
Social Support Initiatives That Facilitate Exercise Participation in Community Gyms for People with Disability: A Scoping Review

Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Selection of Sources of Evidence
2.5. Data Charting Process and Data Items
2.6. Data Synthesis
3. Results
3.1. Characteristics of Included Studies
3.2. Social Support Strategies
3.2.1. Supervision
3.2.2. Peer Support
3.2.3. Specialist Support
3.2.4. Orientation and Familiarisation Sessions
3.2.5. Other Social Support Strategies
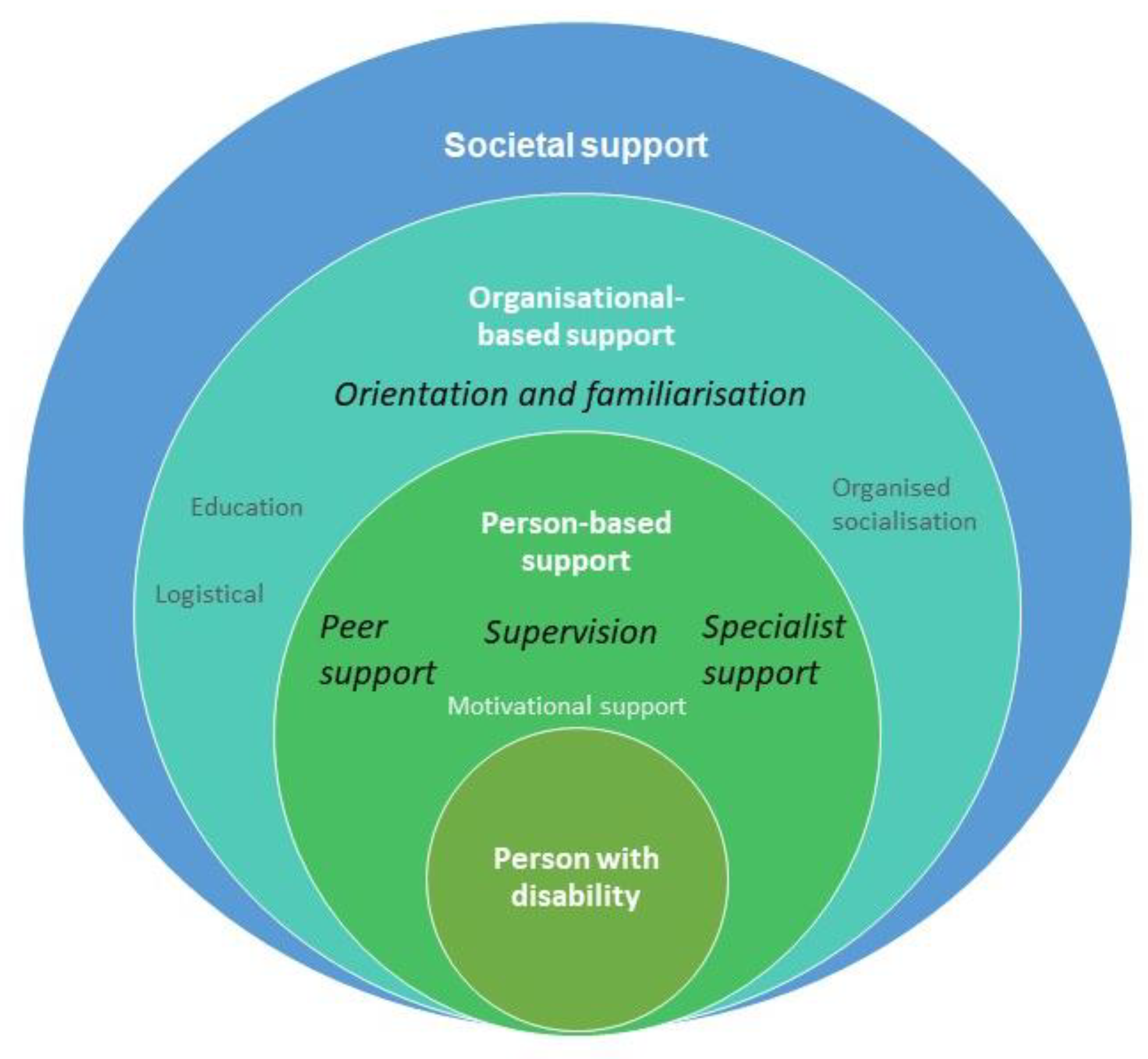
3.3. Mapping Social Supports to the Socio-Ecological Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Section | Item | PRISMA-ScR Checklist Item | Reported on Page # |
|---|---|---|---|
| Title | |||
| Title | 1 | Identify the report as a scoping review. | Page 1 |
| Abstract | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | Page 1 |
| Introduction | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | Pages 1–2 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | Page 2 |
| Methods | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | Page 2 |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | Pages 2–3 |
| Information sources * | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | Pages 3 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | Appendix B |
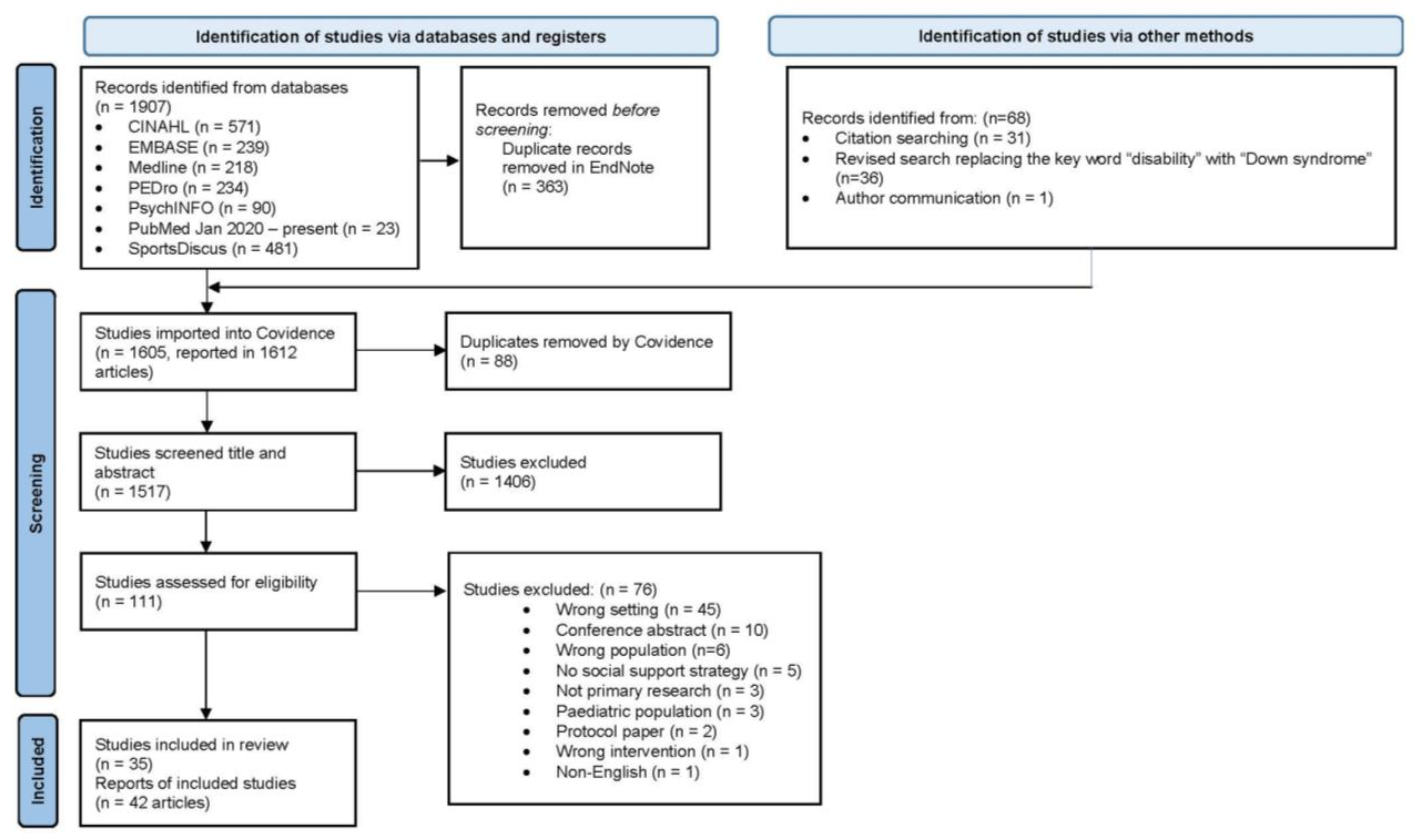
| Selection of sources of evidence † | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | Pages 3 and Figure 1 |
| Data charting process ‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | Page 3 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | Page 3, Appendix C |
| Critical appraisal of individual sources of evidence § | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | N/A |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | Page 3–4 |
| Results | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | Page 3 and Figure 1 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | Page 4 and Table 1 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | N/A |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | Pages 6–9 and Table 2 and Tables S1–S5 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | Pages 6–9 and Table 2 and Tables S1–S5, Figure 2 |
| Discussion | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | Pages 9–11 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | Page 11 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | Page 11 |
| Funding | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | Page 12 |
Appendix B
| Research Question | ||
|---|---|---|
| Identify how social support has been provided to facilitate physical activity participation in community gym settings for adults with disability | ||
| Key Terms | ||
| Concept 1 | Concept 2 | Concept 3 |
|
|
|
| Inclusion Criteria | Exclusion Criteria | |
| ||
| Other Information | ||
Gym context important. Community gyms–focused
| ||
| Databases | ||
| ||
| Medline Search Example | ||
| # | Searches | Results |
| 1 | disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 305,217 |
| 2 | intellectual disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 67,883 |
| 3 | learning disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 18,728 |
| 4 | developmental disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 24,887 |
| 5 | physical disabilit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 7120 |
| 6 | Intellectual Disability/ | 56,819 |
| 7 | Learning Disabilities/ | 14,401 |
| 8 | Developmental Disabilities/ | 21,310 |
| 9 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 | 305,217 |
| 10 | physical activit*.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 129,700 |
| 11 | participation.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 202,081 |
| 12 | exercise.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 383,902 |
| 13 | mobility.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 180,517 |
| 14 | physical training.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 6191 |
| 15 | movement.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 445,888 |
| 16 | motor skills.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 32,232 |
| 17 | balance.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 278,798 |
| 18 | strength.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 358,126 |
| 19 | fitness.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 100,805 |
| 20 | resistance.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 959,784 |
| 21 | training.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 499,173 |
| 22 | physical fitness.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 33,548 |
| 23 | Exercise/ | 123,719 |
| 24 | 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 | 3,102,649 |
| 25 | community gym.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 5 |
| 26 | community gymnasium.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 11 |
| 27 | gym.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 1390 |
| 28 | gymnasium.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 435 |
| 29 | health facility.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 28,258 |
| 30 | wellness center.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 172 |
| 31 | fitness center.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 247 |
| 32 | health club.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 135 |
| 33 | Fitness Centers/ | 618 |
| 34 | YMCA.mp. [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] | 284 |
| 35 | 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 | 31,311 |
| 37 | 9 and 24 and 35 | 183 |
Appendix C. Social Support Strategies: Types and Definitions
References
- Shields, N.; Synnot, A. Perceived barriers and facilitators to participation in physical activity for children with disability: A qualitative study. BMC Pediatr. 2016, 16, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, N.; Synnot, A.J.; Barr, M. Perceived barriers and facilitators to physical activity for children with disability: A systematic review. Br. J. Sport. Med. 2012, 46, 989–997. [Google Scholar] [CrossRef]
- McKenzie, G.; Willis, C.; Shields, N. Barriers and facilitators of physical activity participation for young people and adults with childhood-onset physical disability: A mixed methods systematic review. Dev. Med. Child Neurol. 2021, 63, 914–924. [Google Scholar] [CrossRef] [PubMed]
- Berkman, L.F.; Glass, T.; Brissette, I.; Seeman, T.E. From social integration to health: Durkheim in the new millennium. Soc. Sci. Med. 2000, 51, 843–857. [Google Scholar] [CrossRef] [PubMed]
- Mahy, J.; Shields, N.; Taylor, N.F.; Dodd, K.J. Identifying facilitators and barriers to physical activity for adults with down syndrome. J. Intellect. Disabil. Res. 2010, 54, 795–805. [Google Scholar] [CrossRef]
- UN General Assembly. Convention on the Rights of Persons with Disabilities; United Nations: New York, NY, USA, 2006. [Google Scholar]
- Carlon, S.L.; Taylor, N.F.; Dodd, K.J.; Shields, N. Differences in habitual physical activity levels of young people with cerebral palsy and their typically developing peers: A systematic review. Disabil. Rehabil. 2013, 35, 647–655. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [Green Version]
- Ryan, J.M.; Walsh, M.; Owens, M.; Byrne, M.; Kroll, T.; Hensey, O.; Kerr, C.; Norris, M.; Walsh, A.; Lavelle, G.; et al. Transition to adult services experienced by young people with cerebral palsy: A cross-sectional study. Dev. Med. Child Neurol. 2022. [Google Scholar] [CrossRef]
- Young, N.L.; Barden, W.S.; Mills, W.A.; Burke, T.A.; Law, M.; Boydell, K. Transition to adult-oriented health care: Perspectives of youth and adults with complex physical disabilities. Phys. Occup. Ther. Pediatr. 2009, 29, 345–361. [Google Scholar] [CrossRef]
- George, C.L.; Oriel, K.N.; Blatt, P.J.; Marchese, V. Impact of a community-based exercise program on children and adolescents with disabilities. J. Allied Health 2011, 40, e55–e60. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol. Psychol. Can. 2008, 49, 182–185. [Google Scholar] [CrossRef]
- Bandura, A.; Walters, R.H. Social Learning Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1977; Volume 1. [Google Scholar]
- Hassett, L.M.; Moseley, A.M.; Tate, R.L.; Harmer, A.R.; Fairbairn, T.J.; Leung, J. Efficacy of a fitness centre-based exercise programme compared with a home-based exercise programme in traumatic brain injury: A randomized controlled trial. J. Rehabil. Med. 2009, 41, 247–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenzie, G.; Shields, N.; Willis, C. ‘Finding what works for me’—A qualitative study of factors influencing community gym participation for young adults with cerebral palsy. Disabil. Rehabil. 2022, 1–8. [Google Scholar] [CrossRef]
- Richardson, E.V.; Smith, B.; Papathomas, A. Disability and the gym: Experiences, barriers and facilitators of gym use for individuals with physical disabilities. Disabil. Rehabil. 2017, 39, 1950–1957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, N.; Taylor, N.F. A student-led progressive resistance training program increases lower limb muscle strength in adolescents with Down syndrome: A randomised controlled trial. J. Physiother. 2010, 56, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Shields, N.; Taylor, N.F.; Wee, E.; Wollersheim, D.; O’Shea, S.D.; Fernhall, B. A community-based strength training programme increases muscle strength and physical activity in young people with Down syndrome: A randomised controlled trial. Res. Dev. Disabil. 2013, 34, 4385–4394. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Grimshaw, J. A Guide to Knowledge Synthesis: A Knowledge Synthesis Chapter; Canadian Institutes of Health Research: Ottawa, ON, Canada, 2010. [Google Scholar]
- Kennedy, R.A.; Shields, N. Social Support to Facilitate Physical Activity in Community Gyms for Young Adults with Disability: A Scoping Review Protocol. Available online: https://osf.io/td7r5/ (accessed on 19 October 2022).
- Collett, J.; Franssen, M.; Meaney, A.; Wade, D.; Izadi, H.; Tims, M.; Winward, C.; Bogdanovic, M.; Farmer, A.; Dawes, H. Phase II randomised controlled trial of a 6-month self-managed community exercise programme for people with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2017, 88, 204–211. [Google Scholar] [CrossRef]
- Corcos, D.M.; Robichaud, J.A.; David, F.J.; Leurgans, S.E.; Vaillancourt, D.E.; Poon, C.; Rafferty, M.R.; Kohrt, W.M.; Comella, C.L. A two-year randomized controlled trial of progressive resistance exercise for Parkinson’s disease. Mov. Disord. 2013, 28, 1230–1240. [Google Scholar] [CrossRef] [Green Version]
- Dodd, K.; Taylor, N.; Shields, N.; Prasad, D.; McDonald, E.; Gillon, A. Progressive resistance training did not improve walking but can improve muscle performance, quality of life and fatigue in adults with multiple sclerosis: A randomized controlled trial. Mult. Scler. J. 2011, 17, 1362–1374. [Google Scholar] [CrossRef] [PubMed]
- Elsworth, C.; Winward, C.; Sackley, C.; Meek, C.; Freebody, J.; Esser, P.; Izadi, H.; Soundy, A.; Barker, K.; Hilton-Jones, D.; et al. Supported community exercise in people with long-term neurological conditions: A phase II randomized controlled trial. Clin. Rehabil. 2011, 25, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Fenton, S.A.M.; Veldhuijzen van Zanten, J.J.; Metsios, G.S.; Rouse, P.C.; Yu, C.A.; Ntoumanis, N.; Kitas, G.D.; Duda, J.L. Testing a self-determination theory-based process model of physical activity behavior change in rheumatoid arthritis: Results of a randomized controlled trial. Transl. Behav. Med. 2021, 11, 369–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, J.M.; Bell, K.R.; Powell, J.M.; Behr, J.; Dunn, E.C.; Dikmen, S.; Bombardier, C.H. A randomized controlled trial of exercise to improve mood after traumatic brain injury. PM&R 2010, 2, 911–919. [Google Scholar]
- Kovacic, T.; Kovacic, M.; Ovsenik, R.; Zurc, J. The impact of multicomponent programmes on balance and fall reduction in adults with intellectual disabilities: A randomised trial. J. Intellect. Disabil. Res. 2020, 64, 381–394. [Google Scholar] [CrossRef]
- Lampousi, A.-M.; Berglind, D.; Forsell, Y. Association of changes in cardiorespiratory fitness with health-related quality of life in young adults with mobility disability: Secondary analysis of a randomized controlled trial of mobile app versus supervised training. BMC Public Health 2020, 20, 1721. [Google Scholar] [CrossRef]
- Pau, M.; Corona, F.; Coghe, G.; Marongiu, E.; Loi, A.; Crisafulli, A.; Concu, A.; Galli, M.; Marrosu, M.G.; Cocco, E. Quantitative assessment of the effects of 6 months of adapted physical activity on gait in people with multiple sclerosis: A randomized controlled trial [with consumer summary]. Disabil. Rehabil. 2018, 40, 144–151. [Google Scholar] [CrossRef]
- Shields, N.; Bennell, K.L.; Radcliffe, J.; Taylor, N.F. Is strength training feasible for young people with Prader-Willi syndrome? A phase I randomised controlled trial. Physiotherapy 2020, 106, 136–144. [Google Scholar] [CrossRef]
- Shields, N.; Taylor, N.F.; Dodd, K.J. Effects of a community-based progressive resistance training program on muscle performance and physical function in adults with Down syndrome: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2008, 89, 1215–1220. [Google Scholar] [CrossRef]
- Shields, N.; Willis, C.; Imms, C.; McKenzie, G.; van Dorsselaer, B.; Bruder, A.M.; Kennedy, R.A.; Bhowon, Y.; Southby, A.; Prendergast, L.A.; et al. Feasibility of scaling-up a community-based exercise program for young people with disability. Disabil. Rehabil. 2021, 44, 1669–1681. [Google Scholar] [CrossRef]
- Sims, J.; Galea, M.; Taylor, N.; Dodd, K.; Jespersen, S.; Joubert, L.; Joubert, J. Regenerate: Assessing the feasibility of a strength-training program to enhance the physical and mental health of chronic post stroke patients with depression. Int. J. Geriatr. Psychiatry 2009, 24, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Taylor, N.F.; Dodd, K.J.; Baker, R.J.; Willoughby, K.; Thomason, P.; Graham, H.K. Progressive resistance training and mobility-related function in young people with cerebral palsy: A randomized controlled trial. Dev. Med. Child Neurol. 2013, 55, 806–812. [Google Scholar] [CrossRef]
- Wallace, A.; Pietrusz, A.; Dewar, E.; Dudziec, M.; Jones, K.; Hennis, P.; Sterr, A.; Baio, G.; Machado, P.M.; Laurá, M.; et al. Community exercise is feasible for neuromuscular diseases and can improve aerobic capacity. Neurology 2019, 92, e1773–e1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pett, M.; Clark, L.; Eldredge, A.; Cardell, B.; Jordan, K.; Chambless, C.; Burley, J. Effecting healthy lifestyle changes in overweight and obese young adults with intellectual disability. Am. J. Intellect. Dev. Disabil. 2013, 118, 224–243. [Google Scholar] [CrossRef]
- Poliakoff, E.; Galpin, A.J.; McDonald, K.; Kellett, M.; Dick, J.P.; Hayes, S.; Wearden, A.J. The effect of gym training on multiple outcomes in Parkinson’s disease: A pilot randomised waiting-list controlled trial. NeuroRehabilitation 2013, 32, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Obrusnikova, I.; Cavalier, A.R.; Suminski, R.R.; Blair, A.E.; Firkin, C.J.; Steinbrecher, A.M. A Resistance Training Intervention for Adults With Intellectual Disability in the Community: A Pilot Randomized Clinical Trial. Adapt. Phys. Act. Q. 2021, 38, 546–568. [Google Scholar] [CrossRef]
- Danoudis, M.; Iansek, R. A long-term community gym program for people with Parkinson’s disease: A feasibility study of the Monash Health “Health and Fitness” model. Disabil. Rehabil. 2021, 44, 7330–7338. [Google Scholar] [CrossRef]
- Duret, C.; Breuckmann, P.; Louchart, M.; Kyereme, F.; Pepin, M.; Koeppel, T. Adapted physical activity in community-dwelling adults with neurological disorders: Design and outcomes of a fitness-center based program. Disabil. Rehabil. 2020, 44, 536–541. [Google Scholar] [CrossRef]
- Morris, S.; Dodd, K.J.; Morris, M.; Matyas, T. Community-based progressive resistance strength training in traumatic brain injury: A multiple, single-system, trial. Adv. Physiother. 2009, 11, 218–226. [Google Scholar] [CrossRef]
- Ploughman, M.; Shears, J.; Harris, C.; Hogan, S.H.; Drodge, O.; Squires, S.; McCarthy, J. Effectiveness of a novel community exercise transition program for people with moderate to severe neurological disabilities. NeuroRehabilitation 2014, 35, 105–112. [Google Scholar] [CrossRef]
- Taylor, N.F.; Dodd, K.J.; Larkin, H. Adults with cerebral palsy benefit from participating in a strength training programme at a community gymnasium. Disabil. Rehabil. 2004, 26, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Taylor, N.F.; Dodd, K.J.; Prasad, D.; Denisenko, S. Progressive resistance exercise for people with multiple sclerosis. Disabil. Rehabil. 2006, 28, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Temple, V.A.; Stanish, H.I. The feasibility of using a peer-guided model to enhance participation in community-based physical activity for youth with intellectual disability. J. Intellect. Disabil. 2011, 15, 209–217. [Google Scholar] [CrossRef]
- Zanudin, A.; Mercer, T.; Samaan, C.; Jagadamma, K.; McKelvie, G.; van der Linden, M. A community-based exercise program for ambulant adolescents and young adults with cerebral palsy, a feasibility study. Eur. J. Adapt. Phys. Act. 2021, 14, 12. [Google Scholar] [CrossRef]
- Handlery, R.; Regan, E.; Foster Lewis, A.; Larsen, C.; Handlery, K.; Flach, A.; Fritz, S. Active Participation of Care Partners in a Physical Activity Intervention Alongside People with Stroke: A Feasibility Study. Physiother. Can. 2022, 74, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Dodd, K.J.; Taylor, N.F.; McBurney, H.; Larkin, H. Strength training can be enjoyable and beneficial for adults with cerebral palsy. Disabil. Rehabil. 2004, 26, 1121–1127. [Google Scholar] [CrossRef]
- Dodd, K.J.; Taylor, N.F.; Denisenko, S.; Prasad, D. A qualitative analysis of a progressive resistance exercise programme for people with multiple sclerosis. Disabil. Rehabil. 2006, 28, 1127–1134. [Google Scholar] [CrossRef]
- Hansen, A.; Søgaard, K.; Minet, L.R.; Jarden, J.O. A 12-week interdisciplinary rehabilitation trial in patients with gliomas—A feasibility study. Disabil. Rehabil. 2018, 40, 1379–1385. [Google Scholar] [CrossRef]
- Shields, N.; van den Bos, R.; Buhlert-Smith, K.; Prendergast, L.; Taylor, N. A community-based exercise program to increase participation in physical activities among youth with disability: A feasibility study. Disabil. Rehabil. 2019, 41, 1152–1159. [Google Scholar] [CrossRef]
- Carter, M.J.; McCown, K.M.; Forest, S.; Martin, J.; Wacker, R.; Gaede, D.; Fernandez, T.A. Exercise and fitness for adults with developmental disabilities: Case report of a group intervention. Ther. Recreat. J. 2004, 38, 72–84. [Google Scholar]
- Stanish, H.I.; Temple, V.A. Exercise behaviours of youths with intellectual disability under two conditions in a community programme. World Leis. J. 2012, 54, 280–287. [Google Scholar] [CrossRef]
- Obrusnikova, I.; Novak, H.M.; Cavalier, A.R. The Effect of Systematic Prompting on the Acquisition of Five Muscle-Strengthening Exercises by Adults With Mild Intellectual Disabilities. Adapt. Phys. Act. Q. 2019, 36, 447–471. [Google Scholar] [CrossRef]
- Stanish, H.I.; Temple, V.A. Efficacy of a peer-guided exercise programme for adolescents with intellectual disability. J. Appl. Res. Intellect. Disabil. 2012, 25, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Bania, T.A.; Dodd, K.J.; Baker, R.J.; Graham, H.K.; Taylor, N.F. The effects of progressive resistance training on daily physical activity in young people with cerebral palsy: A randomised controlled trial. Disabil. Rehabil. 2016, 38, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Obrusnikova, I.; Cavalier, A.R.; Novak, H.M.; Blair-McKinsey, A.E.; Suminski, R.R. Effects of a Community-Based Familiarization Intervention on Independent Performance of Resistance-Training Exercise Tasks by Adults With Intellectual Disability. Intellect. Dev. Disabil. 2021, 59, 239–255. [Google Scholar] [CrossRef]
- Winward, C.; Life Research, G. Supporting community-based exercise in long-term neurological conditions: Experience from the long-term individual fitness enablement (LIFE) project. Clin. Rehabil. 2011, 25, 579–587. [Google Scholar] [CrossRef] [Green Version]
- Berglind, D.; Nyberg, G.; Willmer, M.; Persson, M.; Wells, M.; Forsell, Y. An eHealth program versus a standard care supervised health program and associated health outcomes in individuals with mobility disability: Study protocol for a randomized controlled trial. Trials 2018, 19, 258. [Google Scholar] [CrossRef] [Green Version]
- National Disability Insurance Scheme (NDIS). Available online: https://www.ndis.gov.au/ (accessed on 20 December 2022).
- Starowicz, J.; Pratt, K.; McMorris, C.; Brunton, L. Mental Health Benefits of Physical Activity in Youth with Cerebral Palsy: A Scoping Review. Phys. Occup. Ther. Pediatr. 2022, 42, 434–450. [Google Scholar] [CrossRef]
- Verschuren, O.; Peterson, M.D.; Balemans, A.C.; Hurvitz, E.A. Exercise and physical activity recommendations for people with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 798–808. [Google Scholar] [CrossRef]
- Enright, E.; Beckman, E.M.; Connick, M.J.; Dutia, I.M.; Macaro, A.; Wilson, P.J.; O’Sullivan, J.; Lavalliere, J.-M.; Block, T.; Johnston, L.M.; et al. Competitive sport, therapy, and physical education: Voices of young people with cerebral palsy who have high support needs. Br. J. Sport. Med. 2021, 55, 524–525. [Google Scholar] [CrossRef]


| Authors | Year | Country | Participants Condition | Sample Size (n) | Female (n) | Age (yrs) Mean (SD) [Range] * | Study Design |
| Adolescents and Young Adults (15–30 Years) n = 11 Studies | |||||||
| Shields et al. [33] | 2008 | Australia | Down syndrome | 20 | 7 | 26.8 (7.8) | Randomised controlled trial |
| Shields & Taylor [17] | 2010 | Australia | Down syndrome | 23 | 6 | 15.6 (1.6) | Randomised controlled trial |
| Shields et al. [18] | 2013 | Australia | Down syndrome | 68 | 30 | 17.9 (2.6) | Randomised controlled trial |
| Temple & Stanish # [47] Stanish & Temple # [57] | 2011 2012 b | Canada | Intellectual disability | 20 | 10 | 17.8 (1.6) | Pre-post-test |
| Stanish & Temple [55] | 2012 a | Canada | Intellectual disability | 10 | 5 | 17.9 (2.3) | Within subject |
| Pett et al. [38] | 2013 | USA | Intellectual disability | 23 | 13 | 24.2 (4.2) | Randomised controlled trial |
| Shields et al. [32] | 2020 | Australia | Prader-Willi syndrome | 16 | 8 | 25.8 (8.2) | Randomised controlled trial |
| Taylor et al. # [36] Bania et al. # [58] | 2013 2016 | Australia | Cerebral palsy | 48 | 22 | 18.4 (2.4) | Randomised controlled trial |
| Zanudin et al. [48] | 2021 | Malaysia | Cerebral palsy | 16 | 6 | 19.3 (3.1) [16–24] | Pre-post-test |
| Shields et al. [53] | 2019 | Australia | Disability | 19 | 9 | 18.4 (4.5) | Feasibility study |
| Shields et al. # [34] McKenzie et al. # [15] | 2021 2022 | Australia | Disability Cerebral Palsy | 163 39 | 61 18 | 20.8 (5.0) [13–30] 20.4 (4.6) | Stepped wedge RCT Qualitative |
| Adults (>30 years) n = 24 studies | |||||||
| Carter et al. [54] | 2004 | USA | Developmental disability | 15 | 1 | 44 [29–69] | Case report |
| Obrusnikova et al. [56] | 2019 | USA | Intellectual disability | 3 | 3 | [24–37] | Multiple-baseline single-subject |
| Kovacic et al. [29] | 2020 | Slovenia | Intellectual disability | 150 | NR | [18–50] | Randomised controlled trial |
| Obrusnikova et al. # [59] Obrusnikova et al. # [40] | 2021 a 2021 b | USA | Intellectual disability | 24 | 8 | 26.4 (7.7) [19–44] | Randomised controlled trial |
| Allen et al. # [50] Taylor et al. # [45] | 2004 2004 | Australia | Cerebral palsy | 10 11 | 4 4 | 45.8 (5.4) [40–56] 47.6 (8.2) [40–66] | Qualitative Pre-post test |
| Dodd et al. # [51] Taylor et al. # [46] | 2006 2006 | Australia | Multiple sclerosis | 9 9 | 7 7 | 45.6 (10.7) [27–61] 45.6 (10.7) | Qualitative Pre-post-test |
| Dodd et al. [25] | 2011 | Australia | Multiple sclerosis | 71 | 52 | 49.1 | Randomised controlled trial |
| Pau et al. [31] | 2018 | Italy | Multiple sclerosis | 22 | 10 | 46 | Randomised controlled trial |
| Hassett et al. [14] | 2009 | Australia | Traumatic brain injury | 62 | 9 | 34 | Randomised controlled trial |
| Morris et al. [43] | 2009 | Australia | Traumatic brain injury | 7 | 1 | [21–63] | Single-system AB |
| Hoffman et al. [28] | 2010 | USA | Traumatic brain injury | 80 | 45 | 38.4 | Randomised controlled trial |
| Sims et al. [35] | 2009 | Australia | Stroke | 45 | 18 | 67.1 (15.2) | Pilot RCT |
| Handlery et al. [49] | 2022 | USA | Stroke | 15 | 3 | 67.6 (11.6) | Pre-post-test |
| Poliakoff et al. [39] | 2013 | UK | Parkinson disease | 32 | 11 | 65.2 | Pilot RCT |
| Corcos et al. [24] | 2013 | USA | Parkinson disease | 48 | 20 | 59 | Randomised controlled trial |
| Collett et al. [23] | 2016 | UK | Parkinson disease | 105 | 44 | 66.5 | Randomised controlled trial |
| Danoudis & Iansek [41] | 2021 | Australia | Parkinson disease | 17 | 4 | 70 (6.7) [59–79] | Pre-post-test |
| Hansen et al. [52] | 2018 | Denmark | Glioma | 24 | 10 | 62 [20–77] | Feasibility study |
| Fenton et al. [27] | 2021 | UK | Rheumatic arthritis | 70 | 46 | 56.4 (12.3) | Randomised controlled trial |
| Lampousi et al. [30] | 2020 | Sweden | Mobility disability | 110 | 90 | 35.1 (6.4) | Randomised controlled trial |
| Elsworth et al. # [26] Winward et al. # [60] | 2011 2011 | UK | PD, MS, MND, NMD, CP, TBI, TM | 99 | 48 | 56 (13) | Randomised controlled trial |
| Ploughman et al. [44] | 2014 | Canada | Stroke, PD, MS, TBI, NMD | 27 | 10 | 57.7 (13.6) [32–78] | Repeated measures |
| Wallace et al. [37] | 2019 | UK | CMT, IBM | 45 | 14 | CMT 46 [39–52] IBM 62 [56–67] | Randomized crossover trial |
| Duret et al. [42] | 2020 | France | Stroke, PN, TBI, SCI, other | 79 | 33 | 59 (14) | Pre-post-test |
| Authors (Year) | Physical Activity Intervention | Intervention Duration | Supervision | Peer support | Specialist Support | Orientation | Education | Formal Social Activities | Logistical Support | Motivational |
|---|---|---|---|---|---|---|---|---|---|---|
| Pett et al. (2013) [38] | Aerobic and strength training | 12 weeks | X | X | X | |||||
| Stanish & Temple (2012 b) # [57] Temple & Stanish (2011) # [47] | Aerobic and strength training | 15 weeks | X | X | X | |||||
| Stanish & Temple (2012 a) [55] | Aerobic and strength training | 12 weeks | X | X | ||||||
| Zanudin et al. (2021) [48] | Aerobic and strength training | 18 weeks | X | X | X | |||||
| Shields et al. (2019) [53] | Progressive resistance and aerobic training | 12 weeks | X | X | ||||||
| Shields et al. (2021) # [34] McKenzie et al. (2022) # [15] | Progressive resistance and aerobic training | 12 weeks | X | X | X | |||||
| Shields et al. (2020) [32] | Progressive resistance training | 10 weeks | X | |||||||
| Shields et al. (2008) [33] | Progressive resistance training | 10 weeks | X | X | X | |||||
| Shields & Taylor. (2010) + [17] Shields et al. (2013) + [18] | Progressive resistance training | 10 weeks | X X | X X | ||||||
| Taylor et al. (2013) # [36] Bania et al. (2016) # [58] | Progressive resistance training | 12 weeks | X | X | ||||||
| Hoffman et al. (2010) [28] | Aerobic training | 10 weeks | X | X | X | |||||
| Poliakoff et al. (2013) [39] | Aerobic exercise | 20 weeks | X | X | ||||||
| Wallace et al. (2019) [37] | Aerobic training | 12 weeks | X | X | ||||||
| Carter et al. (2004) [54] | Aerobic and strength training | 10 weeks | X | X | X | X | ||||
| Collett et al. (2016) [23] | Aerobic and strength training | 6 months | X | X | ||||||
| Elsworth et al. (2011) # [26] Winward et al. (2011) # [60] | Aerobic and strength training | 12 weeks | X | X | X | X | X | |||
| Hansen et al. (2018) [52] | Aerobic and strength training | 6 weeks (2nd part) | X | X | X | |||||
| Hassett et al. (2009) [14] | Aerobic and strength training | 12 weeks | X | X | X | |||||
| Lampousi et al. (2020) [30] | Aerobic and strength training | 12 weeks | X | X | X | |||||
| Duret et al. (2020) [42] | Aerobic, strength and balance training | 6 months | X | X | ||||||
| Danoudis & Iansek (2021) [41] | Aerobic, progressive resistance and balance training | 12 months | X | X | X | X | ||||
| Handlery et al. (2022) [49] | Aerobic and strength training alternating with other physical activities | Part 1–8 weeks Part 2–19 weeks | X | X | X | X | X | X | X | |
| Kovacic et al. (2020) [29] | Balance training (Group 1) Aerobic and strength training and wellness program (Group 2) | 16 weeks | X | X Gp 1 only | X Gp 1 only | X | X | |||
| Pau et al. (2018) [31] | Aerobic, gait and strength training | 24 weeks | X | X | X | |||||
| Ploughman et al. (2014) [44] | Aerobic, strength and balance exercises | 10 weeks | X | X | X | |||||
| Allen et al. (2004) # [50] Taylor et al. (2004) # [45] | Progressive resistance training | 10 weeks | X | X | X | X | ||||
| Corcos et al. (2013) [24] | Progressive resistance training | 24 months | X | X | ||||||
| Dodd et al. (2006) # [51] Taylor et al. (2006) # [46] | Progressive resistance training | 10 weeks | X | X | X | X | ||||
| Dodd et al. (2011) [25] | Progressive resistance training | 10 weeks | X | X | X | |||||
| Morris et al. (2009) [43] | Progressive resistance training | 8 weeks | X | X | ||||||
| Sims et al. (2009) [35] | Progressive resistance training | 10 weeks | X | X | X | |||||
| Obrusnikova et al. (2019) + [56] | Strength training | 9 sessions | X | X | X | X | ||||
| Obrusnikova et al. (2021 a) + # ^ [59] Obrusnikova et al. (2021 b) # ^ [40] | Strength training | 3 weeks 13 weeks | X | X | X | X | X 2021b only | |||
| Fenton et al. (2021) [27] | RA-tailored exercise | 3 months | X | X | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kennedy, R.A.; McKenzie, G.; Holmes, C.; Shields, N. Social Support Initiatives That Facilitate Exercise Participation in Community Gyms for People with Disability: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 699. https://doi.org/10.3390/ijerph20010699
Kennedy RA, McKenzie G, Holmes C, Shields N. Social Support Initiatives That Facilitate Exercise Participation in Community Gyms for People with Disability: A Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(1):699. https://doi.org/10.3390/ijerph20010699
Chicago/Turabian StyleKennedy, Rachel A., Georgia McKenzie, Carlee Holmes, and Nora Shields. 2023. "Social Support Initiatives That Facilitate Exercise Participation in Community Gyms for People with Disability: A Scoping Review" International Journal of Environmental Research and Public Health 20, no. 1: 699. https://doi.org/10.3390/ijerph20010699