1. Introduction
COVID-19 pandemic have caused devastating socio-economic impacts, affecting not just human lives, but also trade, economy and businesses and other aspects [
1,
2]. Vaccines became the most important tool for every country to get on the path for recovery. However, the wide-spread acceptance of the vaccines cannot be taken for granted, despite the COVID-19 vaccine being considered one of the most important scientific breakthroughs and health interventions to give herd immunity and end the pandemic [
3]. For example, as of early June 2021, less than half of all eligible Americans (48.6%) were “fully vaccinated” (People who have received an accepted single-dose vaccine or the second dose in a two dose COVID-19 vaccine series). Referring to the same period, other countries such as South Korea itself had low vaccinated rates (less than 10% were fully vaccinated). Even until now, there are still 32% of Americans not fully vaccinated yet [
4].
The willingness to accept COVID-19 vaccines is primarily influenced by the information environment, especially given the lockdowns and remote work conditions that have made reliance on media much stronger [
5]. Today, individuals increasingly rely on the internet and digital technology for health-related news and information [
6], but prior research shows that social media usage could be a hurdle for vaccinations [
7]. However, little is known about whether reliance on different digital media for news would influence vaccination uptake differently. In particular, health-related digital media such as health blogs and alternative health media could serve as important health information sources [
8]. Recent research showed that these platforms could fuel health misinformation and affect vaccine intentions as well [
9,
10,
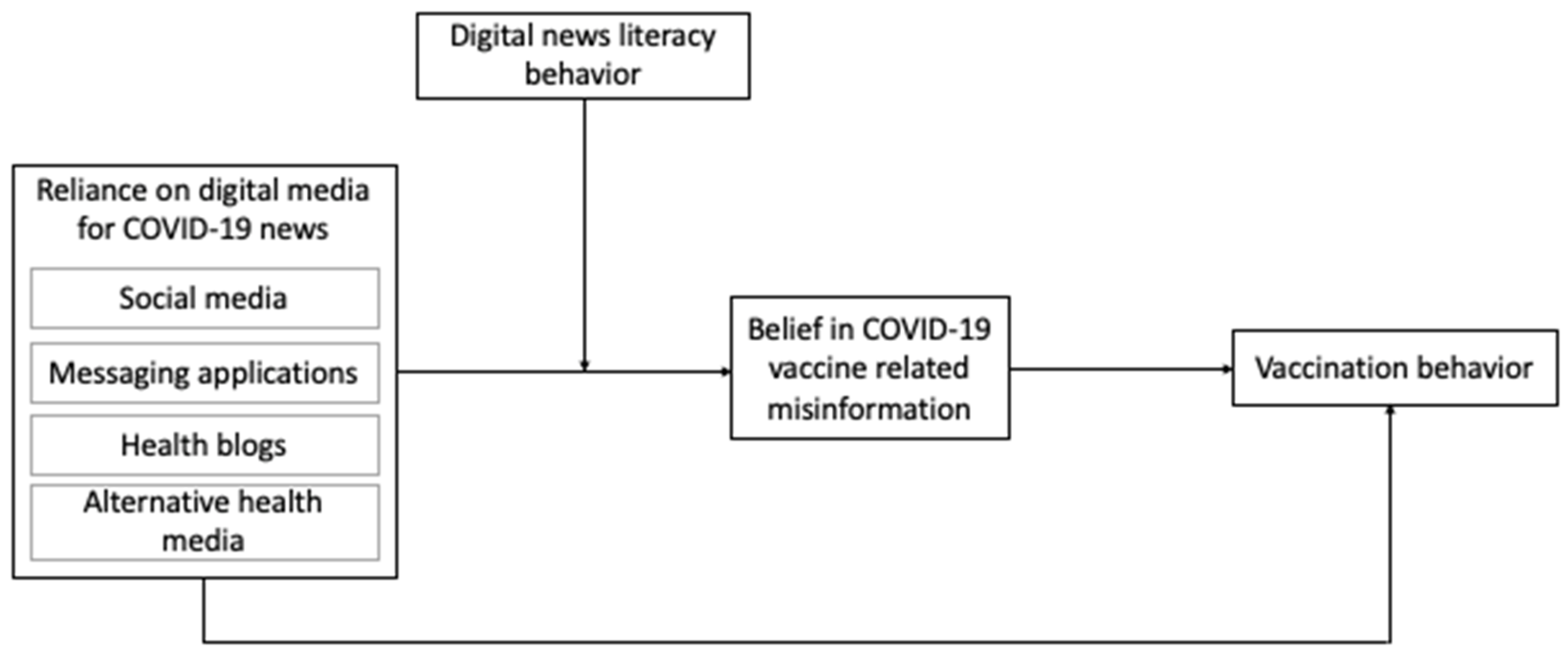
11]. Therefore, this study first investigates how COVID-19 news exposure to diverse digital media, including social media, messaging applications, health blogs, and alternative health media, helps explain vaccination behaviors.
Second, we focus on beliefs in vaccine-related misinformation as an important factor in determining the relationship between news exposure and vaccination behavior. According to the health belief model (HBM), the reason why people will take action to prevent, to screen for, or to control illness conditions could be directly explained by their perceptions such as perceived barriers to health actions [
12]. Misinformation is identified as one important perceived barrier to vaccinations through the lens of HBM [
13]. Additionally, specific cues such as media exposure can also impact the final action an individual takes, and communication scholars tend to conceptualize external cues as the factor that could influence behavior through people’s perceptions [
14]. During health crises such as the COVID-19 pandemic, accessing reliable health information becomes more challenging, whereas vaccine-related misinformation could be easily gained not only from social media but also from other digital platforms such as alternative health media [
15,
16,
17]. Reliance on digital platforms for news acts as a barrier to vaccination to the extent that they may include misinformation about COVID-19 vaccines. Research shows that 409 English-language anti-vaccination social media accounts had 58 million followers [
18]. A high level of misinformation exposure was indeed reported; for example, 73% of Americans had some exposure to misinformation about COVID-19 vaccines in the past 6 months [
19]. The prevalence of vaccine misinformation makes it poignant to understand whether misinformation belief could mediate the relationship between news exposure and vaccination behavior.
Third, we examine the exposure—misinformation belief—vaccination path by taking into account a potentially countervailing factor: individuals’ news literacy behaviors. This is because COVID-19 has led to an unprecedented surge of publications across all areas of knowledge, and individuals are bombarded with a deluge of information about the pandemic over the digital media. So it is crucial to examine how skillfully people dealt with the information overload [
20,
21]. Researchers have pointed out news literacy could be a proactive solution to combatting misinformation [
22,
23], and a few recent studies explored the moderating role of literacy-related factors in the context of media exposure [
15,
24]. However, no study has examined the role of news literacy behaviors so far. News literacy behavior is defined as “the behaviors that occur when people engage with news content in a critical and mindful manner”, which aligns with the core outcome of news literacy programs [
25]. Typical examples of news literacy behavior include using diverse news sources and verifying news content [
25]. Compared to how much knowledge and skills individuals have in navigating the news information environment (i.e., news literacy) and how much they apply news literacy in practice (i.e., news literacy behavior) could be more critical in evaluating news and discerning misinformation.
In sum, we find that there is a lack of research in current literature to (1) understand the mediating role of belief in vaccine misinformation in the relationship between the use of multiple digital media, especially health-specific media, for COVID-19 information and vaccination behavior, and (2) the moderating role of news literacy behavior on this mediated path. This study offers a conceptual model that explains how exposure to different digital media is linked to vaccination via belief in misinformation. We also point out this mediated mechanism can be moderated by news literacy behavior. Further, we compare empirical evidence from two distinct societies (the U.S. vs. South Korea) to see if the model holds in different contexts.
5. Discussion
Although extensive research has found being exposed to and believing in misinformation about COVID-19 vaccines is a challenge for vaccine acceptance [
79,
80], how the countervailing factors such as news literacy could complicate “the information exposure—belief in vaccine misinformation—vaccination” path is yet to be unpacked to understand the communication of scientific information about COVID-19. Our study revealed a significant moderated mediation model where the indirect effects of diverse digital media reliance on vaccination behaviors via vaccine-related misinformation belief were conditioned on NLB. Several intriguing findings merit further discussions.
First, aligning with our expectations, our findings about distinct digital media highlight news exposure through some platforms, particularly messaging applications and AH media, could fuel misinformed beliefs. However, different from our hypotheses, more reliance on social media did not predict stronger belief in vaccine-related misinformation or fewer vaccination behaviors. Despite being different from our expectations, this result about social media should come as no surprise given that some research has indicated that different social media platforms exert different levels of influence on COVID-19 misinformed belief and vaccine willingness. Users of Instagram, YouTube, Snapchat, and TikTok in the UK have a lower willingness to be vaccinated, whereas no significant association is found for Facebook and Twitter [
43]. Due to platform affordances and features, Twitter usage is negatively associated with COVID-19 conspiracy endorsement, but using Facebook and YouTube is more likely to accumulate misinformed beliefs [
81]. Therefore, when treating social media as a whole, it could cancel out individual platforms’ relationships with misbeliefs and result in non-significant results overall.
To answer our research question regarding health blogs, we found it did not have a significant relationship with misinformation belief and vaccination behavior. It is understandable given that patients or laypeople rather than just medical professionals can contribute to the blogosphere, and although laypeople may provide first-hand information about certain diseases such as cancer based on their experience [
56], topics like COVID-19 vaccines are unfamiliar for them, thus related information on health blogs might be less accurate and contain misinformation as well.
While social media is increasingly being regulated to remove and downplay the reach of misinformation, messaging applications and AH media emerge as less regulated grounds for misinformation. Our finding on messaging applications reflects their concerning role in disseminating misinformation, which might be due to their affordance including encrypted technology that protects all text, voice, and media messages, peer-to-peer communication, and group architecture [
82]. These features result in high interactivity index for messaging applications and make it more detrimental to hoodwinking people [
47]. Similarly, our study that brings health-related digital media into misinformation literature showed consumption of AH media was linked to heightened misperception of vaccines, and this finding is the most consistent one across two countries in our research. It also confirms previous research that indicates a strong positive correlation between reliance on AH media and health-related misinformation such as vaccines and genetically modified foods in various contexts [
11,
17,
61,
83]. This again alerts us to pay closer attention to this type of media, especially during the global pandemic rife with misinformation as exposure to it might lead to serious consequences on health matters.
Second, our research indicates misperception of vaccines, to the extent that it is fueled by digital media exposure, acts as an important barrier to vaccination. Specifically, consistent with hypotheses, we found that more reliance on messaging applications or AH media for COVID-19 news was associated with a stronger belief in misinformation, which further led to a lower likelihood to get COVID-19 vaccines. However, this indirect relationship through mediation was largely different from the direct relationship of media reliance on vaccinations where messaging applications reliance predicted stronger vaccination behaviors and AH media reliance was not associated with vaccinations. This shows us that this particular mediation is a partial mediation, such that misinformation beliefs play a mediating role, but do not mediate the entire association between messaging application reliance and vaccine behavior. This mediation suggests it is important to integrate misinformed beliefs to understand the influence of news exposure to different media on health-related behaviors. Although we found that exposure to digital media that can rather easily contain misinformation could fuel vaccine misperceptions and eventually lower vaccinations, we should be alerted that more fact-related news does not necessarily increase vaccination rate as well. Using Twitter data, Lyu et al. [
84] found that more fact-related news was associated with lower vaccination rate in the U.S., which might be because that more fact-related news about the vaccines might raise not only more discussions but more concerns. Further, understanding this mediation process using HBM is in line with prior findings that indicate perceived barriers to self-reported vaccinations involve a misunderstanding of vaccines [
13,
34], and perceived barriers constantly mediate media exposure and behaviors in different contexts [
14].
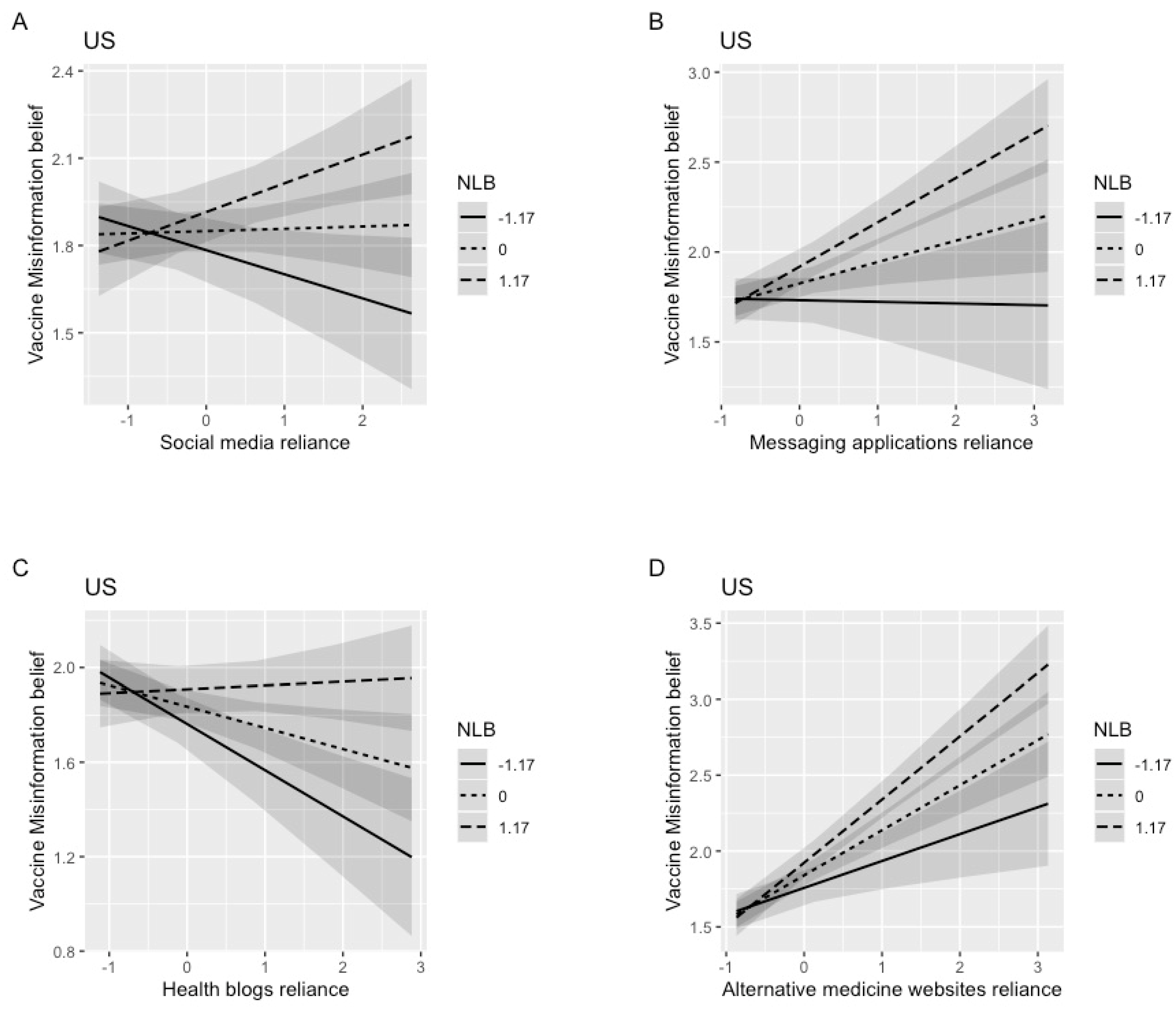
Unexpectedly, different from our hypothesis, our study did not show a protective effect of NLB in the current context. That is to say that NLB moderated the indirect relationship of digital media reliance on vaccination behaviors. Specifically, among those with more NLBs, the indirect association between reliance on messaging applications, AH media or social media, and vaccination behaviors was more negative, whereas the positive indirect association between reliance on health blogs and vaccination behaviors was attenuated. This is because individuals with more NLBs could be more susceptible to vaccine misinformation when they relied on digital media more. This finding is contrary to previous studies which have suggested that NL is a useful tool to save people from the trap of misinformation [
23,
63,
68]. Nevertheless, the moderated mediation relationships reveal the significance of NLB given that only reliance on messaging applications and AH media showed a significant indirect association with vaccination behaviors in the mediation results, whereas after taking NLB into consideration, we found that all types of digital media could have indirect effects on vaccinations through misinformed belief depending on the level of NLB. Hence, NLB is still shown to be an important factor.
Although counterintuitive, current findings for NLB might be explained by motivated reasoning [
85,
86]. Improving news literacy aims to limit reliance on simple, heuristic, or affective cues when individuals process information, increase the thoughtful and systematic routes in messaging processing, hone critical thinking ability, and become more cognitively sophisticated [
87]. However, cognitive sophistication could magnify biased cognitive processing as people tend to be involved in motivated reasoning. So people with greater cognitive sophistication might bolster their views that align with their identities [
88]. Therefore, more NLB might not help people uncover the truth but strengthen misperceptions if they had prior inclinations toward misinformed beliefs about vaccines. This points to the importance of incorporating the pre-existing attitudes towards vaccines into these models in future research to investigate the causes of this counterintuitive finding.
Another potential explanation for this result may be due to individuals’ overconfidence. NLB in our study was measured through self-reporting, but people’s feelings about their news literacy might be untethered from their actual experiences and behaviors [
89]; thus it is possible that some people have a false sense of confidence when it comes to their levels of NLB. Those who have relatively high levels of self-perceived NLB might perceive they have sufficient behavior to evaluate news and information and therefore no further development of the tactics is needed [
89]. Research also found that three in four Americans overestimate their ability to distinguish false news, which in turn influences their perceptions and behaviors such as visiting untrustworthy websites, sharing false information on social media, and believing those contents [
90]. On the other hand, our results suggest that individuals with weaker NLB tend to be less susceptible to vaccine-related misinformation as they get more information on social media or health blogs. Ironically, because these people perceive themselves to be weak in terms of NLB, they may be extra cautious when processing information on these newer platforms, thus becoming more immune to misbeliefs. Simultaneously, this calls for future research using more diverse measurement strategies including cross-validation of behavioral news literacy items.
In terms of societal differences, we only observed the significant moderated mediation model in the U.S, not in the South Korea sample. In making sense of these results, we can first consider the different vaccination rates and sample sizes in Korea vs. the U.S. While data from both countries were collected after seven months since vaccination started in each country, Korea’s vaccination rate was higher than that of the U.S., marking 83% in September 2021 [
91]. The vaccination rate in the U.S. in July 2020 was 67% [
92]. The insignificant results in Korea may be in part due to potential ceiling effects given the high vaccination rates or smaller sample size. In addition, researchers found that scarcity in COVID-19 vaccine supplies may increase vaccine hesitancy [
93], so the vaccine shortage faced by South Korea might influence the public’s perception towards the COVID-19 vaccine, leading to the different results between the U.S. and South Korea samples. Furthermore, public attitudes towards the COVID-19 vaccine have become highly politically polarized in the U.S. [
94], which might also result in the difference in our study. Furthermore, this discrepancy might be attributed to cultural differences. Prior research found a stronger relationship between exposure to misinformation and information avoidance in the South Korea sample compared to the U.S. sample [
95], which reflects the high-uncertainty avoidance culture in South Korea [
96]. Therefore, we suspect that our Korean respondents might tend to avoid some COVID-19 misinformation given that popular misinformation usually contains more persuasive and uncertain words compared to accurate information [
97]. News consumption habits could vary across different cultures, providing promising avenues for future research. Other possible explanations for the country difference might be vaccination campaigns implemented by different societies [
93] or different technology adopted to promote vaccines [
98], which opens more room for future research to explore.
As with all research, our study comes with a few limitations. First, the results are gained from cross-sectional surveys, so they only indicate a correlation rather than a causal relationship. To further examine these relationships, future research should consider using experimental data or panel survey data. Second, the self-reporting of variables such as media reliance for COVID-19 news and news literacy behavior might not reflect participants’ actual behaviors. People might not be able to accurately recall their time spent on getting COVID-19 related news from different media as it may be difficult to separate COVID-19 news from other types of information and from other aims of media usage like entertainment. Furthermore, as mentioned above, people may easily overestimate their levels of NLB. Although we have used an established NLB measure, we may consider adopting more objective measurements in future work. Third and relatedly, we only measured several behaviors and practices in NLB. We may consider other possible applications of news literacy in people’s daily lives such as checking news from unfamiliar sources, evaluating the reliability of news, questioning emotional reactions and bias, or using reverse image search, etc. [
99]. In terms of measures of health blogs, we only asked participants about their usage of health blogs in general, whereas it might be possible that different types of health blogs may have various content quality. For example, blogs that focus on the medical information provided by health professionals could be more reliable than personal journal blogs that primarily are used to archive personal experiences and/or mental states related to personal matters. Therefore, future researchers may consider specifying the meaning of health blogs in questionnaires or examine different types of health blogs in detail. We may also include more items to measure vaccine misperception from multiple aspects. Last, future research could incorporate other factors related to vaccinations such as intentions to get vaccinated [
100], and build a more well-rounded model to explain people’s health decisions.
6. Conclusions
This research shows a significant moderated mediation model, in which the association between online media use and COVID-19 vaccination was mediated through vaccine misperceptions, and this relationship was further moderated by news literacy behavior. Counterintuitively, among those with higher levels of news literacy behavior, the negative indirect association between reliance on social media, messaging applications, or alternative medicine websites and vaccinations was intensified. However, the positive indirect impact of health blogs was attenuated among individuals with stronger news literacy behaviors, compared to those with a low level of news literacy behaviors. Notably, we did not find the above significant relationship in the Korea dataset.
This study has two major practical implications. First, digital media varies in terms of how much it could contribute to people’s vaccine-related misperceptions, so determining which platforms should be paid more attention to is critical for decision-makers to efficiently allocate resources and formulate regulations. In our research, messaging applications and AH media showed a higher likelihood to mislead audiences, which alarms stakeholders that intense scrutiny should not only be on social media giants like Facebook and Twitter but also on other digital media with insidious possibilities to disseminate misinformation. For example, WhatsApp has attempted to limit the number of times a message can be simultaneously forwarded to other users [
101].
Second, although the role of news literacy behaviors did not show a protective effect in the current study, it does not undermine the importance of news literacy education. What is worth reflecting on is what components should news literacy education include. Is educating students to check for different sources or reading the updates and changes to the news story sufficient for combating misinformation? This is in doubt especially when the online information environment might have already been contaminated and rife with misinformation, and people searching for more information from different sources could easily find other news containing similar perspectives due to digital echo chambers and feed algorithms. Although during the pandemic more people check public health websites for facts [
99], we need to be cautious about it given that there lacks information rectification in the current online environment, and fact-checking tools are not popularized yet. Thus simply relying on external tools may not be enough to counter misinformation [
102]; instead, efforts should be directed at building up internal and individualized fortresses such as critical thinking ability to undercut the influence of misinformation, or incorporating the training of discouraging motivated reasoning. Other practical literacy interventions may include teaching people more effective heuristics (e.g., skepticism toward catchy headlines), which should reduce reliance on low-effort processes [
103]. In addition, obtaining news is not the only or the most important purpose to use media; instead, entertainment was selected as the number one reason for media use during the pandemic, especially for young people [
99]. Thus, adopting various news literacy behavior could be time-consuming and tedious that might impede people from adopting news literacy behavior, so educators might think of adding gamification factors in their programs to better improve news literacy [
104].



{kind=link}
{kind=link}
{kind=link}


