
The Effectiveness of E-Health Interventions Promoting Physical Activity and Reducing Sedentary Behavior in College Students: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.2.1. Participants
2.2.2. Interventions
2.2.3. Comparators
2.2.4. Outcomes
2.2.5. Study Design
2.3. Data Extraction
2.4. Risk of Bias (ROB) and Quality Assessment
2.5. Statistical Analyses
3. Results
3.1. Literature Search
3.2. Studies’ Characteristics
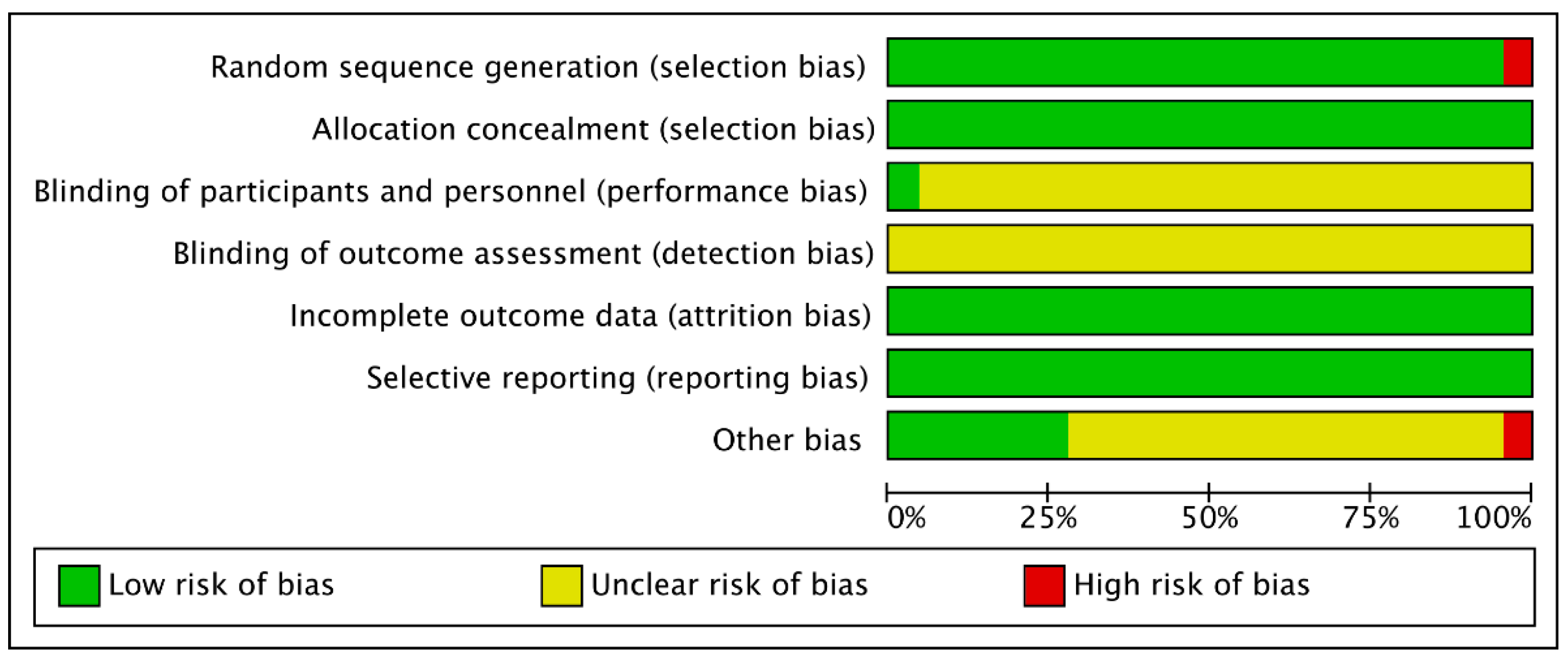
3.3. Quality of Included Studies
3.4. Primary Outcomes
3.5. Subgroup Analysis of PA
3.6. Robustness of the Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

| Study | Participant Characteristic | Study Design | Intervention Mode | Theory | Duration (Follow-Up) | Instrument | Outcome |
|---|---|---|---|---|---|---|---|
| Pope (2020) [48] | n = 44 (IG = 22, CG = 22) Age: 21.6 Female ratio = 72.72% Inactive; USA | Pilot RCT; ITT | MapMyFitness (Apps) to their smartphones | SCT | 10 weeks | ACTi graph GT3X þ accelerometers | 1. MVPA/day(min) 2. SB/day(min) |
| Dillon (2021) [58] | n = 51 (IG = 28, CG = 33) Age: 21.13 (4.81) Female ratio = 80.30% General; Canada | RCT; ITT | Text messages; booklet; counsel session | HAPA | 8 weeks | Validated three-item modified OSPAQ | 1. sitting time (min/workday) 2. Walking time (min/workday) |
| Al-Nawaiseh (2022) [36] | n = 114 (IG = 56, CG = 58) Age: 21.12 (2) Female ratio = 80.70% General; USA | RCT; PP | Smartphone apps for improving the PA (Step counts) (Pacer Pedometer App) | 12 weeks | Pacer Pedometer App | Physical Activity (PA) (Step Counts/Week) | |
| Caso (2020) [60] | n = 80 (IG = 39, CG = 41) Age: 19.74 (1.36) Female ratio = 80.80% General; Italy | RCT; PP | Health Message + self-monitoring Smartphone Apps (HMS) | HAPA | 2 months | A single item obtained from the IPAQ | Number of days spent walking at least 10 min over the last week |
| Alshahrani (2021) [61] | n = 103 (IG = 53, CG = 50) Age: 18–28 Female ratio = 100% General; Saudi Arabia | RCT; PP | Message from WhatsApp (social media) | 10 weeks | GPAQ | MET per week | |
| Pope (2019) [49] | n = 38 (IG = 19, CG = 19) Age: 21.5 (3.4) Female ratio = 26.31% Inactive; USA | Pilot RCT; ITT | Facebook (social media) + Polar M400 | SCT/ SDT | 12 weeks | ACTi Graph Link accelerometers + Polar M400 | 1. MVPA/day(min) 2. LPA/day(min) 3. SB/day(min) |
| Mo (2019) [50] | n = 52 (IG = 17, CG = 35) Age: 20.76 (1.97) Female ratio = 51.92% General; China | RCT; PP | WeChat (social media) | TPB | 7 weeks | IPAQ-S | 1. TPA (min/day) 2. VPA 3. MPA 4. Walking time (min/workday) 5. SB/(min/Sitting time) |
| Maselli (2019) [54] | n = 22 (IG = 11, CG = 11) Age: 22 (2) Female ratio = 60.60% Inactive; Italy | RCT | Accelerometer | SCT/ TTM | 12 weeks (3 months) | IPAQ-S and recorded by ActiGraph-GT3X | 1. min MET/week 2. ACTi graph—MVPA (min/week) |
| Miragall (2017) [51] | n = 48 (IG = 22, CG = 26) Age: 22.18 (3.71) Female ratio = 85.50% Inactive; Spain | RCT; PP | Internet + pedometer | TTM | 3 weeks (3 months) | Pedometers (Fitbit One) | Daily steps |
| Memon (2018) [52] | n = 56 (IG = 28, CG = 28) Age: 20.63 (1.67) Female ratio = 100% Inactive; Pakistan | Pilot RCT; PP | Moves application (from Protogenoi Inc) + financial incentives | 5 weeks | Moves application | Total steps during the intervention | |
| Mbada (2018) [53] | n = 50 (IG = 25, CG = 25) Age: 21.95 (1.28) Female ratio = 100% Inactive; Nigeria | RCT; PP | Short message through mobile phone | 4 weeks (8 weeks) | Pedometer (model JS-206B) | Pedometer reading (steps) | |
| Shin (2017) [46] | n = 64 (IG = 32, CG = 32) Age: 27.8 Female ratio = 0 Inactive; South Korea | Pilot RCT; PP | The smartphone apps for A Fitmeter accelerometer | 12 weeks | IPAQ-S | PA(IPAQ)(kcal/week) | |
| Sharp (2016) [63] | n = 194 (IG = 95, CG = 99) Age: 18 (0.69) Female ratio = 50.51% General; Canada | RCT; ITT | Pedometer | 12 weeks | The modified version of GLTEQ | 1. LPA/week(min) 2. MPA/week(min) 3. VPA/week(min) | |
| Rote (2015) [47] | n = 53 (IG = 27, CG = 26) Age: 18.06 (0.7) Female ratio = 100% Inactive; USA | RCT; PP | Facebook (social media) | 8 weeks | Pedometer | steps/day | |
| Sriramatr (2014) [62] | n = 110 (IG = 55, CG = 55) Age: 19 Female ratio = 100% General; Thailand | RCT; ITT | Website | 3 months (3 months) | Pedometer | steps/day | |
| Kattelmann (2014) [57] | n = 973 (IG = 497, CG = 476) Age: 19.3 (1.1) Female ratio = 67.20% General; USA | RCT; PP | Website and email | 3 months (15 months) | IPAQ | MET/week(min) | |
| Epton (2014) [37] | n = 1039 (IG = 513, CG = 526) Age: 18.9 Female ratio = 58.74% General; England | RCT; PP | Website and email | SAT/ TPB/ II | 1 month (6 months) | IPAQ-S | 1. METS 2. Mean hours sitting |
| Lee (2012) [56] | n = 94 (IG = 46, CG = 48) Age: 16–20 Female ratio = 100% Inactive; Chinese Taiwan | RCT; PP | Pedometer | SET | 12 weeks | Electronic pedometer | Aerobic walking (steps/day) |
| Cavallo (2012) [59] | n = 134 (IG = 67, CG = 67) Age: < 25 Female ratio = 100% Inactive; USA | RCT; ITT | Facebook (social media) + website | 12 weeks | A version of the Paffenbarger activity questionnaire | 1. PA (total kcal) 2. PA (heavy kcal) 3. PA (moderate kcal) 4. PA (light kcal) | |
| Wadsworth (2010) [44] | n = 71 (IG = 34, CG = 37) Age: 18–24 Female ratio = 100% Inactive; USA | RCT; PP | Website | SCT | 6 weeks (6 months) | IPAQ-S | Frequency of MPA (times/week) |
| Mailey (2010) [55] | n = 47 (IG = 23, CG = 24) Age: 25 Female ratio = 68.10% General; USA | RCT; PP | Pedometer +sessions + Internet | SCT | 10 weeks | ACTi Graph accelerometers | PA |
| Spence (2009) [45] | n = 31 (IG = 16, CG = 15) Age: <30 Female ratio = 100% General; Canada | RCT; PP | Pedometer | TPB | one week | IPAQ-S | Walking (IPAQ) |
References
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020; Volume 3. [Google Scholar]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.; Fagerland, M.; Owen, N.; Powell, K.; Bauman, A.; Lee, I. Physical activity attenuates the detrimental association of sitting time with mortality: A harmonised meta-analysis of data from more than one million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneko, K.; Saito, Y.; Nohara, Y.; Kudo, E.; Yamada, M. Does physical activity enhance learning performance?: Learning effectiveness of game-based experiential learning for university library instruction. J. Acad. Librariansh. 2018, 44, 569–581. [Google Scholar] [CrossRef]
- Tao, K.; Liu, W.; Xiong, S.; Ken, L.; Zeng, N.; Peng, Q.; Yan, X.; Wang, J.; Wu, Y.; Lei, M.; et al. Associations between Self-Determined Motivation, Accelerometer-Determined Physical Activity, and Quality of Life in Chinese College Students. Int. J. Environ. Res. Public Health 2019, 16, 2941. [Google Scholar] [CrossRef] [Green Version]
- Keating, X.D.; Guan, J.; Pinero, J.C.; Bridges, D.M. A meta-analysis of college students’ physical activity behaviors. J. Am. Coll. Health 2005, 54, 116–125. [Google Scholar] [CrossRef]
- Martinez-Bello, V.E.; Martinez-Rojas, A.; Molina-Garcia, J. Health-related messages about physical activity promotion: An analysis of photographs on social networking sites of universities. J. High. Educ. Policy Manag. 2017, 39, 75–88. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K.; Kassean, H.K.; Tsala Tsala, J.P.; Sychareun, V.; Muller-Riemenschneider, F. Physical inactivity and associated factors among university students in 23 low-, middle- and high-income countries. Int. J. Public Health 2015, 60, 539–549. [Google Scholar] [CrossRef]
- Chen, P.; Wang, D.; Shen, H.; Yu, L.; Gao, Q.; Mao, L.; Jiang, F.; Luo, Y.; Xie, M.; Zhang, Y.; et al. Physical activity and health in Chinese children and adolescents: Expert consensus statement (2020). Br. J. Sports Med. 2020, 54, 1321–1331. [Google Scholar] [CrossRef]
- Favieri, F.; French, M.N.; Casagrande, M.; Chen, E.Y. Physical activity interventions have a moderate effect in increasing physical activity in university students—A meta-analysis. J. Am. Coll. Health 2022, 1–12. [Google Scholar] [CrossRef]
- Wengreen, H.J.; Moncur, C. Change in diet, physical activity, and body weight among young-adults during the transition from high school to college. Nutr. J. 2009, 8, 32. [Google Scholar] [CrossRef]
- Karabulut, U.S.; Romero, Z.; Conatser, P.; Karabulut, M. Assessing overweight/obesity, dietary habits, and physical activity in Hispanic college students. Exerc. Med. 2018, 2. [Google Scholar] [CrossRef] [Green Version]
- Silva, R.M.F.; Mendonca, C.R.; Noll, M. Barriers to high school and university students’ physical activity: A systematic review protocol. Int. J. Educ. Res. 2021, 106, 101743. [Google Scholar] [CrossRef]
- Schoeppe, S.; Alley, S.; Rebar, A.L.; Hayman, M.; Bray, N.A.; Van Lippevelde, W.; Gnam, J.P.; Bachert, P.; Direito, A.; Vandelanotte, C. Apps to improve diet, physical activity and sedentary behaviour in children and adolescents: A review of quality, features and behaviour change techniques. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 83. [Google Scholar] [CrossRef] [PubMed]
- Schroe, H.; Van Dyck, D.; De Paepe, A.; Poppe, L.; Loh, W.W.; Verloigne, M.; Loeys, T.; De Bourdeaudhuij, I.; Crombez, G. Which behaviour change techniques are effective to promote physical activity and reduce sedentary behaviour in adults: A factorial randomized trial of an e- and m-health intervention. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 127. [Google Scholar] [CrossRef]
- Whatnall, M.C.; Sharkey, T.; Hutchesson, M.J.; Haslam, R.L.; Bezzina, A.; Collins, C.E.; Ashton, L.M. Effectiveness of interventions and behaviour change techniques for improving physical activity in young adults: A systematic review and meta-analysis. J. Sports Sci. 2021, 39, 1754–1771. [Google Scholar] [CrossRef]
- Direito, A.; Carraca, E.; Rawstorn, J.; Whittaker, R.; Maddison, R. mHealth Technologies to Influence Physical Activity and Sedentary Behaviors: Behavior Change Techniques, Systematic Review and Meta-Analysis of Randomized Controlled Trials. Ann. Behav. Med. 2017, 51, 226–239. [Google Scholar] [CrossRef] [Green Version]
- Osipov, A.Y.; Ratmanskaya, T.I.; Zemba, E.A.; Potop, V.; Kudryavtsev, M.D.; Nagovitsyn, R.S. The impact of the universities closure on physical activity and academic performance in physical education in university students during the COVID-19 pandemic. Phys. Educ. Stud. 2021, 25, 20–27. [Google Scholar] [CrossRef]
- Bland, K.A.; Bigaran, A.; Campbell, K.L.; Trevaskis, M.; Zopf, E.M. Exercising in Isolation? The Role of Telehealth in Exercise Oncology During the COVID-19 Pandemic and Beyond. Phys. Ther. 2020, 100, 1713–1716. [Google Scholar] [CrossRef]
- Wang, Q.; Su, M.; Zhang, M.; Li, R. Integrating Digital Technologies and Public Health to Fight Covid-19 Pandemic: Key Technologies, Applications, Challenges and Outlook of Digital Healthcare. Int. J. Environ. Res. Public Health 2021, 18, 6053. [Google Scholar] [CrossRef]
- Eysenbach, G. What is e-health? J. Med. Internet Res. 2001, 3, e833. [Google Scholar] [CrossRef]
- Hayman, M.; Alfrey, K.L.; Cannon, S.; Alley, S.; Rebar, A.L.; Williams, S.; Short, C.E.; Altazan, A.; Comardelle, N.; Currie, S.; et al. Quality, Features, and Presence of Behavior Change Techniques in Mobile Apps Designed to Improve Physical Activity in Pregnant Women: Systematic Search and Content Analysis. JMIR mHealth uHealth 2021, 9, e23649. [Google Scholar] [CrossRef] [PubMed]
- Kip, H.; Kelders, S.M.; Sanderman, R.; van Gemert-Pijnen, L. eHealth Research, Theory and Development: A Multi-Disciplinary Approach; Routledge: London, UK, 2018. [Google Scholar]
- Duff, O.M.; Walsh, D.M.; Furlong, B.A.; O’Connor, N.E.; Moran, K.A.; Woods, C.B. Behavior Change Techniques in Physical Activity eHealth Interventions for People With Cardiovascular Disease: Systematic Review. J. Med. Internet Res. 2017, 19, e281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oosterveen, E.; Tzelepis, F.; Ashton, L.; Hutchesson, M.J. A systematic review of eHealth behavioral interventions targeting smoking, nutrition, alcohol, physical activity and/or obesity for young adults. Prev. Med. 2017, 99, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Khokhar, B.; Jones, J.; Ronksley, P.E.; Armstrong, M.J.; Caird, J.; Rabi, D. Effectiveness of mobile electronic devices in weight loss among overweight and obese populations: A systematic review and meta-analysis. BMC Obes. 2014, 1, 22. [Google Scholar] [CrossRef] [Green Version]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: A systematic review. PLoS Med. 2013, 10, e1001362. [Google Scholar] [CrossRef] [Green Version]
- Cotie, L.M.; Prince, S.A.; Elliott, C.G.; Ziss, M.C.; McDonnell, L.A.; Mullen, K.A.; Hiremath, S.; Pipe, A.L.; Reid, R.D.; Reed, J.L. The effectiveness of eHealth interventions on physical activity and measures of obesity among working-age women: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 1340–1358. [Google Scholar] [CrossRef]
- Laplante, C.; Peng, W. A systematic review of e-health interventions for physical activity: An analysis of study design, intervention characteristics, and outcomes. Telemed. J. eHealth 2011, 17, 509–523. [Google Scholar] [CrossRef]
- Baumann, H.; Fiedler, J.; Wunsch, K.; Woll, A.; Wollesen, B. mHealth Interventions to Reduce Physical Inactivity and Sedentary Behavior in Children and Adolescents: Systematic Review and Meta-analysis of Randomized Controlled Trials. JMIR mHealth uHealth 2022, 10, e35920. [Google Scholar] [CrossRef]
- Champion, K.E.; Parmenter, B.; McGowan, C.; Spring, B.; Wafford, Q.E.; Gardner, L.A.; Thornton, L.; McBride, N.; Barrett, E.L.; Teesson, M.; et al. Effectiveness of school-based eHealth interventions to prevent multiple lifestyle risk behaviours among adolescents: A systematic review and meta-analysis. Lancet Digit. Health 2019, 1, e206–e221. [Google Scholar] [CrossRef] [Green Version]
- Duan, Y.; Shang, B.; Liang, W.; Du, G.; Yang, M.; Rhodes, R.E. Effects of eHealth-Based Multiple Health Behavior Change Interventions on Physical Activity, Healthy Diet, and Weight in People With Noncommunicable Diseases: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e23786. [Google Scholar] [CrossRef]
- Kwan, R.Y.C.; Salihu, D.; Lee, P.H.; Tse, M.; Cheung, D.S.K.; Roopsawang, I.; Choi, K.S. The effect of e-health interventions promoting physical activity in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, W.; Li, M.; Sheng, H.; Zhai, Y. Efficacy of Mobile Health Applications to Improve Physical Activity and Sedentary Behavior: A Systematic Review and Meta-Analysis for Physically Inactive Individuals. Int. J. Environ. Res. Public Health 2022, 19, 4905. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, J.R.D.; Jay, S.; Hadden, N.; Whittaker, P.J. Do E-health interventions improve physical activity in young people: A systematic review. Public Health 2017, 148, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Al-Nawaiseh, H.K.; McIntosh, W.A.; McKyer, L.J. An-m-Health Intervention Using Smartphone App to Improve Physical Activity in College Students: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 7228. [Google Scholar] [CrossRef]
- Epton, T.; Norman, P.; Dadzie, A.S.; Harris, P.R.; Webb, T.L.; Sheeran, P.; Julious, S.A.; Ciravegna, F.; Brennan, A.; Meier, P.S.; et al. A theory-based online health behaviour intervention for new university students (U@Uni): Results from a randomised controlled trial. BMC Public Health 2014, 14, 563. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.; Rainie, L.; Zickuhr, K. College Students and Technology. 2011. Available online: https://policycommons.net/artifacts/624103/college-students-and-technology/1605386/ (accessed on 19 July 2011).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1. 0. Chapter 8: Assessing Risk of Bias in Included Studies; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Juni, P.; Bartlett, C.; Holenstein, F.; Sterne, J. How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study. Health Technol. Assess. 2003, 7, 1–76. [Google Scholar] [CrossRef]
- Wadsworth, D.D.; Hallam, J.S. Effect of a web site intervention on physical activity of college females. Am. J. Health Behav. 2010, 34, 60–69. [Google Scholar] [CrossRef]
- Spence, J.C.; Burgess, J.; Rodgers, W.; Murray, T. Effect of pretesting on intentions and behaviour: A pedometer and walking intervention. Psychol. Health 2009, 24, 777–789. [Google Scholar] [CrossRef]
- Shin, D.W.; Yun, J.M.; Shin, J.H.; Kwon, H.; Min, H.Y.; Joh, H.K.; Chung, W.J.; Park, J.H.; Jung, K.T.; Cho, B. Enhancing physical activity and reducing obesity through smartcare and financial incentives: A pilot randomized trial. Obesity 2017, 25, 302–310. [Google Scholar] [CrossRef] [Green Version]
- Rote, A.E.; Klos, L.A.; Brondino, M.J.; Harley, A.E.; Swartz, A.M. The Efficacy of a Walking Intervention Using Social Media to Increase Physical Activity: A Randomized Trial. J. Phys. Act. Health 2015, 12 (Suppl. S1), S18–S25. [Google Scholar] [CrossRef] [Green Version]
- Pope, Z.C.; Gao, Z. Feasibility of smartphone application- and social media-based intervention on college students’ health outcomes: A pilot randomized trial. J. Am. Coll. Health 2022, 70, 89–98. [Google Scholar] [CrossRef]
- Pope, Z.C.; Barr-Anderson, D.J.; Lewis, B.A.; Pereira, M.A.; Gao, Z. Use of Wearable Technology and Social Media to Improve Physical Activity and Dietary Behaviors among College Students: A 12-Week Randomized Pilot Study. Int. J. Environ. Res. Public Health 2019, 16, 3579. [Google Scholar] [CrossRef] [Green Version]
- Mo, D.; Xiang, M.; Luo, M.; Dong, Y.; Fang, Y.; Zhang, S.; Zhang, Z.; Liang, H. Using Gamification and Social Incentives to Increase Physical Activity and Related Social Cognition among Undergraduate Students in Shanghai, China. Int. J. Environ. Res. Public Health 2019, 16, 858. [Google Scholar] [CrossRef] [Green Version]
- Miragall, M.; Dominguez-Rodriguez, A.; Navarro, J.; Cebolla, A.; Banos, R.M. Increasing physical activity through an Internet-based motivational intervention supported by pedometers in a sample of sedentary students: A randomised controlled trial. Psychol. Health 2018, 33, 465–482. [Google Scholar] [CrossRef]
- Memon, A.R.; Masood, T.; Awan, W.A.; Waqas, A. The effectiveness of an incentivized physical activity programme (Active Student) among female medical students in Pakistan: A Randomized Controlled Trial. J. Pak. Med. Assoc. 2018, 68, 1438–1445. [Google Scholar]
- Mbada, C.E.; Akinola, O.; Olumomi, G.O.; Idowu, O.A.; Akinwande, O.A.; Fatoye, C.T.; Borode, A.; Awotidebe, T.O.; Awotipe, A.A.; Adamolekun, O.E.; et al. Effect of structured short message service-based educational programme on physical activity and body weight status among Nigerian female undergraduates. Niger. J. Health Sci. 2018, 18, 37–42. [Google Scholar] [CrossRef]
- Maselli, M.; Gobbi, E.; Carraro, A. Effectiveness of individual counseling and activity monitors to promote physical activity among university students. J. Sports Med. Phys. Fit. 2019, 59, 132–140. [Google Scholar] [CrossRef]
- Mailey, E.L.; Wojcicki, T.R.; Motl, R.W.; Hu, L.; Strauser, D.R.; Collins, K.D.; McAuley, E. Internet-delivered physical activity intervention for college students with mental health disorders: A randomized pilot trial. Psychol. Health Med. 2010, 15, 646–659. [Google Scholar] [CrossRef]
- Lee, L.L.; Kuo, Y.C.; Fanaw, D.; Perng, S.J.; Juang, I.F. The effect of an intervention combining self-efficacy theory and pedometers on promoting physical activity among adolescents. J. Clin. Nurs. 2012, 21, 914–922. [Google Scholar] [CrossRef]
- Kattelmann, K.K.; Bredbenner, C.B.; White, A.A.; Greene, G.W.; Hoerr, S.L.; Kidd, T.; Colby, S.; Horacek, T.M.; Phillips, B.W.; Koenings, M.M.; et al. The effects of Young Adults Eating and Active for Health (YEAH): A theory-based Web-delivered intervention. J. Nutr. Educ. Behav. 2014, 46, S27–S41. [Google Scholar] [CrossRef]
- Dillon, K.; Rollo, S.; Prapavessis, H. A combined health action process approach and mHealth intervention to reduce sedentary behaviour in university students—A randomized controlled trial. Psychol. Health 2022, 37, 692–711. [Google Scholar] [CrossRef]
- Cavallo, D.N.; Tate, D.F.; Ries, A.V.; Brown, J.D.; DeVellis, R.F.; Ammerman, A.S. A social media-based physical activity intervention: A randomized controlled trial. Am. J. Prev. Med. 2012, 43, 527–532. [Google Scholar] [CrossRef] [Green Version]
- Caso, D.; Carfora, V.; Capasso, M.; Oliano, D.; Conner, M. Using Messages Targeting Psychological versus Physical Health Benefits to Promote Walking Behaviour: A Randomised Controlled Trial. Appl. Psychol. Health Well Being 2021, 13, 152–173. [Google Scholar] [CrossRef]
- Alshahrani, A.; Siddiqui, A.; Khalil, S.; Farag, S.; Alshahrani, N.; Alsabaani, A.; Korairi, H. WhatsApp-based intervention for promoting physical activity among female college students, Saudi Arabia: A randomized controlled trial. East Mediterr. Health J. 2021, 27, 782–789. [Google Scholar] [CrossRef]
- Sriramatr, S.; Berry, T.R.; Spence, J.C. An Internet-based intervention for promoting and maintaining physical activity: A randomized controlled trial. Am. J. Health Behav. 2014, 38, 430–439. [Google Scholar] [CrossRef]
- Sharp, P.; Caperchione, C. The effects of a pedometer-based intervention on first-year university students: A randomized control trial. J. Am. Coll. Health 2016, 64, 630–638. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Imrey, P.B. Limitations of Meta-analyses of Studies With High Heterogeneity. JAMA Netw. Open 2020, 3, e1919325. [Google Scholar] [CrossRef] [Green Version]
- Butler, S.; Sculley, D.; Santos, D.; Fellas, A.; Girones, X.; Singh-Grewal, D.; Coda, A. Effectiveness of eHealth and mHealth Interventions Supporting Children and Young People Living With Juvenile Idiopathic Arthritis: Systematic Review and Meta-analysis. J. Med. Internet Res. 2022, 24, e30457. [Google Scholar] [CrossRef]
- McEwan, D.; Beauchamp, M.R.; Kouvousis, C.; Ray, C.M.; Wyrough, A.; Rhodes, R.E. Examining the active ingredients of physical activity interventions underpinned by theory versus no stated theory: A meta-analysis. Health Psychol. Rev. 2019, 13, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Gourlan, M.; Bernard, P.; Bortolon, C.; Romain, A.J.; Lareyre, O.; Carayol, M.; Ninot, G.; Boiche, J. Efficacy of theory-based interventions to promote physical activity. A meta-analysis of randomised controlled trials. Health Psychol. Rev. 2016, 10, 50–66. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Sheldon, T.A.; Sutton, A.J.; Abrams, K.R.; Jones, D.R. Methods for exploring heterogeneity in meta-analysis. Eval. Health Prof. 2001, 24, 126–151. [Google Scholar] [CrossRef] [PubMed]
- Kratzke, C.; Cox, C. Smartphone technology and apps: Rapidly changing health promotion. Glob. J. Health Educ. Promot. 2012, 15. [Google Scholar]
- Laranjo, L.; Ding, D.; Heleno, B.; Kocaballi, B.; Quiroz, J.C.; Tong, H.L.; Chahwan, B.; Neves, A.L.; Gabarron, E.; Dao, K.P.; et al. Do smartphone applications and activity trackers increase physical activity in adults? Systematic review, meta-analysis and metaregression. Br. J. Sports Med. 2021, 55, 422–432. [Google Scholar] [CrossRef]
- Ang, S.M.; Chen, J.; Liew, J.H.; Johal, J.; Dan, Y.Y.; Allman-Farinelli, M.; Lim, S.L. Efficacy of Interventions That Incorporate Mobile Apps in Facilitating Weight Loss and Health Behavior Change in the Asian Population: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e28185. [Google Scholar] [CrossRef]
- McEwan, D.; Harden, S.M.; Zumbo, B.D.; Sylvester, B.D.; Kaulius, M.; Ruissen, G.R.; Dowd, A.J.; Beauchamp, M.R. The effectiveness of multi-component goal setting interventions for changing physical activity behaviour: A systematic review and meta-analysis. Health Psychol. Rev. 2016, 10, 67–88. [Google Scholar] [CrossRef]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [Green Version]
- Lauderdale, M.E.; Yli-Piipari, S.; Irwin, C.C.; Layne, T.E. Gender Differences Regarding Motivation for Physical Activity Among College Students: A Self-Determination Approach. Phys. Educ. 2015, 72, 153–172. [Google Scholar]
- Annett, J. Subjective rating scales: Science or art? Ergonomics 2002, 45, 966–987. [Google Scholar] [CrossRef]
- Gosney, J.L.; Scott, J.A.; Snook, E.M.; Motl, R.W. Physical activity and multiple sclerosis: Validity of self-report and objective measures. Fam. Community Health 2007, 30, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.J.; Murphy, M.H.; MacDonncha, C.; Murphy, N.; Nevill, A.M.; Woods, C.B. Validity and Reliability of Three Self-Report Instruments for Assessing Attainment of Physical Activity Guidelines in University Students. Meas. Phys. Educ. Exerc. Sci. 2017, 21, 134–141. [Google Scholar] [CrossRef]
- Monninghoff, A.; Kramer, J.N.; Hess, A.J.; Ismailova, K.; Teepe, G.W.; Tudor Car, L.; Muller-Riemenschneider, F.; Kowatsch, T. Long-term Effectiveness of mHealth Physical Activity Interventions: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Med. Internet Res. 2021, 23, e26699. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.; Othman, A.T.; Yuan, F.; Liang, J. The Effectiveness of Planning Interventions for Improving Physical Activity in the General Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 7337. [Google Scholar] [CrossRef]
- Belanger-Gravel, A.; Godin, G.; Amireault, S. A meta-analytic review of the effect of implementation intentions on physical activity. Health Psychol. Rev. 2013, 7, 23–54. [Google Scholar] [CrossRef]
- Vieira da Silva, M.A.; Sao-Joao, T.M.; Brizon, V.C.; Franco, D.H.; Mialhe, F.L. Impact of implementation intentions on physical activity practice in adults: A systematic review and meta-analysis of randomized clinical trials. PLoS ONE 2018, 13, e0206294. [Google Scholar] [CrossRef]
- Castro, O.; Bennie, J.; Vergeer, I.; Bosselut, G.; Biddle, S.J.H. How Sedentary Are University Students? A Systematic Review and Meta-Analysis. Prev. Sci. 2020, 21, 332–343. [Google Scholar] [CrossRef]
- Buckingham, S.A.; Williams, A.J.; Morrissey, K.; Price, L.; Harrison, J. Mobile health interventions to promote physical activity and reduce sedentary behaviour in the workplace: A systematic review. Digit. Health 2019, 5, 2055207619839883. [Google Scholar] [CrossRef] [Green Version]
- Fitzsimons, C.F.; Kirk, A.; Baker, G.; Michie, F.; Kane, C.; Mutrie, N. Using an individualised consultation and activPAL feedback to reduce sedentary time in older Scottish adults: Results of a feasibility and pilot study. Prev. Med. 2013, 57, 718–720. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Moderators | Categories | Studies | Heterogeneity Test | SMD and 95% CI | p | |
|---|---|---|---|---|---|---|
| p | I2 (%) | |||||
| All studies | 31 | <0.001 | 83.4 | 0.32 (0.19, 0.45) | <0.001 | |
| Outcome | TPA | 8 | <0.001 | 80.2 | 0.34 (0.10, 0.58) | 0.005 |
| MVPA | 8 | 0.042 | 52 | 0.17 (0.01, 0.32) | 0.036 | |
| LPA | 3 | 0.089 | 58.6 | −0.18 (−0.53, 0.18) | 0.327 | |
| Walking | 6 | <0.001 | 84 | 0.35 (−0.06, 0.76) | 0.092 | |
| Steps | 6 | <0.001 | 85 | 0.75 (0.23, 1.28) | 0.005 | |
| Between | 0.031 | |||||
| Participant | Inactive | 17 | <0.001 | 77.5 | 0.19 (−0.03, 0.40) | 0.087 |
| Healthy | 14 | <0.001 | 87.1 | 0.45 (0.27, 0.63) | 0.000 | |
| Between | 0.066 | |||||
| Theory | Yes | 16 | <0.001 | 72.9 | 0.36 (0.13, 0.60) | 0.002 |
| No | 15 | <0.001 | 87.6 | 0.28 (0.11, 0.44) | 0.001 | |
| Between | 0.553 | |||||
| Intervention mode | Smartphone app | 8 | 0.014 | 60.2 | 0.46 (0.19, 0.73) | 0.001 |
| Social media | 9 | <0.001 | 80.9 | 0.26 (−0.07, 0.60) | 0.123 | |
| Accelerometer or Pedometer | 7 | <0.001 | 75.9 | 0.31 (−0.04, 0.66) | 0.078 | |
| Online | 7 | <0.001 | 90.6 | 0.23 (0.04, 0.43) | 0.020 | |
| Between | 0.598 | |||||
| Region | Developing | 8 | <0.001 | 82.6 | 0.63 (0.22, 1.04) | 0.002 |
| Developed | 23 | <0.001 | 75.9 | 0.20 (0.08, 0.32) | 0.001 | |
| Between | 0.046 | |||||
| Instrument | Objective | 13 | <0.001 | 80.2 | 0.52 (0.19, 0.85) | 0.002 |
| Subjective | 18 | <0.001 | 73.8 | 0.16 (0.04, 0.27) | 0.006 | |
| Between | 0.044 | |||||
| Duration | >8 weeks | 18 | <0.001 | 85.7 | 0.22 (0.06, 0.38) | 0.007 |
| ≤8 weeks | 13 | <0.001 | 74.4 | 0.50 (0.25, 0.75) | <0.001 | |
| Between | 0.061 | |||||
| Female ratio | All | 11 | <0.001 | 85.5 | 0.43 (0.10, 0.76) | 0.011 |
| Partial | 20 | <0.001 | 80.7 | 0.26 (0.12, 0.40) | <0.001 | |
| Between | 0.349 | |||||
| Moderators | Categories | Studies | Heterogeneity Test | SMD and 95% CI | p | |
|---|---|---|---|---|---|---|
| p | I2 (%) | |||||
| All studies | 10 | <0.001 | 92.2 | 0.24 (−0.01, 0.49) | 0.057 | |
| Outcome | TPA | 3 | 0.373 | 0 | 0.02 (−0.06, 0.11) | 0.580 |
| MVPA | 3 | 0.144 | 48.4 | −0.22 (−0.55, 0.10) | 0.171 | |
| Walking | 1 | −0.17 (−0.30, −0.04) | 0.009 | |||
| Steps | 3 | 0.414 | 0 | 1.17 (0.87, 1.46) | <0.001 | |
| Between | <0.001 | |||||
| Participant | Inactive | 5 | 0.025 | 64.2 | 0.48 (−0.01, 0.96) | 0.053 |
| Healthy | 5 | <0.001 | 95.4 | 0.10 (−0.18, 0.38) | 0.500 | |
| Between | 0.182 | |||||
| Theory | Yes | 5 | 0.020 | 65.7 | 0.26 (−0.12, 0.64) | 0.176 |
| No | 5 | <0.001 | 95.4 | 0.24 (−0.11, 0.58) | 0.178 | |
| Between | 0.918 | |||||
| Intervention mode | Smartphone app | 1 | 0.90 (0.31, 1.48) | 0.003 | ||
| Social media | ||||||
| Accelerometer or pedometer | 3 | 0.034 | 70.3 | 0.45 (−0.36, 1.26) | 0.275 | |
| Online | 6 | <0.001 | 94.3 | 0.10 (−0.16, 0.36) | 0.462 | |
| Between | 0.043 | |||||
| Region | Developing | 2 | 0.206 | 37.6 | 1.17 (0.73, 1.62) | <0.001 |
| Developed | 8 | <0.001 | 87.2 | −0.00 (−0.20, 0.20) | 0.995 | |
| Between | <0.001 | |||||
| Instrument | objective | 4 | 0.006 | 75.7 | 0.83 (0.23, 1.42) | 0.007 |
| Subjective | 6 | <0.001 | 87.2 | −0.08 (−0.26, 0.11) | 0.410 | |
| Between | 0.005 | |||||
| Duration | >8 weeks | 6 | <0.001 | 86.5 | −0.11 (−0.29, 0.07) | 0.232 |
| ≤8 weeks | 4 | 0.259 | 25.4 | 1.06 (0.72, 1.39) | <0.001 | |
| Between | <0.001 | |||||
| Female ratio | All | 3 | <0.001 | 86 | 0.79 (0.02, 1.56) | 0.044 |
| Partial | 7 | <0.001 | 88.8 | −0.01 (−0.22, 0.20) | 0.912 | |
| Between | 0.049 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, S.; Yuan, F.; Othman, A.T.; Zhou, X.; Shen, G.; Liang, J. The Effectiveness of E-Health Interventions Promoting Physical Activity and Reducing Sedentary Behavior in College Students: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2023, 20, 318. https://doi.org/10.3390/ijerph20010318
Peng S, Yuan F, Othman AT, Zhou X, Shen G, Liang J. The Effectiveness of E-Health Interventions Promoting Physical Activity and Reducing Sedentary Behavior in College Students: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2023; 20(1):318. https://doi.org/10.3390/ijerph20010318
Chicago/Turabian StylePeng, Sanying, Fang Yuan, Ahmad Tajuddin Othman, Xiaogang Zhou, Gang Shen, and Jinghong Liang. 2023. "The Effectiveness of E-Health Interventions Promoting Physical Activity and Reducing Sedentary Behavior in College Students: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 20, no. 1: 318. https://doi.org/10.3390/ijerph20010318