
Determinants of Care Pathways for C-PTSD Patients in French Psychotrauma Centers: A Qualitative Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants Recruitment
2.3. Data Collection
2.4. Data Analysis
2.4.1. Open Coding
2.4.2. Axial and Selective Coding
2.5. Trustworthiness, Reliability, and Ethical Concerns
3. Results
3.1. Participants
3.2. Phenomena and Logics Interacting in the Construction of the Care Pathway
3.2.1. Conceptions of C-PTSD
“… C-PTSD or complex trauma, I don’t feel competent to say that I know exactly what one is and what the other is. I wouldn’t be able to make a theoretical difference, but since the new ICD 11 definition, I have a compass to discuss with my colleagues in a common language”(Psychologist-I14)
- (i).
- The importance of the traumatic history in understanding the symptoms:
“In most cases, the multiplicity of traumatic events in the patient’s life course will allow us to predict whether the clinic will be associated with simple or complex.”(EMDR nurse practitioner-I2)
- (ii).
- The functional impact of C-PTSD through interpersonal or emotional dysregulation, social and occupational repercussions, and changes in the client’s agentivity are key assessment parameters in the treatment strategy.
- (iii).
- Need longer, more complex and tailored care than other PTSD sufferers.
“I often ask myself: are we talking about a borderline personality or a traumatic personality in these people?”(Psychologist-I13)
- -
- Certain professionals do not consider personality changes a specific focus for specialized intervention tasks in the field of psychotrauma care. Instead, they propose that these changes, viewed as a comorbidity that could be present in this population, necessitate general mental health interventions:
“… As far as complex traumas are concerned, related to abuse since childhood, where we sense that the young woman is in a borderline state and so on, I stick mainly to general psychiatric care and not to something that stigmatizes her in the question of trauma, avoiding “it’s all about the trauma”, when in fact there are many other things behind it and there have been changes in the personality, before or after the trauma, I don’t know… But often it goes far beyond the question of trauma and many other psychiatric issues are involved.”(Psychologist-I5)
- -
- In contrast, other professionals believe that traditional psychological and psychiatric healthcare tends to overlook these aspects of personality change and disorders. They argue that these elements warrant the attention of CRPs, as recognizing the connection between trauma and personality opens up new ways of conceptualizing symptoms and providing comprehensive support to clients:
“… in fact, what people diagnosed as borderline personality, in 95% of cases, it is complex post-traumatic stress disorder, with a disturbance in attachment, interpersonal relationships, emotional security, and so on. (…) I find that the strength of trauma is that it gives them an angle to work on their personality… Once we explain that these are ultimately people who have experienced such and such a trauma at such and such a time in their lives that it has disturbed them so much that it leads to a presentation of their personality. It allows us to conceptualize things differently and to accept a different kind of care.”(Psychiatrist-I9)
“… I think that, as in all disciplines, we have lenses and that certain approaches mean that we do not hear, listen, welcome and accompany or consider care in the same way, whether we rely on this or that clinical hypothesis.”(Psychologist-I14)
“If we really want to study the improvement of a symptomatology linked to a therapy on complex trauma with the ICD 11 criteria, the criteria are relevant. Then, on the clinical evaluation, here, we are really working on the essentially PTSD dimension part, whether it is simple PTSD or complex PTSD…so we will continue to use the DSM-5.”(Psychiatrist-I1)
3.2.2. The Use of Diagnostic or Therapeutic Tools: A Central Issue in the Organization of Care
- -
- Brief therapy is used to treat the core symptoms of PTSD (intrusion, hypervigilance, avoidance) and then externalized care for other dimensions, symptoms, or post-traumatic personality functioning.
- -
- Brief therapy is used when other treatments fail by CRPs that are skeptical about brief therapy because the treatment goals and their duration are considered too restrictive.
- -
- Brief therapies are employed to address both the core symptoms of PTSD and additional symptoms, although it is acknowledged that they may provide only partial improvement for all the symptoms present. The number of therapy sessions is limited, but the treatment objectives can extend beyond the basic symptoms of PTSD. This includes conducting a comprehensive assessment and offering support for overall functioning, personality, and relationship work. If the client desires further assistance, a referral can be made to a private practice psychologist with expertise in psychotrauma for continued treatment.
“There are people who have too many dissociative symptoms that they find difficult to control and stabilize. So, we have developed a group therapy for them…”(Psychiatrist-I9)
“… In the case of one woman who had started EMDR therapy, which was very trauma-focused, we did not adequately assess the impact it would have in the hours that followed. And how the consequences of that impact would be handled by the external environment. We then said to ourselves that we hadn’t assessed the situation sufficiently and hadn’t put up enough safety nets to contain it…”(Child psychiatrist-I11)
“I trained myself [in EMDR] because I realized that the question of language, […] the stakes of internal conflictuality were not enough to accompany what was happening directly in the person’s body and the way it was affected”.(Psychologist-I14)
3.2.3. Perceptions of Care Needs
- -
- The socioeconomic and cultural diversity of the populations encountered, but also the reception capacities of the CRPs and the availability of downstream care professionals:
“There’s a reality on the ground that means we have to manage to adapt, and sometimes it’s not to say we have to circumvent, but sometimes the directives we have, we have to know how to minimize them…”(Psychologist-I13)
- -
- Carers’ individual theoretical backgrounds and the “center effect” specific to each CRP influence their care plans, as this carer suggests:
“… I would alienate all my colleagues, because it’s not the… it’s the essence of the service, we come to this service to do this.”(Child psychologist-I6)
“… Anyway, if it’s feasible on an outpatient basis, why not, but I find it would be difficult, given the strong demand for referral to the CRP”(Psychiatrist-I9)
3.2.4. The Encounter between Caregivers and Individuals, and Its Challenges
“The disadvantage is that the person doesn’t necessarily want to talk to their doctor, or they don’t really have a doctor, and so they have to go to a doctor’s appointment first. So it can block some people.”(Psychologist-I13)
“…It is better to spend time adapting and building a very good relationship with the person. There will be less avoidance afterwards, rather than trying to deal with the trauma very quickly and not adapting, and the person will blow you off and not come back.”(Psychologist-I13)
3.2.5. The Healthcare Network
“… We have opened up quite widely so that we can train professionals who specialize in early childhood as well as in the medico-social field. We also train lawyers, the police, school health workers… and then, of course, all health professionals.”(Child psychiatrist-I11)
3.2.6. Care Strategy
“To treat complex PTSD from beginning to end, i.e., to follow it in all its dimensions, requires several years of care. We have chosen not to be involved in this function, but only in the PTSD part, in order to be able to provide short-term care and, above all, to ensure a turnover and to be able to respond to requests for care. The demand for care is enormous and if we do not have a CRP with an absolutely huge number of professionals, we will have to share and distribute care…”(Psychiatrist-I1)
“We externalize when there is a lot of emotional regulation work before, that is to say that here, the idea is really a short, intensive care but with a limited number of sessions”(Psychiatrist-I1)
“… we should not do too much stabilization if we want to stabilize client because they are already in a situation where they are destabilized, it is better to go straight to the problem, i.e., to the trauma, and so there is a period of psycho-education and empowerment training which is important, much more than saying here it is unstable or we will never do it… The objectives are really to treat the trauma, i.e., the exposure, the emotional regulation and to try to minimize the stabilization period as much as possible. Because otherwise we can spend months doing stabilization”(Psychiatrist-I9)
“… professionals are more into acute and rapid care than in long-term care which can sometimes require more complicated psychotherapeutic know-how… Often, these personalities, even in psychiatry, we no longer talk about their traumas, and we are satisfied with a semblance of balance that we try to achieve by doing this pseudo-stabilization without tackling the heart of the problem, which is security, the repetition of the trauma and so on”(Psychiatrist-I9)
“In people with C-PTSD [we should] work on lowering the triad of trauma symptoms and also accompany the person on a personality change. Because in fact the problem is that if you only work on the trauma but you don’t work on the construction of the personality, there is a good chance that the person will get back into situations that put them in danger, and as a result, they will relive the trauma and again, they will have to be taken care of. Whereas if you consolidate self-confidence or personality elements that could put them in danger, you consolidate a possible reduction in the recurrence of trauma.”(Psychologist-I13)
“It is an ethical dilemma that consists in asking ourselves: are we offering the best possible care to very few people? Do we try to be egalitarian and give everybody the same kind of care…?”(Psychiatrist-I10)
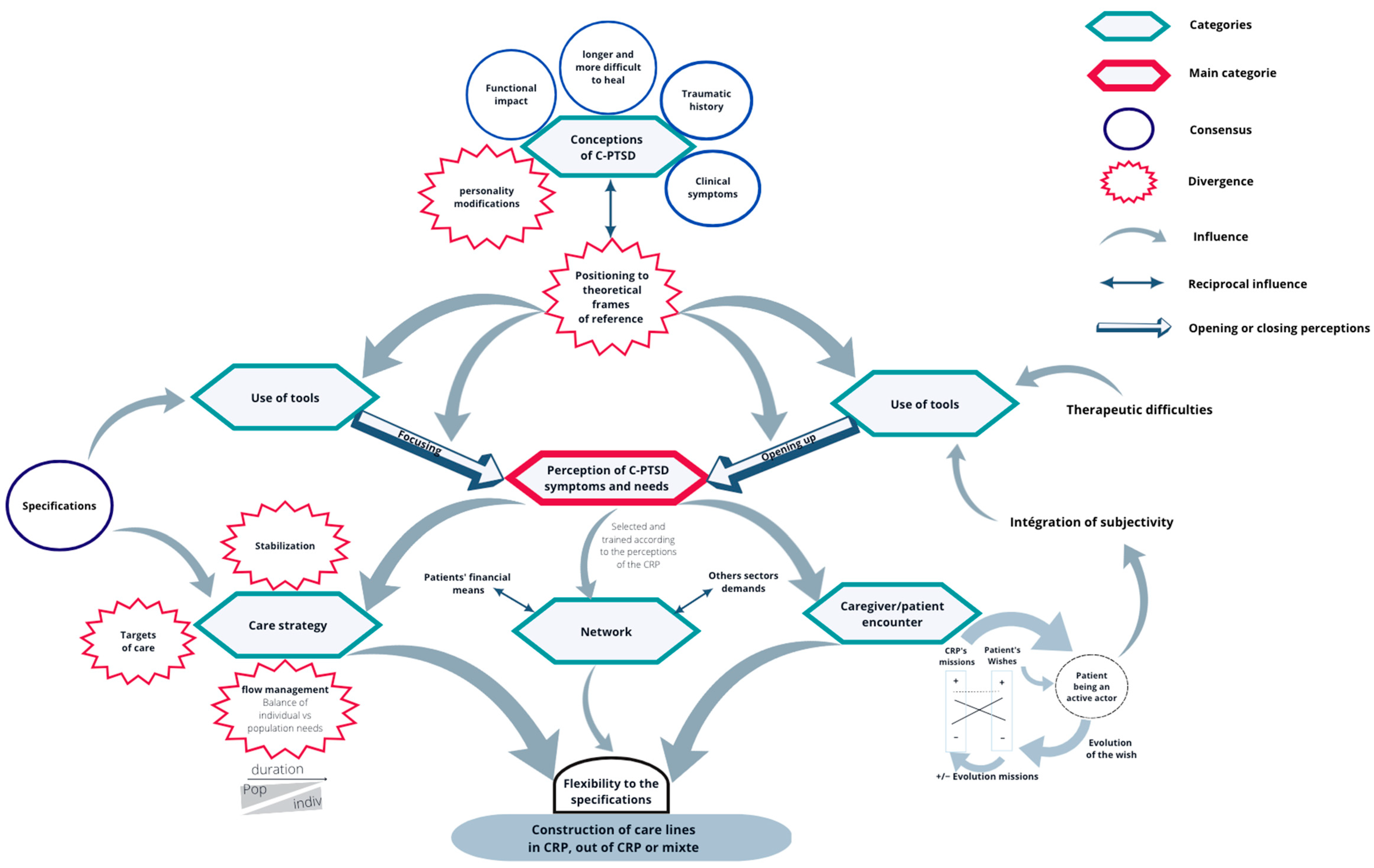
3.3. General Model
- -
- The choice of theoretical framework: The theoretical framework adopted by the caregivers plays a crucial role in shaping their perceptions. Different theoretical perspectives may emphasize different aspects of the clients’ needs.
- -
- The caregivers’ relationship with diagnostic and therapeutic tools: The caregivers’ familiarity and comfort with available diagnostic and therapeutic tools also influences their perceptions. This relationship can affect the way they perceive and respond to the clients’ symptoms and needs.
- -
- The organization and content of caregiver–client interactions: The nature of exchanges between caregivers and clients significantly affects their perceptions of the clients’ needs.
4. Discussion
4.1. Comparison with the Literature
4.1.1. The Plural Essence of C-PTSD
4.1.2. C-PTSD in the Nosography
- -
- To simplify the diagnosis of PTSD: the DSM-5 diagnosis of PTSD, described as 20 symptoms in 4 clusters and a dissociative subtype, results in 636,120 possible presentations, making assessment and treatment planning difficult.
- -
- To clarify the spectrum of psychotrauma and facilitate the development of personalized medicine. Specifying the spectrum by identifying greater categorical homogeneity will stimulate medical research to provide more specific and effective personalized care.
4.1.3. CRP Targets and Strategies
4.1.4. CRPs Forced to Act as Public Health Decision Makers
“-Physical, sexual, psychological violence (intimate partner violence, violence in the family, at work, in times of war, exile and migration …);
“-Exposure to a traumatic event such as an assault, accident, natural disaster, traumatic death, and others.”[30]
4.2. Limitations of the Study
4.3. Perspectives
4.3.1. Reorganizing Care around an Emerging Disorder
- -
- Instead of striving to identify a single optimal strategy while disregarding others, it is more productive to engage in constructive and collaborative work that embraces diverse perspectives.
- -
- Start small by rapidly testing multiple hypotheses and potential solutions in the communities most affected by persistent health problems and with the most to gain, rather than fully deploying a few purely theoretical ideas.
4.3.2. The Key Future Role of the CRPs
- -
- Relational/individual:
- ○
- Promote quality attachment and work against abuse and violence at home;
- ○
- Prenatal and postnatal counseling and investment in parenting education, as a study suggests a reduction in the incidence of incest among invested parents [34].
- -
- Community:
- ○
- Social bonding tools, mobilization for investment to identify and address common problems, and a working committee to improve community life;
- ○
- -
- Institutional:
- ○
- Invest against bullying in schools;
- ○
- Promote dignity by working to reduce the stigmatization or depersonalization of victims and to take greater account of their subjective experiences;
- ○
- Intensify the identification of situations with the potential for chronic traumatization, both in primary healthcare and outside the health sector;
- ○
- Raise awareness of psychological trauma in the initial training of the justice system or law enforcement;
- ○
- Implement immigration management policies that respect human dignity.
- -
- Macro-social:
- ○
- Publicity campaign on psychological trauma, facilitating access to information and promoting the principles of resilience;
- ○
- ○
- Reduce social and economic inequalities, which are related to a general health inequality within the population, but also to the likelihood of being exposed to adversities such as neglect, abuse, violence, discrimination, and humiliation, with multiple consequences for the child’s development, in terms of both physical and mental health [39].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- First, M.B.; Reed, G.M.; Hyman, S.E.; Saxena, S. The development of the ICD-11 Clinical Descriptions and Diagnostic Guidelines for Mental and Behavioural Disorders. World Psychiatry 2015, 14, 82–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maercker, A.; Brewin, C.R.; Bryant, R.A.; Cloitre, M.; van Ommeren, M.; Jones, L.M.; Humayan, A.; Kagee, A.; Llosa, A.E.; Rousseau, C.; et al. Diagnosis and classification of disorders specifically associated with stress: Proposals for ICD-11. World Psychiatry 2013, 12, 198–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herman, J.L. Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. J. Traum. Stress 1992, 5, 377–391. [Google Scholar] [CrossRef]
- Bell, C.C. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 1994; Volume xxvii, p. 886. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; Available online: https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890425596 (accessed on 27 May 2023).
- World Health Organization. International. International Classification of Diseases 11th REVISION (ICD-11). Available online: https://www.who.int/standards/classifcations/classifcation-of-diseases (accessed on 5 May 2023).
- Hyland, P.; Karatzias, T.; Shevlin, M.; Cloitre, M. Examining the Discriminant Validity of Complex Posttraumatic Stress Disorder and Borderline Personality Disorder Symptoms: Results From a United Kingdom Population Sample. J. Trauma. Stress 2019, 32, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Knefel, M.; Karatzias, T.; Ben-Ezra, M.; Cloitre, M.; Lueger-Schuster, B.; Maercker, A. The replicability of ICD-11 complex post-traumatic stress disorder symptom networks in adults. Br. J. Psychiatry 2019, 214, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.D.; Courtois, C.A. Complex PTSD and borderline personality disorder. Borderline Personal. Disord. Emot. Dysregulation 2021, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Cloitre, M.; Stolbach, B.C.; Herman, J.L.; van der Kolk, B.; Pynoos, R.; Wang, J.; Petkova, E. A developmental approach to complex PTSD: Childhood and adult cumulative trauma as predictors of symptom complexity: Childhood and Adult Cumulative Trauma as Predictors of Symptom Complexity. J. Traum. Stress 2009, 22, 399–408. [Google Scholar] [CrossRef]
- Knefel, M.; Tran, U.S.; Lueger-Schuster, B. The association of posttraumatic stress disorder, complex posttraumatic stress disorder, and borderline personality disorder from a network analytical perspective. J. Anxiety Disord. 2016, 43, 70–78. [Google Scholar] [CrossRef]
- Gilbar, O. Examining the boundaries between ICD-11 PTSD/CPTSD and depression and anxiety symptoms: A network analysis perspective. J. Affect. Disord. 2020, 262, 429–439. [Google Scholar] [CrossRef]
- Dorrepaal, E.; Thomaes, K.; Smit, J.H.; van Balkom, A.J.L.M.; Veltman, D.J.; Hoogendoorn, A.W.; Draijer, N. Stabilizing Group Treatment for Complex Posttraumatic Stress Disorder Related to Child Abuse Based on Psychoeducation and Cognitive Behavioural Therapy: A Multisite Randomized Controlled Trial. Psychother. Psychosom. 2012, 81, 217–225. [Google Scholar] [CrossRef]
- Sachser, C.; Keller, F.; Goldbeck, L. Complex PTSD as proposed for ICD-11: Validation of a new disorder in children and adolescents and their response to Trauma-Focused Cognitive Behavioral Therapy. J. Child Psychol. Psychiatry 2017, 58, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Karatzias, T.; Murphy, P.; Cloitre, M.; Bisson, J.; Roberts, N.; Shevlin, M.; Hyland, P.; Maercker, A.; Ben-Ezra, M.; Coventry, P.; et al. Psychological interventions for ICD-11 complex PTSD symptoms: Systematic review and meta-analysis. Psychol. Med. 2019, 49, 1761–1775. [Google Scholar] [CrossRef] [PubMed]
- Cousin, O.; Landour, J.; Delage, P.; Fortino, S.; Paoletti, M. #MeToo, #Travail ? Nouv. Rev. Trav. 2019, 15. [Google Scholar] [CrossRef]
- Impact de la pandémie de COVID-19 sur les violences domestiques. Bull Académie Natl Médecine. March 2021, 205, 213–214. [CrossRef]
- Ministère des Solidarités et de la Santé. Les 1000 Premiers Jours -Là où Tout Commence. 2020. Available online: https://sante.gouv.fr/IMG/pdf/rapport-1000-premiers-jours.pdf (accessed on 10 June 2022).
- Pires, A.P. Échantillonnage et Recherche Qualitative: Essai Théorique et Méthodologique; Tremblay, J.-M., Ed.; Classiques des Sciences Sociales: Saguenay, QC, Canada, 2007; Available online: http://classiques.uqac.ca/contemporains/pires_alvaro/echantillonnage_recherche_qualitative/echantillonnage.html (accessed on 26 August 2022).
- Lejeune, C. Étiqueter: Des propriétés aux catégories. In Manuel D’analyse Qualitative; Méthodes en sciences humaines; De Boeck Supérieur: Louvain-la-Neuve, Belgium, 2019; Volume 2e éd., Chapitre 3, pp. 61–100. Available online: https://www.cairn.info/manuel-d-analyse-qualitative--9782807323582-p-61.htm (accessed on 5 January 2022).
- Lejeune, C. Articuler: Le codage axial. In Manuel d’analyse Qualitative; Méthodes en sciences humaines; De Boeck Supérieur: Louvain-la-Neuve, Belgium, 2019; Volume 2e éd., Chapitre 4, pp. 101–116. Available online: https://www.cairn.info/manuel-d-analyse-qualitative--9782807323582-p-101.htm (accessed on 5 January 2022).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- de Jong, J.T.V.M.; Komproe, I.H.; Spinazzola, J.; van der Kolk, B.A.; Van Ommeren, M.H. DESNOS in three postconflict settings: Assessing cross-cultural construct equivalence: DESNOS in Three Postconflict Settings. J. Traum. Stress 2005, 18, 13–21. [Google Scholar] [CrossRef]
- Lewis-Fernández, R.; Kirmayer, L.J. Cultural concepts of distress and psychiatric disorders: Understanding symptom experience and expression in context. Transcult. Psychiatry 2019, 56, 786–803. [Google Scholar] [CrossRef]
- Cloitre, M. ICD-11 complex post-traumatic stress disorder: Simplifying diagnosis in trauma populations. Br. J. Psychiatry 2020, 216, 129–131. [Google Scholar] [CrossRef]
- Powers, A.; Petri, J.M.; Sleep, C.; Mekawi, Y.; Lathan, E.C.; Shebuski, K.; Bradley, B.; Fani, N. Distinguishing PTSD, complex PTSD, and borderline personality disorder using exploratory structural equation modeling in a trauma-exposed urban sample. J. Anxiety Disord. 2022, 88, 102558. [Google Scholar] [CrossRef]
- Bohus, M.; Kleindienst, N.; Hahn, C.; Müller-Engelmann, M.; Ludäscher, P.; Steil, R.; Fydrich, T.; Kuehner, C.; Resick, P.A.; Stiglmayr, C.; et al. Dialectical Behavior Therapy for Posttraumatic Stress Disorder (DBT-PTSD) Compared with Cognitive Processing Therapy (CPT) in Complex Presentations of PTSD in Women Survivors of Childhood Abuse: A Randomized Clinical Trial. JAMA Psychiatry 2020, 77, 1235. [Google Scholar] [CrossRef]
- Steil, R.; Dittmann, C.; Müller-Engelmann, M.; Dyer, A.; Maasch, A.-M.; Priebe, K. Dialectical behaviour therapy for posttraumatic stress disorder related to childhood sexual abuse: A pilot study in an outpatient treatment setting. Eur. J. Psychotraumatol. 2018, 9, 1423832. [Google Scholar] [CrossRef] [Green Version]
- Courreges, C.; Fourcade, S. BO Santé—Protection sociale—Solidarité, French Ministry of solidarity and health official bulletin, France. 2018. Available online: https://sante.gouv.fr/fichiers/bo/2018/18-07/ste_20180007_0000_0027.pdf (accessed on 10 October 2022).
- Institut National de la Statistique et des Études Économiques. Cadre de Vie et Sécurité—2017. Progedo-Adisp; 2017. Available online: https://data.progedo.fr/studies/doi/10.13144/lil-1247 (accessed on 30 September 2022).
- Roberts, J.P.; Fisher, T.R.; Trowbridge, M.J.; Bent, C. A design thinking framework for healthcare management and innovation. Healthcare 2016, 4, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Salter, M.; Hall, H. Reducing Shame, Promoting Dignity: A Model for the Primary Prevention of Complex Post-Traumatic Stress Disorder. Trauma Violence Abus. 2022, 23, 906–919. [Google Scholar] [CrossRef]
- Williams, L.M.; Finkelhor, D. Paternal caregiving and incest: Test of a biosocial model. Am. J. Orthopsychiatry 1995, 65, 101–113. [Google Scholar] [CrossRef]
- Atkinson, D. Toward a Sociocognitive Approach to Second Language Acquisition. Mod. Lang. J. 2002, 86, 525–545. [Google Scholar] [CrossRef]
- Chen, J.; Multicultural Centre for Women’s Health. Intersectionality Matters: A Guide to Engaging Immigrant and Refugee Communities in Australia; Multicultural Centre for Women’s Health: Collingwood, Australia, 2017; Available online: https://books.google.fr/books?id=CL5IzQEACAAJ (accessed on 3 March 2023).
- Jeremiah, R.D.; Gamache, P.E.; Hegamin-Younger, C. Beyond Behavioral Adjustments: How Determinants of Contemporary Caribbean Masculinities Thwart Efforts to Eliminate Domestic Violence. Int. J. Men Health 2013, 12, 228–244. [Google Scholar] [CrossRef]
- Tolman, R.M.; Rosen, D. Domestic Violence in the Lives of Women Receiving Welfare: Mental Health, Substance Dependence, and Economic Well-Being. Violence Against Women 2001, 7, 141–158. [Google Scholar] [CrossRef]
- Marmot, M. The health gap: The challenge of an unequal world. Lancet 2015, 386, 2442–2444. [Google Scholar] [CrossRef]


{kind=link}
| Question | |
|---|---|
| Main | Additional |
| What is your view of the role of the CRP in client care? | Does your CRP have specificities? How are clients referred to your facility? How and by whom is a client’s care plan designed (secretary, psychiatrist, psychologist, nurse, multidisciplinary consultation)? |
| What is your understanding of complex post-traumatic stress? | What is your definition of complex PTSD? Do you think you have a good knowledge of this new nosography? Do you think it is helpful to distinguish between C-PTSD and PTSD for treatment purposes? |
| How is the issue of complex post-traumatic stress disorder addressed in your CRP? | Does this clinic raise any specific questions or precautions? Is it a problem from your point of view? |
| How are complex PTSD clients currently managed at your CRP? | +/− Clinical client’s descriptions given to the participant: In your opinion, what should be the immediate treatment plan for this client? Over the medium and longer term? How do you imagine the current care of this client? (Which actors?) How would you ideally manage this client in your CRP? |
| What do you think about the role of CRP in the C-PTSD pathway? | Reception, triage, orientation, psycho-education, treatment? Do you have an opinion on care networks? What do you think about a possible standardization of practices? |
| Do you have anything you would like to add? | What would you like to know about how other CRPs work with C-PTSD clients? What are your thoughts on how other CRPs work with people with PTSD and C-PTSD? |
| Participant | Interview Number | Length (min) | Profession | Age | Years of Experience in Trauma Care |
|---|---|---|---|---|---|
| CRP 1 | I1 | 42 | Psychiatrist | 44 | 10 |
| I2 | 50 | EMDR * nurse practitioner | 44 | 15 | |
| I3 | 53 | EMDR * nurse practitioner | 43 | 3 | |
| CRP 2 | I4 | 68 | Psychologist | 53 | 12 |
| I5 | 53 | Psychologist | 39 | 18 | |
| I6 | 82 | Child psychologist | 37 | 13 | |
| CRP 3 | I7 | 49 | Psychologist | 29 | 4 |
| I8 | 67 | Nurse | 60 | 3 | |
| I9 | 22 | Psychiatrist | 49 | 20 | |
| I10 | 48 | Psychiatrist | 30 | 0.5 | |
| CRP 4 | I11 | 62 | Child psychiatrist | 38 | 1 |
| I12 | 35 | Psychologist | 27 | 4 | |
| I13 | 60 | Psychologist | 32 | 7 | |
| CRP 5 | I14 | 74 | Psychologist | 46 | 10 |
| I15 | 29 | Secretary | 49 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salome, G.; Vignaud, P.; Galia, P.; Prieto, N.; Chauliac, N. Determinants of Care Pathways for C-PTSD Patients in French Psychotrauma Centers: A Qualitative Study. Int. J. Environ. Res. Public Health 2023, 20, 6278. https://doi.org/10.3390/ijerph20136278
Salome G, Vignaud P, Galia P, Prieto N, Chauliac N. Determinants of Care Pathways for C-PTSD Patients in French Psychotrauma Centers: A Qualitative Study. International Journal of Environmental Research and Public Health. 2023; 20(13):6278. https://doi.org/10.3390/ijerph20136278
Chicago/Turabian StyleSalome, Germain, Philippe Vignaud, Perrine Galia, Nathalie Prieto, and Nicolas Chauliac. 2023. "Determinants of Care Pathways for C-PTSD Patients in French Psychotrauma Centers: A Qualitative Study" International Journal of Environmental Research and Public Health 20, no. 13: 6278. https://doi.org/10.3390/ijerph20136278