
Efficacy of MMP-8 Level in Gingival Crevicular Fluid to Predict the Outcome of Nonsurgical Periodontal Treatment: A Systematic Review

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and the Focused Question
2.2. Search Strategy and Eligibility Criteria
- Original studies (randomized and controlled clinical trials (RCT and CCT)) published in the English language.
- Monitoring periodontal treatment prognosis using concentration of whole MMP-8 (not activate MMP-8) at baseline.
- Subjects were healthy with no systemic illness.
- Non-smoker subjects suffering from periodontitis.
- Treated with NSPT (manual, ultrasonic, or both).
- Minimum follow-up duration of three months for clinical indicators and GCF MMP-8 level.
- One of the arms of the study to involve NSPT (manual or ultrasonic or both) only.
- No history of periodontal treatment in the past three months.
- Case series, case reports, experimental or animal studies, observational studies, and review papers.
- Studies reporting pooled GCF MMP-8 of smokers and non-smokers as one group.
- Use of antibiotics or host modulation therapy (such as doxycycline) in the last three months.
- Pregnant or lactating women and patients on steroid or immunosuppressive therapy.
- Follow-up period of less than three months.
2.3. Literature Screening and Data Extraction
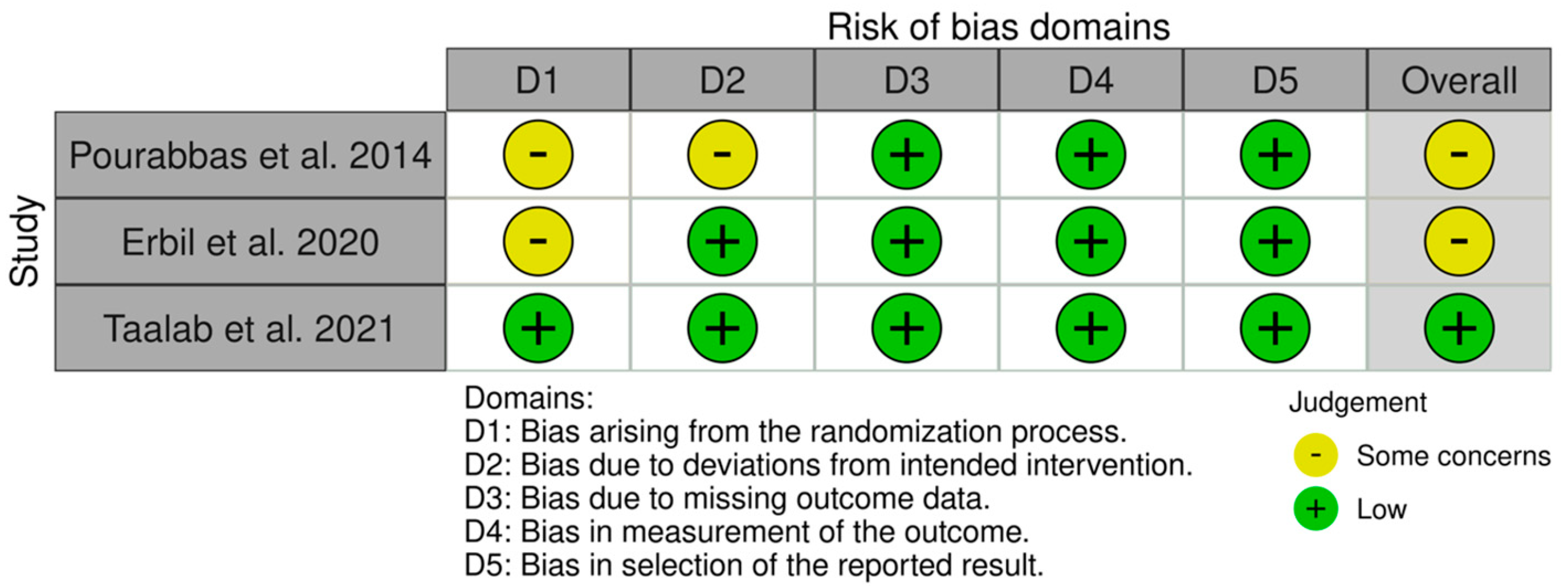
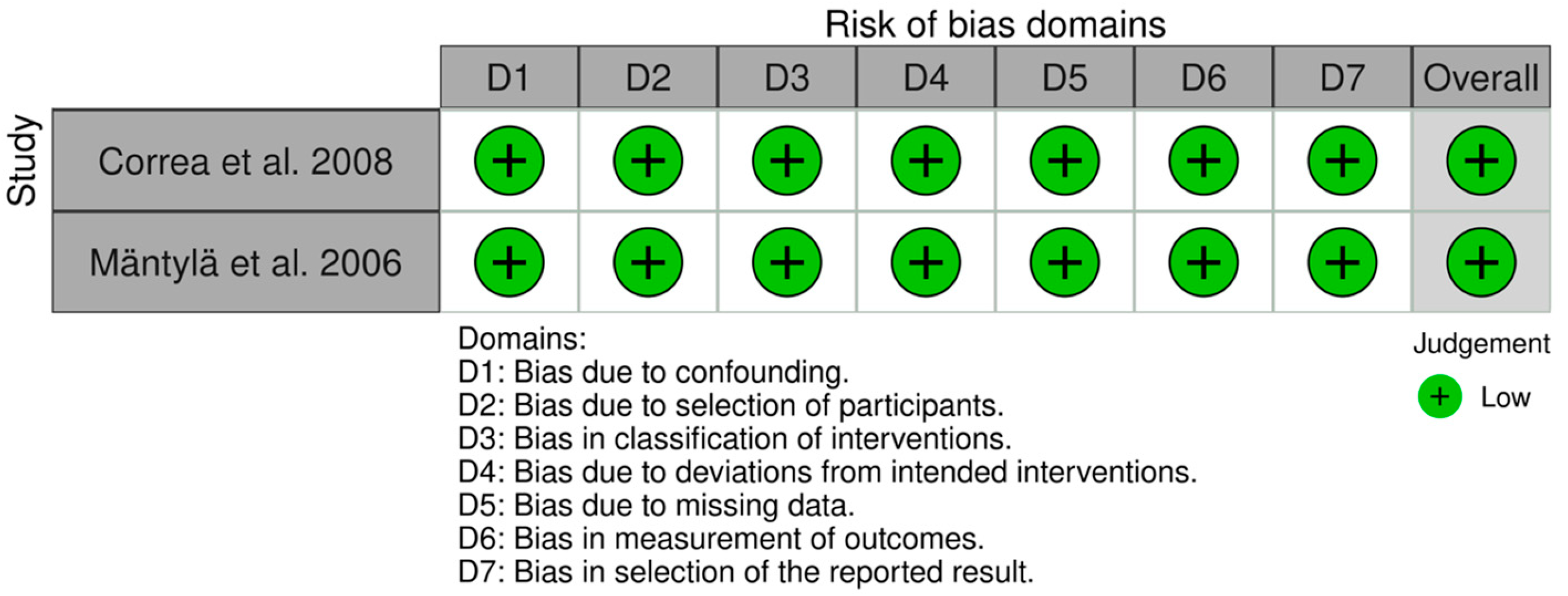
2.4. Quality Appraisal
3. Results
3.1. Selection of Studies
3.2. Study Design and Populations
3.3. Follow-Up Periods
3.4. GCF Collection, Elution, and Storage Methods
3.5. Biochemical Assays and Concentration of GCF MMP-8
3.6. Measurement of PPD and Case Definition of Periodontitis
3.7. Changes in PPD
3.8. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hajishengallis, G.; Lamont, R.J. Beyond the red complex and into more complexity: The polymicrobial synergy and dysbiosis (PSD) model of periodontal disease etiology. Mol. Oral Microbiol. 2012, 27, 409–419. [Google Scholar] [CrossRef] [Green Version]
- Page, R.C. Critical issues in periodontal research. J. Dent. Res. 1995, 74, 1118–1128. [Google Scholar] [CrossRef] [PubMed]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions-Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Joss, A.; Orsanic, T.; Gusberti, F.A.; Siegrist, B.E. Bleeding on probing. A predictor for the progression of periodontal disease? J. Clin. Periodontol. 1986, 13, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Gul, S.S.; Abdulkareem, A.A.; Sha, A.M.; Rawlinson, A. Diagnostic Accuracy of Oral Fluids Biomarker Profile to Determine the Current and Future Status of Periodontal and Peri-Implant Diseases. Diagnostics 2020, 10, 838. [Google Scholar] [CrossRef] [PubMed]
- Ansai, T.; Awano, S.; Soh, I. Problems and future approaches for assessment of periodontal disease. Front. Public Health 2014, 2, 54. [Google Scholar] [CrossRef]
- Baelum, V.; López, R. Defining and predicting outcomes of non-surgical periodontal treatment: A 1-yr follow-up study. Eur. J. Oral Sci. 2016, 124, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque-induced gingivitis: Case definition and diagnostic considerations. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S44–S67. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. S1), S159–S172. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.; Khalid, T.; Bettiol, S.; Crocombe, L.A. Non-surgical periodontal therapy effectively improves patient-reported outcomes: A systematic review. Int. J. Dent. Hyg. 2021, 19, 18–28. [Google Scholar] [CrossRef]
- Gul, S.S.; Douglas, C.W.; Griffiths, G.S.; Rawlinson, A. A pilot study of active enzyme levels in gingival crevicular fluid of patients with chronic periodontal disease. J. Clin. Periodontol. 2016, 43, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Gul, S.S.; Griffiths, G.S.; Stafford, G.P.; Al-Zubidi, M.I.; Rawlinson, A.; Douglas, C.W.I. Investigation of a Novel Predictive Biomarker Profile for the Outcome of Periodontal Treatment. J. Periodontol. 2017, 88, 1135–1144. [Google Scholar] [CrossRef]
- Saglie, F.R.; Marfany, A.; Camargo, P. Intragingival occurrence of Actinobacillus actinomycetemcomitans and Bacteroides gingivalis in active destructive periodontal lesions. J. Periodontol. 1988, 59, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, G.S.; Ayob, R.; Guerrero, A.; Nibali, L.; Suvan, J.; Moles, D.R.; Tonetti, M.S. Amoxicillin and metronidazole as an adjunctive treatment in generalized aggressive periodontitis at initial therapy or re-treatment: A randomized controlled clinical trial. J. Clin. Periodontol. 2011, 38, 43–49. [Google Scholar] [CrossRef]
- Graziani, F.; Karapetsa, D.; Mardas, N.; Leow, N.; Donos, N. Surgical treatment of the residual periodontal pocket. Periodontology 2000 2018, 76, 150–163. [Google Scholar] [CrossRef] [Green Version]
- Fatima, T.; Khurshid, Z.; Rehman, A.; Imran, E.; Srivastava, K.C.; Shrivastava, D. Gingival Crevicular Fluid (GCF): A Diagnostic Tool for the Detection of Periodontal Health and Diseases. Molecules 2021, 26, 1208. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, Z.; Mali, M.; Naseem, M.; Najeeb, S.; Zafar, M.S. Human Gingival Crevicular Fluids (GCF) Proteomics: An Overview. Dent. J. 2017, 5, 12. [Google Scholar] [CrossRef]
- Qasim, S.S.B.; Al-Otaibi, D.; Al-Jasser, R.; Gul, S.S.; Zafar, M.S. An Evidence-Based Update on the Molecular Mechanisms Underlying Periodontal Diseases. Int. J. Mol. Sci. 2020, 21, 3829. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Alassiri, S.; Grigoriadis, A.; Räisänen, I.T.; Pärnänen, P.; Nwhator, S.O.; Gieselmann, D.R.; Sakellari, D. Active MMP-8 (aMMP-8) as a Grading and Staging Biomarker in the Periodontitis Classification. Diagnostics 2020, 10, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorsa, T.; Gursoy, U.K.; Nwhator, S.; Hernandez, M.; Tervahartiala, T.; Leppilahti, J.; Gursoy, M.; Könönen, E.; Emingil, G.; Pussinen, P.J.; et al. Analysis of matrix metalloproteinases, especially MMP-8, in gingival creviclular fluid, mouthrinse and saliva for monitoring periodontal diseases. Periodontology 2000 2016, 70, 142–163. [Google Scholar] [CrossRef] [PubMed]
- De Morais, E.F.; Pinheiro, J.C.; Leite, R.B.; Santos, P.P.A.; Barboza, C.A.G.; Freitas, R.A. Matrix metalloproteinase-8 levels in periodontal disease patients: A systematic review. J. Periodontal Res. 2018, 53, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Chhina, S.; Arora, S.A. A systematic review of biomarkers of gingival crevicular fluid: Their predictive role in diagnosis of periodontal disease status. J. Oral Biol. Craniofacial Res. 2018, 8, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ (Clin. Res. Ed.) 2021, 372, n71. [Google Scholar] [CrossRef]
- Cobb, C.M. Non-surgical pocket therapy: Mechanical. Ann. Periodontol. 1996, 1, 443–490. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ (Clin. Res. Ed.) 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ (Clin. Res. Ed.) 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Mäntylä, P.; Stenman, M.; Kinane, D.; Salo, T.; Suomalainen, K.; Tikanoja, S.; Sorsa, T. Monitoring periodontal disease status in smokers and nonsmokers using a gingival crevicular fluid matrix metalloproteinase-8-specific chair-side test. J. Periodontal Res. 2006, 41, 503–512. [Google Scholar] [CrossRef]
- Correa, F.O.; Gonçalves, D.; Figueredo, C.M.; Gustafsson, A.; Orrico, S.R. The short-term effectiveness of non-surgical treatment in reducing levels of interleukin-1beta and proteases in gingival crevicular fluid from patients with type 2 diabetes mellitus and chronic periodontitis. J. Periodontol. 2008, 79, 2143–2150. [Google Scholar] [CrossRef]
- Pourabbas, R.; Kashefimehr, A.; Rahmanpour, N.; Babaloo, Z.; Kishen, A.; Tenenbaum, H.C.; Azarpazhooh, A. Effects of photodynamic therapy on clinical and gingival crevicular fluid inflammatory biomarkers in chronic periodontitis: A split-mouth randomized clinical trial. J. Periodontol. 2014, 85, 1222–1229. [Google Scholar] [CrossRef] [PubMed]
- Erbil, D.; Nazaroglu, K.; Baser, U.; İssever, H.; Mese, S.; İsik, A.G. Clinical and Immunological Effects of Er, Cr:YSGG Laser in Nonsurgical Periodontal Treatment: A Randomized Clinical Trial. Photobiomodul. Photomed. Laser Surg. 2020, 38, 316–322. [Google Scholar] [CrossRef]
- Taalab, M.R.; Mahmoud, S.A.; Moslemany, R.M.E.; Abdelaziz, D.M. Intrapocket application of tea tree oil gel in the treatment of stage 2 periodontitis. BMC Oral Health 2021, 21, 239. [Google Scholar] [CrossRef] [PubMed]
- Eltas, A.; Orbak, R. Effect of 1064-nm Nd:YAG laser therapy on GCF IL-1β and MMP-8 levels in patients with chronic periodontitis. Lasers Med. Sci. 2012, 27, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Azmak, N.; Atilla, G.; Luoto, H.; Sorsa, T. The effect of subgingival controlled-release delivery of chlorhexidine chip on clinical parameters and matrix metalloproteinase-8 levels in gingival crevicular fluid. J. Periodontol. 2002, 73, 608–615. [Google Scholar] [CrossRef]
- Emingil, G.; Han, B.; Gürkan, A.; Berdeli, A.; Tervahartiala, T.; Salo, T.; Pussinen, P.J.; Köse, T.; Atilla, G.; Sorsa, T. Matrix metalloproteinase (MMP)-8 and tissue inhibitor of MMP-1 (TIMP-1) gene polymorphisms in generalized aggressive periodontitis: Gingival crevicular fluid MMP-8 and TIMP-1 levels and outcome of periodontal therapy. J. Periodontol. 2014, 85, 1070–1080. [Google Scholar] [CrossRef]
- Cosgarea, R.; Eick, S.; Jepsen, S.; Arweiler, N.B.; Juncar, R.; Tristiu, R.; Salvi, G.E.; Heumann, C.; Sculean, A. Microbiological and host-derived biomarker evaluation following non-surgical periodontal therapy with short-term administration of systemic antimicrobials: Secondary outcomes of an RCT. Sci. Rep. 2020, 10, 16322. [Google Scholar] [CrossRef]
- Emingil, G.; Han, B.; Ozdemir, G.; Tervahartiala, T.; Vural, C.; Atilla, G.; Baylas, H.; Sorsa, T. Effect of azithromycin, as an adjunct to nonsurgical periodontal treatment, on microbiological parameters and gingival crevicular fluid biomarkers in generalized aggressive periodontitis. J. Periodontal Res. 2012, 47, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Marcaccini, A.M.; Meschiari, C.A.; Zuardi, L.R.; de Sousa, T.S.; Taba, M., Jr.; Teofilo, J.M.; Jacob-Ferreira, A.L.; Tanus-Santos, J.E.; Novaes, A.B., Jr.; Gerlach, R.F. Gingival crevicular fluid levels of MMP-8, MMP-9, TIMP-2, and MPO decrease after periodontal therapy. J. Clin. Periodontol. 2010, 37, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- Basegmez, C.; Berber, L.; Yalcin, F. Clinical and biochemical efficacy of minocycline in nonsurgical periodontal therapy: A randomized controlled pilot study. J. Clin. Pharmacol. 2011, 51, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.; Vázquez-Villegas, P.; Rito-Palomares, M.; Martinez-Chapa, S.O. Advantages, Disadvantages and Modifications of Conventional ELISA. In Enzyme-Linked Immunosorbent Assay (ELISA): From A to Z; Hosseini, S., Vázquez-Villegas, P., Rito-Palomares, M., Martinez-Chapa, S.O., Eds.; Springer: Singapore, 2018; pp. 67–115. [Google Scholar] [CrossRef]
- Zhu, L.; Leinonen, J.; Zhang, W.M.; Finne, P.; Stenman, U.H. Dual-label immunoassay for simultaneous measurement of prostate-specific antigen (PSA)-alpha1-antichymotrypsin complex together with free or total PSA. Clin. Chem. 2003, 49, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheng, S.L.; Bao, S.H.; Huang, G.; Wang, L.M. Development of time-resolved immunofluorometric assays for vascular endothelial growth factor and application on plasma of patients with gastric tumours. Clin. Exp. Immunol. 2008, 151, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Elshal, M.F.; McCoy, J.P. Multiplex bead array assays: Performance evaluation and comparison of sensitivity to ELISA. Methods 2006, 38, 317–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorat, A.A.; Suryanarayanan, R. Characterization of Phosphate Buffered Saline (PBS) in Frozen State and after Freeze-Drying. Pharm. Res. 2019, 36, 98. [Google Scholar] [CrossRef] [PubMed]
- Pikal-Cleland, K.A.; Rodríguez-Hornedo, N.; Amidon, G.L.; Carpenter, J.F. Protein denaturation during freezing and thawing in phosphate buffer systems: Monomeric and tetrameric beta-galactosidase. Arch. Biochem. Biophys. 2000, 384, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Kolhe, P.; Amend, E.; Singh, S.K. Impact of freezing on pH of buffered solutions and consequences for monoclonal antibody aggregation. Biotechnol. Prog. 2010, 26, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Sieracki, N.A.; Hwang, H.J.; Lee, M.K.; Garner, D.K.; Lu, Y. A temperature independent pH (TIP) buffer for biomedical biophysical applications at low temperatures. Chem. Commun. 2008, 7, 823–825. [Google Scholar] [CrossRef] [PubMed]
- Sulik, A.; Wojtkowska, M.; Oldak, E. Preanalytical factors affecting the stability of matrix metalloproteinase-2 concentrations in cerebrospinal fluid. Clin. Chim. Acta Int. J. Clin. Chem. 2008, 392, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Kisand, K.; Kerna, I.; Kumm, J.; Jonsson, H.; Tamm, A. Impact of cryopreservation on serum concentration of matrix metalloproteinases (MMP)-7, TIMP-1, vascular growth factors (VEGF) and VEGF-R2 in Biobank samples. Clin. Chem. Lab. Med. 2011, 49, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Darby, I.B.; Said, S.; Luoto, H.; Sorsa, T.; Tikanoja, S.; Mäntylä, P. Changes in gingival crevicular fluid matrix metalloproteinase-8 levels during periodontal treatment and maintenance. J. Periodontal Res. 2003, 38, 400–404. [Google Scholar] [CrossRef]
- Kinney, J.S.; Morelli, T.; Oh, M.; Braun, T.M.; Ramseier, C.A.; Sugai, J.V.; Giannobile, W.V. Crevicular fluid biomarkers and periodontal disease progression. J. Clin. Periodontol. 2014, 41, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Choi, D.H.; Moon, I.S.; Choi, B.K.; Paik, J.W.; Kim, Y.S.; Choi, S.H.; Kim, C.K. Effects of sub-antimicrobial dose doxycycline therapy on crevicular fluid MMP-8, and gingival tissue MMP-9, TIMP-1 and IL-6 levels in chronic periodontitis. J. Periodontal Res. 2004, 39, 20–26. [Google Scholar] [CrossRef]
- Skurska, A.; Dolinska, E.; Pietruska, M.; Pietruski, J.K.; Dymicka, V.; Kemona, H.; Arweiler, N.B.; Milewsk, R.; Sculean, A. Effect of nonsurgical periodontal treatment in conjunction with either systemic administration of amoxicillin and metronidazole or additional photodynamic therapy on the concentration of matrix metalloproteinases 8 and 9 in gingival crevicular fluid in patients with aggressive periodontitis. BMC Oral Health 2015, 15, 63. [Google Scholar]
- Nardi, G.M.; Cesarano, F.; Papa, G.; Chiavistelli, L.; Ardan, R.; Jedlinski, M.; Mazur, M.; Grassi, R.; Grassi, F.R. Evaluation of Salivary Matrix Metalloproteinase (MMP-8) in Periodontal Patients Undergoing Non-Surgical Periodontal Therapy and Mouthwash Based on Ozonated Olive Oil: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 6619. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Duan, D.; Ma, R.; Ding, Y.; Xu, Y.; Zhou, X.; Zhao, L.; Xu, X. The combined use of salivary biomarkers and clinical parameters to predict the outcome of scaling and root planing: A cohort study. J. Clin. Periodontol. 2020, 47, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Buduneli, N.; Vardar, S.; Atilla, G.; Sorsa, T.; Luoto, H.; Baylas, H. Gingival crevicular fluid matrix metalloproteinase-8 levels following adjunctive use of meloxicam and initial phase of periodontal therapy. J. Periodontol. 2002, 73, 103–109. [Google Scholar] [CrossRef]
- Farhad, S.Z.; Aminzadeh, A.; Mafi, M.; Barekatain, M.; Naghney, M.; Ghafari, M.R. The effect of adjunctive low-dose doxycycline and licorice therapy on gingival crevicular fluid matrix metalloproteinase-8 levels in chronic periodontitis. Dent. Res. J. (Isfahan) 2013, 10, 624–629. [Google Scholar]
- Kurtis, B.; Tüter, G.; Serdar, M.; Pinar, S.; Demirel, I.; Toyman, U. GCF MMP-8 levels in smokers and non-smokers with chronic periodontitis following scaling and root planing accompanied by systemic use of flurbiprofen. J. Periodontol. 2007, 78, 1954–1961. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Cox, S.W.; Eley, B.M.; Mäntylä, P.; Rönkä, H.; Sorsa, T. Matrix metalloproteinase-8 levels and elastase activities in gingival crevicular fluid from chronic adult periodontitis patients. J. Clin. Periodontol. 2000, 27, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Ozgören, O.; Develioglu, H.; Güncü, G.; Akman, A.; Berker, E. The adjunctive effect of tenoxicam during non-surgical periodontal treatment on clinical parameters and gingival crevicular fluid levels of MMP-8 and TNF-α in patients with chronic periodontitis—Randomized, double-blind clinical trial. Adv. Clin. Exp. Med. 2014, 23, 559–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tüter, G.; Serdar, M.; Kurtiş, B.; Walker, S.G.; Atak, A.; Toyman, U.; Pinar, S.; Aykan, T. Effects of scaling and root planing and subantimicrobial dose doxycycline on gingival crevicular fluid levels of matrix metalloproteinase-8, -13 and serum levels of HsCRP in patients with chronic periodontitis. J. Periodontol. 2010, 81, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Jentsch, H.F.; Buchmann, A.; Friedrich, A.; Eick, S. Nonsurgical therapy of chronic periodontitis with adjunctive systemic azithromycin or amoxicillin/metronidazole. Clin. Oral Investig. 2016, 20, 1765–1773. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, P.F.; Huang, H.; Mcaninley, S.; Alfant, B.; Harrison, P.; Aukhil, I.; Walker, C.; Shaddox, L.M. Periodontal treatment reduces matrix metalloproteinase levels in localized aggressive periodontitis. J. Periodontol. 2013, 84, 1801–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppilahti, J.M.; Sorsa, T.; Kallio, M.A.; Tervahartiala, T.; Emingil, G.; Han, B.; Mäntylä, P. The utility of gingival crevicular fluid matrix metalloproteinase-8 response patterns in prediction of site-level clinical treatment outcome. J. Periodontol. 2015, 86, 777–787. [Google Scholar] [CrossRef]
- De Oliveira, R.R.; Schwartz-Filho, H.O.; Novaes, A.B.; Garlet, G.P.; De Souza, R.F.; Taba, M.; Scombatti De Souza, S.L.; Ribeiro, F.J. Antimicrobial photodynamic therapy in the non-surgical treatment of aggressive periodontitis: Cytokine profile in gingival crevicular fluid, preliminary results. J. Periodontol. 2009, 80, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Holmlund, A.; Hänström, L.; Lerner, U.H. Bone resorbing activity and cytokine levels in gingival crevicular fluid before and after treatment of periodontal disease. J. Clin. Periodontol. 2004, 31, 475–482. [Google Scholar] [CrossRef]
- Emingil, G.; Atilla, G.; Sorsa, T.; Savolainen, P.; Baylas, H. Effectiveness of adjunctive low-dose doxycycline therapy on clinical parameters and gingival crevicular fluid laminin-5 gamma2 chain levels in chronic periodontitis. J. Periodontol. 2004, 75, 1387–1396. [Google Scholar] [CrossRef]
- Reddy, N.R.; Roopa, D.; Babu, D.S.; Kumar, P.M.; Raju, C.M.; Kumar, N.S. Estimation of matrix metalloproteinase-3 levels in gingival crevicular fluid in periodontal disease, health and after scaling and root planing. J. Indian Soc. Periodontol. 2012, 16, 549–552. [Google Scholar] [CrossRef]
- Koromantzos, P.A.; Makrilakis, K.; Dereka, X.; Offenbacher, S.; Katsilambros, N.; Vrotsos, I.A.; Madianos, P.N. Effect of non-surgical periodontal therapy on C-reactive protein, oxidative stress, and matrix metalloproteinase (MMP)-9 and MMP-2 levels in patients with type 2 diabetes: A randomized controlled study. J. Periodontol. 2012, 83, 3–10. [Google Scholar] [CrossRef]
- Okuda, K.; Miyazaki, A.; Momose, M.; Murata, M.; Nomura, T.; Kubota, T.; Wolff, L.F.; Yoshie, H. Levels of tissue inhibitor of metalloproteinases-1 and matrix metalloproteinases-1 and -8 in gingival crevicular fluid following treatment with enamel matrix derivative (EMDOGAIN). J. Periodontal Res. 2001, 36, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Górska, R.; Nedzi-Góra, M. The effects of the initial treatment phase and of adjunctive low-dose doxycycline therapy on clinical parameters and MMP-8, MMP-9, and TIMP-1 levels in the saliva and peripheral blood of patients with chronic periodontitis. Arch. Immunol. Exp. (Warsz) 2006, 54, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Ağan, S.; Sönmez, S.; Serdar, M. The effect of topical doxycycline usage on gingival crevicular fluid MMP-8 levels of chronic and aggressive periodontitis patients: A pilot study. Int. J. Dent. Hyg. 2006, 4, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Kurgan, Ş.; Fentoğlu, Ö.; Önder, C.; Serdar, M.; Eser, F.; Tatakis, D.N.; Günhan, M. The effects of periodontal therapy on gingival crevicular fluid matrix metalloproteinase-8, interleukin-6 and prostaglandin E2 levels in patients with rheumatoid arthritis. J. Periodontal Res. 2016, 51, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Leppilahti, J.M.; Kallio, M.A.; Tervahartiala, T.; Sorsa, T.; Mäntylä, P. Gingival crevicular fluid matrix metalloproteinase-8 levels predict treatment outcome among smokers with chronic periodontitis. J. Periodontol. 2014, 85, 250–260. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author, Year | Reason(s) for Exclusion | |
|---|---|---|
| 1 | Eltas, Orbak [33] | Smoking status was not determined |
| 2 | Azmak, Atilla, Luoto, Sorsa [34] | |
| 3 | Gul, Griffiths, Stafford, Al-Zubidi, Rawlinson, Douglas [12] | Data of smoker and non-smoker individuals were combined |
| 4 | Emingil, Han, Gürkan, Berdeli, Tervahartiala, Salo, Pussinen, Köse, Atilla, Sorsa [35] | |
| 5 | Cosgarea, Eick, Jepsen, Arweiler, Juncar, Tristiu, Salvi, Heumann, Sculean [34] | |
| 6 | Emingil, Han, Ozdemir, Tervahartiala, Vural, Atilla, Baylas, Sorsa [37] | |
| 7 | Marcaccini, Meschiari, Zuardi, de Sousa, Taba, Teofilo, Jacob-Ferreira, Tanus-Santos, Novaes, Gerlach [38] | Concentration of whole MMP-8 was not reported |
| Author, Year | Study Design | Sample Characteristics | Interventions/Follow-Up for GCF Collection | GCF Collection Method/MMP-8 Assays | Sample Elution/Storage | Baseline GCF MMP-8 (ng/mL) ǂ |
|---|---|---|---|---|---|---|
| Mäntylä et al., 2006 [28] | Prospective clinical trial with parallel-arm design | Periodontitis, patients Non-smoker (n = 5), smoker (n = 11) | Oral hygiene instructions and SD Ɨ GCF samples were collected bimonthly over 12 months | Filter paper # was placed into the gingival sulcus for 30 s Selected sites/teeth: NR MMP-8-specific periodontal chair side dipstick test and time-resolved IFMA | The strip was put in a test tube containing 0.5 mL of pH 7.4 HEPES-buffer. The proteins absorbed by the sample strip were then eluted for 5 min in the buffer. There was no storage used. | 3997 ± 3126 ¶ |
| Correa et al., 2008 [29] | Clinical trial with parallel-arm design | Control arm: systemically healthy with periodontitis (n = 26) Study: patients with type 2 diabetes mellitus and periodontitis (n = 23) | Oral hygiene instructions and supra- and SD via manual instruments Ɨ Samples from GCF were taken at baseline and after 3 months | GCF was collected from five or six deep sites (PD ≥ 5 mm, CAL ≥ 4 mm, and BOP) and five or six shallow sites (PD ≤ 3 mm, CAL ≤ 2 mm, and BOP) in separate non-adjacent teeth GCF was collected for 30 s with paper strips (PerioPaper: Oraflow, Inc., NY, USA) placed in sulcus until resistance was felt Concentrations were determined using an antibody pair and recombinant MMP-8, and the results were evaluated using a multiplex bead method | Each subject’s samples from the same site type (deep or shallow) were combined together in an Eppendorf tube containing 1 mL PBS. After 40 min of elution at room temperature, the samples were centrifuged for 10 min at 3000× g, and the supernatant was collected and promptly frozen at −70 °C. | 20.6 (11.5/32.3) § |
| Pourabbas et al., 2014 [30] | Split-mouth RCT | Chronic periodontitis patients (n = 22) One side assigned as a control and the other as a study side | SD only Ɨ GCF collection was done at the start of the study and 3 months afterwards | Sterile paper strips (PerioCol paper, Oraflow, NY, USA) were placed into the deepest portion of the periodontal pockets of all treated teeth and kept in place for 30 s The sandwich ELISA was used for GCF MMP-8 analysis | The strips were placed in sterile microtubes containing 250 µL PBS. The samples were kept at −70 °C after being left at 4 °C for up to 2 h. | 306.34 ± 255.97 ¶ |
| Erbil et al., 2020 [31] | Multi-center, parallel RCT | Patients with periodontitis Control (n = 29), study (n = 30) | SD only Ɨ The data were recorded at baseline, 6 weeks, and 3 months following the therapy | For sampling, the deepest pockets (maximum of 9 mm) of single-rooted teeth were chosen (4 sites/patient); for 30 s, paper strips (PerioPaper: Oraflow, Inc., NY, USA) were carefully placed into the pockets GCF MMP-8 concentration was determined by ELISA | Each patient’s pooled strips were put in sterile Eppendorf tubes and kept at −80 °C. | 331.50 ± 299.70 ¶ |
| Taalab et al., 2021 [32] | Parallel arm RCT | Patients with stage 2, grade B periodontitis Patients (n = 30) were randomly and equally assigned to study or control group | Full mouth supra- and SD with manual and ultrasonic scalers, as well as advice about oral hygiene measures Ɨ GCF was collected at 1, 3, and 6 months following therapy | GCF samples were obtained by placing prefabricated paper points into the deepest location until resistance was felt, then left for 30 s Sandwich ELISA was used to assay level of GCF MMP-8 | The samples were diluted in 1 mL of PBS. After leaving samples for 15 min in PBS, they were frozen at −20 °C. | 2.00 ± 1.60 ¶ |
| Author, Year | Age Range Mean ± SD (Years) | Case Definition of Periodontitis | Details of PPD Measurement | Baseline PPD (mm) | ∆ Mean PPD Reduction (mm) ǂ |
|---|---|---|---|---|---|
| Mäntylä et al., 2006 [28] | NR NR | At least 20 teeth, and at least five locations with 4 mm PPD and radiographic bone loss | Details of measurements: NR Clinical parameters were measured by manual periodontal probe (Type: NR) | 5.00 ± 2.10 ¶ | 2.20 ± 0.80 ¶ * |
| Correa et al., 2008 [29] | NR 41.60 ± 7.10 | ≥15 teeth, at least five teeth with one or more sites with PPD ≥ 5 mm, CAL ≥ 4 mm, visible plaque, and BOP | PPD was measured at six sites per tooth using a conventional manual probe (North Carolina probe) | 3.60 § | 1.20 § |
| Pourabbas et al., 2014 [30] | 18 to 70 46 ± 8 | ≥12 natural teeth, with at least three in each quadrant; ≥3 mm CAL in at least 30% of the teeth; and ≥1 site/quadrant with PPD ≥ 4 mm and BOP | Using a conventional manual probe (UNC-15), PPD was measured at six sites per tooth | 4.47 ± 1.23 ¶ | 1.27 ± 0.08 ¶ * |
| Erbil et al., 2020 [31] | 31 to 56 39.72 ± 6.16 | More than three teeth in each quadrant; at least four periodontal pockets with a PPD ≥ 5 mm | PPD was measured at six sites per tooth by a standard manual probe (Williams periodontal probe) | 4–6 mm: 4.70 ± 0.70 ¶ >6 mm: 7.50 ± 0.70 ¶ | 4–6 mm: 1.40 ± 0.01 ¶ * >6 mm: 2.30 ± 0.50 ¶ * |
| Taalab et al., 2021 [32] | 25–50 28.9 ± 6.30 | CAL = 3 to 4 mm, BOP, and radiographic horizontal bone loss in the root’s coronal third (15–33%); no tooth loss as a result of periodontitis | PPD was measured by a standard manual probe (Williams periodontal probe) | 5.50 ± 1.10 ¶ | 1.20 ± 0.40 ¶ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gul, S.S.; Zardawi, F.M.; Abdulkareem, A.A.; Shaikh, M.S.; Al-Rawi, N.H.; Zafar, M.S. Efficacy of MMP-8 Level in Gingival Crevicular Fluid to Predict the Outcome of Nonsurgical Periodontal Treatment: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 3131. https://doi.org/10.3390/ijerph19053131
Gul SS, Zardawi FM, Abdulkareem AA, Shaikh MS, Al-Rawi NH, Zafar MS. Efficacy of MMP-8 Level in Gingival Crevicular Fluid to Predict the Outcome of Nonsurgical Periodontal Treatment: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(5):3131. https://doi.org/10.3390/ijerph19053131
Chicago/Turabian StyleGul, Sarhang Sarwat, Faraedon Mostafa Zardawi, Ali Abbas Abdulkareem, Muhammad Saad Shaikh, Natheer Hashim Al-Rawi, and Muhammad Sohail Zafar. 2022. "Efficacy of MMP-8 Level in Gingival Crevicular Fluid to Predict the Outcome of Nonsurgical Periodontal Treatment: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 5: 3131. https://doi.org/10.3390/ijerph19053131