
A Cross-Sectional Study of Knowledge, Attitudes, and Practices concerning COVID-19 Outbreaks in the General Population in Malang District, Indonesia



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design
2.3. Measures
2.3.1. Knowledge, Attitudes, and Practices regarding COVID-19 Prevention
2.3.2. Sociodemographic and Other Factors
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics and Other Factors
3.2. Knowledge, Attitudes and Practices regarding COVID-19
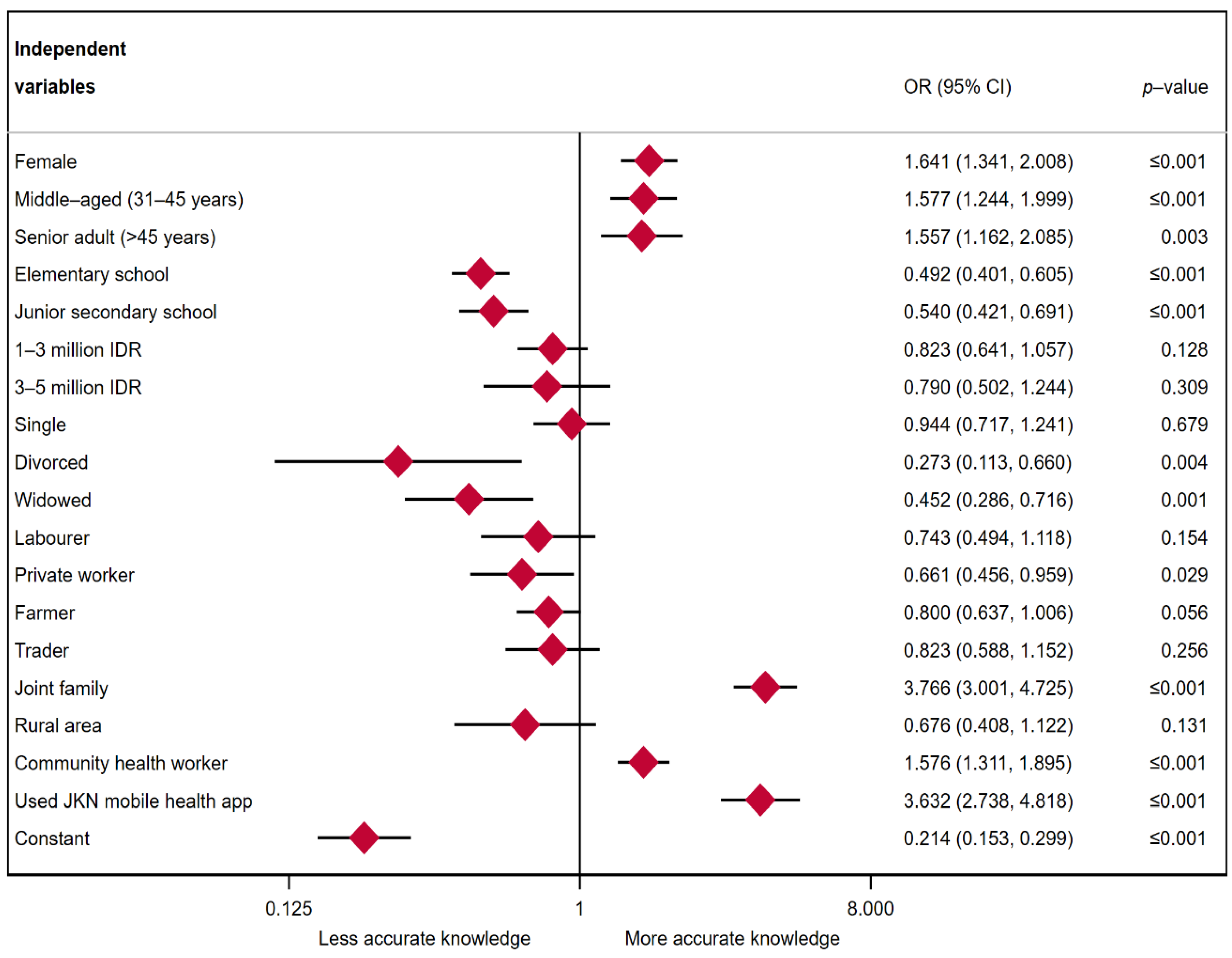
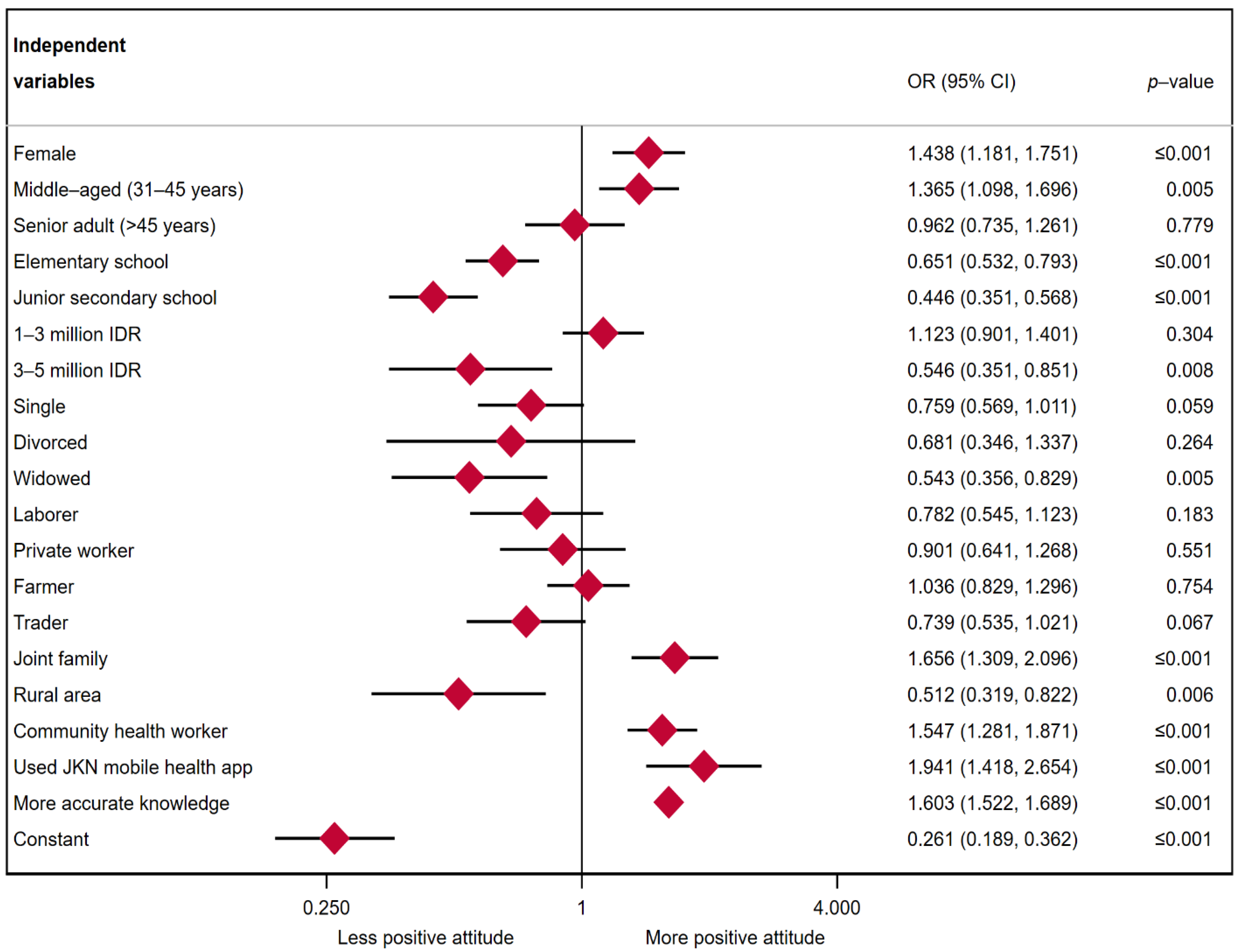
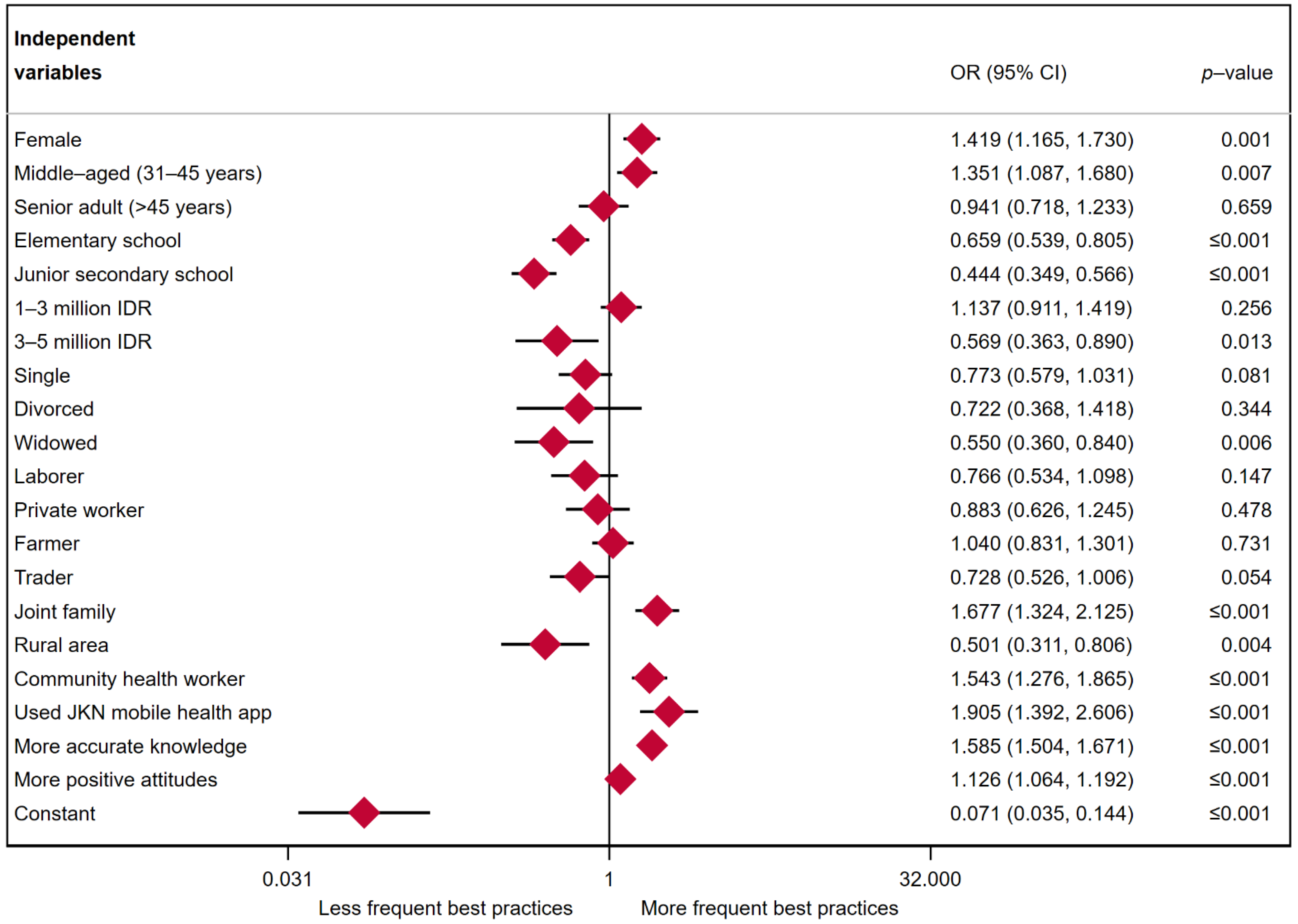
3.3. Multiple Logistic Regression Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease |
| KAP | Knowledge, attitudes, and practices |
| WHO | World Health Organization |
| MERS-CoV | Middle East respiratory syndrome coronavirus |
| IDR | Indonesian Rupiah |
| CI | Confidence Interval |
| USD | United States Dollar |
| OR | Odds ratio |
References
- Person, B.; Sy, F.; Holton, K.; Govert, B.; Liang, A. Fear and stigma: The epidemic within the SARS outbreak. Emerg. Infect. Dis. 2004, 10, 358. [Google Scholar] [CrossRef] [PubMed]
- Masoud, A.T.; Zaazouee, M.S.; Elsayed, S.M.; Ragab, K.M.; Kamal, E.M.; Alnasser, Y.T.; Assar, A.; Nourelden, A.Z.; Istatiah, L.J.; Abd-Elgawad, M.M. KAP-COVIDGLOBAL: A multinational survey of the levels and determinants of public knowledge, attitudes and practices towards COVID-19. BMJ Open 2021, 11, e043971. [Google Scholar] [CrossRef] [PubMed]
- Ferdous, M.Z.; Islam, M.S.; Sikder, M.T.; Mosaddek, A.S.M.; Zegarra-Valdivia, J.; Gozal, D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: An online-based cross-sectional study. PLoS ONE 2020, 15, e0239254. [Google Scholar] [CrossRef] [PubMed]
- Bates, B.R.; Moncayo, A.L.; Costales, J.A.; Herrera-Cespedes, C.A.; Grijalva, M.J. Knowledge, attitudes, and practices towards COVID-19 among Ecuadorians during the outbreak: An online cross-sectional survey. J. Community Health 2020, 45, 1158–1167. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.A.; Alshammary, F.; Amin, J.; Rathore, H.A.; Hassan, I.; Ilyas, M.; Khursheed Alam, M. Knowledge and practice regarding prevention of COVID-19 among the Saudi Arabian population. Work 2020, 66, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Al-Hanawi, M.K.; Angawi, K.; Alshareef, N.; Qattan, A.; Helmy, H.Z.; Abudawood, Y.; Alqurashi, M.; Kattan, W.M.; Kadasah, N.A.; Chirwa, G.C. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: A cross-sectional study. Front. Public Health 2020, 8, 217. [Google Scholar] [CrossRef]
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745. [Google Scholar] [CrossRef]
- Yapi, R.B.; Houngbedji, C.A.; N’Guessan, D.K.; Dindé, A.O.; Sanhoun, A.R.; Amin, A.; Gboko, K.D.; Heitz-Tokpa, K.; Fokou, G.; Bonfoh, B. Knowledge, Attitudes, and Practices (KAP) Regarding the COVID-19 Outbreak in Côte d’Ivoire: Understanding the Non-Compliance of Populations with Non-Pharmaceutical Interventions. Int. J. Environ. Res. Public Health 2021, 18, 4757. [Google Scholar] [CrossRef]
- Fridman, I.; Lucas, N.; Henke, D.; Zigler, C.K. Association between public knowledge about COVID-19, trust in information sources, and adherence to social distancing: Cross-sectional survey. JMIR Public Health Surveill. 2020, 6, e22060. [Google Scholar] [CrossRef]
- Bassi, A.; Arfin, S.; John, O.; Jha, V. An overview of mobile applications (apps) to support the coronavirus disease 2019 response in India. Indian J. Med. Res. 2020, 151, 468. [Google Scholar]
- Pascawati, N.A.; Satoto, T.B.T. Public knowledge, attitudes and practices towards COVID-19. Int. J. Public Health Sci. 2020, 9, 292–302. [Google Scholar]
- Olivia, S.; Gibson, J.; Nasrudin, R.A. Indonesia in the Time of COVID-19. Bull. Indones. Econ. Stud. 2020, 56, 143–174. [Google Scholar] [CrossRef]
- Firmansyah, M.I.; Rahmanto, F.; Setyawan, D. The preparedness for the COVID-19 pandemic management in Indonesia. J. Adm. Kesehat. Indones. 2020, 8, 188–201. [Google Scholar] [CrossRef]
- Windarwati, H.D.; Ati, N.A.L.; Paraswati, M.D.; Ilmy, S.K.; Supianto, A.A.; Rizzal, A.F.; Sulaksono, A.D.; Lestari, R.; Supriati, L. Stressor, coping mechanism, and motivation among health care workers in dealing with stress due to the COVID-19 pandemic in Indonesia. Asian J. Psychiatry 2021, 56, 102470. [Google Scholar] [CrossRef] [PubMed]
- Papagiannis, D.; Malli, F.; Raptis, D.G.; Papathanasiou, I.V.; Fradelos, E.C.; Daniil, Z.; Rachiotis, G.; Gourgoulianis, K.I. Assessment of knowledge, attitudes, and practices towards new coronavirus (SARS-CoV-2) of health care professionals in Greece before the outbreak period. Int. J. Environ. Res. Public Health 2020, 17, 4925. [Google Scholar] [CrossRef] [PubMed]
- Badan Pusat Statistik. Profil Kependudukan Kabupaten Malang; BPS Kabupaten Malang: Malang, Indonesia, 2021. [Google Scholar]
- Worldometer. (n.d.). COVID live-Coronavirus Statistics. Available online: https://www.worldometers.info/coronavirus/ (accessed on 27 March 2022).
- Indonesia Ministry of Health. Peta Sebaran COVID-19 Indonesia (In Indonesian Language). Available online: https://covid19.go.id/peta-sebaran-covid19 (accessed on 27 March 2022).
- Dinas Kesehatan Kabupaten Malang. Profile Puskesmas Kabupaten Malang (In Indonesian language); Dinkes Kab. Malang: Malang, Indonesia, 2020. [Google Scholar]
- Lakshminarasimhappa, M. Web-Based and Smart Mobile App for Data Collection: Kobo Toolbox/Kobo Collect. J. Indian Libr. Assoc. 2021, 57, 72–79. [Google Scholar]
- Wahed, W.Y.A.; Hefzy, E.M.; Ahmed, M.I.; Hamed, N.S. Assessment of knowledge, attitudes, and perception of health care workers regarding COVID-19, a cross-sectional study from Egypt. J. Community Health 2020, 45, 1242–1251. [Google Scholar] [CrossRef]
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Sulistyawati, S.; Hidayat, M.S.; Wijayanti, S.P.M.; Sukesi, T.W.; Hastuti, S.K.W.; Mulasari, S.A.; Tentama, F.; Rokhmayanti, R.; Putra, U.Y.; Djannah, S.N. Knowledge, attitude, and practice towards COVID-19 among university students in Indonesia: A cross-sectional study. Int. J. Public Health 2021, 10, 735–743. [Google Scholar] [CrossRef]
- Azlan, A.A.; Hamzah, M.R.; Sern, T.J.; Ayub, S.H.; Mohamad, E. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS ONE 2020, 15, e0233668. [Google Scholar] [CrossRef]
- Yue, S.; Zhang, J.; Cao, M.; Chen, B. Knowledge, attitudes and practices of COVID-19 among urban and rural residents in China: A cross-sectional study. J. Community Health 2021, 46, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Reuben, R.C.; Danladi, M.M.; Saleh, D.A.; Ejembi, P.E. Knowledge, attitudes and practices towards COVID-19: An epidemiological survey in North-Central Nigeria. J. Community Health 2021, 46, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, M.A.; Noreen, M.; Saleem, T.; Yousaf, I. A cross-sectional survey of knowledge, attitude, and practices (KAP) toward pandemic COVID-19 among the general population of Jammu and Kashmir, India. Soc. Work Public Health 2020, 35, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Kang, B.-A.; You, M. Knowledge, attitudes, and practices (KAP) toward COVID-19: A cross-sectional study in South Korea. BMC Public Health 2021, 21, 295. [Google Scholar] [CrossRef]
- Rivera-Lozada, O.; Galvez, C.A.; Castro-Alzate, E.; Bonilla-Asalde, C.A. Factors associated with knowledge, attitudes and preventive practices towards COVID-19 in health care professionals in Lima, Peru. F1000Research 2021, 10, 1–31. [Google Scholar] [CrossRef]
- Hossain, M.A.; Jahid, M.I.K.; Hossain, K.M.A.; Walton, L.M.; Uddin, Z.; Haque, M.O.; Kabir, M.F.; Arafat, S.Y.; Sakel, M.; Faruqui, R. Knowledge, attitudes, and fear of COVID-19 during the Rapid Rise Period in Bangladesh. PLoS ONE 2020, 15, e0239646. [Google Scholar] [CrossRef]
- Honarvar, B.; Lankarani, K.B.; Kharmandar, A.; Shaygani, F.; Zahedroozgar, M.; Haghighi, M.R.R.; Ghahramani, S.; Honarvar, H.; Daryabadi, M.M.; Salavati, Z. Knowledge, attitudes, risk perceptions, and practices of adults toward COVID-19: A population and field-based study from Iran. Int. J. Public Health 2020, 65, 731–739. [Google Scholar] [CrossRef]
- Rahman, A.; Sathi, N.J. Knowledge, Attitude, and Preventive Practices toward COVID-19 among Bangladeshi Internet Users. Electron. J. Gen. Med. 2020, 17, em245. [Google Scholar] [CrossRef]
- Sheeran, P.; Maki, A.; Montanaro, E.; Avishai-Yitshak, A.; Bryan, A.; Klein, W.M.; Miles, E.; Rothman, A.J. The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: A meta-analysis. Health Psychol. 2016, 35, 1178. [Google Scholar] [CrossRef]
- McEachan, R.; Taylor, N.; Harrison, R.; Lawton, R.; Gardner, P.; Conner, M. Meta-analysis of the reasoned action approach (RAA) to understanding health behaviors. Ann. Behav. Med. 2016, 50, 592–612. [Google Scholar] [CrossRef] [Green Version]
- Godin, G.; Kok, G. The theory of planned behavior: A review of its applications to health-related behaviors. Am. J. Health Promot. 1996, 11, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.T.; Lee, M.; Lee, J.C.Y.; Lee, N.C.T.; Ng, T.Y.; Shafie, A.A.; Thong, K.S. Public KAP towards COVID-19 and antibiotics resistance: A Malaysian survey of knowledge and awareness. Int. J. Environ. Res. Public Health 2021, 18, 3964. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.H.; Alqahtani, S.A.; Alhodaib, A.S.; Al-Wathinani, A.M.; Daoulah, A.; Alhamid, S.; Al-Otaibi, S.N.; Abufayyah, M.; Wazzan, A.M.; Alshahrani, S.S. Knowledge, Attitude, and Practice (KAP) toward the Novel Coronavirus (COVID-19) Pandemic in a Saudi Population-Based Survey. Int. J. Environ. Res. Public Health 2021, 18, 5286. [Google Scholar] [CrossRef] [PubMed]
- Alnasser, A.H.A.; Al-Tawfiq, J.A.; Al-Kalif, M.S.H.; Shahadah, R.F.B.; Almuqati, K.S.A.; Al-Sulaiman, B.S.A.; Alharbi, K.K.S.; Alabbad, F.Y.M.; Alabbad, J.Y.M.; Alquwaiz, I.A.I. Public knowledge, attitudes, and practice towards COVID-19 pandemic in Saudi Arabia: A web-based cross-sectional survey. Med. Sci. 2021, 9, 11. [Google Scholar] [CrossRef]
- Inad, N. Knowledge, Attitude and Practices (KAP) during the COVID-19 pandemic among Palestinians in the Hebron governorate, Palestine. Indian J. Posit. Psychol. 2021, 12, 35–39. [Google Scholar]
- Warner, D.; Procaccino, J.D. Women seeking health information: Distinguishing the web user. J. Health Commun. 2007, 12, 787–814. [Google Scholar] [CrossRef]
- Saah, F.I.; Amu, H.; Seidu, A.-A.; Bain, L.E. Health knowledge and care seeking behaviour in resource-limited settings amidst the COVID-19 pandemic: A qualitative study in Ghana. PLoS ONE 2021, 16, e0250940. [Google Scholar] [CrossRef]
- Muslih, M.; Susanti, H.D.; Rias, Y.A.; Chung, M.-H. Knowledge, attitude and practice of Indonesian residents toward COVID-19: A cross-sectional survey. Int. J. Environ. Res. Public Health 2021, 18, 4473. [Google Scholar] [CrossRef]
- Cotten, S.R.; Gupta, S.S. Characteristics of online and offline health information seekers and factors that discriminate between them. Soc. Sci. Med. 2004, 59, 1795–1806. [Google Scholar] [CrossRef]
- Mistry, S.K.; Ali, A.M.; Yadav, U.N.; Ghimire, S.; Hossain, M.B.; Das Shuvo, S.; Saha, M.; Sarwar, S.; Nirob, M.M.H.; Sekaran, V.C. Older adults with non-communicable chronic conditions and their health care access amid COVID-19 pandemic in Bangladesh: Findings from a cross-sectional study. PLoS ONE 2021, 16, e0255534. [Google Scholar] [CrossRef]
- Suryadarma, D.; Jones, G.W. Education in Indonesia; Institute of Southeast Asian Studies: Pasar Panjang, Singapore, 2013. [Google Scholar]
- Peretti-Watel, P.; Seror, V.; Cortaredona, S.; Launay, O.; Raude, J.; Verger, P.; Beck, F.; Legleye, S.; L’haridon, O.; Ward, J. Attitudes about COVID-19 lockdown among general population, France, March 2020. Emerg. Infect. Dis. 2021, 27, 301. [Google Scholar] [CrossRef] [PubMed]
- Puspitasari, I.M.; Yusuf, L.; Sinuraya, R.K.; Abdulah, R.; Koyama, H. Knowledge, attitude, and practice during the COVID-19 pandemic: A review. J. Multidiscip. Healthc. 2020, 13, 727. [Google Scholar] [CrossRef] [PubMed]
- Nobles, J.; Buttenheim, A. Marriage and socioeconomic change in contemporary Indonesia. J. Marriage Fam. 2008, 70, 904–918. [Google Scholar] [CrossRef] [PubMed]
- Goldman, N.; Korenman, S.; Weinstein, R. Marital status and health among the elderly. Soc. Sci. Med. 1995, 40, 1717–1730. [Google Scholar] [CrossRef]
- Mohammed, M.; Sha’aban, A.; Jatau, A.I.; Yunusa, I.; Isa, A.M.; Wada, A.S.; Obamiro, K.; Zainal, H.; Ibrahim, B. Assessment of COVID-19 information overload among the general public. J. Racial Ethn. Health Disparities 2021, 9, 184–192. [Google Scholar] [CrossRef]
- Chua, A.Q.; Tan, M.M.J.; Verma, M.; Han, E.K.L.; Hsu, L.Y.; Cook, A.R.; Teo, Y.Y.; Lee, V.J.; Legido-Quigley, H. Health system resilience in managing the COVID-19 pandemic: Lessons from Singapore. BMJ Glob. Health 2020, 5, e003317. [Google Scholar] [CrossRef]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatry 2020, 51, 102083. [Google Scholar]
- Peña-Longobardo, L.; Rodríguez-Sánchez, B.; Oliva-Moreno, J. The impact of widowhood on wellbeing, health, and care use: A longitudinal analysis across Europe. Econ. Hum. Biol. 2021, 43, 101049. [Google Scholar] [CrossRef]
- Zehra, S.S.; Khalil, M.A.; Shoukat, L. When the Big Shots Deviate: On the KAP of Religious Clerics Regarding Prevention of COVID-19. Risk Manag. Healthc. Policy 2020, 13, 2801. [Google Scholar] [CrossRef]
- Marmot, M. The influence of income on health: Views of an epidemiologist. Health Aff. 2002, 21, 31–46. [Google Scholar] [CrossRef]
- Lau, L.L.; Hung, N.; Go, D.J.; Ferma, J.; Choi, M.; Dodd, W.; Wei, X. Knowledge, attitudes and practices of COVID-19 among income-poor households in the Philippines: A cross-sectional study. J. Glob. Health 2020, 10, 011007. [Google Scholar] [CrossRef] [PubMed]
- Weech-Maldonado, R.; Miller, M.J.; Lord, J.C. The relationships among socio-demographics, perceived health, and happiness. Appl. Res. Qual. Life 2017, 12, 289–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirowsky, J.; Ross, C.E. Education, Social Status, and Health; Routledge: Abingdon, UK, 2017. [Google Scholar]
- Shih, S.F.; Wagner, A.L.; Masters, N.B.; Prosser, L.A.; Lu, Y.; Zikmund-Fisher, B.J. Vaccine hesitancy and rejection of a vaccine for the novel coronavirus in the United States. Front. Immunol. 2021, 12, 2275. [Google Scholar] [CrossRef] [PubMed]
- Saqlain, M.; Ahmed, A.; Gulzar, A.; Naz, S.; Munir, M.M.; Ahmed, Z.; Kamran, S. Public Knowledge and Practices regarding COVID-19: A cross-sectional survey from Pakistan. Front. Public Health 2021, 9, 377. [Google Scholar]
- Bhaumik, S.; Moola, S.; Tyagi, J.; Nambiar, D.; Kakoti, M. Community health workers for pandemic response: A rapid evidence synthesis. BMJ Glob. Health 2020, 5, e002769. [Google Scholar] [CrossRef]
- Mane Abhay, B.; Khandekar Sanjay, V. Strengthening primary health care through Asha Workers: A novel approach in India. Prim. Health Care 2014, 4, 2167-1079. [Google Scholar]
- Gilson, L.; Walt, G.; Heggenhougen, K.; Owuor-Omondi, L.; Perera, M.; Ross, D.; Salazar, L. National community health worker programs: How can they be strengthened? J. Public Health Policy 1989, 10, 518–532. [Google Scholar] [CrossRef]
- Johnson, C.D.; Noyes, J.; Haines, A.; Thomas, K.; Stockport, C.; Ribas, A.N.; Harris, M. Learning from the Brazilian community health worker model in North Wales. Glob. Health 2013, 9, 25. [Google Scholar] [CrossRef] [Green Version]
- Sujarwoto, S.; Maharani, A. Participation in community-based health care interventions (CBHIs) and its association with hypertension awareness, control and treatment in Indonesia. PLoS ONE 2020, 15, e0244333. [Google Scholar] [CrossRef]
- Hassounah, M.; Raheel, H.; Alhefzi, M. Digital response during the COVID-19 pandemic in Saudi Arabia. J. Med. Internet Res. 2020, 22, e19338. [Google Scholar] [CrossRef]
- Huang, Z.; Guo, H.; Lee, Y.-M.; Ho, E.C.; Ang, H.; Chow, A. Performance of digital contact tracing tools for COVID-19 response in Singapore: Cross-sectional study. JMIR Mhealth Uhealth 2020, 8, e23148. [Google Scholar] [CrossRef] [PubMed]
- Whitelaw, S.; Mamas, M.A.; Topol, E.; Van Spall, H.G. Applications of digital technology in COVID-19 pandemic planning and response. Lancet Digit. Health 2020, 2, e435–e440. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No | Knowledge about COVID-19 | Coding and Cut-Off Levels |
|---|---|---|
| 1 | Is COVID-19 a dangerous disease? | Correct answer = 1, wrong answer or don’t know = 0. A cut-off level of ≥4 was chosen to indicate a respondent with a precise understanding of COVID-19 [4]. |
| 2 | Does it affect only humans? | |
| 3 | Does it transmit from humans to animals? | |
| 4 | Does it transmit from animals to humans? | |
| 5 | Is it transmitted by animal products (e.g., milk, meat)? | |
| 6 | Is it transmitted in well-cooked products? | |
| Attitudes toward COVID-19 | ||
| 1 | It is crucial to report a suspected case to health authorities | Disagree = 0, undecided = 1, agree = 2. A cut-off level of ≥11 was set to indicate a respondent with positive attitudes towards the prevention of COVID-19 [4]. |
| 2 | It is important to use a face mask in crowded places | |
| 3 | It is important to wash hands and face after being outside | |
| 4 | COVID-19 is a preventable disease | |
| 5 | It can be treated at home | |
| 6 | Health education can play an important role in COVID-19 prevention | |
| Practice toward COVID-19 | ||
| 1 | Do you use tissues or handkerchiefs when you cough/sneeze? | Yes = 1, no = 0, sometimes = 0 for questions 1–6. For question 7, yes = 0, sometimes = 0, no = 1. A cut-off level of ≥6 was set to indicate frequent best practices [4]. |
| 2 | Do you wash hands frequently using water and soap? | |
| 3 | Do you avoid touching face and eyes? | |
| 4 | Do you maintain social distance (or quarantine at home)? | |
| 5 | Do you eat healthy food focusing on the outbreak? | |
| 6 | Do you maintain a healthy lifestyle focusing on the outbreak? | |
| 7 | Do you obey all government rules related to COVID? |
| Variables | n (%) |
|---|---|
| Sex | |
| Male | 1286 (37.6) |
| Female | 2139 (62.4) |
| Age | |
| Young adult (17–30 years) | 1146 (33.5) |
| Middle-aged adult (30–45 years) | 1565 (45.7) |
| Older adult (>45 years) | 714 (20.8) |
| Education | |
| Elementary or less | 1763 (51.5) |
| Junior secondary | 699 (20.4) |
| High school or more | 963 (28.1) |
| Monthly family income (in IDR) | |
| <1 million | 2818 (82.3) |
| 1–3 million | 485 (14.1) |
| >3 million | 122 (3.6) |
| Marital status | |
| Single | 736 (21.5) |
| Married | 2508 (73.2) |
| Divorced | 41 (1.2) |
| Widowed | 140 (4.1) |
| Type of employment | |
| Student | 948 (27.7) |
| Laborer (i.e., construction, factory workers) | 205 (6.0) |
| Civil servant | 62 (1.8) |
| Privately employed (i.e., bank, supermarket, restaurant, hotel) | 230 (6.7) |
| Farmer | 1763 (51.5) |
| Trader (merchant, dealer, salesperson) | 217 (6.3) |
| Family type | |
| Nuclear | 2185 (63.8) |
| Joint | 1240 (36.2) |
| Used JKN COVID-19 screening app | |
| No | 3179 (92.8) |
| Yes | 246 (7.2) |
| Informed by community health workers about COVID-19 prevention | |
| No | 2596 (75.8) |
| Yes | 829 (24.2) |
| Residential area | |
| Rural | 3325 (97.1) |
| Urban | 100 (2.9) |
| Knowledge about COVID-19 | |
| More accurate | 914 (25.3%) |
| Less accurate | 2661 (74.7%) |
| Attitudes towards COVID-19 | |
| More positive attitude | 784 (36.6%) |
| Less positive attitude | 2641 (62.4%) |
| Practices regarding COVID-19 | |
| More frequent best practices | 1670 (48.8%) |
| Less frequent best practices | 1755 (51.2%) |
| Knowledge about COVID-19 | Yes | No | Don’t Know |
|---|---|---|---|
| Is COVID-19 a dangerous disease? | 3251 (94.9%) | 84 (2.5%) | 90 (2.6%) |
| Does it affect only humans? | 2484 (72.5%) | 586 (17.1%) | 355 (10.4%) |
| Does it transmit from humans to animals? | 1133 (33.1%) | 1063 (31.0%) | 1229 (35.9%) |
| Does it transmit from animals to humans? | 1608 (46.9%) | 640 (18.7%) | 1177 (34.4%) |
| Is it transmitted by animal products (e.g., milk, meat)? | 1039 (30.3%) | 1116 (32.6%) | 1270 (37.1%) |
| Is it transmitted in well-cooked products? | 730 (21.3%) | 1696 (49.5%) | 999 (29.2%) |
| Attitudes toward COVID-19 | Agree | Undecided | Disagree |
| It is crucial to report a suspected case to health authorities | 3209 (93.7%) | 159 (4.6%) | 57 (1.7%) |
| It is important to use a face mask in crowded places | 3328 (97.2%) | 62 (1.8%) | 35 (1.0%) |
| It is important to wash hands and face after being outside | 3305 (96.5%) | 63 (1.8%) | 57 (1.7%) |
| COVID-19 is a preventable disease | 3151 (92.0%) | 211 (6.2%) | 63 (1.8%) |
| It can be treated at home | 2388 (69.7%) | 532 (15.5%) | 505 (14.7%) |
| Health education can play an important role in COVID-19 prevention | 3198 (93.4%) | 140 (4.1%) | 87 (2.5%) |
| Practices regarding COVID-19 | Yes | No | Sometimes |
| Do you use tissues or handkerchiefs when you cough/sneeze? | 1983 (57.9%) | 231 (6.7%) | 1211 (35.4%) |
| Do you wash your hands frequently using water and soap? | 2470 (72.1%) | 66 (1.9%) | 889 (26.0%) |
| Do you avoid touching face and eyes? | 1774 (51.8%) | 340 (9.9%) | 1311 (38.3%) |
| Do you maintain social distance (or quarantine at home)? | 1961 (57.3%) | 371 (10.8%) | 1093 (31.9%) |
| Do you eat healthy food focusing on the outbreak? | 2123 (62.0%) | 207 (6.0%) | 1095 (32.0%) |
| Do you maintain a healthy lifestyle focusing on the outbreak? | 2374 (69.3%) | 112 (3.3%) | 939 (27.4%) |
| Do you obey all government rules related to COVID-19? | 1984 (57.9%) | 590 (17.2%) | 851 (24.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sujarwoto, S.; Holipah, H.; Maharani, A. A Cross-Sectional Study of Knowledge, Attitudes, and Practices concerning COVID-19 Outbreaks in the General Population in Malang District, Indonesia. Int. J. Environ. Res. Public Health 2022, 19, 4287. https://doi.org/10.3390/ijerph19074287
Sujarwoto S, Holipah H, Maharani A. A Cross-Sectional Study of Knowledge, Attitudes, and Practices concerning COVID-19 Outbreaks in the General Population in Malang District, Indonesia. International Journal of Environmental Research and Public Health. 2022; 19(7):4287. https://doi.org/10.3390/ijerph19074287
Chicago/Turabian StyleSujarwoto, Sujarwoto, Holipah Holipah, and Asri Maharani. 2022. "A Cross-Sectional Study of Knowledge, Attitudes, and Practices concerning COVID-19 Outbreaks in the General Population in Malang District, Indonesia" International Journal of Environmental Research and Public Health 19, no. 7: 4287. https://doi.org/10.3390/ijerph19074287