
Tele-Medicine Based and Self-Administered Interactive Exercise Program (Tele-Exergame) to Improve Cognition in Older Adults with Mild Cognitive Impairment or Dementia: A Feasibility, Acceptability, and Proof-of-Concept Study
 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
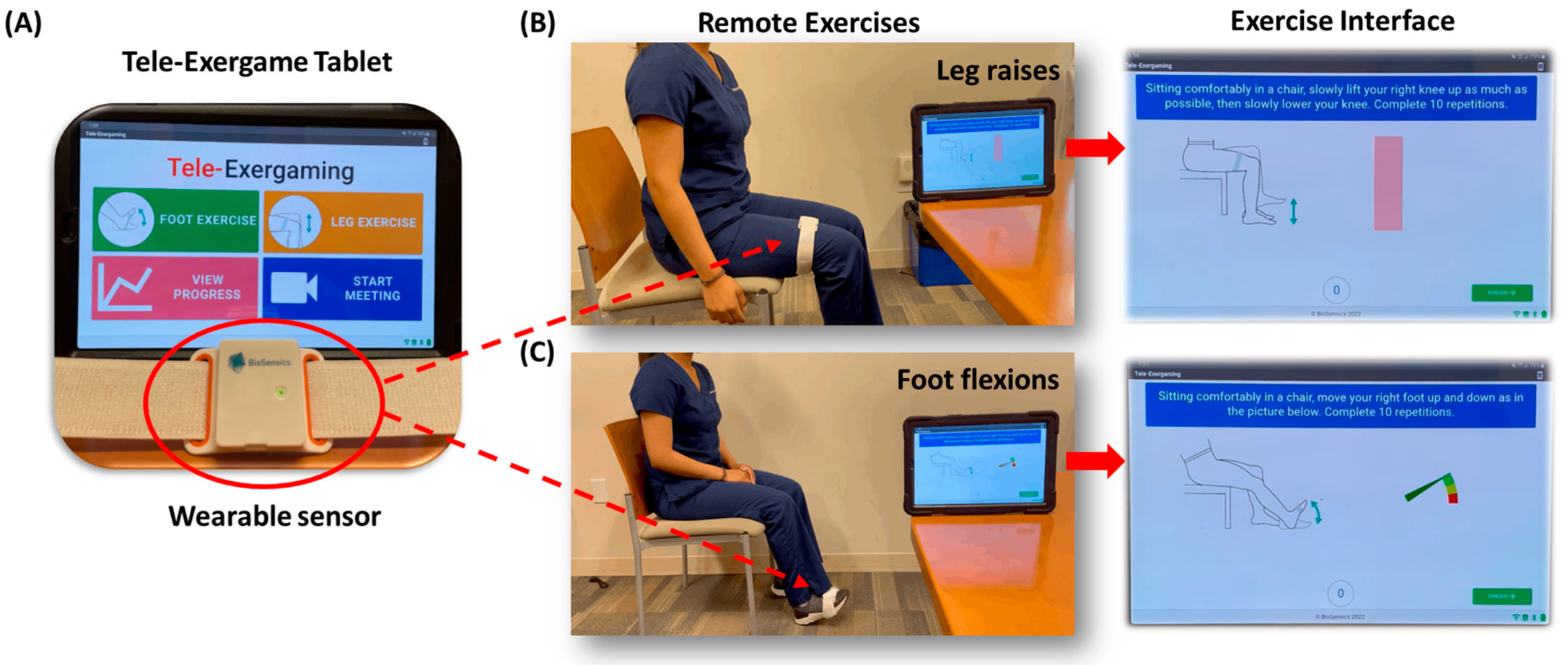
2.1. Tele-Exergame
2.2. Participants and Demographics
2.3. Experimental Procedures
2.4. Data and Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Acceptance of Tele-Exergame
3.3. Cognition and Anxiety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Verghese, J.; Annweiler, C.; Ayers, E.; Barzilai, N.; Beauchet, O.; Bennett, D.A.; Bridenbaugh, S.A.; Buchman, A.S.; Callisaya, M.L.; Camicioli, R.; et al. Motoric cognitive risk syndrome: Multicountry prevalence and dementia risk. Neurology 2014, 83, 718–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panza, F.; Solfrizzi, V.; Barulli, M.R.; Santamato, A.; Seripa, D.; Pilotto, A.; Logroscino, G. Cognitive frailty: A systematic review of epidemiological and neurobiological evidence of an age-related clinical condition. Rejuvenation Res. 2015, 18, 389–412. [Google Scholar] [CrossRef] [PubMed]
- HHS. Dramatic Changes in U.S. In Aging Highlighted in New Census, NIH Report. Available online: https://www.nih.gov/news-events/news-releases/dramatic-changes-us-aging-highlighted-new-census-nih-report (accessed on 22 August 2022).
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2013, 9, 63–75.e62. [Google Scholar] [CrossRef] [PubMed]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The impact of mild cognitive impairment on gait and balance: A systematic review and meta-analysis of studies using instrumented assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef] [Green Version]
- Callahan, K.E.; Lovato, J.F.; Miller, M.E.; Easterling, D.; Snitz, B.; Williamson, J.D. Associations between mild cognitive impairment and hospitalization and readmission. J. Am. Geriatr. Soc. 2015, 63, 1880–1885. [Google Scholar] [CrossRef] [Green Version]
- Muir, S.W.; Gopaul, K.; Montero Odasso, M.M. The role of cognitive impairment in fall risk among older adults: A systematic review and meta-analysis. Age Ageing 2012, 41, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Plassman, B.L.; Langa, K.M.; Fisher, G.G.; Heeringa, S.G.; Weir, D.R.; Ofstedal, M.B.; Burke, J.R.; Hurd, M.D.; Potter, G.G.; Rodgers, W.L.; et al. Prevalence of cognitive impairment without dementia in the United States. Ann. Intern. Med. 2008, 148, 427–434. [Google Scholar] [CrossRef] [Green Version]
- van Gelder, B.M.; Tijhuis, M.A.; Kalmijn, S.; Giampaoli, S.; Nissinen, A.; Kromhout, D. Physical activity in relation to cognitive decline in elderly men: The FINE Study. Neurology 2004, 63, 2316–2321. [Google Scholar] [CrossRef]
- Gallardo-Gómez, D.; Del Pozo-Cruz, J.; Noetel, M.; Álvarez-Barbosa, F.; Alfonso-Rosa, R.M.; Del Pozo Cruz, B. Optimal dose and type of exercise to improve cognitive function in older adults: A systematic review and bayesian model-based network meta-analysis of RCTs. Ageing Res. Rev. 2022, 76, 101591. [Google Scholar] [CrossRef]
- Levin, O.; Netz, Y.; Ziv, G. The beneficial effects of different types of exercise interventions on motor and cognitive functions in older age: A systematic review. Eur. Rev. Aging Phys. Act. Off. J. Eur. Group Res. Into Elder. Phys. Act. 2017, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Teraz, K.; Šlosar, L.; Paravlić, A.H.; de Bruin, E.D.; Marusic, U. Impact of motor-cognitive interventions on selected gait and balance outcomes in older adults: A systematic review and meta-analysis of randomized controlled trials. Front. Psychol. 2022, 13, 837710. [Google Scholar] [CrossRef] [PubMed]
- Wollesen, B.; Wildbredt, A.; van Schooten, K.S.; Lim, M.L.; Delbaere, K. The effects of cognitive-motor training interventions on executive functions in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. Off. J. Eur. Group Res. Elder. Phys. Act. 2020, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Kiper, P.; Richard, M.; Stefanutti, F.; Pierson-Poinsignon, R.; Cacciante, L.; Perin, C.; Mazzucchelli, M.; Viganò, B.; Meroni, R. Combined Motor and Cognitive Rehabilitation: The Impact on Motor Performance in Patients with Mild Cognitive Impairment. Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 276. [Google Scholar] [CrossRef] [PubMed]
- Bamidis, P.D.; Vivas, A.B.; Styliadis, C.; Frantzidis, C.; Klados, M.; Schlee, W.; Siountas, A.; Papageorgiou, S.G. A review of physical and cognitive interventions in aging. Neurosci. Biobehav. Rev. 2014, 44, 206–220. [Google Scholar] [CrossRef]
- Zhu, S.; Sui, Y.; Shen, Y.; Zhu, Y.; Ali, N.; Guo, C.; Wang, T. Effects of virtual reality intervention on cognition and motor function in older adults with mild cognitive impairment or dementia: A systematic review and meta-analysis. Front. Aging Neurosci. 2021, 13, 586999. [Google Scholar] [CrossRef]
- Brennan, D.M.; Tindall, L.; Theodoros, D.; Brown, J.; Campbell, M.; Christiana, D.; Smith, D.; Cason, J.; Lee, A.; American Telemedicine, A. A blueprint for telerehabilitation guidelines—October 2010. Telemed. J. eHealth 2011, 17, 662–665. [Google Scholar] [CrossRef]
- Mishra, R.K.; Park, C.; Momin, A.S.; Rafaei, N.E.; Kunik, M.; York, M.K.; Najafi, B. Care4AD: A Technology-Driven Platform for Care Coordination and Management: Acceptability Study in Dementia. Gerontology 2022. [Google Scholar] [CrossRef]
- Dai, B.; Larnyo, E.; Tetteh, E.A.; Aboagye, A.K.; Musah, A.-A.I. Factors Affecting Caregivers’ Acceptance of the Use of Wearable Devices by Patients With Dementia: An Extension of the Unified Theory of Acceptance and Use of Technology Model. Am. J. Alzheimer’s Dis. Other Dement. 2020, 35, 1533317519883493. [Google Scholar] [CrossRef] [Green Version]
- Czarnuch, S.; Ricciardelli, R.; Mihailidis, A. Predicting the role of assistive technologies in the lives of people with dementia using objective care recipient factors. BMC Geriatr. 2016, 16, 143. [Google Scholar] [CrossRef]
- Miguel Cruz, A.; Lopez Portillo, H.P.; Daum, C.; Rutledge, E.; King, S.; Liu, L. Technology Acceptance and Usability of a Mobile App to Support the Workflow of Health Care Aides Who Provide Services to Older Adults: Pilot Mixed Methods Study. JMIR Aging 2022, 5, e37521. [Google Scholar] [CrossRef] [PubMed]
- Rahemi, H.; Chung, J.; Hinko, V.; Hoeglinger, S.; Martinek, W.A.; Montero-Baker, M.; Mills, J.L.; Najafi, B. Pilot study evaluating the efficacy of exergaming for the prevention of deep venous thrombosis. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Al-Ali, F.; Kang, G.E.; Hamad, A.I.; Ibrahim, R.A.; Talal, T.K.; Najafi, B. Application of wearables to facilitate virtually supervised intradialytic exercise for reducing depression symptoms. Sensors 2020, 20, 1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, R.K.; Park, C.; Zhou, H.; Najafi, B.; Thrasher, T.A. Evaluation of motor and cognitive performance in people with Parkinson’s disease using instrumented trail-making test. Gerontology 2022, 68, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Billis, E.; Strimpakos, N.; Kapreli, E.; Sakellari, V.; Skelton, D.A.; Dontas, I.; Ioannou, F.; Filon, G.; Gioftsos, G. Cross-cultural validation of the Falls Efficacy Scale International (FES-I) in Greek community-dwelling older adults. Disabil. Rehabil. 2011, 33, 1776–1784. [Google Scholar] [CrossRef]
- Park, C.; Atique, M.M.U.; Mishra, R.; Najafi, B. Association between fall history and gait, balance, physical activity, depression, fear of falling, and motor capacity: A 6-month follow-up study. Int. J. Environ. Res. Public Health 2022, 19, 10785. [Google Scholar] [CrossRef]
- Radloff, L.S. A self-report depression scale for research in the general population. Appl. Psychol Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Masrom, M. Technology acceptance model and e-learning. Technology 2007, 21, 81. [Google Scholar]
- Ciesielska, N.; Sokołowski, R.; Mazur, E.; Podhorecka, M.; Polak-Szabela, A.; Kędziora-Kornatowska, K. Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatr. Pol. 2016, 50, 1039–1052. [Google Scholar] [CrossRef]
- Rector, N.A.; Arnold, P.D. Chapter 7—Assessment of patients with anxiety disorders. In Psychiatric Clinical Skills; Goldbloom, D.S., Ed.; Mosby: Philadelphia, PA, USA, 2006; pp. 71–89. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Taylor & Francis: Abingdon, UK, 2013. [Google Scholar]
- Thakur, A.; Sharma, R.; Sharma, S.K.; Thakur, K.; Jelly, P. Effect of buerger allen exercise on foot perfusion among patient with diabetes mellitus: A systematic review & meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102393. [Google Scholar] [CrossRef]
- Horak, F.; King, L.; Mancini, M. Role of body-worn movement monitor technology for balance and gait rehabilitation. Phys. Ther. 2015, 95, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Grewal, G.; Lee-Eng, J.; Talal, T.K.; Menzies, R.A.; Armstrong, D.G. Game-based Guided Exercise: Using an Avatar with Real-Time Feed back to Improve Postural Stability in Diabetic Peripheral Neuropathy. In DIABETES; American Diabetes Association: Arlington, VA, USA, 2014; p. A186. [Google Scholar]
- Zijlstra, A.; Mancini, M.; Chiari, L.; Zijlstra, W. Biofeedback for training balance and mobility tasks in older populations: A systematic review. J. Neuroeng. Rehabil. 2010, 7, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordt, K.; Gerhardy, T.; Najafi, B.; Schwenk, M. Effects of Wearable Sensor-Based Balance and Gait Training on Balance, Gait, and Functional Performance in Healthy and Patient Populations: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Gerontology 2018, 64, 74–89. [Google Scholar] [CrossRef] [PubMed]
- Wulf, G. Attentional focus and motor learning: A review of 10 years of research. e-J. Beweg. Und Train. 2007, 1, 1–11. [Google Scholar]
- van Diest, M.; Lamoth, C.J.; Stegenga, J.; Verkerke, G.J.; Postema, K. Exergaming for balance training of elderly: State of the art and future developments. J. Neuroeng. Rehabil. 2013, 10, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baram, Y. Virtual sensory feedback for gait improvement in neurological patients. Front. Neurol. 2013, 4, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, C.Z.; Wong, D.W.; Lam, W.K.; Wan, A.H.; Lee, W.C. Balance Improvement Effects of Biofeedback Systems with State-of-the-Art Wearable Sensors: A Systematic Review. Sensors 2016, 16, 434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poynter, L.; Kwan, J.; Sayer, A.A.; Vassallo, M. Does cognitive impairment affect rehabilitation outcome? J. Am. Geriatr. Soc. 2011, 59, 2108–2111. [Google Scholar] [CrossRef] [PubMed]
- Shah, D.C.; Evans, M.; King, D. Prevalence of mental illness in a rehabilitation unit for older adults. Postgrad. Med. J. 2000, 76, 153–156. [Google Scholar] [CrossRef]
- Forkan, R.; Pumper, B.; Smyth, N.; Wirkkala, H.; Ciol, M.A.; Shumway-Cook, A. Exercise adherence following physical therapy intervention in older adults with impaired balance. Phys. Ther. 2006, 86, 401–410. [Google Scholar] [CrossRef]
- Hill, K.D.; LoGiudice, D.; Lautenschlager, N.T.; Said, C.M.; Dodd, K.J.; Suttanon, P. Effectiveness of balance training exercise in people with mild to moderate severity Alzheimer’s disease: Protocol for a randomised trial. BMC Geriatr. 2009, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tak, E.; van Uffelen, J.; Paw, M.; van Mechelen, W.; Hopman-Rock, M. Adherence to exercise programs and determinants of maintenance in older adults with mild cognitive impairment. J. Aging Phys. Act. 2012, 20, 32–46. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, M.; Dutzi, I.; Englert, S.; Micol, W.; Najafi, B.; Mohler, J.; Hauer, K. An intensive exercise program improves motor performances in patients with dementia: Translational model of geriatric rehabilitation. J. Alzheimers Dis. 2014, 39, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Lei, H.; Toosizadeh, N.; Schwenk, M.; Sherman, S.; Karp, S.; Sternberg, E.; Najafi, B. A Pilot Clinical Trial to Objectively Assess the Efficacy of Electroacupuncture on Gait in Patients with Parkinson’s Disease Using Body Worn Sensors. PLoS ONE 2016, 11, e0155613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Wardt, V.; Hancox, J.; Gondek, D.; Logan, P.; Nair, R.D.; Pollock, K.; Harwood, R. Adherence support strategies for exercise interventions in people with mild cognitive impairment and dementia: A systematic review. Prev. Med. Rep. 2017, 7, 38–45. [Google Scholar] [CrossRef]
- Kairy, D.; Lehoux, P.; Vincent, C.; Visintin, M. A systematic review of clinical outcomes, clinical process, healthcare utilization and costs associated with telerehabilitation. Disabil. Rehabil. 2009, 31, 427–447. [Google Scholar] [CrossRef]
- Cotelli, M.; Manenti, R.; Brambilla, M.; Gobbi, E.; Ferrari, C.; Binetti, G.; Cappa, S.F. Cognitive telerehabilitation in mild cognitive impairment, Alzheimer’s disease and frontotemporal dementia: A systematic review. J. Telemed. Telecare 2017, 25, 67–79. [Google Scholar] [CrossRef]
- McCue, M.; Fairman, A.; Pramuka, M. Enhancing quality of life through telerehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2010, 21, 195–205. [Google Scholar] [CrossRef]
- Evertson, L.C.; Jennings, L.A.; Reuben, D.B.; Zaila, K.E.; Akram, N.; Romero, T.; Tan, Z.S. Caregiver outcomes of a dementia care program. Geriatr. Nurs. 2021, 42, 447–459. [Google Scholar] [CrossRef]
- Hill, N.T.; Mowszowski, L.; Naismith, S.L.; Chadwick, V.L.; Valenzuela, M.; Lampit, A. Computerized cognitive training in older adults with mild cognitive impairment or dementia: A systematic review and meta-analysis. Am. J. Psychiatry 2017, 174, 329–340. [Google Scholar] [CrossRef] [Green Version]
- Ordonez, T.N.; Borges, F.; Kanashiro, C.S.; Santos, C.; Hora, S.S.; Lima-Silva, T.B. Actively station: Effects on global cognition of mature adults and healthy elderly program using eletronic games. Dement. Neuropsychol. 2017, 11, 186–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bechly, K.E.; Carender, W.J.; Myles, J.D.; Sienko, K.H. Determining the preferred modality for real-time biofeedback during balance training. Gait Posture 2013, 37, 391–396. [Google Scholar] [CrossRef] [PubMed]
- PRC. Mobile Fact Sheet. Available online: https://www.pewresearch.org/internet/fact-sheet/mobile/ (accessed on 26 August 2022).
- Ginis, P.; Nieuwboer, A.; Dorfman, M.; Ferrari, A.; Gazit, E.; Canning, C.G.; Rocchi, L.; Chiari, L.; Hausdorff, J.M.; Mirelman, A. Feasibility and effects of home-based smartphone-delivered automated feedback training for gait in people with Parkinson’s disease: A pilot randomized controlled trial. Parkinsonism Relat. Disord. 2016, 22, 28–34. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Mean ± Standard Deviation or N (%) | |
|---|---|
| Number of participants | 14 |
| Demographics | |
| Age, years | 68.1 ± 5.4 |
| Gender (Female) | 12 (85.7) |
| BMI, kg/m2 | 31.5 ± 7.2 |
| Clinical characteristics | |
| High blood pressure | 12 (85.7) |
| Heart disease or circulation problems | 1 (7.1) |
| Musculoskeletal problems | 5 (35.7) |
| Stroke | 1 (7.1) |
| Depression | 5 (35.7) |
| Sleep problems, n | 7 (50.0) |
| Diabetes | 5 (35.7) |
| Osteoarthritis | 2 (14.3) |
| Rheumatoid arthritis | 2 (14.3) |
| Cancer | 1 (7.1) |
| Urinary tract problems | 2 (14.3) |
| Digestive problems | 5 (35.7) |
| Hearing problems | 3 (21.4) |
| Walking assistance use | 4 (28.6) |
| Had fallen in the past year | 1 (7.1) |
| Daily prescription medications, number | 5.4 ± 2.5 |
| Daily over-the-counter medications, number | 0.9 ± 1.3 |
| Fear of falling and Depression | |
| Concern for fall (FES-I score) | 25.7 ± 6.7 |
| High concern, FES-I ≥ 28 | 5 (35.7) |
| Depression (CES-D score) | 11.8 ± 10.7 |
| Depressed, CES-D ≥ 16 | 4 (28.6) |
| Question | Pre | Post | Mean Difference | Cohen’s d | p Value | |
|---|---|---|---|---|---|---|
| User-friendliness and ease of use | ||||||
| Q1 | I tried very hard during this exercise. | 2.0 ± 1.4 | 0.9 ± 1.2 | −55.0% | 0.84 | 0.032 * |
| Q2 | I would describe this training exercise as very interesting. | 3.1 ± 0.3 | 3.5 ± 0.5 | 12.9% | 0.97 | 0.037 * |
| Perception of Benefit | ||||||
| Q3 | I feel more energetic at home after doing exercise. | 3.0 ± 0.5 | 3.7 ± 0.5 | 23.3% | 1.40 | 0.025 * |
| Q4 | Exercise improves my self-awareness. | 3.1 ± 0.3 | 3.7 ± 0.5 | 19.4% | 1.46 | 0.005 * |
| Q5 | Exercising increases my mental alertness. | 2.9 ± 0.7 | 3.5 ± 0.7 | 20.7% | 0.86 | 0.005 * |
| Q6 | Exercise improves the quality of my work. | 3.1 ± 0.6 | 3.7 ± 0.5 | 19.4% | 1.09 | 0.024 * |
| Q7 | Exercise improves overall body functioning for me. | 3.2 ± 0.4 | 3.7 ± 0.5 | 15.6% | 1.10 | 0.015 * |
| Q8 | Exercise increases my stamina. | 3.2 ± 0.4 | 3.7 ± 0.5 | 15.6% | 1.10 | 0.015 * |
| Q9 | Exercise improves my flexibility. | 3.2 ± 0.4 | 3.7 ± 0.5 | 15.6% | 1.10 | 0.015 * |
| Attitude towards Use | ||||||
| Q10 | I will do similar or more advanced tele-Exergame again. | 3.2 ± 0.4 | 3.6 ± 0.5 | 15.6% | 1.10 | 0.037 * |
| Q11 | Overall, I am very satisfied with the tele-Exergame program I received. | 3.1 ± 0.6 | 3.8 ± 0.4 | 22.6% | 1.37 | 0.010 * |
| Pre | Post | Mean Difference | Cohen’s d | p Value | |
|---|---|---|---|---|---|
| Montreal Cognitive Assessment (MoCA) score | 20.6 ± 5.0 | 22.6 ± 5.6 | 9.7% | 0.38 | 0.017 * |
| Beck anxiety inventory (BAI) score | 9.6 ± 8.4 | 6.9 ± 10.1 | −27.6% | 0.29 | 0.019 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, C.; Mishra, R.k.; York, M.K.; Enriquez, A.; Lindsay, A.; Barchard, G.; Vaziri, A.; Najafi, B. Tele-Medicine Based and Self-Administered Interactive Exercise Program (Tele-Exergame) to Improve Cognition in Older Adults with Mild Cognitive Impairment or Dementia: A Feasibility, Acceptability, and Proof-of-Concept Study. Int. J. Environ. Res. Public Health 2022, 19, 16361. https://doi.org/10.3390/ijerph192316361
Park C, Mishra Rk, York MK, Enriquez A, Lindsay A, Barchard G, Vaziri A, Najafi B. Tele-Medicine Based and Self-Administered Interactive Exercise Program (Tele-Exergame) to Improve Cognition in Older Adults with Mild Cognitive Impairment or Dementia: A Feasibility, Acceptability, and Proof-of-Concept Study. International Journal of Environmental Research and Public Health. 2022; 19(23):16361. https://doi.org/10.3390/ijerph192316361
Chicago/Turabian StylePark, Catherine, Ram kinker Mishra, Michele K. York, Ana Enriquez, Abigail Lindsay, Gregory Barchard, Ashkan Vaziri, and Bijan Najafi. 2022. "Tele-Medicine Based and Self-Administered Interactive Exercise Program (Tele-Exergame) to Improve Cognition in Older Adults with Mild Cognitive Impairment or Dementia: A Feasibility, Acceptability, and Proof-of-Concept Study" International Journal of Environmental Research and Public Health 19, no. 23: 16361. https://doi.org/10.3390/ijerph192316361