
Effects of Coaching-Based Teleoccupational Guidance for Home-Based Stroke Survivors and Their Family Caregivers: A Pilot Randomised Controlled Trial
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
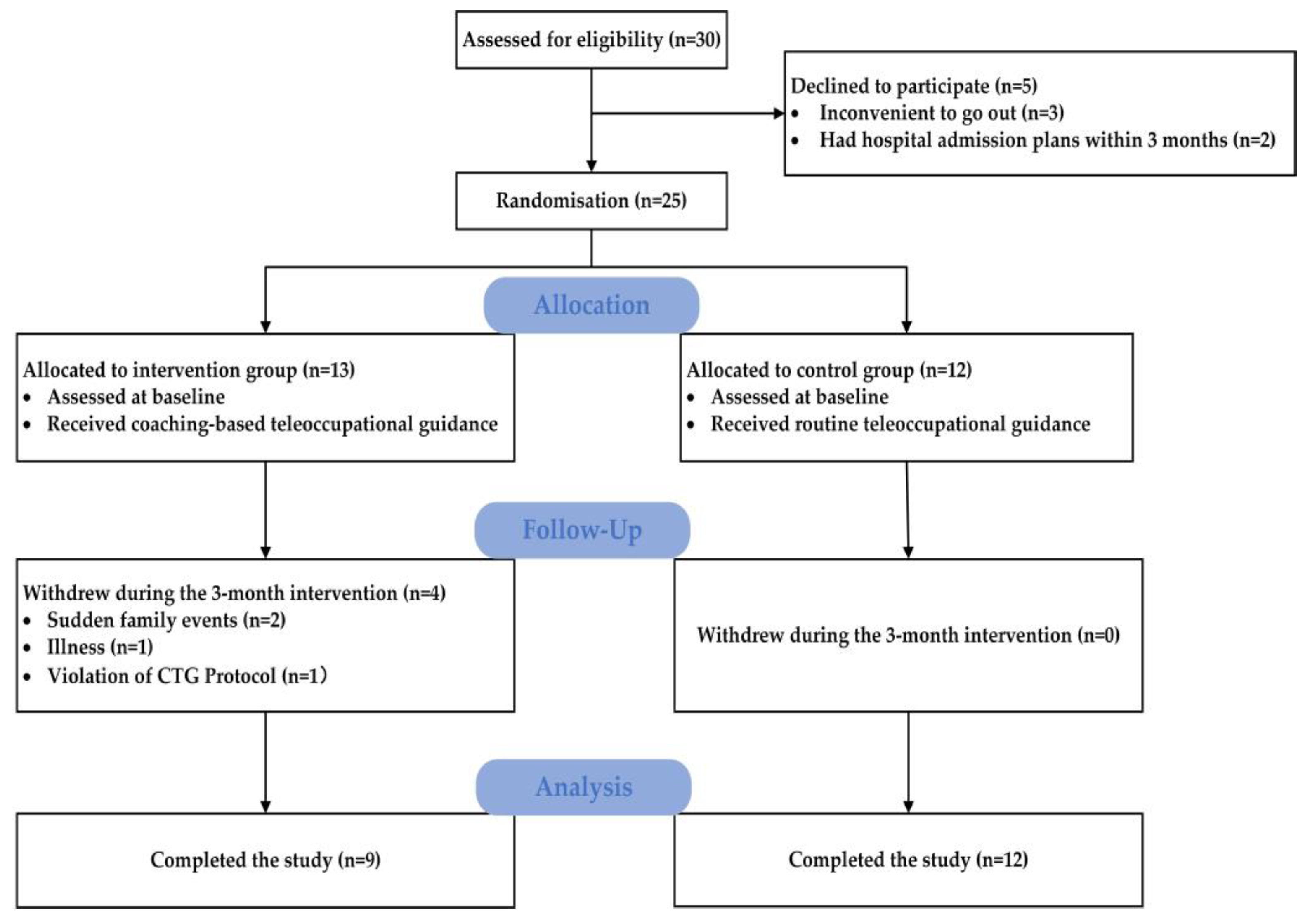
2.2. Study Participants
2.3. Randomisation and Blinding
2.4. Interventions
2.4.1. Coaching-Based Teleoccupational Guidance (Intervention Group)
2.4.2. Routine Teleoccupational Guidance (RTG, Control Group)
2.5. Outcome Measures
2.5.1. Feasibility Measures
2.5.2. Effectiveness Outcome Measures
- Participation was assessed using the Reintegration to Normal Living Index (RNLI), which is a self-reported satisfaction scale to test participation from the perspective of physical activities and social events. The RNLI has been translated into Chinese and has been proven reliable and valid for the Chinese population with Cronbach’s α of 0.92 [17];
- IADL were assessed using the Lawton Instructive Activities of Daily Life (Lawton IADL) scale [18], which tests instructive activities of daily living (ADLs) from the perspective of using the telephone, shopping, preparing food, housekeeping, doing laundry, using transportation, handling medications, and handling finances, and which has been widely applied to Chinese stroke survivors;
- Intrinsic motivation was assessed using the Intrinsic Motivation Inventory (IMI) [19], which is a self-reported scale to test motivational structures for targeted activities from perspectives of interest/enjoyment, perceived competence, pressure/tension, and value/usefulness;
- Motor function was assessed using the Fugl–Meyer Assessment—Upper Extremity (FMA-UE) scale and the 6 min walking test (6MWT) [20,21]. The FMA-UE scale is used to assess the movement, coordination, and reflex actions of the shoulder, elbow, forearm, wrist, and hand; it is an important indicator for evaluating motor function of the upper extremity with good reliability and validity. The 6MWT refers to the walking distance of patients in 6 min, which can reflect the walking capacity of stroke survivors in home environments. The FMA-UE scale and the 6MWT have been widely applied to Chinese stroke survivors;
- QoL was assessed using the Stroke-Specific Quality of Life Scale (SS-QOL), which is a 49-item self-reported test of QoL regarding energy, family roles, language, mobility, mood, personality, self-care, social roles, thinking, upper extremity function, vision, and work/productivity. The SS-QOL has been translated into Chinese and has good internal consistency with Cronbach’s α for each domain ranging from 0.63 to 0.90 [22].
- Perceived benefits were assessed using the Caregiver Benefit Finding Scale (CBFS). The CBFS was designed by Chinese scholars, with a Cronbach’s α range of 0.885 to 0.953 for the subscales, and is a self-reported scale to test caregivers’ perceived benefits from perspectives of individual growth, health promotion, family growth, and self-sublimation [23];
- Caregiver-related burden was assessed using the Chinese version of the Zarit Caregiver Burden Interview (ZBI-c), which is a 22-item self-reported scale evaluating caregiver burden from the dimensions of personal strain and role strain. The ZBI-c was validated in the Chinese population with a Cronbach’s α of 0.87 [24].
2.6. Statistical Analyses
2.7. Sample Size
3. Results
3.1. Demographic Data
3.2. Feasibility Objectives
3.3. Effectiveness Assessments
4. Discussion
5. Recommendations for Future Studies
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global stroke fact sheet 2022. Int. J. Stroke 2022, 17, 18–29. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Le Danseur, M. Stroke rehabilitation. Crit. Care Nurs. Clin. North Am. 2020, 32, 97–108. [Google Scholar] [CrossRef]
- Faiz, K.W.; Labberton, A.S.; Thommessen, B.; Rønning, O.M.; Barra, M. Stroke-related knowledge and lifestyle behavior among stroke survivors. J. Stroke Cerebrovasc. Dis. 2019, 28, 104359. [Google Scholar] [CrossRef] [PubMed]
- Fini, N.A.; Bernhardt, J.; Churilov, L.; Clark, R.; Holland, A.E. Adherence to physical activity and cardiovascular recommendations during the 2years after stroke rehabilitation discharge. Ann. Phys. Rehabil. Med. 2021, 64, 101455. [Google Scholar] [CrossRef] [PubMed]
- Szczepańska-Gieracha, J.; Mazurek, J. The role of self-efficacy in the recovery process of stroke survivors. Psychol. Res. Behav. Manag. 2020, 13, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Wolever, R.Q.; Eisenberg, D.M. What is health coaching anyway?: Standards needed to enable rigorous research. Arch. Intern. Med. 2011, 171, 2017–2018. [Google Scholar] [CrossRef]
- Butterworth, S.; Linden, A.; McClay, W.; Leo, M.C. Effect of motivational interviewing-based health coaching on employees’ physical and mental health status. J. Occup. Health Psychol. 2006, 11, 358–365. [Google Scholar] [CrossRef] [Green Version]
- Field, P.; Franklin, R.C.; Barker, R.; Ring, I.; Leggat, P.; Canuto, K. Heart disease, hospitalisation and referral: Coaching to Achieving Cardiovascular Health through cardiac rehabilitation in Queensland. Aust. J. Rural. Health 2020, 28, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Young, H.M.; Miyamoto, S.; Dharmar, M.; Tang-Feldman, Y. Nurse coaching and mobile health compared with usual care to improve diabetes self-efficacy for persons with type 2 diabetes: Randomized controlled. JMIR Mhealth Uhealth 2020, 8, e16665. [Google Scholar] [CrossRef]
- Deiorio, N.M.; Carney, P.A.; Kahl, L.E.; Bonura, E.M.; Juve, A.M. Coaching: A new model for academic and career achievement. Med. Educ. Online 2016, 21, 33480. [Google Scholar] [CrossRef]
- Nott, M.; Wiseman, L.; Seymour, T.; Pike, S.; Cuming, T.; Wall, G. Stroke self-management and the role of self-efficacy. Disabil. Rehabil. 2021, 43, 1410–1419. [Google Scholar] [CrossRef]
- Barzel, A.; Ketels, G.; Stark, A.; Tetzlaff, B.; Daubmann, A.; Wegscheider, K.; van den Bussche, H.; Scherer, M. Home-based constraint-induced movement therapy for patients with upper limb dysfunction after stroke (HOMECIMT): A cluster-randomised, controlled trial. Lancet Neurol. 2015, 14, 893–902. [Google Scholar] [CrossRef]
- Kessler, D.; Anderson, N.D.; Dawson, D.R. Occupational performance coaching for stroke survivors delivered via telerehabilitation using a single-case experimental design. Br. J. Occup. Ther. 2021, 84, 488–496. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. Consort 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Yan, Y.N.; Sun, Z.X.; Ge, X.J.; Qin, X.L.; Lin, K.C. Coaching-Based teleoccupational guidance for home-based stroke survivors and their family caregivers: Study protocol for a superior randomized controlled trial. Evid. -Based Complement. Altern. Med. 2022, 2022, 9123498. [Google Scholar] [CrossRef]
- Pang, M.Y.; Lau, R.W.; Yeung, P.K.; Liao, L.R.; Chung, R.C. Development and validation of the Chinese version of the Reintegration to Normal Living Index for use with stroke patients. J. Rehabil. Med. Off. J. UEMS Eur. Board Phys. Rehabil. Med. 2011, 43, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Ghaffari, A.; Rostami, H.R.; Akbarfahimi, M. Predictors of instrumental activities of daily living performance in patients with stroke. Occup. Ther. Int. 2021, 2021, 6675680. [Google Scholar] [CrossRef]
- Choi, J.; Mogami, T.; Medalia, A. Intrinsic motivation inventory: An adapted measure for schizophrenia research. Schizophr. Bull. 2010, 36, 966–976. [Google Scholar] [CrossRef] [Green Version]
- Woodbury, M.L.; Velozo, C.A.; Richards, L.G.; Duncan, P.W.; Studenski, S.; Lai, S.M. Longitudinal stability of the Fugl-Meyer Assessment of the upper extremity. Arch. Phys. Med. Rehabil. 2008, 89, 1563–1569. [Google Scholar] [CrossRef]
- Kubo, H.; Nozoe, M.; Yamamoto, M.; Kamo, A.; Noguchi, M.; Kanai, M.; Mase, K.; Shimada, S. Safety and feasibility of the 6-minute walk test in patients with acute stroke. J. Stroke Cerebrovasc. Dis. 2018, 27, 1632–1638. [Google Scholar] [CrossRef] [PubMed]
- Lo, S.H.; Chang, A.M.; Chau, J.P. Establishing equivalence of a Chinese version of the stroke specific quality of life measure for stroke survivors. Disabil. Rehabil. 2017, 39, 1079–1086. [Google Scholar] [CrossRef] [PubMed]
- Mei, Y.X.; Lin, B.L.; Zhang, W.H.; Wang, S.S.; Zhang, Z.X.; Yang, D.B.; Cheung, D.S.K. Creating a caregiver benefit finding scale of family caregivers of stroke survivors: Development and psychometric evaluation. Front. Psychiatry 2020, 11, 734. [Google Scholar] [CrossRef] [PubMed]
- Ko, K.T.; Yip, P.K.; Liu, S.I.; Huang, C.R. Chinese version of the Zarit caregiver burden interview: A validation study. Am. J. Geriatr. Psychiatry 2008, 16, 513–518. [Google Scholar] [CrossRef]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef] [Green Version]
- Smallfield, S.; Molitor, W.L. Occupational therapy interventions supporting social participation and leisure engagement for community-dwelling older adults: A systematic review. Am. J. Occup. Ther. 2018, 72, 7204190020p1–7204190020p8. [Google Scholar] [CrossRef]
- Algurén, B.; Fridlund, B.; Cieza, A.; Sunnerhagen, K.S.; Christensson, L. Factors associated with health-related quality of life after stroke: A 1-year prospective cohort study. Neurorehabilit. Neural Repair 2012, 26, 266–274. [Google Scholar] [CrossRef] [Green Version]
- Bourget, N.; Deblock-Bellamy, A.; Blanchette, A.K.; Batcho, C.S. Use and psychometric properties of the reintegration to normal living index in rehabilitation: A systematic review. Ann. Phys. Rehabil. Med. 2018, 61, 262–269. [Google Scholar] [CrossRef]
- Hammel, J.; Magasi, S.; Heinemann, A.; Whiteneck, G.; Bogner, J.; Rodriguez, E. What does participation mean? An insider perspective from people with disabilities. Disabil. Rehabil. 2008, 30, 1445–1460. [Google Scholar] [CrossRef]
- Kessler, D.; Egan, M.; Dubouloz, C.J.; McEwen, S.; Graham, F.P. Occupational performance coaching for stroke survivors: A pilot randomized controlled trial. Am. J. Occup. Ther. 2017, 71, 7103190020p1–7103190020p7. [Google Scholar] [CrossRef]
- Demain, S.; Wiles, R.; Roberts, L.; McPherson, K. Recovery plateau following stroke: Fact or fiction? Disabil. Rehabil. 2006, 28, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Byblow, W.D. Predicting and accelerating motor recovery after stroke. Curr. Opin. Neurol. 2014, 27, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Page, S.J.; Gater, D.R.; Bach-Y-Rita, P. Reconsidering the motor recovery plateau in stroke rehabilitation. Arch. Phys. Med. Rehabil. 2004, 85, 1377–1381. [Google Scholar] [CrossRef] [PubMed]
- Helgeson, V.S.; Reynolds, K.A.; Tomich, P.L. A meta-analytic review of benefit finding and growth. J. Consult. Clin. Psychol. 2006, 74, 797–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokorelias, K.M.; Lu, F.K.T.; Santos, J.R.; Xu, Y.; Leung, R.; Cameron, J.I. “Caregiving is a full-time job” impacting stroke caregivers’ health and well-being: A qualitative meta-synthesis. Health Soc. Care Community 2020, 28, 325–340. [Google Scholar] [CrossRef] [Green Version]
- Fu, B.; Mei, Y.X.; Lin, B.L.; Guo, Y.W.; Zhang, X.Z.; Qi, B.; Wang, Y. Effects of a benefit-finding intervention in stroke caregivers in communities. Clin. Gerontol. 2022, 45, 1317–1329. [Google Scholar] [CrossRef]


{kind=link}
| Variable | CTG (n = 13) | RTG (n = 12) | p Value |
|---|---|---|---|
| Age (years) | 51.31 ± 8.56 | 53.25 ± 5.75 | 0.514 a |
| Sex (male/female) | 12/1 | 10/2 | 0.490 b |
| Type of stroke (ischaemic/haemorrhagic) | 7/6 | 8/4 | 0.513 b |
| Paretic side (left/right) | 10/3 | 7/5 | 0.319 b |
| Months after stroke | 10.31 ± 3.82 | 10.92 ± 2.07 | 0.629 a |
| Education | |||
| Lower than high school | 4 | 6 | 0.602 c |
| High school | 5 | 2 | |
| Higher education or higher | 4 | 4 | |
| Modified Rankin Scale | |||
| 2, Slight disability | 0 | 1 | 0.298 c |
| 3, Moderate disability | 13 | 11 | |
| 4, Moderately severe disability | 0 | 0 | |
| Caregiver Role | |||
| Couple | 12 | 11 | 0.367 b |
| Child | 1 | 0 | |
| Siblings | 0 | 1 | |
| Caregiver education level | |||
| Lower than high school | 6 | 5 | 0.403 c |
| High school | 3 | 0 | |
| Higher education or higher | 4 | 7 | |
| Outcome measures | |||
| Stroke survivors | |||
| RNLI | 54.00 ± 20.24 | 64.92 ± 23.38 | 0.277 a |
| Lawton IADL | 11.67 ± 4.21 | 13.92 ± 4.56 | 0.262 a |
| IMI | 143.67 ± 23.87 | 145.00 ± 10.72 | 0.865 a |
| FMA-UE | 36.67 ± 19.07 | 35.50 ± 12.44 | 0.867 a |
| 6MWT | 129.00 ± 59.36 | 126.08 ± 56.27 | 0.910 a |
| SS-QOL | 166.33 ± 27.72 | 160.42 ± 29.94 | 0.649 a |
| Caregivers | |||
| CBFS | 92.33 ± 22.80 | 95.00 ± 10.87 | 0.725 a |
| ZBI-c | 43.67 ± 9.37 | 40.33 ± 11.00 | 0.474 a |
| Variable | CTG (n = 9) | RTG (n = 12) | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | p Value | Cohen’s d | Pre-Test | Post-Test | p Value | Cohen’s d | |
| Mean ± SD | Mean ± SD | |||||||
| RNLI | 54.00 ± 20.24 | 77.56 ± 23.68 | <0.001 | 1.066 | 64.92 ± 23.38 | 79.33 ± 17.79 | <0.001 | 0.694 |
| Lawton IADL | 11.67 ± 4.21 | 20.33 ± 3.54 | <0.001 | 2.227 | 13.92 ± 4.56 | 17.08 ± 3.12 | <0.001 | 0.809 |
| IMI | 143.67 ± 23.87 | 156.67 ± 25.16 | <0.001 | 0.530 | 145.00 ± 10.72 | 152.17 ± 11.40 | <0.001 | 0.648 |
| FMA-UE | 36.67 ± 19.07 | 36.67 ± 19.04 | 0.028 | 0.125 | 35.50 ± 12.44 | 36.50 ± 11.90 | 0.002 | 0.082 |
| 6MWT | 129.00 ± 59.36 | 152.33 ± 60.95 | <0.001 | 0.388 | 126.08 ± 56.27 | 145.67 ± 54.86 | <0.001 | 0.353 |
| SS-QOL | 166.33 ± 27.72 | 180.89 ± 28.58 | <0.001 | 0.517 | 160.42 ± 29.94 | 173.92 ± 28.03 | <0.001 | 0.466 |
| CBFS | 92.33 ± 22.80 | 108.89 ± 19.56 | <0.001 | 0.780 | 95.00 ± 10.87 | 106.42 ± 11.72 | <0.001 | 1.024 |
| ZBI-c | 43.67 ± 9.37 | 24.56 ± 9.08 | <0.001 | 2.071 | 40.33 ± 11.00 | 25.42 ± 10.78 | <0.001 | 1.369 |
| Variable | CTG (n = 9) | RTG (n = 12) | p Value | ED, CTG vs. RTG (95% CI) | Cohen’s d |
|---|---|---|---|---|---|
| Pre-Test to Post-Test | Pre-Test to Post-Test | ||||
| Mean ± SD | Mean ± SD | ||||
| RNLI | 23.56 ± 6.98 | 14.42 ± 7.95 | 0.013 * | 9.14 (2.16–16.11) | 0.360 |
| Lawton IADL | 8.67 ± 3.94 | 3.17 ± 2.33 | <0.001 * | 5.50 (2.63–8.87) | 1.416 |
| IMI | 13.00 ± 5.55 | 7.17 ± 3.83 | 0.010 * | 5.83(1.56–10.11) | 1.223 |
| FMA-UE | 1.00 ± 1.12 | 1.00 ± 0.85 | 1.00 | 0.00 (−0.90 to 0.90) | 0.000 |
| 6MWT | 23.33 ± 5.98 | 19.58 ± 3.34 | 0.08 | 3.75 (−0.53 to 8.03) | 0.774 |
| SS-QOL | 14.56 ± 1.59 | 13.50 ± 3.78 | 0.443 | 1.06 (−1.76 to 3.87) | 0.302 |
| CBFS | 16.56 ± 4.69 | 11.42 ± 3.55 | 0.010 * | 5.14 (1.38–8.90) | 1.236 |
| ZBI-c | −19.11 ± 4.76 | −14.92 ± 4.98 | 0.067 | −4.19 (−8.71 to 0.32) | 1.370 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Yan, Y.-N.; Sun, Z.-X.; Yan, D.-R.; Chen, Y.-W.; Lin, K.-C.; Ge, X.-J.; Qin, X.-L. Effects of Coaching-Based Teleoccupational Guidance for Home-Based Stroke Survivors and Their Family Caregivers: A Pilot Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 16355. https://doi.org/10.3390/ijerph192316355
Zhang L, Yan Y-N, Sun Z-X, Yan D-R, Chen Y-W, Lin K-C, Ge X-J, Qin X-L. Effects of Coaching-Based Teleoccupational Guidance for Home-Based Stroke Survivors and Their Family Caregivers: A Pilot Randomised Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(23):16355. https://doi.org/10.3390/ijerph192316355
Chicago/Turabian StyleZhang, Li, Yan-Ning Yan, Zeng-Xin Sun, Dong-Rui Yan, Yuan-Wu Chen, Keh-Chung Lin, Xin-Jing Ge, and Xiao-Lu Qin. 2022. "Effects of Coaching-Based Teleoccupational Guidance for Home-Based Stroke Survivors and Their Family Caregivers: A Pilot Randomised Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 23: 16355. https://doi.org/10.3390/ijerph192316355