
Violence across the Life Course and Implications for Intervention Design: Findings from the Maisha Fiti Study with Female Sex Workers in Nairobi, Kenya
 , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling
2.2. Ethics and Informed Consent
2.3. Behavioural–Biological Survey
2.4. Laboratory Methods
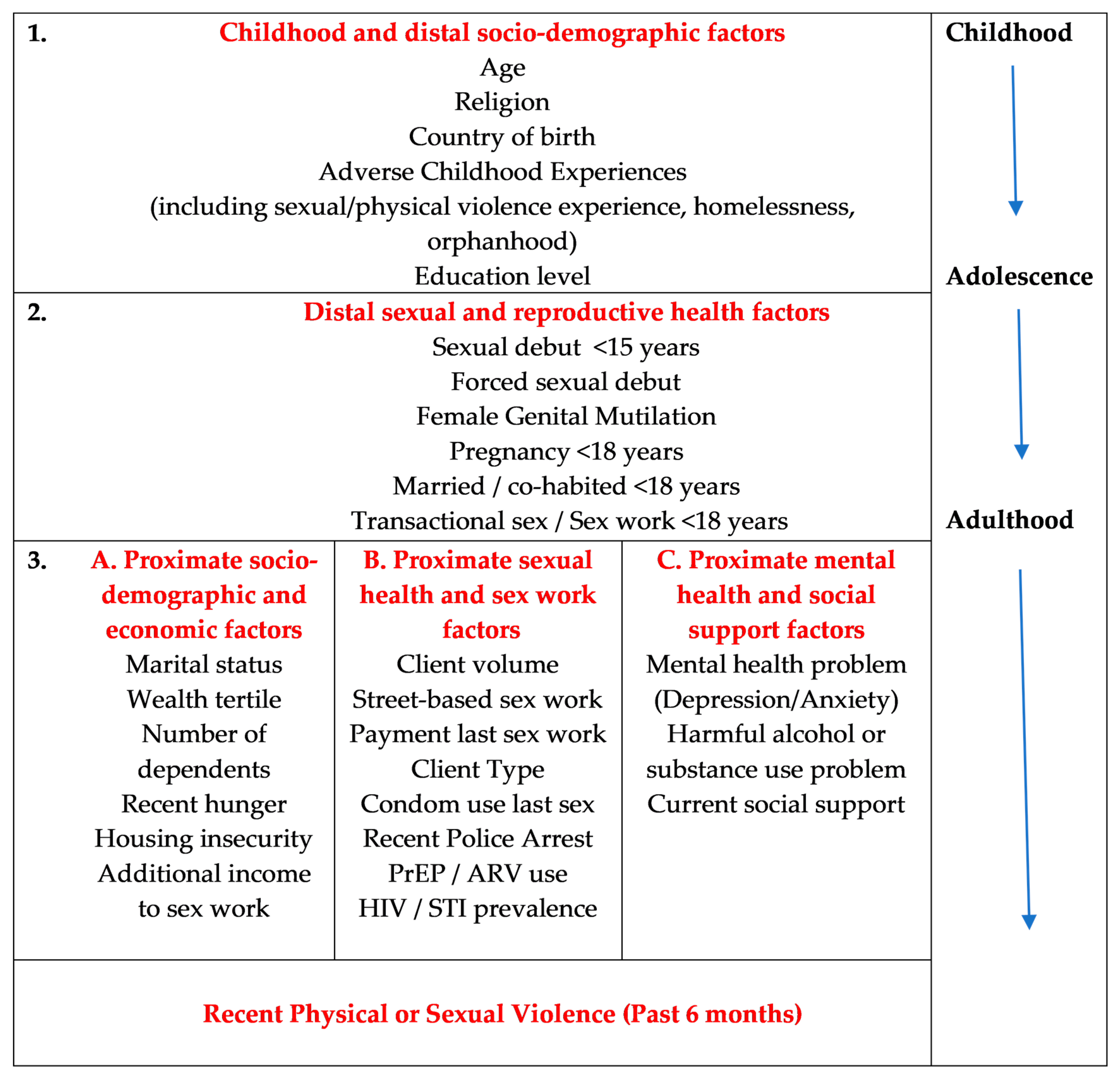
2.5. Conceptual Framework
2.6. Statistical Analyses
3. Results
3.1. Sample Demographics and Sex Work Characteristics
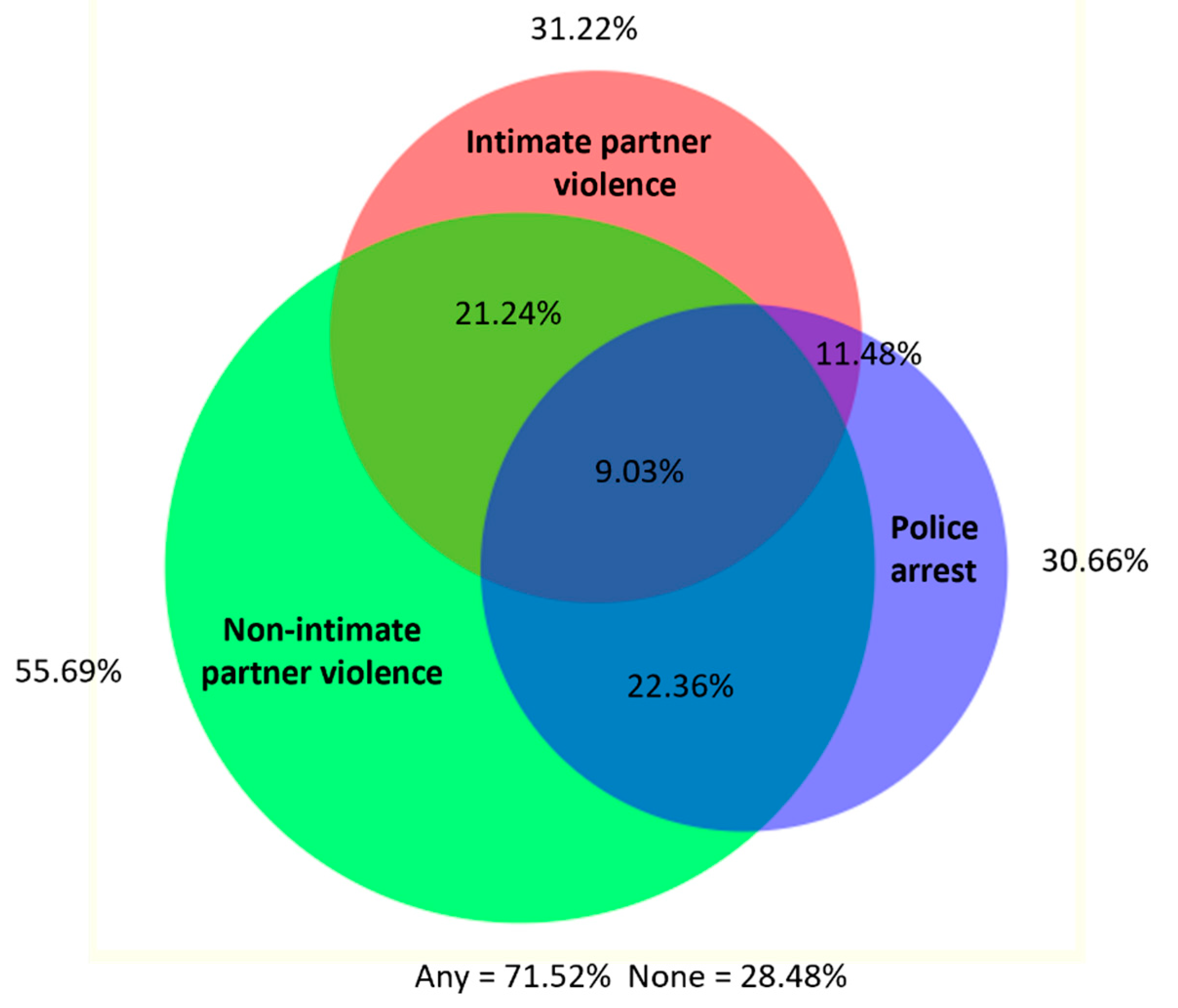
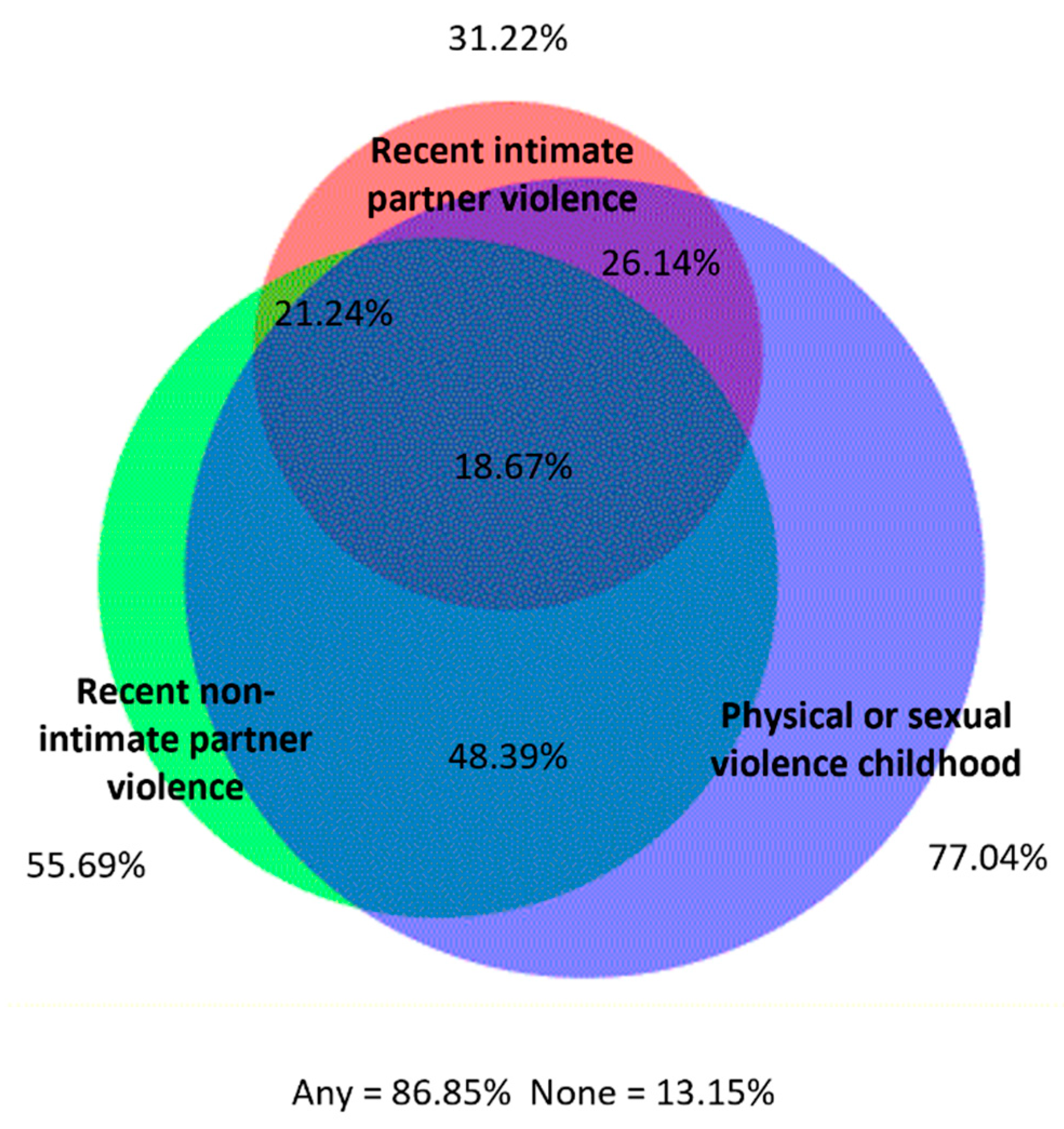
3.2. Violence Experience across the Life-Course
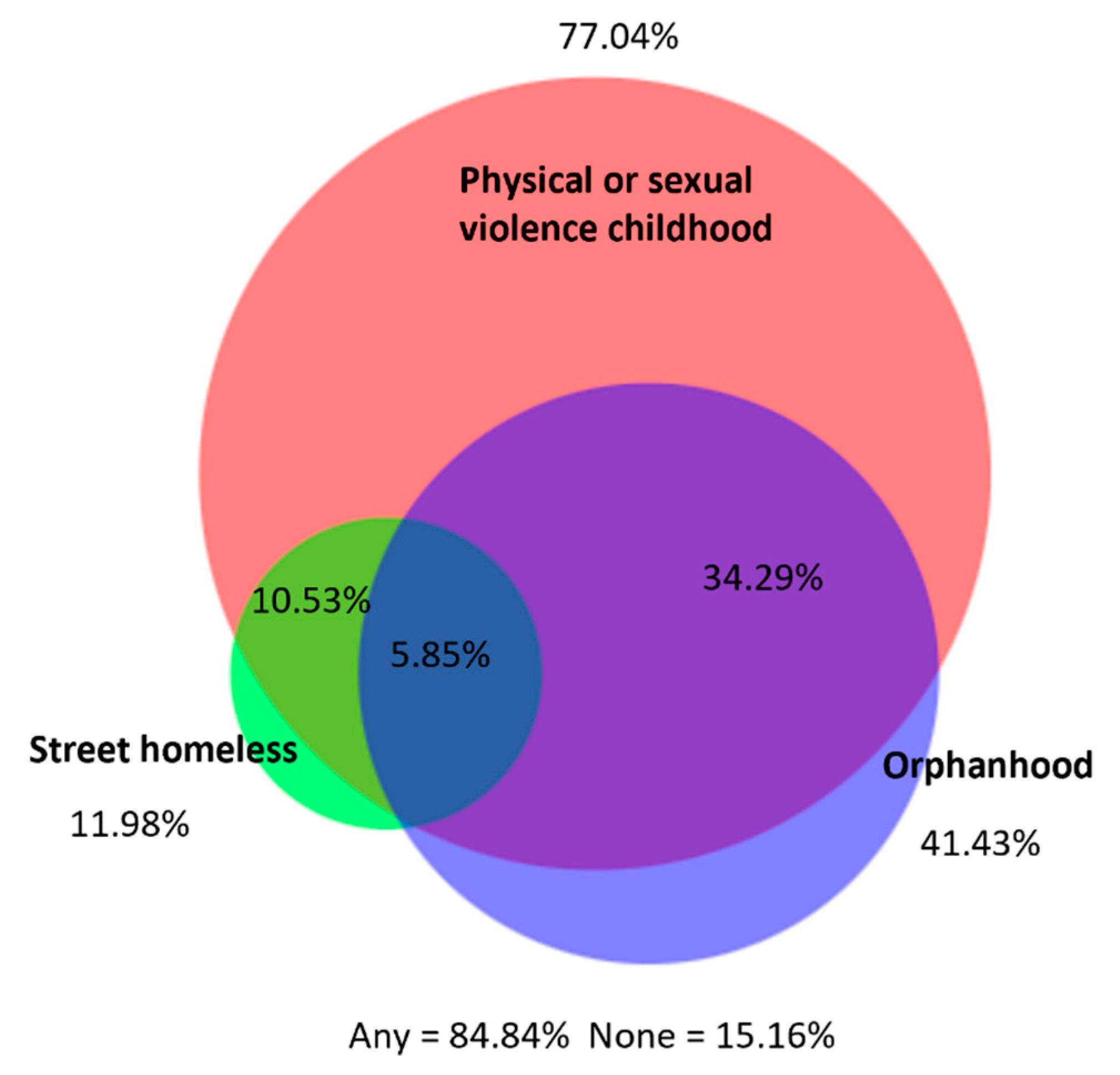
3.3. Witnessing Violence by Children of FSWs
3.4. Associations with Recent Physical or Sexual Violence Experience by Any Perpetrator
3.5. Associations with Recent Physical or Sexual Violence Experience by an Intimate Partner
3.6. Associations with Recent Physical or Sexual Violence Experience by a Non-Intimate Partner
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Violence Against Women Prevalence Estimates, 2018: Global, Regional and National Prevalence Estimates for Intimate Partner Violence Against Women and Global and Regional Prevalence Estimates for Non-Partner Sexual Violence Against Women; World Health Organisation: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240022256 (accessed on 7 July 2022).
- Garcia-Moreno, C.; Jansen, H.A.; Ellsberg, M.; Heise, L.; Watts, C.H. Prevalence of intimate partner violence: Findings from the WHO multi-country study on women’s health and domestic violence. Lancet 2006, 368, 1260–1269. [Google Scholar] [CrossRef]
- Kenya National Bureau of Statistics. The 2014 Kenya Demographic and Health Survey; Kenya National Bureau of Statistics: Nairobi, Kenya, 2015; Available online: https://dhsprogram.com/pubs/pdf/fr308/fr308.pdf (accessed on 30 June 2022).
- Abramsky, T.; Watts, C.H.; Garcia-Moreno, C.; Devries, K.; Kiss, L.; Ellsberg, M.; Jansen, H.A.; Heise, L. What factors are associated with recent intimate partner violence? findings from the WHO multi-country study on women’s health and domestic violence. BMC Public Health 2011, 11, 109. [Google Scholar] [CrossRef] [Green Version]
- Hughes, K.; Bellis, M.A.; Hardcastle, K.A.; Sethi, D.; Butchart, A.; Mikton, C.; Jones, L.; Dunne, M.P. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, e356–e366. [Google Scholar] [CrossRef] [Green Version]
- Jewkes, R.; Fulu, E.; Naved, R.T.; Chirwa, E.; Dunkle, K.; Haardörfer, R.; Garcia-Moreno, C.; on behalf of the UN Multi-country Study on Men and Violence Study Team. Women’s and men’s reports of past-year prevalence of intimate partner violence and rape and women’s risk factors for intimate partner violence: A multicountry cross-sectional study in Asia and the Pacific. PLoS Med. 2017, 14, e1002381. [Google Scholar] [CrossRef] [Green Version]
- Richter, L.; Komárek, A.; Desmond, C.; Celentano, D.; Morin, S.; Sweat, M.; Chariyalertsak, S.; Chingono, A.; Gray, G.; Mbwambo, J.; et al. Reported physical and sexual abuse in childhood and adult HIV risk behaviour in three African countries: Findings from Project Accept (HPTN-043). AIDS Behav. 2014, 18, 381–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunkle, K.L.; Decker, M.R. Gender-based violence and HIV: Reviewing the evidence for links and causal pathways in the general population and high-risk groups. Am. J. Reprod. Immunol. 2013, 69 (Suppl. 1), 20–26. [Google Scholar] [CrossRef] [PubMed]
- Hatcher, A.M.; Gibbs, A.; McBride, R.S.; Rebombo, D.; Khumalo, M.; Christofides, N.J. Gendered syndemic of intimate partner violence, alcohol misuse, and HIV risk among peri-urban, heterosexual men in South Africa. Soc. Sci. Med. 2022, 295, 112637. [Google Scholar] [CrossRef]
- Jewkes, R.; Flood, M.; Lang, J. From work with men and boys to changes of social norms and reduction of inequities in gender relations: A conceptual shift in prevention of violence against women and girls. Lancet 2015, 385, 1580–1589. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Marshall, C.M.; Rees, H.C.; Nunez, A.; Ezeanolue, E.E.; Ehiri, J.E. Intimate partner violence and HIV infection among women: A systematic review and meta-analysis. J. Int. AIDS Soc. 2014, 17, 18845. [Google Scholar] [CrossRef]
- El-Bassel, N.; Mukherjee, T.I.; Stoicescu, C.; Starbird, L.E.; Stockman, J.K.; Frye, V.; Gilbert, L. Intertwined epidemics: Progress, gaps, and opportunities to address intimate partner violence and HIV among key populations of women. Lancet HIV 2022, 9, e202–e213. [Google Scholar] [CrossRef]
- Li, Q.; Li, X.; Stanton, B. Alcohol use among female sex workers and male clients: An integrative review of global literature. Alcohol Alcohol. 2010, 45, 188–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deering, K.N.; Amin, A.; Shoveller, J.; Nesbitt, A.; Garcia-Moreno, C.; Duff, P.; Argento, E.; Shannon, K. A systematic review of the correlates of violence against sex workers. Am. J. Public Health 2014, 104, e42–e54. [Google Scholar] [CrossRef]
- UNAIDS. UNAIDS Data 2020; UNAIDS: Geneva, Switzerland, 2020; Available online: https://www.unaids.org/sites/default/files/media_asset/2020_aids-data-book_en.pdf (accessed on 7 July 2022).
- Platt, L.; Grenfell, P.; Meiksin, R.; Elmes, J.; Sherman, S.G.; Sanders, T.; Mwangi, P.; Crago, A.L. Associations between sex work laws and sex workers’ health: A systematic review and meta-analysis of quantitative and qualitative studies. PLoS Med. 2018, 15, e1002680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbote, D.K.; Nyblade, L.; Kemunto, C.; Giger, K.; Kimani, J.; Mingkwan, P.; Njuguna, S.; Oga, E.; Kraemer, J.D. Police Discrimination, Misconduct, and Stigmatization of Female Sex Workers in Kenya: Associations with Delayed and Avoided Health Care Utilization and Lower Consistent Condom Use. Health Hum. Rights 2020, 22, 199–212. [Google Scholar]
- Okal, J.; Chersich, M.F.; Tsui, S.; Sutherland, E.; Temmerman, M.; Luchters, S. Sexual and physical violence against female sex workers in Kenya: A qualitative enquiry. AIDS Care 2011, 23, 612–618. [Google Scholar] [CrossRef]
- Nyariki, E.; Wanjiru, R.; Shah, P.; Weiss, H.A.; Seeley, J.; Kimani, J.; Beattie, T.S. Managing motherhood—The experience of female sex workers in Nairobi, Kenya. Cult. Health Sex. 2022, in press. [Google Scholar] [CrossRef]
- Panchanadeswaran, S.; Johnson, S.C.; Sivaram, S.; Srikrishnan, A.K.; Latkin, C.; Bentley, M.E.; Solomon, S.; Go, V.F.; Celentano, D. Intimate partner violence is as important as client violence in increasing street-based female sex workers’ vulnerability to HIV in India. Int. J. Drug Policy 2008, 19, 106–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peitzmeier, S.M.; Wirtz, A.L.; Beyrer, C.; Peryshkina, A.; Sherman, S.G.; Colantuoni, E.; Decker, M.R. Polyvictimization Among Russian Sex Workers: Intimate Partner, Police, and Pimp Violence Cluster With Client Violence. J. Interpers. Violence 2021, 36, NP8056–NP8081. [Google Scholar] [CrossRef]
- UNAIDS. Country Factsheets, Kenya 2021. Available online: https://www.unaids.org/en/regionscountries/countries/kenya (accessed on 16 May 2023).
- Kenya National Bureau of Statistics (KNBS). 2019 Kenya Population and Housing Census Volume I: Population by County and Sub-County. 2019. Available online: https://www.knbs.or.ke/publications/ (accessed on 16 May 2023).
- National AIDS and STI Control Programme. Key Population Mapping and Size Estimation in Selected Counties in Kenya: Phase 1; National AIDS and STI Control Programme: Nairobi, Kenya, 2019; Available online: https://hivpreventioncoalition.unaids.org/wp-content/uploads/2020/02/KPSE-Phase1-Final-Report.pdf (accessed on 21 November 2022).
- Devries, K.M.; Mak, J.Y.; Bacchus, L.J.; Child, J.C.; Falder, G.; Petzold, M.; Astbury, J.; Watts, C.H. Intimate partner violence and incident depressive symptoms and suicide attempts: A systematic review of longitudinal studies. PLoS Med. 2013, 10, e1001439. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Adverse Childhood Experiences International Questionnaire (ACE-IQ); World Health Organisation: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-(ace-iq) (accessed on 31 October 2022).
- Beksinska, A.; Jama, Z.; Kabuti, R.; Kungu, M.; Babu, H.; Nyariki, E.; Shah, P.; Nyabuto, C.; Okumu, M.; Mahero, A.; et al. Prevalence and correlates of common mental health problems and recent suicidal thoughts and behaviours among female sex workers in Nairobi, Kenya. BMC Psychiatry 2021, 21, 503. [Google Scholar] [CrossRef]
- Chibanda, D.; Verhey, R.; Gibson, L.J.; Munetsi, E.; Machando, D.; Rusakaniko, S.; Munjoma, R.; Araya, R.; Weiss, H.A.; Abas, M. Validation of screening tools for depression and anxiety disorders in a primary care population with high HIV prevalence in Zimbabwe. J. Affect. Disord. 2016, 198, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Mwangi, P.; Nyongesa, M.K.; Koot, H.M.; Cuijpers, P.; Newton, C.; Abubakar, A. Validation of a Swahili version of the 9-item Patient Health Questionnaire (PHQ-9) among adults living with HIV compared to a community sample from Kilifi, Kenya. J. Affect. Disord. Rep. 2020, 1, 100013. [Google Scholar] [CrossRef]
- Nyongesa, M.K.; Mwangi, P.; Koot, H.M.; Cuijpers, P.; Newton, C.; Abubakar, A. The reliability, validity and factorial structure of the Swahili version of the 7-item generalized anxiety disorder scale (GAD-7) among adults living with HIV from Kilifi, Kenya. Ann. Gen. Psychiatry 2020, 19, 62. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): Manual for Use in Primary Care; World Health Organisation: Paris, France, 2010; Available online: https://apps.who.int/iris/handle/10665/44320 (accessed on 12 July 2022).
- Burton-Jeangros, C.; Cullati, S.; Sacker, A.; Blane, D. (Eds.) Introduction. In A Life Course Perspective on Health Trajectories and Transitions; Springer: Cham, Switzerland, 2015; pp. 1–18. [Google Scholar]
- Heise, L.L. Violence against women: An integrated, ecological framework. Violence Against Women 1998, 4, 262–290. [Google Scholar] [CrossRef] [PubMed]
- Zalwango, F.; Eriksson, L.; Seeley, J.; Nakamanya, S.; Vandepitte, J. Parenting and money making: Sex work and womens choices in urban Uganda. Wagadu 2010, 8, 71–92. [Google Scholar]
- Wanjiru, R.; Nyariki, E.; Babu, H.; Lwingi, I.; Liku, J.; Jama, Z.; Kung’u, M.; Ngurukiri, P.; Nyamweya, C.; Shah, P.; et al. Beaten but not down! Exploring resilience among female sex workers (FSWs) in Nairobi, Kenya. BMC Public Health 2022, 22, 965. [Google Scholar] [CrossRef]
- Pack, A.P.; L’Engle, K.; Mwarogo, P.; Kingola, N. Intimate partner violence against female sex workers in Mombasa, Kenya. Cult. Health Sex. 2014, 16, 217–230. [Google Scholar] [CrossRef]
- Coetzee, J.; Gray, G.E.; Jewkes, R. Prevalence and patterns of victimization and polyvictimization among female sex workers in Soweto, a South African township: A cross-sectional, respondent-driven sampling study. Glob. Health Action 2017, 10, 1403815. [Google Scholar] [CrossRef] [Green Version]
- Mutagoma, M.; Nyirazinyoye, L.; Sebuhoro, D.; Riedel, D.J.; Ntaganira, J. Sexual and physical violence and associated factors among female sex workers in Rwanda: A cross-sectional survey. Int. J. STD AIDS 2019, 30, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Park, J.N.; Decker, M.R.; Bass, J.K.; Galai, N.; Tomko, C.; Jain, K.M.; Footer, K.H.A.; Sherman, S.G. Cumulative Violence and PTSD Symptom Severity Among Urban Street-Based Female Sex Workers. J. Interpers. Violence 2021, 36, 10383–10404. [Google Scholar] [CrossRef]
- Jewkes, R.; Otwombe, K.; Dunkle, K.; Milovanovic, M.; Hlongwane, K.; Jaffer, M.; Matuludi, M.; Mbowane, V.; Hopkins, K.L.; Hill, N.; et al. Sexual IPV and non-partner rape of female sex workers: Findings of a cross-sectional community-centric national study in South Africa. SSM Ment. Health 2021, 1, 100012. [Google Scholar] [CrossRef] [PubMed]
- Decker, M.R.; Lyons, C.; Guan, K.; Mosenge, V.; Fouda, G.; Levitt, D.; Abelson, A.; Nunez, G.T.; Njindam, I.M.; Kurani, S.; et al. A Systematic Review of Gender-Based Violence Prevention and Response Interventions for HIV Key Populations: Female Sex Workers, Men Who Have Sex With Men, and People Who Inject Drugs. Trauma Violence Abus. 2022, 23, 676–694. [Google Scholar] [CrossRef] [PubMed]
- Beattie, T.S.; Bhattacharjee, P.; Isac, S.; Mohan, H.L.; Simic-Lawson, M.; Ramesh, B.M.; Blanchard, J.F.; Moses, S.; Watts, C.H.; Heise, L. Declines in violence and police arrest among female sex workers in Karnataka state, south India, following a comprehensive HIV prevention programme. J. Int. AIDS Soc. 2015, 18, 20079. [Google Scholar] [CrossRef]
- Bhattacharjee, P.; Isac, S.; McClarty, L.M.; Mohan, H.L.; Maddur, S.; Jagannath, S.B.; Venkataramaiah, B.K.; Moses, S.; Blanchard, J.F.; Gurnani, V. Strategies for reducing police arrest in the context of an HIV prevention programme for female sex workers: Evidence from structural interventions in Karnataka, South India. J. Int. AIDS Society 2016, 19, 20856. [Google Scholar] [CrossRef] [Green Version]
- Isac, S.; Ramesh, B.M.; Rajaram, S.; Washington, R.; Bradley, J.E.; Reza-Paul, S.; Beattie, T.S.; Alary, M.; Blanchard, J.F.; Moses, S. Changes in HIV and syphilis prevalence among female sex workers from three serial cross-sectional surveys in Karnataka state, South India. BMJ Open 2015, 5, e007106. [Google Scholar] [CrossRef] [Green Version]
- Decker, M.R.; Wirtz, A.L.; Pretorius, C.; Sherman, S.G.; Sweat, M.D.; Baral, S.D.; Beyrer, C.; Kerrigan, D.L. Estimating the impact of reducing violence against female sex workers on HIV epidemics in Kenya and Ukraine: A policy modeling exercise. Am. J. Reprod. Immunol. 2013, 69 (Suppl. 1), 122–132. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, P.; Morales, G.J.; Kilonzo, T.M.; Dayton, R.L.; Musundi, R.T.; Mbole, J.M.; Malaba, S.J.; Ogwang, B.E.; Isac, S.K.; Moses, S.; et al. Can a national government implement a violence prevention and response strategy for key populations in a criminalized setting? A case study from Kenya. J. Int. AIDS Soc. 2018, 21 (Suppl. 5), e25122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. INSPIRE: Seven Strategies for Ending Violence Against Children; World Health Organisation: Geneva, Switzerland, 2016; Available online: https://www.who.int/publications/i/item/9789241565356 (accessed on 5 July 2022).
- Jones, L.M.; Finkelhor, D.; Halter, S. Child Maltreatment Trends in the 1990s: Why Does Neglect Differ From Sexual and Physical Abuse? Child Maltreatment 2006, 11, 107–120. [Google Scholar] [CrossRef]
- Jewkes, R.; Nduna, M.; Jama-Shai, N.; Chirwa, E.; Dunkle, K. Understanding the Relationships between Gender Inequitable Behaviours, Childhood Trauma and Socio-Economic Status in Single and Multiple Perpetrator Rape in Rural South Africa: Structural Equation Modelling. PLoS ONE 2016, 11, e0154903. [Google Scholar] [CrossRef] [Green Version]
- Yount, K.M.; Krause, K.H.; Miedema, S.S. Preventing gender-based violence victimization in adolescent girls in lower-income countries: Systematic review of reviews. Soc. Sci. Med. 2017, 192, 1–13. [Google Scholar] [CrossRef]
- Shannon, K.; Strathdee, S.A.; Goldenberg, S.M.; Duff, P.; Mwangi, P.; Rusakova, M.; Reza-Paul, S.; Lau, J.; Deering, K.; Pickles, M.R.; et al. Global epidemiology of HIV among female sex workers: Influence of structural determinants. Lancet 2015, 385, 55–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunkle, K.L.; Jewkes, R. Effective HIV prevention requires gender-transformative work with men. Sex. Transm. Infect. 2007, 83, 173–174. [Google Scholar] [CrossRef] [PubMed]
- Fulu, E.; Warner, X.; Miedema, S.; Jewkes, R.; Roselli, T.; Lang, J. Why Do Some Men Use Violence Against Women and How Can We Prevent It? Summary Report of Quantitative Findings From the United Nations Multi-Country Study on Men and Violence in Asia and the Pacific; UNDP; UNFPA; UN Women; UNV: Bangkok, Thailand, 2013. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Tool/Question | Category |
|---|---|---|
| Childhood and Distal Socio-Demographic Factors | ||
| ACEs | WHO Adverse Childhood Experiences International Questionnaire (ACE-IQ) [26] | Individually and Ordered categorical variable (each ACE scores one point): <4, 5–8, 9–12 [27] |
| Distal Sexual and Reproductive Health Factors | ||
| Forced sexual debut | Would you say you wanted to have sex that first time, or was it against your will? | I wanted to have sex vs. I was tricked into having sex, or I was pressured into having sex vs. I was physically forced to have sex |
| Female Genital Mutilation | Have you ever had a surgical procedure used for modifying the vagina or restoration of the hymen, including female genital circumcision, incision with insertion of substance into the lesion? | No vs. Yes |
| Age at first sex work | How old were you when you first received money/goods in exchange for sex? | <18, 18–24, 25–40 years |
| Proximate Socio-Demographic and Economic Factors | ||
| Wealth Tertiles | 14 household asset questions used in the Kenyan Demographic Health Surveys [3] | Principle component analysis (PCA) used to compute household wealth tertiles: Low, Medium, High |
| Number of dependents | Not including yourself, how many people living in your household are dependent on your income? How many people outside your household are dependent on your income? | 0–1, 2–3, 4+ dependents |
| Recent hunger | Thinking now about the past 7 days, have you or anyone in your family skipped a meal because there was not enough food? | No vs. Yes |
| Proximate Sexual Health and Sex Work Factors | ||
| Recent police arrest | Have you been arrested in the past 6 months because you are a sex worker? | No vs. Yes |
| Current PrEp/PEP/ARV use | Are you currently taking PrEP? (HIV negative) Are you currently taking PEP? (HIV negative) Are you currently taking ARVs? (HIV positive) | No vs. Yes |
| Proximate Mental Health, Alcohol and Substance Use and Social Support Factors | ||
| Depression | Patient Health Questionnaire-9 (PHQ-9) [28,29] | none 0–4; mild 5–9; moderate-severe 10+ |
| Anxiety | Generalised Anxiety Disorder-7 Assessment (GAD-7) [28,30] | None 0–4; mild 5–9; moderate-severe 10+ |
| Harmful alcohol use | WHO ASSIST (Alcohol, Smoking and Substance Involvement Screening Test) tool [31] | Low risk 0–10; moderate risk ≥11; high risk >27 |
| Harmful substance use | WHO ASSIST (Alcohol, Smoking and Substance Involvement Screening Test) tool [31] | Low risk 0–4; moderate risk >4; high risk >27 |
| Current social support | Do you have someone who you can talk to about your problems? | Yes/Sometimes vs. No |
| n 1003 | % | % Physical or Sexual Violence by any Perpetrator Past 6 Months (n = 646) | ||
|---|---|---|---|---|
| Childhood and Distal Socio-Demographic Factors | ||||
| Age (years) | 18–24 | 212 353 438 | 11.7 39.4 48.9 | 60.4 70.8 61.2 |
| 25–34 | ||||
| 35–45 | ||||
| Mean Age 33.7 (SD 7.1) | ||||
| Religion | Catholic | 375 | 36.9 | 62.0 |
| Protestant | 534 | 54.4 | 67.2 | |
| Muslim | 46 | 4.6 | 68.3 | |
| Other/None | 46 | 4.1 | 57.8 | |
| Country of birth | Kenya | 989 | 98.7 | 65.2 |
| Other | 14 | 1.3 | 45.8 | |
| Total number of Adverse Childhood Experiences * | 0–4 | 282 | 28.4 | 43.1 |
| 5–8 | 548 | 54.3 | 69.6 | |
| 9–12 | 173 | 17.3 | 85.8 | |
| Education Level | <Primary | 169 | 17.8 | 63.0 |
| Primary only | 525 | 52.3 | 65.5 | |
| ≥Secondary | 309 | 29.9 | 64.9 | |
| Distal Sexual and Reproductive Health Factors | ||||
| Age at sexual debut (years) | <16 | 369 | 37.3 | 69.8 |
| 16–17 | 312 | 30.0 | 66.2 | |
| 18+ | 315 | 32.7 | 58.1 | |
| Sexual debut forced | Consented | 695 | 68.8 | 60.4 |
| Tricked/pressured | 194 | 19.6 | 71.4 | |
| Forced | 110 | 11.6 | 80.2 | |
| Eldest child conceived when <18 years | No | 517 | 52.4 | 63.1 |
| Yes | 486 | 47.7 | 66.9 | |
| Married/co-habited < 18 years | No | 759 | 75.8 | 64.0 |
| Yes | 244 | 24.3 | 67.8 | |
| Age at first sex work | <18 | 176 | 16.6 | 71.2 |
| 18–24 | 474 | 44.9 | 65.6 | |
| 25–40 | 341 | 38.5 | 61.6 | |
| Proximate socio-demographic and economic Factors | ||||
| Current Intimate Partner | No | 392 | 40.2 | 59.6 |
| Yes | 610 | 59.8 | 68.4 | |
| Current living status | Lives alone | 139 | 13.8 | 53.6 |
| Lives with parents/friends | 103 | 7.7 | 60.4 | |
| Lives with children only | 693 | 7.2 | 66.6 | |
| Lives with partner (+/− children) | 67 | 6.8 | 74.6 | |
| Number of children living with her | None | 113 | 12.3 | 58.6 |
| 1–2 | 558 | 64.7 | 66.4 | |
| 3+ | 193 | 23.0 | 71.3 | |
| Wealth Tertile | Low | 334 | 32.6 | 71.4 |
| Medium | 333 | 33.5 | 68.0 | |
| High | 333 | 34.0 | 55.4 | |
| Number of people dependent on her income | 0–1 | 178 | 15.4 | 54.3 |
| 2–3 | 475 | 48.6 | 63.9 | |
| 4+ | 350 | 36.0 | 70.7 | |
| Recent hunger past 7 days | No | 670 | 66.1 | 59.6 |
| Yes | 331 | 33.9 | 75.0 | |
| Additional income to sex work | No | 571 | 56.4 | 68.4 |
| Yes | 432 | 43.7 | 60.4 | |
| Proximate Sexual Health and Sex Work Factors | ||||
| Client volume past week | <5 | 607 | 60.9 | 62.4 |
| 5–9 | 250 | 24.8 | 70.9 | |
| 10+ | 137 | 14.2 | 66.0 | |
| Place where solicit clients | Phone/internet | 54 | 5.4 | 61.9 |
| Home/middle-men/markets | 15 | 1.6 | 67.9 | |
| Brothel/escort service/massage | 14 | 1.5 | 53.9 | |
| Bar/club/lodge | 620 | 61.5 | 62.5 | |
| Street/bus/taxi | 294 | 30.0 | 71.5 | |
| Condom use last sex with a client | No | 174 | 17.3 | 67.2 |
| Yes | 819 | 82.7 | 64.5 | |
| Condom use last sex (any partner) | No | 236 | 22.8 | 70.7 |
| Yes | 765 | 77.2 | 63.1 | |
| HIV prevalence | Negative | 746 | 72.0 | 65.6 |
| Positive | 257 | 28.0 | 63.1 | |
| Bacterial STI prevalence ** | None | 891 | 89.8 | 64.9 |
| One+ | 112 | 10.2 | 65.2 | |
| Proximate Mental Health, Alcohol and Substance Use and Social Support factors | ||||
| Depression or Anxiety score (PHQ-9/GAD-7) | Low | 481 | 47.1 | 58.2 |
| Mild | 279 | 27.9 | 67.9 | |
| Moderate/Severe | 243 | 25.0 | 74.1 | |
| Alcohol risk score (WHO ASSIST) | Low 0–10 | 697 | 70.2 | 59.2 |
| Moderate 11–26 | 207 | 20.4 | 73.6 | |
| High 27+ | 95 | 9.4 | 88.1 | |
| Substance *** risk score (WHO ASSIST) | Low | 759 | 96.4 | 61.7 |
| Moderate | 228 | 21.8 | 73.9 | |
| High | 18 | 1.8 | 90.7 | |
| Has someone can talk to | No | 278 | 27.5 | 64.4 |
| Yes | 725 | 72.5 | 65.1 | |
| Belongs to an FSW CBO | No | 907 | 90.4 | 63.4 |
| Yes | 96 | 9.6 | 78.6 | |
| n | % | ||
|---|---|---|---|
| Childhood violence experiences (<18 years old) | Witnessed physical abuse at home | 707 | 70.7 |
| Experienced verbal abuse | 609 | 61.3 | |
| Experienced threats of or actual abandonment | 433 | 43.5 | |
| Experienced physical abuse | 656 | 65.8 | |
| Experienced sexual violence | 460 | 46.2 | |
| Experienced physical or sexual violence | 769 | 77.0 | |
| Witnessed community violence | 896 | 88.7 | |
| Experienced war/collective violence | 353 | 34.3 | |
| Experienced physical violence from soldiers, police, militia, or gangs | 104 | 10.5 | |
| Had a family member or friend who was beaten up or killed | 192 | 19.5 | |
| Experienced female genital cutting | 60 | 6.3 | |
| Experienced forced sexual debut | 110 | 11.6 | |
| Violence experiences from any perpetrator (IP or non-IP) | Physical or sexual violence ever | 811 | 81.6 |
| Emotional violence in the past 6 months | 746 | 74.8 | |
| Physical violence in the past 6 months | 552 | 55.0 | |
| Sexual violence in the past 6 months | 499 | 50.6 | |
| Sexual violence in the past 7 days | 61 | 6.4 | |
| Physical or sexual violence in the past 6 months | 646 | 64.9 | |
| Drugged or imprisoned in the past 6 months | 221 | 22.1 | |
| Intimate partner violence (IPV) experiences | Physical or sexual violence ever | 560 | 56.3 |
| Emotional violence in the past 6 months | 302 | 29.5 | |
| Physical violence in the past 6 months | 254 | 25.2 | |
| Sexual violence in the past 6 months | 220 | 22.6 | |
| Sexual violence in the past 7 days | 44 | 4.6 | |
| Physical or sexual violence in the past 6 months | 313 | 31.2 | |
| Drugged or imprisoned in the past 6 months | 68 | 6.9 | |
| Violence experiences from others (non-IP) | Physical or sexual violence ever | 688 | 69.2 |
| Emotional violence in the past 6 months | 698 | 70.1 | |
| Physical violence in the past 6 months | 446 | 44.7 | |
| Sexual violence in the past 6 months | 397 | 40.1 | |
| Gang rape in the past 6 months | 23 | 2.4 | |
| Sexual violence in the past 7 days | 27 | 2.8 | |
| Physical or sexual violence in the past 6 months | 554 | 55.7 | |
| Drugged or imprisoned by non-IP in the past 6 months | 184 | 18.5 | |
| Police experiences | Arrested ever because of sex work | 563 | 58.4 |
| Arrested in the past 6 months because of sex work | 302 | 30.7 | |
| Avoided arrest in the past 6 months using sex | 67 | 6.8 | |
| Imprisoned in the past 6 months because of sex work | 61 | 6.5 |
| n = 911 * | % | ||
|---|---|---|---|
| Children <18 years | Children witness IP violence ever | 211 | 23.8 |
| Children witness non-IP violence ever | 139 | 15.7 | |
| Children witness IP or non-IP violence ever | 297 | 33.5 | |
| Children witness IP violence in the past 6 months | 100 | 11.0 | |
| Children witness non-IP violence in the past 6 months | 89 | 10.1 | |
| Children witness IP or non-IP violence in the past 6 months | 163 | 18.1 |
| n (% *) | Crude Odds Ratio (95% CI) | Adjusted Odds Ratio ** (95% CI) | p-Value *** | |||
|---|---|---|---|---|---|---|
| Model 1 | Age (years) | 18–24 | 212 (60.4) | Ref | Ref | 0.3 |
| 25–34 | 353 (70.8) | 1.59 (1.12–2.26) | 1.73 (1.18–2.53) | |||
| 35–45 | 438 (61.2) | 1.03 (0.74–1.44) | 1.12 (0.78–1.62) | |||
| Total number of Adverse Childhood Experiences | 0–4 | 282 (43.1) | Ref | Ref | <0.001 | |
| 5–8 | 548 (69.6) | 3.02 (2.25–4.05) | 3.01 (2.23–4.07) | |||
| 9–12 | 173 (85.8) | 7.98 (4.97–12.81) | 7.92 (4.93–12.74) | |||
| Model 2 | Sexual debut forced | Consented | 695 (60.4) | Ref | Ref | 0.003 |
| Tricked/Pressured | 194 (71.4) | 1.64 (1.16–2.31) | 1.40 (0.97–2.03) | |||
| Forced | 110 (80.2) | 2.65 (1.63–4.31) | 1.97 (1.18–3.29) | |||
| Model 3A | Current Intimate Partner | No | 392 (59.6) | Ref | Ref | 0.0006 |
| Yes | 610 (68.4) | 1.47 (1.13–1.90) | 1.67 (1.25–2.23) | |||
| Number of people dependent on her income | 0–1 | 178 (54.3) | Ref | Ref | 0.07 | |
| 2–3 | 475 (63.9) | 1.49 (1.05–2.12) | 1.31 (0.88–1.95) | |||
| 4+ | 350 (70.7) | 2.03 (1.40–2.96) | 1.52 (0.98–2.34) | |||
| Additional income from sex work | No | 571 (68.4) | Ref | Ref | 0.004 | |
| Yes | 432 (60.4) | 0.71 (0.55–0.91) | 0.65 (0.49–0.87) | |||
| Recent hunger past 7 days | No | 670 (59.6) | Ref | Ref | 0.04 | |
| Yes | 331 (75.0) | 2.03 (1.52, 2.70) | 1.39 (1.01, 1.92) | |||
| Model 3B | Street-based sex work | No | 705 (62.2) | Ref | Ref | 0.08 |
| Yes | 294 (71.5) | 1.52 (1.14–2.04) | 1.34 (0.97–1.85) | |||
| Condom use last sex (any partner) | No | 236(70.7) | Ref | Ref | 0.04 | |
| Yes | 765 (63.1) | 0.71 (0.52–0.97) | 0.68 (0.48, 0.98) | |||
| Current Prep, PEP or ARV use | No | 540 (65.0) | Ref | Ref | 0.8 | |
| Yes | 450 (65.3) | 1.02 (0.79–1.32) | 1.04 (0.77–1.40) | |||
| Police Arrest past 6 months | No | 701 (58.0) | Ref | Ref | <0.001 | |
| Yes | 302 (80.4) | 2.96 (2.16–4.06) | 2.40 (1.71–3.39) | |||
| Model 3C | Depression or Anxiety score (PHQ-9/GAD-7) | Low | 481 (58.2) | Ref | Ref | 0.5 |
| Mild | 279 (67.9) | 1.51 (1.11–2.06) | 1.26 (0.89–1.78) | |||
| Moderate/Severe | 243 (74.1) | 2.05 (1.47–2.87) | 1.09 (0.73–1.62) | |||
| Alcohol risk score (WHO ASSIST) | Low 0–10 | 697 (59.2) | Ref | Ref | <0.001 | |
| Moderate 11–26 | 207 (73.6) | 1.92 (1.37–2.71) | 1.37 (0.94–2.01) | |||
| High 27+ | 95 (88.1) | 5.11 (2.77–9.42) | 3.34 (1.74–6.42) | |||
| Social support | Not CBO member | 907 (63.4) | Ref | Ref | 0.01 | |
| Belongs to CBO | 96 (78.6) | 2.12 (1.30–3.48) | 1.91 (1.14–3.21) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beattie, T.S.; Kabuti, R.; Beksinska, A.; Babu, H.; Kung’u, M.; The Maisha Fiti Study Champions; Shah, P.; Nyariki, E.; Nyamweya, C.; Okumu, M.; et al. Violence across the Life Course and Implications for Intervention Design: Findings from the Maisha Fiti Study with Female Sex Workers in Nairobi, Kenya. Int. J. Environ. Res. Public Health 2023, 20, 6046. https://doi.org/10.3390/ijerph20116046
Beattie TS, Kabuti R, Beksinska A, Babu H, Kung’u M, The Maisha Fiti Study Champions, Shah P, Nyariki E, Nyamweya C, Okumu M, et al. Violence across the Life Course and Implications for Intervention Design: Findings from the Maisha Fiti Study with Female Sex Workers in Nairobi, Kenya. International Journal of Environmental Research and Public Health. 2023; 20(11):6046. https://doi.org/10.3390/ijerph20116046
Chicago/Turabian StyleBeattie, Tara S., Rhoda Kabuti, Alicja Beksinska, Hellen Babu, Mary Kung’u, The Maisha Fiti Study Champions, Pooja Shah, Emily Nyariki, Chrispo Nyamweya, Monica Okumu, and et al. 2023. "Violence across the Life Course and Implications for Intervention Design: Findings from the Maisha Fiti Study with Female Sex Workers in Nairobi, Kenya" International Journal of Environmental Research and Public Health 20, no. 11: 6046. https://doi.org/10.3390/ijerph20116046