
Rapid Antigen Test LumiraDxTM vs. Real Time Polymerase Chain Reaction for the Diagnosis of SARS-CoV-2 Infection: A Retrospective Cohort Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Testing Procedure and Data Collection
2.2. Statistical Methods
3. Results
3.1. Study Population
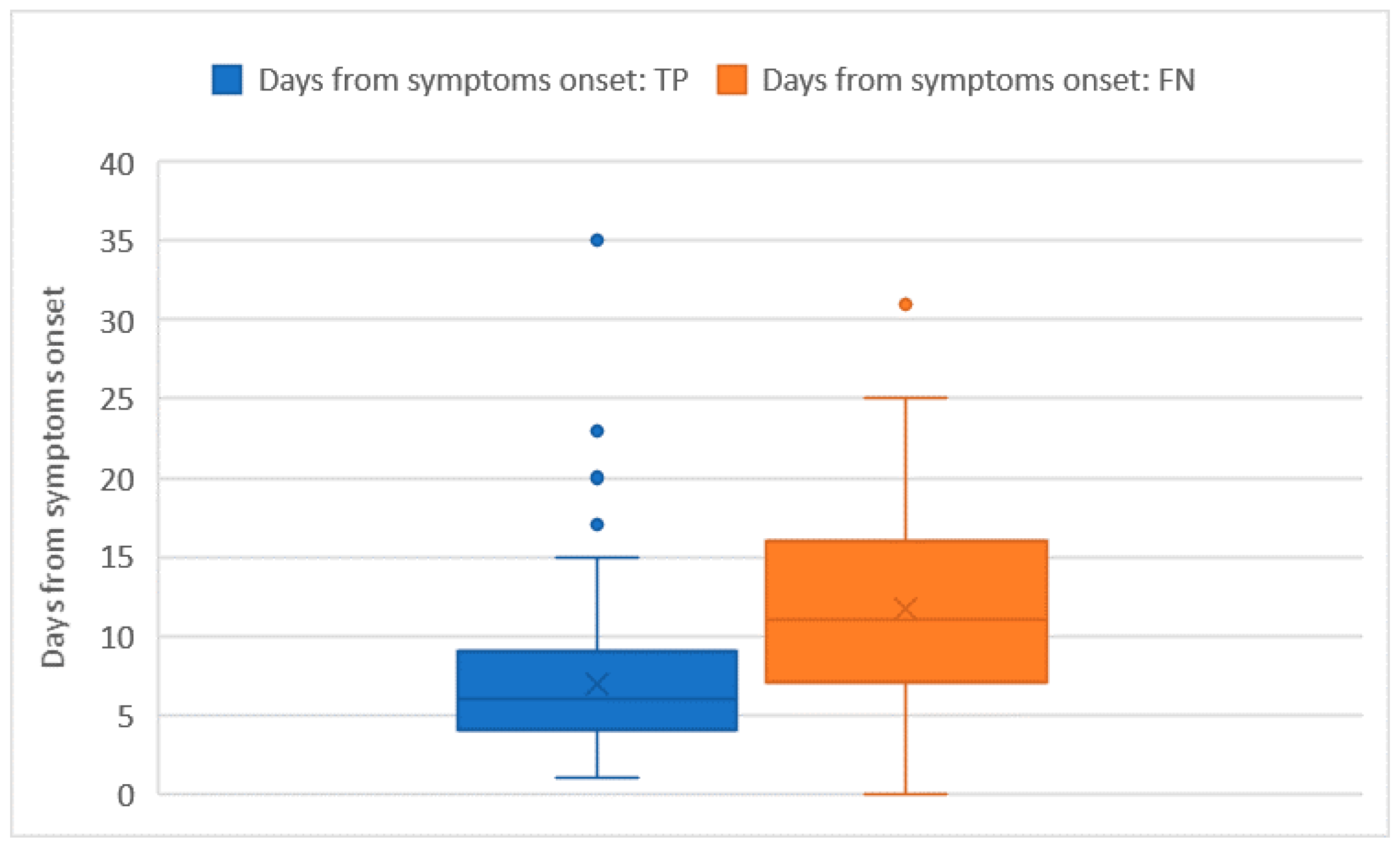
3.2. Impact of Ct Values and Days from Symptoms’ Onset on LumiraDx™ Sensitivity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Health Emergencies, Coronavirus Disease (COVID-19) Outbreak. World Health Organization: Geneva, Switzerland. 2020. Available online: https://www.euro.who.int/en/search?q=Health+Emergencies%2C+Coronavirus+Disease+%28COVID-19%29+ (accessed on 6 February 2022).
- Mathuria, J.P.; Yadav, R.; Rajkumar. Laboratory diagnosis of SARS-CoV-2—A review of current methods. J. Infect. Public Health 2020, 13, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Huff, H.V.; Singh, A. Asymptomatic transmission during the COVID-19 pandemic and implications for public health strategies. Clin. Infect. Dis. 2020, 71, 2752–2756. [Google Scholar] [CrossRef] [PubMed]
- Manabe, Y.C.; Sharfstein, J.S.; Armstrong, K. The Need for More and Better Testing for COVID-19. JAMA 2020, 324, 2153–2154. [Google Scholar] [CrossRef] [PubMed]
- FIND. SARS-CoV-2 Diagnostic Pipeline. Available online: https://www.finddx.org/covid-19/pipeline/?avance=Commercialized&type=Rapid+diagnostic+tests&test_target=Antigen&status=all§ion=immunoassays&action=default#diag_tab (accessed on 21 December 2020).
- Linares, M.; Pérez-Tanoira, R.; Carrero, A.; Romanyk, J.; Pérez-García, F.; Gómez-Herruz, P.; Arroyo, T.; Cuadros, J. Panbio antigen rapid test is reliable to diagnose SARS-CoV-2 infection in the first 7 days after the onset of symptoms. J. Clin. Virol. 2020, 133, 104659. [Google Scholar] [CrossRef] [PubMed]
- Nalumansi, A.; Lutalo, T.; Kayiwa, J.; Watera, C.; Balinandi, S.; Kiconco, J.; Nakaseegu, J.; Olara, D.; Odwilo, E.; Serwanga, J.; et al. Field Evaluation of the Performance of a SARS-CoV-2 Antigen Rapid Diagnostic Test in Uganda using Nasopharyngeal Samples. Int. J. Infect. Dis. 2021, 104, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Mak, G.C.K.; Lau, S.S.Y.; Wong, K.K.Y.; Chow, N.L.S.; Lau, C.S.; Lam, E.T.K.; Chan, R.C.W.; Tsang, D.N.C. Analytical sensitivity and clinical sensitivity of the three rapid antigen detection kits for detection of SARS-CoV-2 virus. J. Clin. Virol. 2020, 133, 104684. [Google Scholar] [CrossRef] [PubMed]
- Cerutti, F.; Burdino, E.; Milia, M.G.; Allice, T.; Gregori, G.; Bruzzone, B.; Ghisetti, V. Urgent need of rapid tests for SARS-CoV-2 antigen detection: Evaluation of the SD-Biosensor antigen test for SARS-CoV-2. J. Clin. Virol. 2020, 132, 104654. [Google Scholar] [CrossRef] [PubMed]
- Scohy, A.; Anantharajah, A.; Bodéus, M.; Kabamba-Mukadi, B.; Verroken, A.; Rodriguez-Villalobos, H. Low performance of rapid antigen detection test as frontline testing for COVID-19 diagnosis. J. Clin. Virol. 2020, 129, 104455. [Google Scholar] [CrossRef] [PubMed]
- Lambert-Niclot, S.; Cuffel, A.; Le Pape, S.; Vauloup-Fellous, C.; Morand-Joubert, L.; Roque-Afonso, A.-M.; Le Goff, J.; Delaugerre, C. Evaluation of a Rapid Diagnostic Assay for Detection of SARS-CoV-2 Antigen in Nasopharyngeal Swabs. J. Clin. Microbiol. 2020, 58, e00977-20. [Google Scholar] [CrossRef] [PubMed]
- Brummer, L.E.; Katzenschlager, S.; Gaeddert, M.; Erdmann, C.; Schmitz, S.; Bota, M.; Grilli, M.; Larmann, J.; Weigand, M.A.; Pollock, N.R.; et al. Accuracy of novel antigen rapid diagnostics for SARS-CoV-2: A living systematic review and meta-analysis. PLoS Med. 2021, 18, e1003735. [Google Scholar] [CrossRef] [PubMed]
- LumiraDx. Available online: https://www.lumiradx.com/assts/pfds/covid-19-antigen-test/sars-cov-2-antigent-product-insert/antigen-test-strip-produvt-insert-de-en.pdf?v=10 (accessed on 4 February 2022).
- Administration UFaD. Emergency Use Authorization. 2020. Available online: https://www.fda.gov/emergency-preparedness-and-response/mcm-legal-regulatory-and-policy-framework/emergency-use-authorization (accessed on 12 February 2021).
- Limited, L. COVID-19 SARS-CoV-2 Antigen Test. 2020. Available online: https://www.lumiradx.com/uk-en/customer-services (accessed on 12 February 2021).
- Alliance, W.B. New COVID-19 Testing Service Now Available in Boots UK Stores. LumiraDx: London, UK, 2020. Available online: https://www.boots-uk.com/corporate-social-responsibility/ (accessed on 12 January 2021).
- Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection, World Health Organization. Interim Guidance. WHO. 6 October 2021. Available online: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-sars-cov-2infection-using-rapid-immunoassays (accessed on 5 February 2022).
- European Centre for Disease Prevention and Control. Option for the Use of Rapid Antigen Detection Tests for OCVID-19 in the EU/EEA—First Update. ECDC. 26 October 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/options-use-rapid-antigen-tests-covid-19-eueea-first-update (accessed on 5 February 2022).
- Kruger, L.J.; Klein, J.A.F.; Tobian, F.; Gaeddert, M.; Lainati, F.; Klemm, S.; Schnitzler, P.; Bartenschlager, R.; Cerikan, B.; Neufeldt, C.J.; et al. Evaluation of accuracy, exclusivity, limit-of-detection and ease-of-use of LumiraDx™-Antigen-detecting point-of-care device for SARSCoV-2. Infection 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mak, G.C.K.; Cheng, P.K.C.; Lau, S.S.Y.; Wong, K.K.Y.; Lau, C.S.; Lam, E.T.K.; Chan, R.C.W.; Tsang, D.N.C. Evaluation of rapid antigen test for detection of SARS-CoV-2 virus. J. Clin. Virol. 2020, 129, 104500. [Google Scholar] [CrossRef] [PubMed]
- Kohmer, N.; Toptan, T.; Pallas, C.; Karaca, O.; Pfeiffer, A.; Westhaus, S.; Widera, M.; Berger, A.; Hoehl, S.; Kammel, M.; et al. The Comparative Clinical Performance of Four SARS-CoV-2 Rapid Antigen Tests and Their Correlation to Infectivity In Vitro. J. Clin. Med. 2021, 10, 328. [Google Scholar] [CrossRef] [PubMed]
- Kissler, S.M.; Fauver, J.R.; Mack, C.; Olesen, S.W.; Tai, C.; Shiue, K.Y.; Kalinich, C.C.; Jednak, S.; Ott, I.M.; Vogels, C.B.F.; et al. Viral dynamics of acute SARS-CoV-2 infection and applications to diagnostic and public health strategies. PLoS Biol. 2021, 19, e3001333. [Google Scholar] [CrossRef] [PubMed]
- Sia, S.F.; Yan, L.; Chin, A.W.H.; Fung, K.; Choy, K.-T.; Wong, A.Y.L.; Kaewpreedee, P.; Perera, R.A.P.M.; Poon, L.L.M.; Nicholls, J.M.; et al. Pathogenesis and transmission of SARS-CoV-2 in golden hamsters. Nature 2020, 583, 834–838. [Google Scholar] [CrossRef] [PubMed]
- Wolfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-19. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bullard, J.; Dust, K.; Funk, D.; Strong, J.E.; Alexander, D.; Garnett, L.; Boodman, C.; Bello, A.; Hedley, A.; Schiffman, Z.; et al. Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic Samples. Clin. Infect. Dis. 2020, 71, 2663–2666. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID.19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cevik, M.; Tate, M.; Lloyd, O.; Maraolo, A.E.; Schafers, J.; Ho, A. SARS-CoV-2, SARS-CoV, and MERS-CoV viral load dynamics, duration of viral shedding, and infectiousness: A systematic review and meta-analysis. Lancet Microbe 2021, 2, e13–e22. [Google Scholar] [CrossRef]
- Walsh, K.A.; Jordan, K.; Clyne, B.; Rohde, D.; Drummond, L.; Byrne, P.; Ahern, S.; Carty, P.G.; O’Brien, K.K.; O’Murchu, E.; et al. SARS-CoV-2 detection, viral load and infectivity over the course of an infection. J. Infect. 2020, 81, 357–371. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.iss.it/primo-piano/-/asset_publisher/3f4alMwzN1Z7/content/cs-n%25C2%25B0-25-2021-covid-19-in-italia-la-variante-inglese-all-91-6%2525.-il-4-0%2525-dei-casi-con-quella-brasiliana- (accessed on 6 February 2022).
- European Centre for Disease Prevention and Control. SARS-CoV-2 Variants of Concern as of 3 February 2022. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 3 February 2022).
- Medical Device Network. LumiraDx’s COVID-19 Antigen Test Can Identify Omicron Variant. Available online: https://www.medicaldevice-network.com/news/lumiradx-covid-19-antigen-omicron-variant/ (accessed on 5 February 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Test n | LumiraDxTM + n (%) | LumiraDxTM − n (%) | RT-PCR + n (%) | RT-PCR − n (%) | FN n (%) | FP n (%) |
|---|---|---|---|---|---|---|---|
| Sex | |||||||
| F | 105 | 64 (61) | 41 (39) | 81 (77.1) | 24 (22.9) | 18 (43.9) | 1 (1.6) |
| M | 177 | 113 (63.8) | 64 (36.2) | 147 (83.1) | 30 (16.9) | 36 (56.3) | 2 (1.8) |
| Age class | |||||||
| 0–39 | 37 | 13 (35.1) | 24 (64.9) | 18 (48.6) | 19 (51.4) | 6 (25) | 1 (7.7) |
| 40–59 | 88 | 55 (62.5) | 33 (37.5) | 69 (78.4) | 19 (21.6) | 15 (45.5) | 1 (1.8) |
| 60–79 | 115 | 80 (69.6) | 35 (30.4) | 106 (92.2) | 9 (7.8) | 27 (77.1) | 1 (1.3) |
| 80+ | 42 | 29 (69) | 13 (31) | 35 (83.3) | 7 (16.7) | 6 (46.2) | 0 (0) |
| Diagnosis | |||||||
| Asymptomatic | 32 | 4 (12.5) | 28 (87.5) | 6 (18.8) | 26 (81.3) | 3 (10.7) | 1 (25) |
| Pauci-symptomatic | 146 | 117 (80.1) | 29 (19.9) | 138 (94.5) | 8 (5.5) | 23 (79.3) | 2 (1.7) |
| Pneumonia | 102 | 55 (53.9) | 47 (46.1%) | 83 (81.4) | 19 (18.6) | 28 (59.6) | 0 (0) |
| Neurological symptoms | 2 | 1 (50) | 1 (50) | 1 (50) | 1 (50) | 0 (0) | 0 (0) |
| Overall | 282 | 177 (62.8) | 105 (3.2) | 228 (80.9) | 54 (19.1) | 54 (51.4) | 3 (1.7) |
| Attributes of Tested Subject | Sensitivity | Specificity | PPV | NPV | Accuracy | K |
|---|---|---|---|---|---|---|
| Sex | ||||||
| F | 77.8 (68.7–86.9) | 95.8 (87.8–100) | 98.4 (95.4–100) | 56.1 (40.9–71.3) | 81.9 (74.5–89.3) | 0.59 (0.43–0.74) |
| M | 75.5 (68.5–82.5) | 93.3 (84.4–100) | 98.2 (95.8–100) | 43.8 (31.6–56) | 78.5 (72.5–84.5) | 0.47 (0.35–0.60) |
| Age class | ||||||
| 0–39 | 66.7 (44.9–88.5) | 94.7 (84.7–100) | 92.3 (77.8–100) | 75 (57.7–92.3) | 81.1 (68.5–93.7) | 0.62 (0.37–0.86) |
| 40–59 | 78.3 (68.6–88) | 94.7 (84.7–100) | 98.2 (94.7–100) | 54.4 (37.4–71.4) | 81.8 (73.7–89.9) | 0.58 (0.40–0.76) |
| 60–79 | 74.5 (66.2–82.8) | 88.9 (68.4–100) | 98.8 (96.4–100) | 22.9 (9–36.8) | 75.7 (67.9–83.5) | 0.27 (0.11–0.44) |
| 80+ | 82.9 (70.4–95.4) | 100 (100–100) | 100 (100–100) | 53.8 (26.7–80.9) | 85.7 (75.1–96.3) | 0.62 (0.36–0.88) |
| Diagnosis | ||||||
| Asymptomatic | 50 (10–90) | 96.2 (88.8–100) | 75 (32.6–100) | 89.3 (77.8–100) | 87.5 (76–99) | 0.53 (0.13–0.93) |
| Pauci-symptomatic | 83.3 (77.1–89.5) | 75 (45–100) | 98.3 (96–100) | 20.7 (6–35.4) | 82.9 (76.8–89) | 0.26 (0.07–0.45) |
| Pneumonia | 66.3 (56.1–76.5) | 100 (100–100) | 100 (100–100) | 40.4 (26.4–54.4) | 72.5 (63.8–81.2) | 0.42 (0.27–0.57) |
| Neurological symptoms | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 100 (100–100) | 1 (1–1) |
| Overall | 76.3 (70.8–81.8) | 94.4 (88.3–100) | 98.3 (96.4–100) | 48.6 (39–58.2) | 79.8 (75.1–84.5) | 0.52 (0.42–0.62) |
| Considered Outcome: False Negative Result of LumiraDxTM Swab | |||||
|---|---|---|---|---|---|
| Model | p-Value | adjOR | 95% CI adjOR | ||
| Lower | Upper | ||||
| Age group | 0–39 | Ref | - | - | - |
| 40–59 | 0.837 | 0.846 | 0.173 | 4.146 | |
| 60–79 | 0.704 | 1.348 | 0.289 | 6.279 | |
| 80+ | 0.424 | 0.475 | 0.076 | 2.952 | |
| Sex | Male | 0.434 | 0.716 | 0.311 | 1.652 |
| Days | ≤10 | Ref | - | - | - |
| 11–19 | 0.001 | 4.326 | 1.816 | 10.304 | |
| ≥20 | 0.001 | 16.014 | 3.116 | 82.314 | |
| Ct | ≤25 | Ref | - | - | - |
| 26–31 | 0.007 | 3.936 | 1.463 | 10.588 | |
| ≥32 | <0.001 | 14.482 | 5.443 | 38.532 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cattelan, A.M.; Sasset, L.; Zabeo, F.; Ferrari, A.; Rossi, L.; Mazzitelli, M.; Cocchio, S.; Baldo, V. Rapid Antigen Test LumiraDxTM vs. Real Time Polymerase Chain Reaction for the Diagnosis of SARS-CoV-2 Infection: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 3826. https://doi.org/10.3390/ijerph19073826
Cattelan AM, Sasset L, Zabeo F, Ferrari A, Rossi L, Mazzitelli M, Cocchio S, Baldo V. Rapid Antigen Test LumiraDxTM vs. Real Time Polymerase Chain Reaction for the Diagnosis of SARS-CoV-2 Infection: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(7):3826. https://doi.org/10.3390/ijerph19073826
Chicago/Turabian StyleCattelan, Anna Maria, Lolita Sasset, Federico Zabeo, Anna Ferrari, Lucia Rossi, Maria Mazzitelli, Silvia Cocchio, and Vincenzo Baldo. 2022. "Rapid Antigen Test LumiraDxTM vs. Real Time Polymerase Chain Reaction for the Diagnosis of SARS-CoV-2 Infection: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 7: 3826. https://doi.org/10.3390/ijerph19073826