

COVID-19 Vaccination and Late-Onset Myasthenia Gravis: A New Case Report and Review of the Literature


Abstract
:1. Introduction
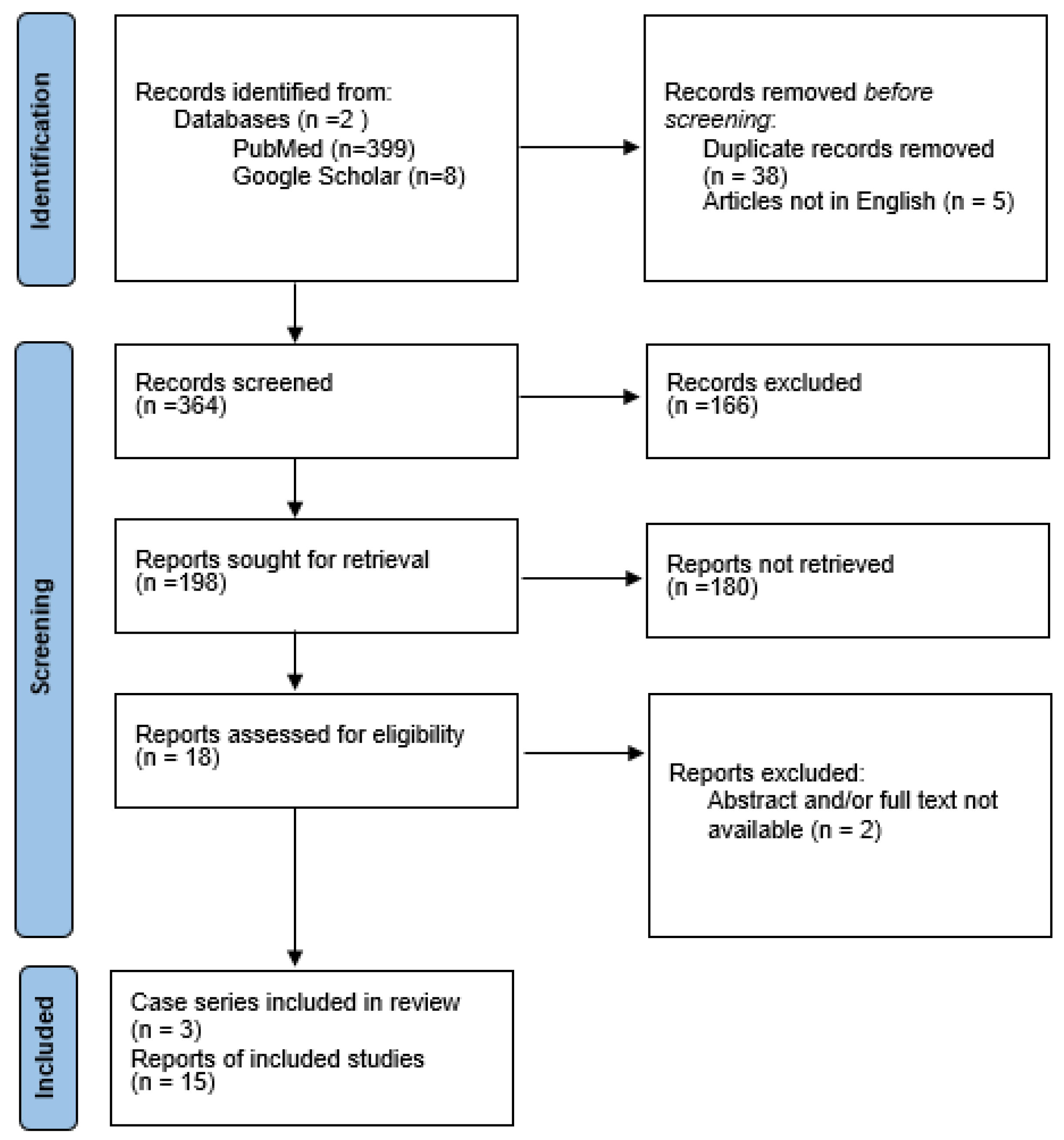
2. Materials and Methods
2.1. Literature Revision
2.2. Statistical Analysis
3. Results
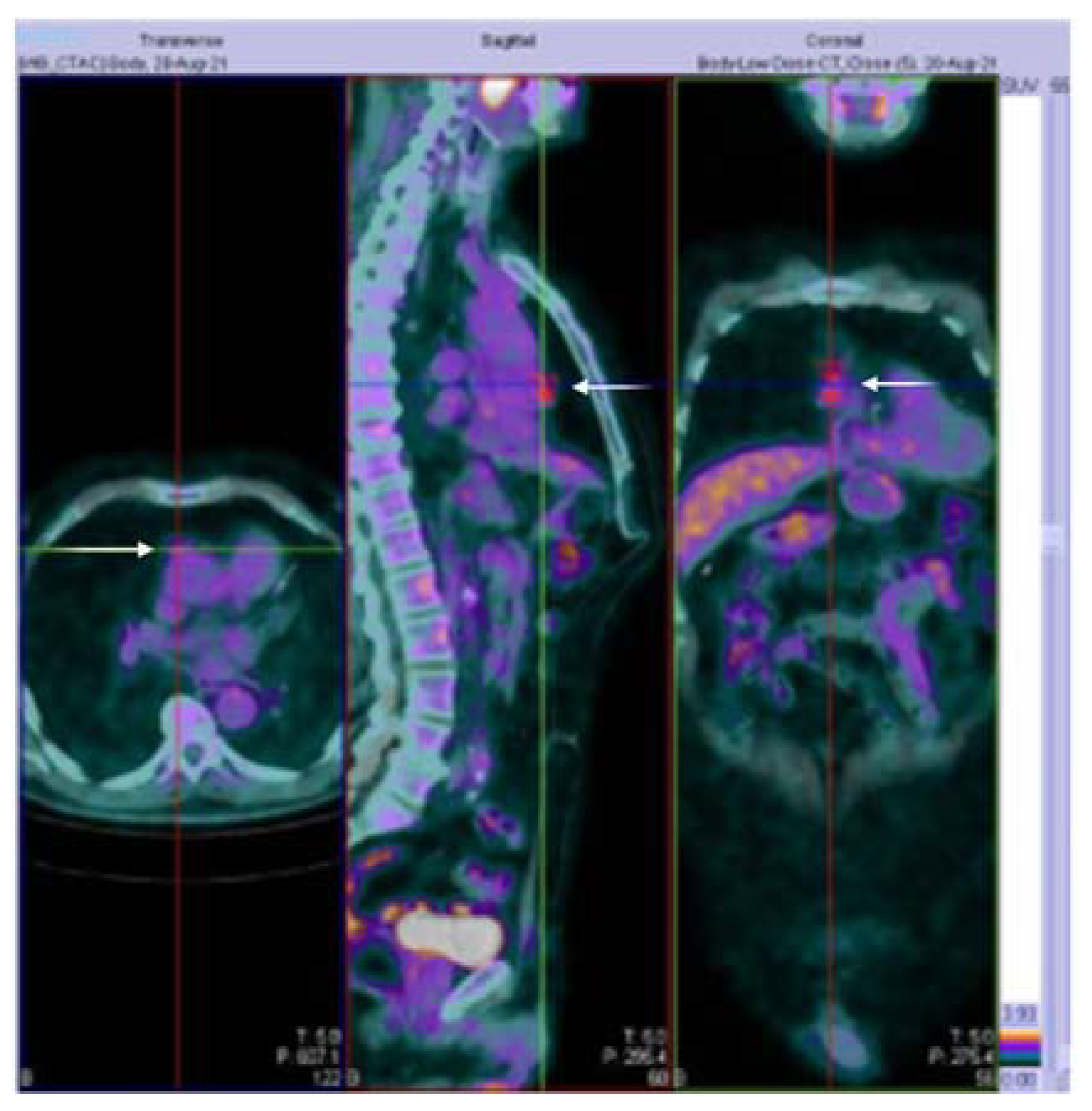
3.1. Case Presentation
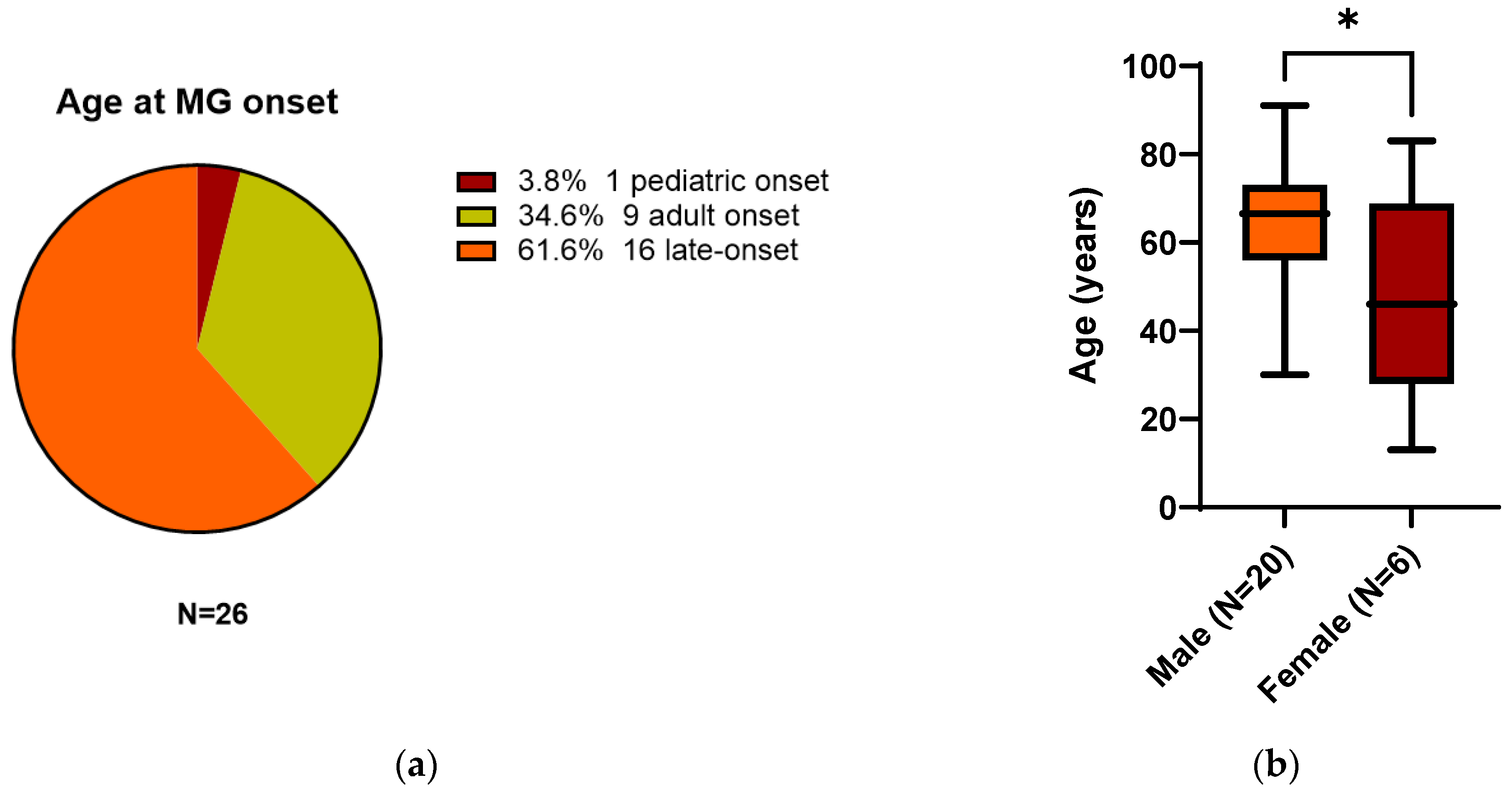
3.2. All 26 Reported Patients
4. Discussion
5. Conclusions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age/Sex | Vaccine Name/Dose | Days Onset | Abs Status | First Symptom | MG Type | Treatment | Follow-Up | Chest-CT | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 65/M | Pfizer-BioNTech/3° | 21 | AchR+ | Diplopia | Ocular | P300 mg/S10 mg | Good recovery at 2MTHs | no | [40] |
| 2 | 82/M | Pfizer-BioNTech/2° | 2 | AchR+ | Slurred speech | Generalized | IV-P/IV-IG/S | Improved | no | [14] |
| 3 | 91/M | Pfizer-BioNTech/2° | 10 | AchR+ | Oculobulbar | Oculobulbar | P90 mg | Unchanged | no | [41] |
| 4 | 80/M | Moderna mRNA1273/2° | 6 | AchR+ | Oculobulbar | Oculobulbar | P90 mg/PLAEX/AZA150 mg | Mild ptosis at 3MTHs | no | [41] |
| 5 | 55/M | Moderna mRNA1273/1° | 3 | AchR+ | ULs-neck-diplopia | Generalized | P240 mg/IV-IG/S50 mg | Mild UL at 3MTHs | no | [41] |
| 6 | 73/M | O.A ChAdOx1/1° | 8 | AchR and RF+ | Monolateral ptosis | Ocular | P240 mg | NR | no | [42] |
| 7 | 30/M | Moderna mRNA1273/1° | 2 | AchR+ | Diplopia | Generalized | P90 mg/S10 mg | NR | no | [26] |
| 8 | 35/M | O.A ChAdOx1/1° | 7 | AchR+ | Diplopia | Ocular | NR | NR | no | [43] |
| 9 | 33/F | Pfizer-BioNTech/2° | 0 | Double-seronegative | GW and diplopia | Generalized | P360 mg | Partial improvement | TH | [44] |
| 10 | 72/M | Pfizer-BioNTech/2° | 1 | NR | NR | NR | S60 mg/PLAEX | Recovered | NR | [45] |
| 11 | 73/M | Pfizer-BioNTech/2° | 7 | NR | Ocular signs | Generalized | PLAEX/P/S | NR | NR | [45] |
| 12 | 65/M | Pfizer-BioNTech/3° | 3 | AchR+ | Diplopia | Ocular | PLAEX/P180 mg | Improvement at 3MTHs | no | [46] |
| 13 | 60/M | Moderna mRNA-1273/3° | 6 | AchR and ANA+ | Dysarthria | Generalized | P/S | Improvement | no | [47] |
| 14 | 13/F | Pfizer-BioNTech/1° | 14 | AchR negative | NR | Generalized | P/S | NR | NR | [38] |
| 15 | 59/M | O.A ChAdOx1/1° | 2 | AchR+ | NR | Generalized | P/S | NR | NR | [38] |
| 16 | 63/M | Pfizer-BioNTech/3° | 3 | AchR+ | NR | Ocular | P | NR | NR | [38] |
| 17 | 73/M | Pfizer-BioNTech/3° | 12 | AchR+ | NR | Generalized | P/IV-IG/S | NR | NR | [38] |
| 18 | 50/M | Pfizer-BioNTech/1° | 7 | AchR+ | NR | Ocular | P | NR | NR | [38] |
| 19 | 83/F | Pfizer-BioNTech/1° | 6 | AchR+ | NR | Generalized | P/IV-IG/S | NR | NR | [38] |
| 20 | 77/M | O.A ChAdOx1/1° | 3 | AchR+ | NR | Generalized | P/PLEX/S | NR | NR | [38] |
| 21 | 53/M | O.A ChAdOx1/1° | 1 | AchR+ | diplopia | Generalized | P360 mg/S15 mg | Improvement at 1MTH | no | [48] |
| 22 | 68/M | Sinopharm/2° | 3 | AchR+ | Dysarthria/dysphagia | Oculobulbar | P180 mg/IVIG/S | Improvement | no | [49] |
| 23 | 46/F | Pfizer-BioNTech/1° | 2 | Triple-seronegative | Monolateral ptosis | Generalized | P/PLAEX/S/M | Stabilization | no | [50] |
| 24 | 46/F | Pfizer-BioNTech/1° | 5 | AchR+ | LL weakness | Generalized | P/PLAEX/S/M | Stabilization | TH | [51] |
| 25 | 64/F | Pfizer-BioNTech/2° | 12 | AchR+ | NR | NR | NR | NR | NR | [30] |
| 26 * | 73/M | O.A ChAdOx1/1° | 28 | AchR+ | Diplopia | Generalized | P360 mg/S12.5 mg/AZA | Improvement | T |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Acter, T.; Uddin, N.; Das, J.; Akhter, A.; Choudhury, T.R.; Kim, S. Evolution of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) as coronavirus disease 2019 (COVID-19) pandemic: A global health emergency. Sci. Total Environ. 2020, 730, 138996. [Google Scholar] [CrossRef] [PubMed]
- Tondo, G.; Virgilio, E.; Naldi, A.; Bianchi, A.; Comi, C. Safety of COVID-19 Vaccines: Spotlight on Neurological Complications. Life 2022, 12, 1338. [Google Scholar] [CrossRef] [PubMed]
- Francis, A.I.; Ghany, S.; Gilkes, T.; Umakanthan, S. Review of COVID-19 vaccine subtypes, efficacy and geographical distributions. Postgrad. Med. J. 2022, 98, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Hasanzad, M.; Namazi, H.; Larijani, B. COVID-19 anti-vaccine attitude and hesitancy. J. Diabetes Metab. Disord. 2022, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Causality Assessment of an Adverse Event Following Immunization (AEFI): User Manual for the Revised WHO Classification. Available online: https://www.who.int/publications-detail-redirect/9789241516990 (accessed on 15 October 2022).
- The Use of the WHO-UMC System for Standardised Case Causality Assessment. Available online: https://www.who.int/publications/m/item/WHO-causality-assessment (accessed on 15 October 2022).
- Estephan, E.D.P.; Baima, J.P.S.; Zambon, A.A. Myasthenia gravis in clinical practice. Arq. Neuro-Psiquiatr. 2022, 80, 257–265. [Google Scholar] [CrossRef]
- Huda, S.; Woodhall, M.R.; Vincent, A.; Heckmann, J.M. Characteristics Of acetylcholine-receptor-antibody-negative myasthenia gravis in a South African cohort. Muscle Nerve 2016, 54, 1023–1029. [Google Scholar] [CrossRef]
- Vincent, A.; Newsom-Davis, J. Acetylcholine receptor antibody as a diagnostic test for myasthenia gravis: Results in 153 validated cases and 2967 diagnostic assays. J. Neurol. Neurosurg. Psychiatry 1985, 48, 1246–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenti, M.V.; Rossi, C.M.; Melazzini, F.; Gastaldi, M.; Bugatti, S.; Rotondi, M.; Bianchi, P.I.; Gentile, A.; Chiovato, L.; Montecucco, C.; et al. Seronegative autoimmune diseases: A challenging diagnosis. Autoimmun. Rev. 2022, 21, 103143. [Google Scholar] [CrossRef]
- Kwon, Y.N.; Woodhall, M.; Sung, J.-J.; Kim, K.-K.; Lim, Y.-M.; Kim, H.; Kim, J.-E.; Baek, S.-H.; Kim, B.-J.; Park, J.-S.; et al. Clinical pitfalls and serological diagnostics of MuSK myasthenia gravis. J. Neurol. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Spagni, G.; Gastaldi, M.; Businaro, P.; Chemkhi, Z.; Carrozza, C.; Mascagna, G.; Falso, S.; Scaranzin, S.; Franciotta, D.; Evoli, A.; et al. Comparison of Fixed and Live Cell-Based Assay for the Detection of AChR and MuSK Antibodies in Myasthenia Gravis. Neurol. Neuroimmunol. Neuroinflammation 2023, 10, e200038. [Google Scholar] [CrossRef]
- Damato, V.; Spagni, G.; Monte, G.; Woodhall, M.; Jacobson, L.; Falso, S.; Smith, T.; Iorio, R.; Waters, P.; Irani, S.R.; et al. Clinical value of cell-based assays in the characterisation of seronegative myasthenia gravis. J. Neurol. Neurosurg. Psychiatry 2022, 93, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Chavez, A.; Pougnier, C. A Case of COVID-19 Vaccine Associated New Diagnosis Myasthenia Gravis. J. Prim. Care Community Health 2021, 12, 21501327211051933. [Google Scholar] [CrossRef] [PubMed]
- Gilhus, N.E. Myasthenia Gravis. N. Engl. J. Med. 2016, 375, 2570–2581. [Google Scholar] [CrossRef]
- Gilhus, N.E.; Verschuuren, J.J. Myasthenia gravis: Subgroup classification and therapeutic strategies. Lancet Neurol. 2015, 14, 1023–1036. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M. Dysphonia as first symptom of late-onset myasthenia gravis. J. Gen. Intern. Med. 2006, 21, C4–C6. [Google Scholar] [CrossRef] [PubMed]
- Sih, M.; Soliven, B.; Mathenia, N.; Jacobsen, J.; Rezania, K. Head-drop: A frequent feature of late-onset myasthenia gravis. Muscle Nerve 2017, 56, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Toba, H.; Kondo, K.; Sadohara, Y.; Otsuka, H.; Morimoto, M.; Kajiura, K.; Nakagawa, Y.; Yoshida, M.; Kawakami, Y.; Takizawa, H.; et al. 18F-fluorodeoxyglucose positron emission tomography/computed tomography and the relationship between fluorodeoxyglucose uptake and the expression of hypoxia-inducible factor-1α, glucose transporter-1 and vascular endothelial growth factor in thymic epithelial tumours. Eur. J. Cardiothorac. Surg. 2013, 44, e105–e112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomiyama, N.; Johkoh, T.; Mihara, N.; Honda, O.; Kozuka, T.; Koyama, M.; Hamada, S.; Okumura, M.; Ohta, M.; Eimoto, T.; et al. Using the World Health Organization Classification of thymic epithelial neoplasms to describe CT findings. AJR Am. J. Roentgenol. 2002, 179, 881–886. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.S.; Cardwell, C.R.; McCarron, P.O.; McConville, J. A systematic review of population based epidemiological studies in Myasthenia Gravis. BMC Neurol. 2010, 10, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, L.H. The epidemiology of myasthenia gravis. Semin. Neurol. 2004, 24, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Bedlack, R.S.; Sanders, D.B. On the concept of myasthenic crisis. J. Clin. Neuromuscul. Dis. 2002, 4, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Tugasworo, D.; Kurnianto, A.; Retnaningsih; Andhitara, Y.; Ardhini, R.; Budiman, J. The relationship between myasthenia gravis and COVID-19: A systematic review. Egypt. J. Neurol. Psychiatry Neurosurg. 2022, 58, 1–13. [Google Scholar] [CrossRef]
- Chung, J.Y.; Lee, S.J.; Shin, B.S.; Kang, H.G. Myasthenia gravis following human papillomavirus vaccination: A case report. BMC Neurol. 2018, 18, 222. [Google Scholar] [CrossRef] [Green Version]
- Hoshina, Y.; Sowers, C.; Baker, V. Myasthenia Gravis Presenting after Administration of the mRNA-1273 Vaccine. Eur. J. Case Rep. Intern. Med. 2022, 9, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Rabaan, A.A.; Mutair, A.A.; Hajissa, K.; Alfaraj, A.H.; Al-Jishi, J.M.; Alhajri, M.; Alwarthan, S.; Alsuliman, S.A.; Al-Najjar, A.H.; Al Zaydani, I.A.; et al. A Comprehensive Review on the Current Vaccines and Their Efficacies to Combat SARS-CoV-2 Variants. Vaccines 2022, 10, 1655. [Google Scholar] [CrossRef] [PubMed]
- Ishizuchi, K.; Takizawa, T.; Sekiguchi, K.; Motegi, H.; Oyama, M.; Nakahara, J.; Suzuki, S. Flare of myasthenia gravis induced by COVID-19 vaccines. J. Neurol. Sci. 2022, 436, 120225. [Google Scholar] [CrossRef]
- Li, H.Y.; Shao, L.Y.; Song, M.; Hu, S.M.; Yue, Y.X.; Li, H.F. Safety of inactivated SARS-CoV-2 vaccines in myasthenia gravis: A survey-based study. Front. Immunol. 2022, 13, 923017. [Google Scholar] [CrossRef] [PubMed]
- Sansone, G.; Bonifati, D.M. Vaccines and myasthenia gravis: A comprehensive review and retrospective study of SARS-CoV-2 vaccination in a large cohort of myasthenic patients. J. Neurol. 2022, 269, 3965–3981. [Google Scholar] [CrossRef] [PubMed]
- Doron, A.; Piura, Y.; Vigiser, I.; Kolb, H.; Regev, K.; Nesher, N.; Karni, A. BNT162b2 mRNA COVID-19 vaccine three-dose safety and risk of COVID-19 in patients with myasthenia gravis during the alpha, delta, and omicron waves. J. Neurol. 2022, 269, 6193–6201. [Google Scholar] [CrossRef]
- Lee, J.R.; Jaffry, M.; Mandava, K.; Rosario, S.; Jaffry, K.; Jedidi, K.; Souayah, N. Is COVID-19 Vaccination Associated with an Increased Reporting Rate of Myasthenia Gravis? A Vaccine Adverse Event Reporting System (VAERS) Study (P11-13.002). Neurology 2022, 98, 1795. [Google Scholar]
- Lupica, A.; Di Stefano, V.; Iacono, S.; Pignolo, A.; Quartana, M.; Gagliardo, A.; Fierro, B.; Brighina, F. Impact of COVID-19 in AChR Myasthenia Gravis and the Safety of Vaccines: Data from an Italian Cohort. Neurol. Int. 2022, 14, 406–416. [Google Scholar] [CrossRef]
- Tagliaferri, A.R.; Narvaneni, S.; Azzam, M.H.; Grist, W. A Case of COVID-19 Vaccine Causing a Myasthenia Gravis Crisis. Cureus 2021, 13, e15581. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Handunnetthi, L.; Saatci, D.; Pan, J.; Katikireddi, S.V.; Razvi, S.; Hunt, D.; Mei, X.W.; Dixon, S.; Zaccardi, F.; et al. Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. Nat. Med. 2021, 27, 2144–2153. [Google Scholar] [CrossRef]
- Wraith, D.C.; Goldman, M.; Lambert, P.H. Vaccination and autoimmune disease: What is the evidence? Lancet 2003, 362, 1659–1666. [Google Scholar] [CrossRef]
- Caron, P. Autoimmune and inflammatory thyroid diseases following vaccination with SARS-CoV-2 vaccines: From etiopathogenesis to clinical management. Endocrine 2022, 78, 406–417. [Google Scholar] [CrossRef]
- Ramdas, S.; Hum, R.M.; Price, A.; Paul, A.; Bland, J.; Burke, G.; Farrugia, M.; Palace, J.; Storrie, A.; Ho, P.; et al. SARS-CoV-2 vaccination and new-onset myasthenia gravis: A report of 7 cases and review of the literature. Neuromuscul. Disord. 2022, 32, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Mirmosayyeb, O.; Moases Ghaffary, E.; Mazdak, M.; Bagheri, Z.; Bagherieh, S.; Shaygannejad, V. Is Myasthenia Gravis a Real Complication of the COVID-19 Vaccine? A Case Report-Based Systematic Review. Can. J. Infect. Dis. Med. Microbiol. 2022, 2022, 1–7. [Google Scholar] [CrossRef]
- Abicic, A.; Sitas, B.; Adamec, I.; Bilic, E.; Habek, M. New-Onset Ocular Myasthenia Gravis After Booster Dose of COVID-19 Vaccine. Cureus 2022, 14, e27213. [Google Scholar] [CrossRef] [PubMed]
- Fanella, G.; Baiata, C.; Candeloro, E.; Toscano, G.; Colnaghi, S.; Mauri, M.; Cariddi, L.P.; Rebecchi, V.; Solazzo, F.; Banfi, P.; et al. New-onset myasthenia gravis after mRNA SARS-CoV-2 vaccination: A case series. Neurol. Sci. 2022, 43, 5799–5802. [Google Scholar] [CrossRef] [PubMed]
- Galassi, G.; Rispoli, V.; Iori, E.; Ariatti, A.; Marchioni, A. Coincidental Onset of Ocular Myasthenia Gravis Following ChAdOx1 n-CoV-19 Vaccine against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Isr. Med. Assoc. J. 2022, 24, 9–10. [Google Scholar] [PubMed]
- Kang, M.C.; Park, K.A.; Min, J.H.; Oh, S.Y. Myasthenia gravis with ocular symptoms following a ChAdOx1 nCoV-19 vaccination: A case report. Am. J. Ophthalmol. Case Rep. 2022, 27, 101620. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.A.; Lee, C.; Park, J.H.; Lee, J.H. Early-Onset Myasthenia Gravis Following COVID-19 Vaccination. J. Korean Med. Sci. 2022, 37, e50. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination. Vaccines 2021, 9, 435. [Google Scholar] [CrossRef] [PubMed]
- Poli, K.; Poli, S.; Ziemann, U. Multiple Autoimmune Syndromes Including Acute Disseminated Encephalomyelitis, Myasthenia Gravis, and Thyroiditis Following Messenger Ribonucleic Acid-Based COVID-19 Vaccination: A Case Report. Front. Neurol. 2022, 13, 913515. [Google Scholar] [CrossRef]
- Slavin, E.; Fitzig, J.; Neubert, C.; Garcia-Lopez, F.; Cuevas-Trisan, R. New-onset myasthenia gravis confirmed by electrodiagnostic studies after a third dose of SARS-CoV-2 mRNA-1273 vaccine: A case report. Am. J. Phys. Med. Rehabil. 2022, 101, e176–e179. [Google Scholar] [CrossRef]
- Huang, B.-D.; Hsueh, H.-W.; Yang, S.-H.; Lin, C.-W. New-Onset Myasthenia Gravis After ChAdOx1 nCOV-19 Vaccine Inoculation. J. Neuro-Ophthalmol. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Abna, Z.; Khanmoradi, Z.; Abna, Z. A new case of myasthenia gravis following COVID-19 Vaccination. Neuroimmunol. Rep. 2022, 2, 100128. [Google Scholar] [CrossRef]
- Most, D.; Tiem, M.; Ferrey, D.; Dunn-Pirio, A. Myasthenia Gravis Syndrome Following COVID-19 Vaccination and Subsequent Tolerance of Booster Vaccine: A Case Report (P4-1.005). Neurology 2022, 98, 3817. [Google Scholar]
- Bui, A.; Shrivastava, S. Progressive Ascending Weakness after the Pfizer/Biontech COVID-19 Vaccine. Chest 2022, 162, A69. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virgilio, E.; Tondo, G.; Montabone, C.; Comi, C. COVID-19 Vaccination and Late-Onset Myasthenia Gravis: A New Case Report and Review of the Literature. Int. J. Environ. Res. Public Health 2023, 20, 467. https://doi.org/10.3390/ijerph20010467
Virgilio E, Tondo G, Montabone C, Comi C. COVID-19 Vaccination and Late-Onset Myasthenia Gravis: A New Case Report and Review of the Literature. International Journal of Environmental Research and Public Health. 2023; 20(1):467. https://doi.org/10.3390/ijerph20010467
Chicago/Turabian StyleVirgilio, Eleonora, Giacomo Tondo, Claudia Montabone, and Cristoforo Comi. 2023. "COVID-19 Vaccination and Late-Onset Myasthenia Gravis: A New Case Report and Review of the Literature" International Journal of Environmental Research and Public Health 20, no. 1: 467. https://doi.org/10.3390/ijerph20010467