manderson, L.; Jewett, S. Risk. Lifestyle and non-communicable diseases of poverty. Global. Health. 2023, 19, 13. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.M.S.; Purnat, T.D.; Phuong, N.T.A.; Mwingira, U.; Schacht, K.; Fröschl, G. Non-Communicable diseases (NCDs) in developing countries: A symposium report. Global. Health 2014, 10, 81. [Google Scholar] [CrossRef] [PubMed]
- Musaiger, A.O.; Al-Hazzaa, H.M. Prevalence and risk factors associated with nutrition-related noncommunicable diseases in the Eastern Mediterranean region. Int. J. Gen. Med. 2012, 5, 199–217. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases Country Profiles 2018. 2018. Available online: https://apps.who.int/iris/handle/10665/274512 (accessed on 15 June 2023).
- Hyseni, L.; Atkinson, M.; Bromley, H.; Orton, L.; Lloyd-Williams, F.; McGill, R.; Capewell, S. The effects of policy actions to improve population dietary patterns and prevent diet-related non-communicable diseases: Scoping review. Eur. J. Clin. Nutr. 2017, 71, 694–711. [Google Scholar] [CrossRef]
- Vorster, H.; Badham, J.; Venter, C. An introduction to the revised food-based dietary guidelines for South Africa. S. Afr. J. Clin. Nutr. 2013, 26, S5–S12. [Google Scholar]
- Mbhenyane, X.G. Indigenous foods and their contribution to nutrient requirements. South African J. Clin. Nutr. 2017, 30, 5–7. [Google Scholar]
- Olatona, F.A.; Onabanjo, O.O.; Ugbaja, R.N.; Nnoaham, K.E.; Adelekan, D.A. Dietary habits and metabolic risk factors for non-communicable diseases in a university undergraduate population. J. Health Popul. Nutr. 2018, 37, 21. [Google Scholar] [CrossRef]
- Akinola, R.; Pereira, L.M.; Mabhaudhi, T.; de Bruin, F.M.; Rusch, L. A review of indigenous food crops in Africa and the implications for more sustainable and healthy food systems. Sustainability 2020, 12, 3493. [Google Scholar] [CrossRef] [PubMed]
- Chyne, D.A.L.; Ananthan, R.; Longvah, T. Food compositional analysis of indigenous foods consumed by the Khasi of Meghalaya, North-East India. J. Food Compos. Anal. 2019, 77, 91–100. [Google Scholar] [CrossRef]
- Kapoor, R.; Sabharwal, M.; Ghosh-Jerath, S. Indigenous foods of India: A comprehensive narrative review of nutritive values, antinutrient content and mineral bioavailability of traditional foods consumed by indigenous communities of India. Front. Sustain. Food Syst. 2022, 6, 696228. [Google Scholar] [CrossRef] [PubMed]
- Takaidza, S. ‘Indigenous South African food: Nutrition and health benefits’ Phytochemicals in Agriculture and Food [Working Title]. IntechOpen 2023. [Google Scholar] [CrossRef]
- South African Department Agriculture, Forestry and Fisheries. Most common indigenous food crops of South Africa. 2013. Available online: https://www.nda.agric.za/docs/Brochures/Indigfoodcrps.pdf (accessed on 14 June 2019).
- Cloete, P.C.; Idsardi, E.F. Consumption of indigenous and traditional food crops: Perceptions and realities from South Africa. Agroecol. Sustain. Food Syst. 2013, 37, 902–914. [Google Scholar] [CrossRef]
- Pillay-Van Wyk, V.; Dorrington, R.E.; Bradshaw, D. Rapidly changing mortality profiles in South Africa in its nine provinces. S. Afr. Med. J. 2017, 107, 168–169. [Google Scholar] [CrossRef]
- Vorster, H.E.H. The link between poverty and malnutrition: A South African perspective. Health SA Gesondheid 2010, 15, 6. [Google Scholar] [CrossRef]
- Dweba, T.P.; Mearns, M.A. Conserving indigenous knowledge as the key to the current and future use of traditional vegetables. Int. J. Inf. Manag. 2011, 31, 564–571. [Google Scholar] [CrossRef]
- Creswell, J.W.A. Concise Introduction to Mixed Methods Research; Sage: Thousand Oaks, CA, USA, 2015; ISBN 9781483359045. [Google Scholar]
- Bhattacherjee, A. Social Science Research: Principles, Methods, and Practices. University of South Florida. 2012. Available online: http://scholarcommons.usf.edu/cgi/viewcontent.cgi?article=1002&context=oa_textbooks (accessed on 2 September 2020).
- Quiroga Ledezma, C.C. Native food crops for present and future generations: Their role in nutrition and health. In Sustainability of the Food System: Sovereignty, Waste, and Nutrients Bioavailability; Betoret, N., Betoret, E., Eds.; Academic Press: London, UK, 2020. [Google Scholar] [CrossRef]
- Van der Hoeven, M.; Osei, J.; Greeff, M.; Kruger, A.; Faber, M.; Smuts, C.M. Indigenous and traditional plants: South African parents’ knowledge, perceptions and uses and their children’s sensory acceptance. J. Ethnobiol. Ethnomed. 2013, 9, 78. [Google Scholar] [CrossRef]
- Bvenura, C.; Sivakumar, D. The role of wild fruits and vegetables in delivering a balanced and healthy diet. Food Res. Int. 2017, 99, 15–30. [Google Scholar] [CrossRef]
- Masekoameng, M.R.; Molotja, M.C. The role of indigenous foods and indigenous knowledge systems for rural households’ food security in Sekhukhune district, Limpopo province, South Africa. J. Consum. Sci. 2019, 4, 34–48. [Google Scholar]
- Spires, M.; Sanders, D.; Puoane, T.; Hoelzel, P.; Swart, R. Diet-related non-communicable diseases in South Africa: Determinants and policy responses. S. Afr. Health Rev. 2016, 2016, 35–42. [Google Scholar]
- Nengovhela, R.; Taruvinga, A.; Mushunje, A. Determinants of indigenous fruits consumption frequency among rural households: Evidence from Mutale Local Municipality, South Africa. J. Adv. Agric. Technol. 2018, 5. [Google Scholar] [CrossRef]
- Ferguson, M.; Brown, C.; Georga, C.; Miles, E.; Wilson, A.; Brimblecombe, J. Traditional food availability and consumption in remote Aboriginal communities in the Northern Territory, Australia. Aust. N. Z. J. Public Health 2017, 41, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Bultosa, G.; Molapisi, M.; Tselaesele, N.; Kobue-Lekalake, R.; Haki, G.D.; Makhabu, S.; Sekwati-Monang, B.; Seifu, E.; Nthoiwa, G.P. Plant-based traditional foods and beverages of Ramotswa Village, Botswana. J. Ethn. Foods 2020, 7, 1. [Google Scholar] [CrossRef]
- Department of Agriculture, Forestry and Fisheries. Production Guidelines for Mobola plum. 2015. Available online: https://www.dalrrd.gov.za/Portals/0/Brochures%20and%20Production%20guidelines/Mobola%20plum%20.pdf (accessed on 11 September 2021).
- Macintyre, U.E.; Kruger, H.S.; Venter, C.S.; Vorster, H.H. Dietary intakes of an African population in different stages of transition in the Northwest Province, South Africa: The THUSA study. Nutr. Res. 2001, 22, 239–256. [Google Scholar] [CrossRef]
- Demi, S.M. African Indigenous Food Crops: Their Roles in Combatting Chronic Diseases in Ghana. Master’s Thesis, University of Toronto, Toronto, ON, Canada, 2014. [Google Scholar]
- Van der Merwe, J.D.; Cloete, P.C.; Van der Hoeven, M. Promoting food security through indigenous and traditional food crops. Agroecol. Sustain. Food Syst. 2016, 40, 830–847. [Google Scholar] [CrossRef]
- Majova, V.J. The Rural-Urban Linkage in the Use of Traditional Foods by Peri-Urban Households in Nompumelelo Community in East London, Eastern Cape: A Comparative Study. Master’s Thesis, University of South Africa, Pretoria, South Africa, 2001. Available online: https://uir.unisa.ac.za/handle/10500/4973 (accessed on 28 July 2021).
- Gewa, C.A.; Onyango, A.C.; Angano, F.O.; Stabile, B.; Komwa, M.; Thomas, P.; Krall, J. Mothers’ beliefs about indigenous and traditional food affordability, availability and taste are significant predictors of indigenous and traditional food consumption among mothers and young children in rural Kenya. Public Health Nutr. 2019, 22, 2950–2961. [Google Scholar] [CrossRef]
- Musotsi, A.A.; Abukutsa-Onyango, M.O.; Makokha, A. Changing food consumption habits: A case of African indigenous vegetables for food and nutrition security in Kakamega County, Western Kenya. Afr. J. Hortic. Sci. 2017, 12, 30–39. [Google Scholar]
- Cockx, L.; Colen, L.; De Weerdt, J.; Sergio, G.Y.P. Urbanization as a driver of changing food demand in Africa: Evidence from rural-urban migration in Tanzania. Publications Office of the European Union, European Commission, Luxembourg. JRC Tech. Rep. 2019. [Google Scholar] [CrossRef]
- Bharucha, Z.; Pretty, J. The roles and values of wild foods in agricultural systems. Philos. Trans. R. Soc. B Biol. Sci. 2010, 365, 2913–2926. [Google Scholar] [CrossRef] [PubMed]
- Odunitan-Wayas, F.; Okop, K.; Dover, R.; Alaba, O.; Micklesfield, L.; Puoane, T.; Uys, M.; Tsolekile, L.; Levitt, N.; Battersby, J.; et al. Food purchasing characteristics and perceptions of neighborhood food environment of South Africans living in low-, middle- and high-socioeconomic neighborhoods. Sustainability 2018, 10, 4801. [Google Scholar] [CrossRef]
- Sarkar, D.; Walker-Swaney, J.; Shetty, K. Food diversity and indigenous food systems to combat diet-linked chronic diseases. Curr. Dev. Nutr. 2020, 4, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Cheikhyoussef, A.; Embashu, W. Ethnobotanical knowledge on indigenous fruits in Ohangwena and Oshikoto regions in Northern Namibia. J. Ethnobiol. Ethnomed. 2013, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, K. Are Indigenous vegetables underutilized crops? Some Evidence from Eastern Africa and South East Asia. Acta Hortic. 2007, 752, 29–34. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic Variables | Frequency (n) | Percentage (%) | |
|---|---|---|---|
| Gender | Male | 299 | 40.1 |
| Female | 447 | 59.9 | |
| Race | Black | 206 | 27.6 |
| Coloured | 152 | 20.4 | |
| Indian | 142 | 19 | |
| White | 223 | 29.9 | |
| Asian | 21 | 2.8 | |
| Other | 2 | 0.3 | |
| Age group | 18–25 | 207 | 27.7 |
| 26–35 | 215 | 28.8 | |
| 36–45 | 171 | 22.9 | |
| 46–55 | 101 | 13.5 | |
| 56–65 | 37 | 5 | |
| 66+ | 14 | 1.9 | |
| Missing | 1 | 0.1 | |
| Highest education level | Grade 0–7 | 17 | 2.3 |
| Grade 8–12 | 267 | 35.8 | |
| Tertiary Education | 462 | 61.9 | |
| Household size | 1–2 | 145 | 19.4 |
| 3–5 | 441 | 59.1 | |
| 6 or more | 160 | 21.4 | |
| Household Income per month after tax | Less than ZAR 500 | 16 | 2.1 |
| ZAR 500–ZAR 999 | 13 | 1.7 | |
| ZAR 1000–ZAR 1999 | 20 | 2.7 | |
| ZAR 2000–ZAR 2999 | 39 | 5.2 | |
| ZAR 3000–ZAR 4999 | 84 | 11.3 | |
| ZAR 5000–ZAR 9999 | 94 | 12.6 | |
| ZAR 10,000–ZAR 14,999 | 123 | 16.5 | |
| ZAR 15,000–ZAR 24,999 | 117 | 15.7 | |
| ZAR 25,000–ZAR 34,999 | 82 | 11 | |
| ZAR 35,000–ZAR 44,999 | 67 | 9 | |
| ZAR 45,000–ZAR 54,999 | 47 | 6.3 | |
| ZAR 55,000+ | 44 | 5.9 | |
| Area of residence | Urban | 491 | 65.8 |
| Peri-urban | 185 | 24.8 | |
| Rural | 69 | 9.2 | |
| Missing | 1 | 0.1 | |
| Corresponding settlement of urban/peri-urban area | Informal settlement | 60 | 8 |
| Former border or homeland towns | 11 | 1.5 | |
| Township (Kasi) | 189 | 25.3 | |
| Suburb/Edge city | 416 | 55.8 | |
| Missing | 70 | 9.4 | |
| Indigenous Food | Knowledge n (%) | Consumption n (%) | |
|---|---|---|---|
| Grain crops | Pearl millet | 162 (21.7%) | 92 (12.3%) |
| Grain sorghum | 242 (32.4%) | 144 (19.3%) | |
| Cowpea | 139 (18.6%) | 85 (11.4%) | |
| Bambara groundnuts | 112 (15.0%) | 70 (9.4%) | |
| Mungbean | 101 (13.5%) | 60 (8.0%) | |
| Vegetable crops | Cleome | 102 (13.7%) | 62 (8.3%) |
| Amaranth | 108 (14.5%) | 65 (8.7%) | |
| Blackjack | 126 (16.9%) | 61 (8.2%) | |
| Jews mallow | 74 (9.9%) | 49 (6.6%) | |
| Cassava | 98 (13.1%) | 51 (6.8%) | |
| Amadumbe | 144 (19.3%) | 92 (12.3%) | |
| Fruits | Marula | 239 (32.0%) | 141 (18.9%) |
| Red milkwood | 58 (7.8%) | 39 (5.2%) | |
| Mobola plum | 76 (10.2%) | 50 (6.7%) | |
| Wild medlar | 61 (8.2%) | 43 (5.8%) | |
| Num-num | 55 (7.4%) | 32 (4.3%) | |
| Kei apple | 90 (12.1%) | 58 (7.8%) | |
| Natal orange (Strychnos spinosa) | 88 (11.8%) | 50 (6.7%) | |
| Race and consumption of indigenous grain crops | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Race | Pearl Millet | Grain Sorghum | Cowpea | ||||||
| n (%) | Odd ratio (95%CI) | p-Value | n (%) | Odd ratio (95%CI) | p-Value | n (%) | Odd ratio (95%CI) | p-Value | |
| Asian | 2 (9.5%) | 2.5 (0.5–12.4) | 0.262 | 3 (14.3%) | 1.79 (0.48–8.63) | 0.384 | 1 (4.8%) | 0.96 (0.12–7.85) | 0.972 |
| Black | 59 (28.5%) | 9.48 (4.56–19.71) | 0.000 | 86 (41.5%) | 7.63 (4.42–13.16) | 0.000 | 59 (28.5%) | 7.68 (3.90–15.12) | 0.000 |
| Coloured | 10 (6.5%) | 1.65 (0.65–4.16) | 0.288 | 24 (15.6%) | 1.98 (1.04–3.76) | 0.036 | 10 (6.5%) | 1.34 (0.55–3.23) | 0.517 |
| Indian | 13 (9.2%) | 2.40 (0.99–5.76) | 0.051 | 13 (9.2%) | 1.08 (0.52–2.27) | 0.834 | 5 (3.5%) | 0.70 (0.24–2.07) | 0.523 |
| White | 9 (4.0%) | 1 | 19 (8.5%) | 1 | 11 (4.9%) | 1 | |||
| Race and consumption of indigenous vegetable crops | |||||||||
| Race | Cleome | Amaranth | Amadumbe | ||||||
| n (%) | Odd ratio (95%CI) | p-value | n (%) | Odd ratio (95%CI) | p-value | n (%) | Odd ratio (95%CI) | p-value | |
| Asian | 0 (0%) | 1.62 × 10−8 (1.62 × 10−8–1.62 × 10−8) | - | 0 (0%) | 2.01 × 10−8 (2.01 × 10−8–2.01 × 10−8) | - | 0 (0%) | 1.03 × 10−8 (1.03 × 10−8–1.03 × 10−8) | - |
| Black | 42 (20.3%) | 9.21 (3.82–22.17) | 0.000 | 48 (23.2%) | 13.16 (5.12–33.81) | 0.000 | 56 (27.1%) | 16.17 (6.33–41.32) | 0.000 |
| Coloured | 5 (3.2%) | 1.21 (0.36–4.05) | 0.753 | 6 (3.9%) | 1.77 (0.53–5.90) | 0.354 | 13 (8.4%) | 4.02 (1.40–11.52) | 0.010 |
| Indian | 10 (7.0%) | 2.74 (0.97–7.71) | 0.056 | 6 (4.2%) | 1.92 (0.58–6.43) | 0.288 | 19 (13.4%) | 6.74 (2.45–18.48) | 0.000 |
| White | (2.7%) | 1 | 5 (2.2%) | 1 | 5 (2.2%) | 1 | |||
| Race and consumption of indigenous fruit crops | |||||||||
| Race | Marula | Mobola plum | Kei apple | ||||||
| n (%) | Odd ratio (95%CI) | n (%) | Odd ratio (95%CI) | p-value | n (%) | Odd ratio (95%CI) | p-value | ||
| Asian | 1 (4.8%) | 0.33 (0.04–2.59) | 0.294 | 0 (0%) | 5.81 × 10−9 (5.81 × 10−9–5.81 × 10−9) | - | 1 (4.8%) | 0.96 (0.12–7.85) | 0.972 |
| Black | 66 (31.9%) | 3.13 (1.92–5.10) | 0.000 | 22 (10.6%) | 1.92 (0.94–3.92) | 0.073 | 30 (14.5%) | 3.26 (1.59–6.70) | 0.001 |
| Coloured | 26 (16.9%) | 1.36 (0.76–2.41) | 0.295 | 7 (4.5%) | 0.77 (0.30–1.98) | 0.585 | 7 (4.5%) | 0.92 (0.35–2.42) | 0.862 |
| Indian | 20 (14.1%) | 1.10 (0.59–2.02) | 0.768 | 8 (5.6%) | 0.96 (0.39–2.39) | 0.938 | 9 (6.3%) | 1.30 (0.53–3.23) | 0.566 |
| White | 29 (13.0%) | 1 | 13 (5.8%) | 1 | 11 (4.9%) | 1 | |||
| Indigenous Foods | Frequency | Missing n (%) | Total n (%) | |||||
|---|---|---|---|---|---|---|---|---|
| Daily n (%) | Weekly n (%) | Monthly n (%) | Seasonally n (%) | Rarely n (%) | ||||
| Grain crops | Pearl millet | 9 (9.8%) | 19 (20.7%) | 18 (19.6%) | 20 (21.7%) | 22 (23.9%) | 4 (4.3%) | 92 (100%) |
| Grain sorghum | 12 (8.3%) | 28 (19.4%) | 20 (13.9%) | 33 (22.9%) | 42 (29.2%) | 9 (6.3%) | 144 (100%) | |
| Cowpea | 1 (1.2%) | 6 (7.1%) | 19 (22.4%) | 35 (41.2%) | 15 (17.6%) | 9 (10.6%) | 85 (100%) | |
| Bambara groundnuts | 2 (2.9%) | 3 (4.3%) | 4 (5.7%) | 33 (47.1%) | 18 (25.7%) | 10 (14.3%) | 70 (100%) | |
| Mungbean | 1 (1.7%) | 11 (18.3%) | 8 (13.3%) | 15 (25%) | 20 (33.3%) | 5 (8.3%) | 60 (100%) | |
| Vegetable crops | Cleome | 4 (6.5%) | 8 (12.9%) | 6 (9.7%) | 23 (37.1%) | 17 (27.4%) | 4 (6.5%) | 62 (100%) |
| Amaranth | 1 (1.5%) | 5 (7.7%) | 6 (9.2%) | 28 (43.1%) | 19 (29.2%) | 6 (9.2%) | 65 (100%) | |
| Blackjack | 2 (3.3%) | 4 (6.6%) | 6 (9.8%) | 27 (44.3%) | 15 (24.6%) | 7 (11.5%) | 61 (100%) | |
| Jew’s mallow | 1 (2%) | 5 (10.2%) | 4 (8.2%) | 25 (51%) | 11 (22.4%) | 3 (6.1%) | 49 (100%) | |
| Cassava | 1 (2%) | 3 (5.9%) | 5 (9.8%) | 19 (37.3%) | 14 (27.5%) | 9 (17.6%) | 51 (100%) | |
| Amadumbe | 2 (2.2%) | 4 (4.3%) | 17 (18.5%) | 34 (37%) | 27 (29.3%) | 8 (8.7%) | 92 (100%) | |
| Fruits | Marula | 4 (2.8%) | 4 (2.8%) | 2 (1.4%) | 59 (41.8%) | 59 (41.8%) | 13 (9.2%) | 141 (100%) |
| Red milkwood | 1 (2.6%) | 6 (15.4%) | 3 (7.7%) | 14 (35.9%) | 11 (28.2%) | 4 (10.3%) | 39 (100%) | |
| Mobola plum | 2 (4%) | 1 (2%) | 3 (6%) | 21 (42%) | 15 (30%) | 8 (16%) | 50 (100%) | |
| Wild medlar | 1 (2.3%) | 4 (9.3%) | 1 (2.3%) | 11 (25.6%) | 17 (39.5%) | 9 (20.9%) | 43 (100%) | |
| Num-num | 0 (0%) | 0 (0%) | 6 (18.8%) | 14 (43.8%) | 8 (25%) | 4 (12.5%) | 32 (100%) | |
| Kei apple | 4 (6.9%) | 2 (3.4%) | 4 (6.9%) | 27 (46.6%) | 16 (27.6%) | 5 (8.6%) | 58 (100%) | |
| Natal plum | 3 (6%) | 2 (4%) | 5 (10%) | 19 (38%) | 15 (30%) | 6 (12%) | 50 (100%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kesa, H.; Tchuenchieu Kamgain, A.D.; Kwazi Zuma, M.; Mbhenyane, X. Knowledge, Perception and Consumption of Indigenous Foods in Gauteng Region, South Africa. Int. J. Environ. Res. Public Health 2023, 20, 6961. https://doi.org/10.3390/ijerph20206961
Kesa H, Tchuenchieu Kamgain AD, Kwazi Zuma M, Mbhenyane X. Knowledge, Perception and Consumption of Indigenous Foods in Gauteng Region, South Africa. International Journal of Environmental Research and Public Health. 2023; 20(20):6961. https://doi.org/10.3390/ijerph20206961
Chicago/Turabian StyleKesa, Hema, Alex D. Tchuenchieu Kamgain, Mthokozisi Kwazi Zuma, and Xikombiso Mbhenyane. 2023. "Knowledge, Perception and Consumption of Indigenous Foods in Gauteng Region, South Africa" International Journal of Environmental Research and Public Health 20, no. 20: 6961. https://doi.org/10.3390/ijerph20206961