
The Effects of Playground Interventions on Accelerometer-Assessed Physical Activity in Pediatric Populations: A Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
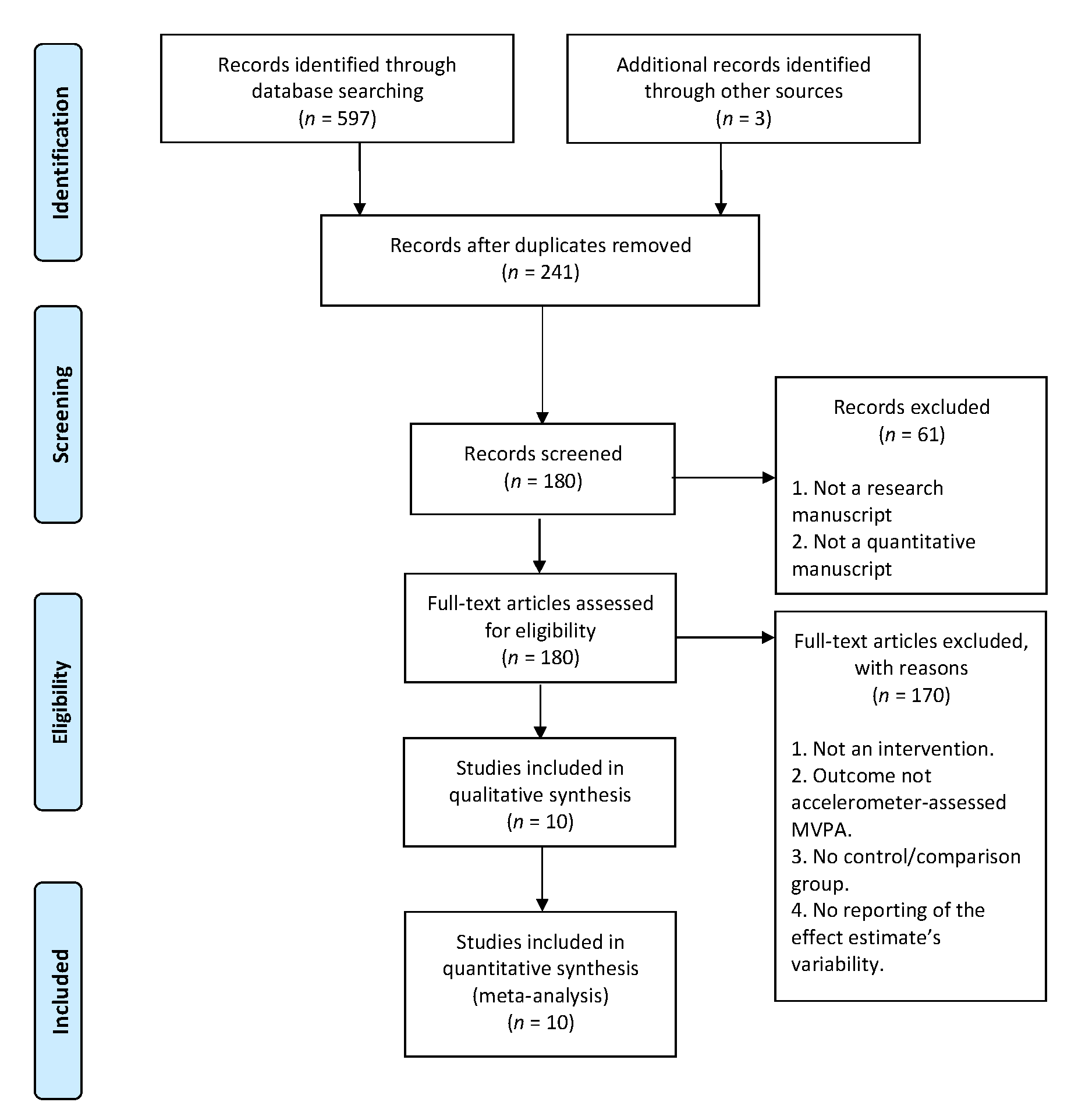
2.1. Study Selection
2.2. Physical Activity Assessment
2.3. Standardized Mean Differences
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Intervention Characteristics
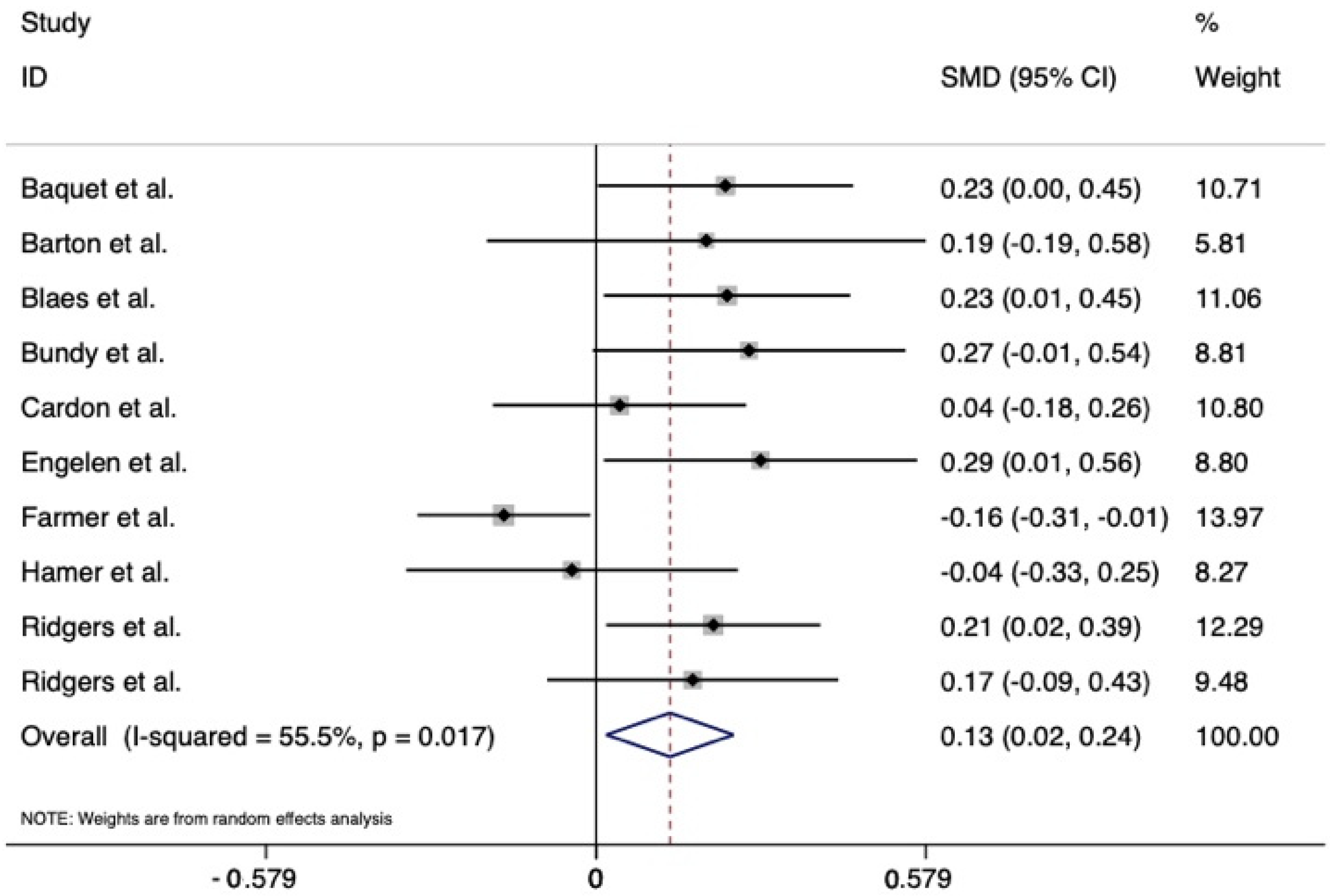
3.3. Meta-Analysis Findings
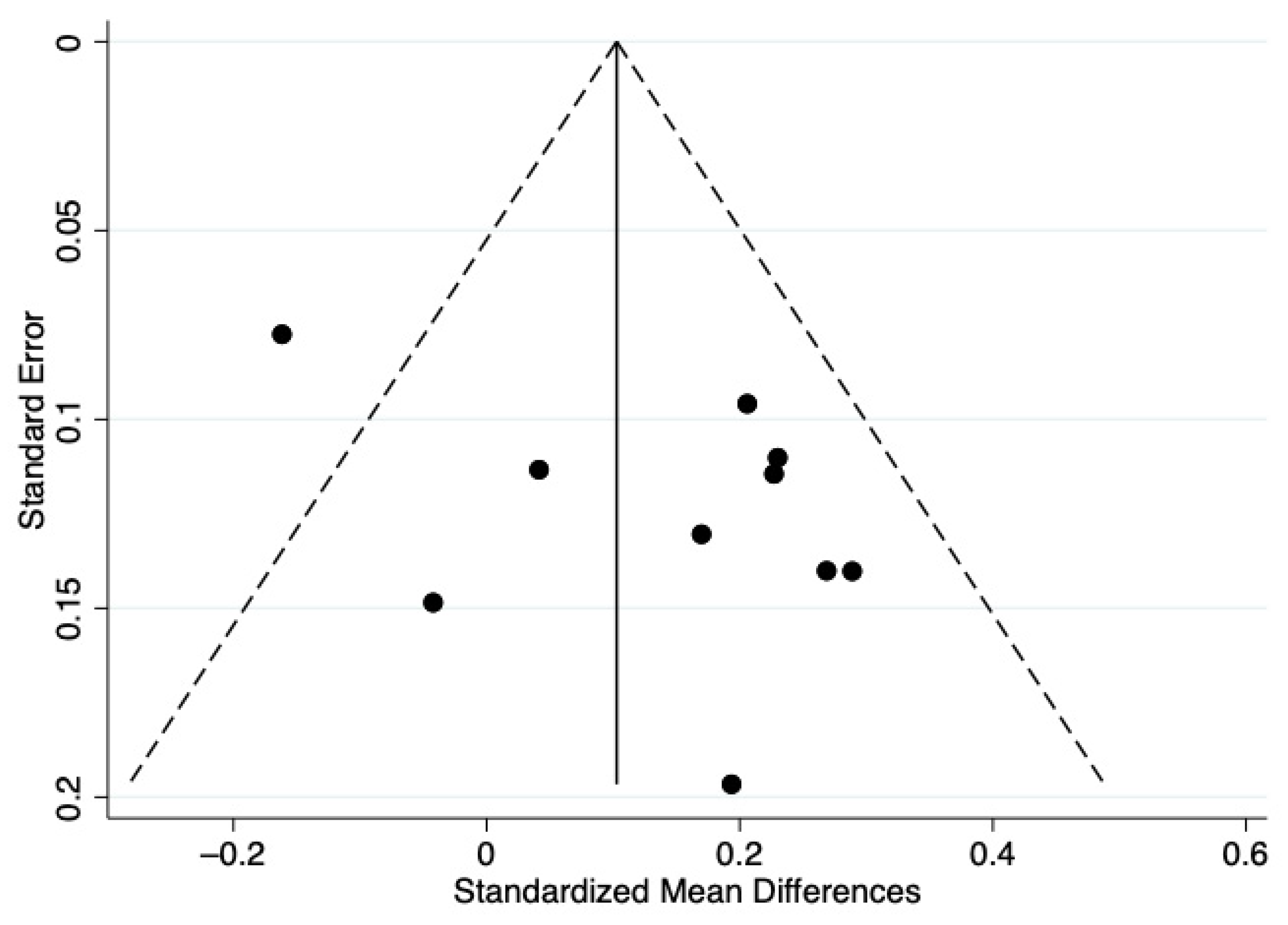
3.4. Results of Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rey, O.; Vallier, J.M.; Nicol, C.; Mercier, C.S.; Maïano, C. Effects of combined vigorous interval training program and diet on body composition, physical fitness, and physical self-perceptions among obese adolescent boys and girls. Pediatr. Exerc. Sci. 2017, 29, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Kantomaa, M.T.; Stamatakis, E.; Kankaanpää, A.; Kajantie, E.; Taanila, A.; Tammelin, T. Associations of physical activity and sedentary behavior with adolescent academic achievement. J. Res. Adolesc. 2016, 26, 432–442. [Google Scholar] [CrossRef]
- McMahon, E.M.; Corcoran, P.; O’Regan, G.; Keeley, H.; Cannon, M.; Carli, V.; Wasserman, D. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur. Child Adolesc. Psychiatry 2017, 26, 111–122. [Google Scholar] [CrossRef] [PubMed]
- British Heart Foundation. The National Audit of Cardiac Rehabilitation: Annual Statistical Report; British Heart Foundation: London, UK, 2015. [Google Scholar]
- National Physical Activity Plan Alliance. The 2018 United States Report Card on Physical Activity for Children and Youth; National Physical Activity Plan Alliance: Washington, DC, USA, 2018. [Google Scholar]
- Frost, M.C.; Kuo, E.S.; Harner, L.T.; Landau, K.R.; Baldassar, K. Increase in physical activity sustained 1 year after playground intervention. Am. J. Prev. Med. 2018, 54, S124–S129. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. School health guidelines to promote healthy eating and physical activity. Recomm. Rep. MMWR 2011, 60, 1. [Google Scholar]
- Koohsari, M.J.; Mavoa, S.; Villanueva, K.; Sugiyama, T.; Badland, H.; Kaczynski, A.T.; Giles-Corti, B. Public open space, physical activity, urban design and public health: Concepts, methods and research agenda. Health Place 2015, 33, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broekhuizen, K.; Scholten, A.M.; de Vries, S.I. The value of (pre) school playgrounds for children’s physical activity level: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, R.M.; Pellegrini, A.D.; Schmidt, S.L. The effects of different recess timing regimens on preschoolers’ classroom attention. Early Child Dev. Care 2006, 176, 735–743. [Google Scholar] [CrossRef]
- Bundy, A.C.; Luckett, T.; Naughton, G.A.; Tranter, P.J.; Wyver, S.R.; Ragen, J.; Spies, G. Playful interaction: Occupational therapy for all children on the school playground. Am. J. Occup. Ther. 2008, 62, 522–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santillan, L.; Frederick, L.; Gilmore, S.; Locke, J. Brief report: Examining the association between classroom social network inclusion and playground peer engagement among children with autism spectrum disorders. Focus Autism Other Dev. Disabil. 2019, 34, 91–96. [Google Scholar] [CrossRef]
- Anderson, D.H.; Trinh, S.M.; Caldarella, P.; Hansen, B.D.; Richardson, M.J. Increasing positive playground interaction for kindergarten students at risk for emotional and behavioral disorders. Early Child Educ. J. 2018, 46, 487–496. [Google Scholar] [CrossRef]
- Bagot, K.L.; Allen, F.C.L.; Toukhsati, S. Perceived restorativeness of children’s school playground environments: Nature, playground features and play period experiences. J. Environ. Psychol. 2015, 41, 1–9. [Google Scholar] [CrossRef]
- Reilly, J.J.; Penpraze, V.; Hislop, J.; Davies, G.; Grant, S.; Paton, J.Y. Objective measurement of physical activity and sedentary behaviour: Review with new data. Arch. Dis. Child. 2008, 93, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Riddoch, C.J.; Mattocks, C.; Deere, K.; Saunders, J.; Kirkby, J.; Tilling, K.; Ness, A.R. Objective measurement of levels and patterns of physical activity. Arch. Dis. Child. 2007, 92, 963–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hnatiuk, J.; Ridgers, N.D.; Salmon, J.; Campbell, K.; McCallum, Z.; Hesketh, K. Physical activity levels and patterns of 19-month-old children. Med. Sci. Sports Exerc. 2012, 44, 1715–1720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliver, M.; Schofield, G.M.; Schluter, P.J. Parent influences on preschoolers’ objectively assessed physical activity. J. Sci. Med. Sport 2020, 13, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Escalante, Y.; García-Hermoso, A.; Backx, K.; Saavedra, J.M. Playground designs to increase physical activity levels during school recess: A systematic review. Health Educ. Behav. 2014, 41, 138–144. [Google Scholar] [CrossRef]
- Erwin, H.E.; Ickes, M.; Ahn, S.; Fedewa, A. Impact of recess interventions on children’s physical activity: A meta-analysis. Am. J. Health Promot. 2014, 28, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Ickes, M.J.; Erwin, H.; Beighle, A. Systematic review of recess interventions to increase physical activity. J. Phys. Act. Health 2013, 10, 910–926. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutrit. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Hillsdale, N.J., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baquet, G.; Aucouturier, J.; Gamelin, F.X.; Berthoin, S. Longitudinal follow-up of physical activity during school recess: Impact of playground markings. Front. Public Health 2018, 6, 283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, J.; Sandercock, G.; Pretty, J.; Wood, C. The effect of playground- and nature-based playtime interventions on physical activity and self-esteem in UK school children. Int. J. Environ. Res. Public Health 2015, 25, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Blaes, A.; Ridgers, N.D.; Aucouturier, J.; Van Praagh, E.; Berthoin, S.; Baquet, G. Effects of a playground marking intervention on school recess physical activity in French children. Prev. Med. 2013, 57, 580–584. [Google Scholar] [CrossRef]
- Bundy, A.C.; Engelen, L.; Wyver, S.; Tranter, P.; Ragen, J.; Bauman, A.; Naughton, G. Sydney Playground Project: A cluster-randomized trial to increase physical activity, play, and social skills. J. Sch. Health 2017, 87, 751–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardon, G.; Labarque, V.; Smits, D.; De Bourdeaudhuij, I. Promoting physical activity at the pre-school playground: The effects of providing markings and play equipment. Prev. Med. 2009, 48, 335–340. [Google Scholar] [CrossRef]
- Engelen, L.; Bundy, A.C.; Naughton, G.; Simpson, J.M.; Bauman, A.; Ragan, J.; van der Ploeg, H.P. Increasing physical activity in young primary school children–it’s child’s play: A cluster randomized controlled trial. Prev. Med. 2013, 56, 319–325. [Google Scholar] [CrossRef]
- Farmer, V.L.; Williams, S.M.; Mann, J.I.; Schofield, G.; McPhee, J.C.; Taylor, R.W. The effect of increasing risk and challenge in the school playground on physical activity and weight in children: A cluster randomized controlled trial (PLAY). Int. J. Obes. 2017, 41, 793–800. [Google Scholar] [CrossRef]
- Hamer, M.; Aggio, D.; Knock, G.; Kipps, C.; Shankar, A.; Smith, L. Effect of major school playground reconstruction on physical activity and sedentary behavior: Camden active spaces. BMC Public Health 2017, 17, 552. [Google Scholar] [CrossRef] [Green Version]
- Ridgers, N.D.; Stratton, G.; Fairclough, S.J.; Twisk, J.W.R. Long-term effects of a playground markings and physical structures on children’s recess physical activity levels. Prev. Med. 2007, 44, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Fairclough, S.J.; Stratton, G. Twelve-month effects of a playground intervention on children’s morning and lunchtime recess physical activity levels. J. Phys. Act. Health 2010, 7, 167–175. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Burns, R.D.; Fu, Y.; Podlog, L.W. School-based physical activity interventions and physical activity enjoyment: A meta-analysis. Prev. Med. 2017, 103, 84–90. [Google Scholar] [CrossRef]
- Dishman, R.K.; Motl, R.W.; Saunders, R.; Felton, G.; Ward, D.S.; Dowda, M.; Pate, R.R. Enjoyment mediates effects of a school-based physical activity intervention. Med. Sci. Sports Exerc. 2005, 37, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Atkin, A.J.; Sharp, S.J.; Harrison, F.; Brage, S.; Van Sluijs, E.M. Seasonal Variation in Children’s Physical Activity and Sedentary Time. Med. Sci. Sports Exerc. 2016, 48, 449–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remmers, T.; Thijs, C.; Timperio, A.; Salmon, J.O.; Veitch, J.; Kremers, S.P.J.; Ridgers, N.D. Daily weather and children’s physical activity patterns. Med. Sci. Sports Exerc. 2017, 49, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Stratton, G.; Mullan, E. The effect of multicolor playground markings on children’s physical activity level during recess. Prev. Med. 2005, 41, 828–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boreham, C.; Riddoch, C. The physical activity, fitness, and health of children. J. Sports Sci. 2001, 19, 915–919. [Google Scholar] [CrossRef] [PubMed]
- Strong, W.B.; Malina, R.M.; Blimkie, C.J.; Daniels, S.R.; Dishman, R.K.; Gutin, B.; Trudeau, F. Evidence based physical activity for school-age youth. J. Pediatr. 2005, 146, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Trudeau, F.; Shephard, R.J. Physical education, school physical activity, school sports and academic performance. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 10. [Google Scholar] [CrossRef] [Green Version]
- Larouche, R.; Garriguet, D.; Tremblay, M.S. Outdoor time, physical activity and sedentary time among young children: The 2012–2013 Canadian Health Measures Survey. Can. J. Public Health 2017, 107, e500–e506. [Google Scholar] [CrossRef] [Green Version]
- Brusseau, T.A.; Burns, R.D. Introduction to multicomponent school-based physical activity programs. In The Routledge Handbook of Youth Physical Activity; Brusseau, T.A., Fairclough, S., Lubans, D., Eds.; Routledge: London, UK, 2020; pp. 557–576. [Google Scholar]
- Carson, R.; Webster, C.A. Comprehensive School Physical Activity Programs: Putting Evidence-Based Research into Practice; Human Kinetics Publishers: Champaign, IL, USA, 2019. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Study | Country | Age (years) (Mean ± SD) | n | Setting | Design | Duration | Accelerometer Processing | Other Outcomes |
|---|---|---|---|---|---|---|---|---|
| Baquet et al. [26] | France | IG: 8.3 ± 1.2 CG: 8.1 ± 1.8 | 283 | 3 Elementary schools | Playground markings; sporting playground zonal design | 12 months | GT1 M ActiGraph Epoch set at 2 s Trost et al. cutpoints | BMI LPA SB |
| Barton et al. [27] | United Kingdom | 8.8 ± 0.5 | 52 | 2 Primary schools | Small equipment; free play | 5 days sports 5 days orienteering | GT1 M ActiGraph Epoch set at 1 s Treuth et al. cutpoints | Self-esteem |
| Blaes et al. [28] | France | IG: 8.7 ± 1.5 CG: 8.9 ± 1.6 | 332 | 4 Primary schools | Playground markings; sporting playground zonal design | 4-day school week in April and May | GT1 M ActiGraph Epoch set at 2 s Trost et al. cutpoints | LPA SB |
| Bundy et al. [29] | Australia | 6.0 ± 0.6 | 206 | 12 Primary schools | Recycled materials with no obvious play use; teacher/parent reframing workshop | 13 weeks | GT3 X ActiGraph Epoch set at 5 s Evenson et al. cutpoints | Acceptance Self-competence SB Social interactions Social skills |
| Cardon et al. [30] | Belgium | 5.3 ± 0.4 | 583 | 40 Pre-schools | Play equipment; playground markings | 4–6 weeks | GT1 M ActiGraph Epoch set at 15 s Sirard et al. cutpoints | LPA SB |
| Engelen et al. [31] | Australia | 6.0 ± 0.6 | 221 | 12 Primary schools | Recycled materials with no obvious play use; teacher-parent workshop | 13 weeks | GT3 X ActiGraph Epoch set at 15 s Evenson et al. cutpoints | LPA SB |
| Farmer et al. [32] | New Zealand | IG: 7.9 ± 1.1 EG: 8.0 ± 1.2 | 840 | 16 Primary schools | Playground action plans | 2 years | GT3 X ActiGraph Epoch set at 15 s Evenson et al. cutpoints | BMI BMI z-score Total PA Waist circumference Waist-to-height ratio |
| Hamer et al. [33] | United Kingdom | 8.0 | 231 | 5 Primary schools 2 Secondary schools | Novel playground design based on emerging themes consultation | 1 year | GT3 X ActiGraph Epoch set at 60 s Self-determined cutpoints (MVPA > 3000 cpm) | LPA SB |
| Ridgers et al. [34] | United Kingdom | IG: 8.3 ± 1.8 yrs CG: 8.0 ± 1.5 yrs | 298 | 15 Primary schools | Sporting playground zonal design; novel structures; small equipment | 6 weeks | Model 7164 ActiGraph Epoch set at 5 s Nilsson et al. cutpoints | HR-assessed MVPA VPA |
| Ridgers et al. [35] | United Kingdom | IG: 8.3 ± 1.8 CG: 8.0 ± 1.4 | 434 | 26 Elementary Schools | Playground markings; sporting playground zonal design; novel structures | 1 year | Model 7164 ActiGraph Epoch set at 5 s Nilsson et al. cutpoints | HR-assessed MVPA HR-assessed VPA |
| Study Omitted | Adjusted Pooled SMD | Adjusted 95% CI |
|---|---|---|
| Baquet et al. [26] | 0.12 | 0.00–0.23 |
| Barton et al. [27] | 0.12 | 0.01–0.25 |
| Blaes et al. [28] | 0.12 | 0.00–0.25 |
| Bundy et al. [29] | 0.12 | 0.00–0.24 |
| Cardon et al. [30] | 0.14 | 0.02–0.27 |
| Engelen et al. [31] | 0.11 | 0.00–0.22 |
| Farmer et al. [32] | 0.18 | 0.10–0.26 |
| Hamer et al. [33] | 0.14 | 0.03–0.25 |
| Ridgers et al. [34] | 0.12 | 0.00–0.25 |
| Ridgers et al. [35] | 0.13 | 0.01–0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pfledderer, C.D.; Kwon, S.; Strehli, I.; Byun, W.; Burns, R.D. The Effects of Playground Interventions on Accelerometer-Assessed Physical Activity in Pediatric Populations: A Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 3445. https://doi.org/10.3390/ijerph19063445
Pfledderer CD, Kwon S, Strehli I, Byun W, Burns RD. The Effects of Playground Interventions on Accelerometer-Assessed Physical Activity in Pediatric Populations: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(6):3445. https://doi.org/10.3390/ijerph19063445
Chicago/Turabian StylePfledderer, Christopher D., Sunku Kwon, Ildiko Strehli, Wonwoo Byun, and Ryan D. Burns. 2022. "The Effects of Playground Interventions on Accelerometer-Assessed Physical Activity in Pediatric Populations: A Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 6: 3445. https://doi.org/10.3390/ijerph19063445