
Evaluation of Multidimensional Functional Impairment in Adult Sexual Assault Survivors, with a Focus on Its Psychological, Physical, and Social Dimensions, Based on Validated Measurements: A PRISMA Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Analysis Strategy
2.4. Quality Assessment of the Included Studies
3. Results
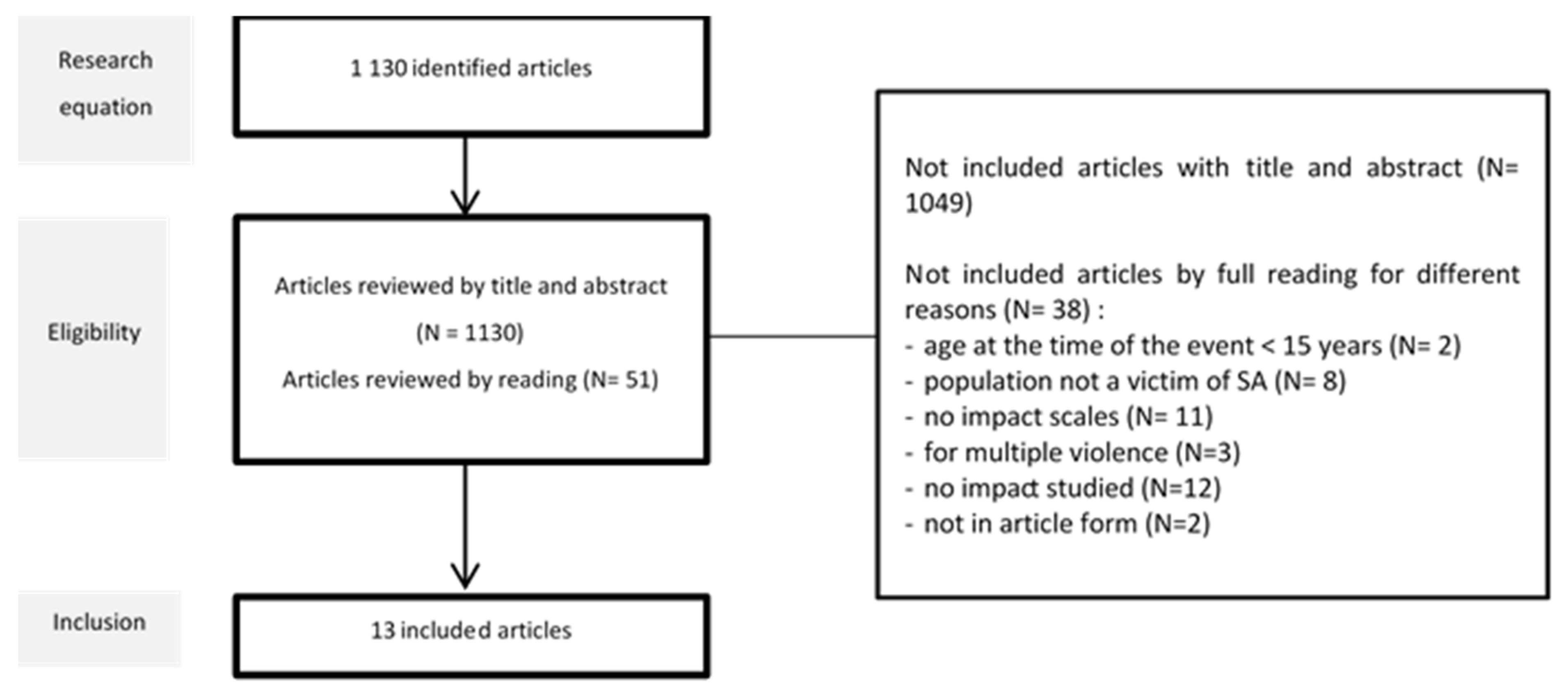
3.1. Selection of Studies
3.2. Characteristics of These Articles
3.2.1. General Characteristics of the Included Articles
3.2.2. Physical Impairment
3.2.3. Sexual Impairment
3.2.4. Psychological Impairment
3.2.5. Social and Occupational Impairment
3.2.6. Quality of Life Impairment
3.3. Assessment of the Quality of the Studies
4. Discussion
4.1. Overall Results
4.2. A Very Limited Body of Literature
4.2.1. Social Support and Avoidant Coping: A Short-Term Coping Strategy That Can Be Adapted but That Is Likely to Be Deleterious in the Medium and Long Term for Survivors
4.2.2. Physical Impairment and Pain Evaluation: A Multisite and Lasting Pain in More Than One in Four Survivors
4.2.3. Sexual Functional Impairment
4.2.4. Psychological Impairment: The Most Important and Generalized Impairment in Survivors
4.3. Limitations and Strengths
4.4. Implications for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Section and Topic | Item # | Checklist Item | Location Where Item Is Reported |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | 1/2 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | 2 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | 2 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | 2 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | 2 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | 2/3 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | 2/3 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | 2/3 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | 2 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | 3 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | 3 |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | 3 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | 3 | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | 3 | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | 3 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | 3 | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | 3 | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | 3 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | 3 |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | 4 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | 4 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | 4–12 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | 4–12 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | 4–12 |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | 4–12 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | 4–12 | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | 4–12 | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | 4–12 | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | 4–12 |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | 4–12 |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | 13 |
| 23b | Discuss any limitations of the evidence included in the review. | 14 | |
| 23c | Discuss any limitations of the review processes used. | 14 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | 15 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | ||
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | ||
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | |
| Competing interests | 26 | Declare any competing interests of review authors. | |
Appendix B
| S1 | S2 | S3 | S4 | S6 | S5 | S7 | S8 | S9 | S10 | S11 | S12 | S13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Title and abstract | x | X | x | x | x | x | x | x | x | x | x | x | x |
| Introduction | |||||||||||||
| Background | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Objectives | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Methods | |||||||||||||
| Study design | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Setting | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Participants | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Variables | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Data sources | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Bias | |||||||||||||
| Study size | x | x | x | x | x | x | x | x | x | x | x | x | |
| Quantitative variables | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Statistical methods | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Results | |||||||||||||
| Participants | |||||||||||||
| a numbers | x | x | x | x | x | x | in method part | x | x | x | x | x | |
| b reasons for non-participation | x | x | x | x | |||||||||
| c flow diagram | x | x | |||||||||||
| Descriptive data | |||||||||||||
| a characteristics | x | x | x | x | x | x | x | x | x | x | x | x | x |
| B number of participants with missing data | x | x | |||||||||||
| c cohort study: summarise follow-up | x | ||||||||||||
| Outcome data | x | x | x | x | x | x | x | x | x | x | x | ||
| Main results | |||||||||||||
| a unadjusted estimates | x | x | x | x | x | x | x | x | x | x | x | x | x |
| b report category boundaries | x | x | x | x | x | x | x | x | x | x | x | ||
| c consider translating estimates | x | x | x | ||||||||||
| Other analyses | x | x | x | x | x | x | x | x | x | x | |||
| Discussion | |||||||||||||
| Key results | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Limitations | x | x | x | x | x | x | x | x | x | x | x | ||
| Interpretation | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Generalisability | x | x | x | x | x | x | x | ||||||
| Other information | |||||||||||||
| Funding | x | x | x | ||||||||||
| Design | Cohort study | Observational study | Cross-sectionnal study | Case-control study | Case-control study | Prospective observational study | Cross-sectionnal study | Longitudinal study | Prospective observational study | ||||
References
- WHO. Violence Against Women: Intimate Partner and Sexual Violence against Women. Available online: https://apps.who.int/iris/bitstream/handle/10665/112325/WHO_RHR_14.11_eng.pdf?sequence=1&isAllowed=y (accessed on 18 April 2023).
- Basile, K.C.; Black, M.C.; Breiding, M.J.; Chen, J.; Merrick, M.T.; Smith, S.G.; Gilbert, L.K.; Patel, N.; Walling, M.; Jain, A. National Intimate Partner and Sexual Violence Survey: 2010 Summary Report. National Center for Injury Prevention and Control (U.S.). Division of Violence Prevention. Available online: https://stacks.cdc.gov/view/cdc/11637 (accessed on 18 April 2023).
- Breiding, M.J.; Smith, S.G.; Basile, K.C.; Walters, M.L.; Chen, J.; Merrick, M.T. Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization—National Intimate Partner and Sexual Violence Survey, United States, 2011. Morb. Mortal Wkly Rep. Surveill. Summ. 2014, 63, 1–18. [Google Scholar]
- Hawks, L.; Woolhandler, S.; Himmelstein, D.U.; Bor, D.H.; Gaffney, A.; McCormick, D. Association between forced sexual initiation and health outcomes among US women. JAMA Intern. Med. 2019, 179, 1551–1558. [Google Scholar] [CrossRef]
- Elliott, D.M.; Mok, D.S.; Briere, J. Adult sexual assault: Prevalence, symptomatology, and sex differences in the general population. J. Trauma Stress 2004, 17, 203–211. [Google Scholar] [CrossRef]
- Masho, S.W.; Odor, R.K.; Adera, T. Sexual assault in Virginia: A population-based study. Womens Health Issues 2005, 15, 157–166. [Google Scholar] [CrossRef]
- Masho, S.W.; Anderson, L. Sexual assault in men: A population-based study of Virginia. Violence Vict. 2009, 24, 98–110. [Google Scholar] [CrossRef]
- Turchik, J.A.; Hassija, C.M. Female sexual victimization among college students: Assault severity, health risk behaviors, and sexual functioning. J. Interpers. Violence 2014, 29, 2439–2457. [Google Scholar] [CrossRef]
- World Health Organization; Pan American Health Organization. Understanding and Addressing Violence Against Women: Sexual Violence; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Plichta, S.B. Intimate partner violence and physical health consequences: Policy and practice implications. J. Interpers. Violence 2004, 19, 1296–1323. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.; Dworkin, E.; Cabral, G. An ecological model of the impact of sexual assault on women’s mental health. Trauma Violence Abuse 2009, 10, 225–246. [Google Scholar] [CrossRef] [Green Version]
- Temple, J.R.; Weston, R.; Rodriguez, B.F.; Marshall, L.L. Differing effects of partner and nonpartner sexual assault on women’s mental health. Violence Against Women 2007, 13, 285v97. [Google Scholar] [CrossRef]
- Rees, S.; Silove, D.; Chey, T.; Ivancic, L.; Steel, Z.; Creamer, M.; Teesson, M.; Bryant, R.; McFarlane, A.C.; Mills, K.L.; et al. Lifetime prevalence of gender-based violence in women and the relationship with mental disorders and psychosocial function. JAMA 2011, 306, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Faravelli, C.; Giugni, A.; Salvatori, S.; Ricca, V. Psychopathology after rape. Am. J. Psychiatry 2004, 161, 1483–1485. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Liu, H.; Petukhova, M.V.; Sampson, N.A.; Aguilar-Gaxiola, S.; Alonso, J.; Andrade, L.H.; Bromet, E.J.; de Girolamo, G.; Haro, J.M.; Hinkov, H.; et al. Association of DSM-IV posttraumatic stress disorder with traumatic experience type and history in the World Health Organization World Mental Health surveys. JAMA Psychiatry 2017, 74, 270–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13 (Suppl. 1), S31–S34. [Google Scholar] [CrossRef]
- Frazier, P.; Tashiro, T.; Berman, M.; Steger, M.; Long, J. Correlates of levels and patterns of positive life changes following sexual assault. J. Consult. Clin. Psychol. 2004, 72, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Ulirsch, J.C.; Ballina, L.E.; Soward, A.C.; Rossi, C.; Hauda, W.; Holbrook, D.; Wheeler, R.; Foley, K.; Batts, J.; Collette, R.; et al. Pain and somatic symptoms are sequelae of sexual assault: Results of a prospective longitudinal study. Eur. J. Pain 2014, 18, 559–566. [Google Scholar] [CrossRef]
- Golding, J.M. Sexual assault history and limitations in physical functioning in two general population samples. Res. Nurs. Health 1996, 19, 33–44. [Google Scholar] [CrossRef]
- Högbeck, I.; Möller, A. Female sexual function six months after sexual assault: Post-traumatic stress disorder strongest risk factor for impaired function. J. Sex Marital. Ther. 2022, 48, 112–120. [Google Scholar] [CrossRef]
- Tadayon, M.; Hatami-Manesh, Z.; Sharifi, N.; Najar, S.; Saki, A.; Pajohideh, Z. The relationship between function and sexual satisfaction with sexual violence among women in Ahvaz, Iran. Electron. Physician 2018, 10, 6608–6615. [Google Scholar] [CrossRef] [Green Version]
- Postma, R.; Bicanic, I.; van der Vaart, H.; Laan, E. Pelvic floor muscle problems mediate sexual problems in young adult rape victims. J. Sex Med. 2013, 10, 1978–1987. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.; Archer, J.; Davies, M. Effects of male rape on psychological functioning. Br. J. Clin. Psychol. 2005, 44, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Seyller, M.; Denis, C.; Dang, C.; Boraud, C.; Lepresle, A.; Lefèvre, T.; Chariot, P. Intimate partner sexual assault: Traumatic injuries, psychological symptoms, and perceived social reactions. Obstet. Gynecol. 2016, 127, 516–526. [Google Scholar] [CrossRef] [PubMed]
- Darves-Bornoz, J.M.; Pierre, F.; Lépine, J.P.; Degiovanni, A.; Gaillard, P. Screening for psychologically traumatized rape victims. Eur. J. Obstet Gynecol. Reprod. Biol. 1998, 77, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Aquino, N.M.R.D.; Sun, S.Y.; Oliveira, E.M.D.; Martins, M.D.G.; Silva, J.D.F.D.; Mattar, R. Sexual violence and its association with health self-perception among pregnant women. Rev. Saude Publica 2009, 43, 954–960. [Google Scholar] [CrossRef] [Green Version]
- Karataş, R.D.; Altınöz, A.E.; Eşsizoğlu, A. Post-traumatic stress disorder and related factors among female victims of sexual assault required to attend a University Hospital in Turkey: A cross-sectional cohort study. Crim. Behav. Ment. Healt 2020, 30, 79–94. [Google Scholar] [CrossRef]
- Gottfried, R.; Lev-Wiesel, R.; Hallak, M.; Lang-Franco, N. Inter-relationships between sexual abuse, female sexual function and childbirth. Midwifery 2015, 31, 1087–1095. [Google Scholar] [CrossRef]
- Holder, N.; Maguen, S.; Holliday, R.; Vogt, D.; Bernhard, P.A.; Hoffmire, C.A.; Blosnich, J.R.; Schneiderman, A.I. Psychosocial outcomes among veteran and non-veteran survivors of sexual assault. J. Interpers. Violence 2023, 38, NP1569-91. [Google Scholar] [CrossRef]
- Sachs-Ericsson, N.; Kendall-Tackett, K.A.; Sheffler, J.; Arce, D.; Rushing, N.C.; Corsentino, E. The influence of prior rape on the psychological and physical health functioning of older adults. Aging Ment. Health 2014, 18, 717–730. [Google Scholar] [CrossRef]
- Feldhaus, K.M.; Houry, D.; Kaminsky, R. Lifetime sexual assault prevalence rates and reporting practices in an emergency department population. Ann. Emerg. Med. 2000, 36, 23–27. [Google Scholar] [CrossRef]
- Dworkin, E.R.; Brill, C.D.; Ullman, S.E. Social reactions to disclosure of interpersonal violence and psychopathology: A systematic review and meta-analysis. Clin. Psychol. Rev. 2019, 72, 101750. [Google Scholar] [CrossRef]
- McQueen, K.; Murphy-Oikonen, J.; Miller, A.; Chambers, L. Sexual assault: Women’s voices on the health impacts of not being believed by police. BMC Womens Health 2021, 21, 217. [Google Scholar]
- Lechner, M.; Bell, K.; Short, N.A.; Martin, S.L.; Black, J.; Buchanan, J.A.; Reese, R.; Ho, J.D.; Reed, G.D.; Platt, M.; et al. Perceived care quality among women receiving Sexual Assault Nurse Examiner (SANE) care: Results from a 1 week post exam survey in a large multisite prospective study. J. Emerg. Nurs. 2021, 47, 449–458. [Google Scholar] [CrossRef]
- García-Moreno, C.; Hegarty, K.; d’Oliveira, A.F.L.; Koziol-McLain, J.; Colombini, M.; Feder, G. The health-systems response to violence against women. Lancet 2015, 385, 1567–1579. [Google Scholar]
- Fedele, E.; Trousset, V.; Schalk, T.; Oliero, J.; Fovet, T.; Lefèvre, T. Identification of Psycho-Socio-Judicial Trajectories and Factors Associated with PTSD after Recent Sexual Assault: The IADViSe Study Protocol for a Multi-Centric Prospective Study Using Mixed Methods and Artificial Intelligence; Preprint; Research Square Company: Durham, NC, USA, 2023. [Google Scholar] [CrossRef]

| Study | Aim | Design | Population | Type of Sexual Violence | Functional Impact | Measure(s) | Stat. Methods | Results |
|---|---|---|---|---|---|---|---|---|
| S1 [20] Frazier P, Journal of Consulting and Clinical Psychology, 2004 DOI: 14756611 | Assess correlates of early reports of positive life changes after sexual assault and individual trajectories of self-reported positive change over time | Cohort prospective | N = 171 women, between 16 and 52 years Recruited from 7 emergency rooms 1-year follow-up (2 weeks, 2 months, 6 months, 12 months) | Sexual violence | SOCIAL IMPACT Social support Approach and avoidant coping Religious coping Perceived control Positive life changes | Social Support Scale—2 items Cronbach: 0.81 Coping Strategies Inventory—CSI—Cronbach: 0.91 for approach coping and 0.84 for avoidant coping Religious coping scale—Cronbach: 0.94 Three scales from the Rape Attribution Questionnaire: Behavioral self-blame—Cronbach: 0.87 Control over recovery—Cronbach: 0.84 Taking precaution—Cronbach: 0.83 14/17 items from 17-item life change scale | Hierarchical linear modeling—HLM | The trajectories of social support, approach coping, religious coping, control over the recovery process and taking precautions were all positively associated with positive-change trajectories, suggesting that increases in these variables were associated with increases in self-reported positive life changes over time |
| S2 [21] Ulirsch JC, European Journal of Pain, 2013 DOI: 24019249 | Assess the incidence and distribution of pain symptoms and other types of somatic symptoms experienced by women sexual assault survivors | Prospective observational study | N = 84 women, 18 years or older (M = 26 years) Recruited through medical care within 48 h of sexual assault | Sexual assault (vaginal, oral, or anal penetration) No repeated assault | PHYSICAL IMPACT Evolution of pain at 1 week, 6 weeks, and 3 months 21 somatic symptoms (headache, dizziness, nausea, noise sensitivity, concentration difficulties, taking longer to think…) | Numeric rating scale—0 to 10—in 8 body regions Numeric rating scale | Incidence rates CI 95% Bonferroni adjusted | Pain reported for: - 1 body region: 58% after 6 weeks and 60% after 3 months - 3 or more body regions: 32% after 6 weeks and 28% after 3 months - More than 10% reported pain in 5 or more body regions Highest prevalence regions: head, neck, back, and abdomen Association between location of trauma during SA and location of pain after 6 weeks and 3 months Somatic symptoms at 6 weeks: 38% showed a significant increase in severity Somatic symptoms at 3 months: 52% showed a significant increase in severity |
| S3 [22] Golding JM, Research in Nursing & Health, 1996 DOI: 8552801 | Hypothesized that sexual assault history is associated with limitations in physical functioning | Prospective observational study | N = 6024 respondents 516 reported a history of sexual assault 52% were female (M = 42 years) | Sexual assault with the sexual assault instrument (62 items) | PHYSICAL IMPACT Physical symptoms Physical functioning | 39 items from the somatization section of the Diagnostic Interview Schedule (DIS). Symptoms were scored as positive only if they were severe, which was defined as causing the respondent to use medication other than aspirin or interfering significantly with their life Number of days spent in bed because of illness Number of days of restricted activity | Physical symptoms reported in SA vs. control: 67.9 vs. 41.7 (p < 0.001) Both bed days and restricted activity days were significantly more common among persons with a history of sexual assault than among those without Number of (SA vs. control): - Bed days 15.9 vs. 10.1 (p = 0.006) - Restricted activity days 18.9 vs. 11.7 (p = 0.002) | |
| S4 [23] Högbeck I, Journal of Sex & Marital Therapy, 2022 DOI: 34338163 | Investigate the effect of sexual assault on sexual function in adult women six months post-assault, as well as the possible correlations between impaired sexual function and assault characteristics, psychiatric morbidity, and post-assault PTSD | Prospective observational study | N = 73 women (M = 24 years) Over 18 years Seen within one month of the index assault in the emergency clinic for rape survivors | Rape or attempted rape (penetration or not) Sexual assault age: M = 24 years No information about repeated violence | SEXUAL IMPACT Sexual function (last 4 weeks) | FEMALE SEXUAL FUNCTION INDEX (38 items measuring sexual function before and after the assault) 26.55 is the optimal cutoff for differentiating women with and without sexual dysfunction Cronbach coefficient: 0.92 to 0.98 | Paired simple t-test Comparisons use Pearson’s chi-square test | 60% estimated their sexual function at six months post-assault as impaired The mean FSFI total score was lower post-assault compared to pre-assault: 23 vs. 28.7 (p < 0.001) |
| S5 [24] Tadayon M, Electronic Physician, 2018 DOI: 29881522 | Determine the relationship between sexual performance and sexual satisfaction in those who have experienced violence, so that we can take steps to improve women’s sexual health | Case-control study | N = 35 women aged 15–45 years, married for at least a year, who have been sexually abused and referred to a forensic medical examination unit (M = 28 years) N = 70 women in control group (M = 29 years) | Sexually abused women referred to a forensic medical examination unit | SEXUAL IMPACT Sexual satisfaction Sexual performance | Larson Sexual Satisfaction Questionnaire—25 items, 5-option Likert scale Dissatisfaction (score under 50), low satisfaction (50–75), moderate satisfaction (75–100), high satisfaction (>100) Cronbach coefficient: >0.7 validated in couple population Sexual Performance Index Questionnaire—6 subscales including libido, sexual desire, lubrication, orgasm, satisfaction, and pain—19 questions—scores below 26 considered as impaired performance Cronbach coefficient: >0.7 | Chi-square test, t-test, Fisher’s exact test | Significant difference between the two groups (SA vs. control) in terms of sexual satisfaction: 71.4 vs. 99.44 (p < 0.001) Significant difference regarding sexual performance (SA vs. control): 17.10 vs. 26.37 (p < 0.001) Statistically significant difference in terms of sexual arousal (decreased in SA), orgasm (id), lubrication (id), pain (increased in SA), and sexual satisfaction (decreased in SA) |
| S6 [25] Postma R, Journal of Sexual Medicine, 2013 DOI: 23679151 | Investigate the effect of rape on sexual problems and on pelvic floor problems | Cross-sectional study | N = 89 women raped during adolescence (M = 20.9 years) N = 114 women in the control group (M = 20.8 years) | Rape includes both attempted and completed rape 20% revictimization | SEXUAL IMPACT Sexual functioning Pelvic floor functioning | Female Sexual Function Index FSFI—cutoff: 26.55 Cronbach coefficient: 0.92 to 0.98 Amsterdam Hyperactive Pelvic Floor Scale-Women 11.00 is the optimal score for differentiating women with and without pelvic floor dysfunction Cronbach coefficient: 0.75 to 0.82 | Sample t-test Pearson’s chi-square tests | Prevalence of sexual dysfunction in SA vs. control: 44.6% (N = 25/56) vs. 19.5% (N = 15/77) Significant difference t: rape survivors had a 2.4 times higher prevalence of sexual dysfunction when compared with the control group More sexual problems for rape survivors: more lubrication problems (D = 0.497, p < 0.001) and more pain (D = 0.695, p < 0.001) Prevalence of pelvic pain in SA vs. control: 33.7% (N = 30/89) vs. 12.4% (N = 14/113) Significant difference: rape survivors had a 2.7 times higher prevalence of pelvic floor dysfunction More significant pelvic floor problems in SA: provoked vulvodynia (p < 0.001), stress (p < 0.001), lower urinary tract symptoms (p < 0.001), and irritable bowel syndrome symptoms (p < 0.001) |
| S7 [26] Walker J, British Journal of Clinical Psychology, 2005 DOI: 10.1348 | Investigate the effects of rape on a non-clinical male sample by comparing them on standard tests with a control group with no prior history of sexual assault | Case-control study | N = 40 male rape survivors (M = 34.2 years) Age of assault: 70% between 16 and 25 years Control group: 40 men with same characteristics | Sexual assault No precision | PSYCHOLOGICAL IMPACT General health PSYCHOLOGICAL IMPACT Trust in the future SOCIAL IMPACT Current self-esteem | General Health Questionnaire (GHQ)—28 items—4-point response scale Cronbach coefficient: 0.85 World Assumptions Scale: People’s basic assumptions about the world in which they live. 32 items—6-point response scale Cronbach coefficient: 0.40 to 0.83 State Self-Esteem Scale—20 items—5-point response scale—Cronbach coefficient: 0.9 | Using t-tests p = 0.01 | Significantly higher score for the survivors on each GHQ subscale: somatic symptoms: 2.96 p = 0.005 social dysfunction: 4.78 p = 0.001 anxiety/insomnia: 4.62 p = 0.001 depression: 7.06 p = 0.001 No significant difference Only self-worth is lower among the survivors (p = 0.001) Significantly lower self-esteem scores in the survivors group (58.95 vs. 74.05, p = 0.001) and for each subscale (performance, social appearance) |
| S8 [27] Seyller M, Obstetrics & Gynecology, 2016 DOI: 10.1097 | Compare the consequences of sexual assault based on the relationship between female survivors and their assailant | Prospective observational study | N = 294 women (M = 23 years) separated into 3 groups: G1: intimate partner: 106 (M = 29 years) G2: acquaintance: 100 (M = 20 years) G3: stranger: 88 (M = 21 years) | Sexual assault (vaginal, anal, or oral penetration, attempts, sexual touching) | PSYCHOLOGICAL IMPACT General health at 1 month after sexual assault | General Health Questionnaire (GHQ)—28 items—4-point response scale—cutoff point of 4/5 Cronbach coefficient: 0.85 | Univariate analyses | Score > 4 points Group 1: 89% Group 2: 93% Group 3: 93% The rates of disturbance of survivors of intimate partner violence are similar to those of other survivors |
| S9 [28] Darves-Bornoz JM, European Journal of Obstetrics & Gynecology and Reproductive Biology, 1997 DOI: 9550204 | Determine whether the General Health Questionnaire, a simple psychological instrument, could be useful to non-specialists in screening for psychologically traumatized rape survivors | Prospective observational study | N = 285 subjects (M = 22.5 years), with 24 men and 261 women Rape survivors attending a consultation for survivors of psychological trauma, within the University Hospital of Tours | Rape (sexual penetration) | PSYCHOLOGICAL IMPACT General health—psychological | General Health Questionnaire (GHQ)—28 items—4-point response scale—cutoff point of 4/5 Cronbach coefficient: 0.95 | SPSS SYSTAT software | Mean score: 11.7, independent of age, gender 72% had a GHQ score equal to or higher than the threshold set at 4 |
| S10 [29] Aquino NM, Revista Saúde Pública, 2009 DOI: 19967257 | Estimate the prevalence of sexual violence history among pregnant women and its association with the self-perception of health status | Cross-sectional study | N = 179 pregnant women (M = 24 years) | Unconsented sexual contact (penetration or not) and acts of a sexual nature but without physical contact, such as voyeurism or exposure to pornography | QUALITY OF LIFE Assessment of health-related quality of life using the Medical Outcomes Study: Physical and mental functioning | 12-Item Short-Form Health Survey—SF-12 | A linear regression analysis of variance | Sexual violence survivors showed significantly lower mean physical (42.2) and mental (37.4) scores than women with no history of sexual violence (51, p < 0.001) |
| S11 [30] Reyhan Dağ Karataş, Criminal Behaviour and Mental Health, 2019 DOI: 32307807 | Determine factors associated with PTSD among women who had been sexually assaulted by comparing those with and without PTSD | Cross-sectional cohort study | N = 78 women approached at least 1 month after assault (M = 27.53 years) PTSD group: 41 (M = 28 years) Non-PTSD group: 19 (M = 24.9 years) | Rape: none, vaginal, vaginal and/or other Repeated assault: 39% in PTSD group, 16% in control group | QUALITY OF LIFE | Medical Outcomes Study Short Form—36-item—SF-36 Assess both positive and negative aspects of health status No Cronbach coefficient | The Mann–Whitney U test used for non-normal variables | The PTSD group differs from the group without PTSD with regard to the higher prevalence of other health problems, including a sense of poor general health, low vitality, impaired social function, impaired physical function, impaired physical role, and impaired emotional role |
| S12 [31] Gottfried R, Midwifery, 2015 DOI: 26324214 | Focuses on the inter-relationships between sexual abuse occurring across the lifespan, distressed female sexual function, and childbirth | Quantitative longitudinal study | N = 300 third term singleton pregnant women (M = 31 years) Sexual abuse: 21% | Sexual abuse: illegal act of forcing another person into any form of sexual activity or contact against their will | SEXUAL IMPACT Sexual dysfunction Subjective severity of respondents’ childbirth experience | Female Sexual Distress Scale-Revised 13 statements on a 5-point scale—cutoff >10 to discriminate women with/without female sexual dysfunction Cronbach coefficient: 0.96 Subjective Birth Experience Questionnaire—13 items on a 5-point scale Cronbach coefficient: 0.77 | Null hypothesis tests, chi-square test, significance, p-value, confidence interval, logistic regression | Women with a history of sexual assault showed approximately twice the prevalence of antenatal/postpartum FSD compared to those without such history Sexual abuse was not found to be related to a negatively experienced birth |
| S13 [32] Holder N, Journal of Interpersonal Violence, 2022 DOI: 10.1177 | Compare profiles of psychosocial outcomes for veteran and non-veteran participants who were exposed to childhood, adult, or military sexual assault | Data from the Comparative Health Assessment Interview Research Study | N = 935 non-veteran women and men who reported sexual assault N = 301 non-veteran women and men who reported sexual assault at 18 years or older N = 399 non-veteran women and men who reported childhood sexual assault | Sexual assault: penetration and touching | PHYSICAL IMPACT Health functioning Health satisfaction SOCIAL IMPACT Social functioning Social satisfaction | Well-Being Inventory Six items—score range 1 to 5 Cronbach coefficient: 0.72 Three items—score range 1 to 5 Cronbach coefficient: 0.75 Three items—score range 1 to 5 Cronbach coefficient: 0.84 Four items—score range 1 to 5 Cronbach coefficient: 0.80 | Z-score comparing between trauma groups | The adult sexual assault group reported worse outcomes than the child sexual assault group: Z-score is higher (so worse) in social satisfaction and functioning and health satisfaction. The score is more or less the same in health functioning WBI health functioning: 3.47 (0.69) WBI health satisfaction: 3.35 (1.06) WBI social functioning: 3.46 (0.99) WBI social satisfaction: 3.76 (0.93) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schalk, T.; Oliero, J.; Fedele, E.; Trousset, V.; Lefèvre, T. Evaluation of Multidimensional Functional Impairment in Adult Sexual Assault Survivors, with a Focus on Its Psychological, Physical, and Social Dimensions, Based on Validated Measurements: A PRISMA Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 6373. https://doi.org/10.3390/ijerph20146373
Schalk T, Oliero J, Fedele E, Trousset V, Lefèvre T. Evaluation of Multidimensional Functional Impairment in Adult Sexual Assault Survivors, with a Focus on Its Psychological, Physical, and Social Dimensions, Based on Validated Measurements: A PRISMA Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(14):6373. https://doi.org/10.3390/ijerph20146373
Chicago/Turabian StyleSchalk, Thibault, Juliette Oliero, Emma Fedele, Victor Trousset, and Thomas Lefèvre. 2023. "Evaluation of Multidimensional Functional Impairment in Adult Sexual Assault Survivors, with a Focus on Its Psychological, Physical, and Social Dimensions, Based on Validated Measurements: A PRISMA Systematic Review" International Journal of Environmental Research and Public Health 20, no. 14: 6373. https://doi.org/10.3390/ijerph20146373