
Effects of Compression Stockings on Body Balance in Hemiplegic Patients with Subacute Stroke

Abstract
:1. Introduction
2. Materials and Methods
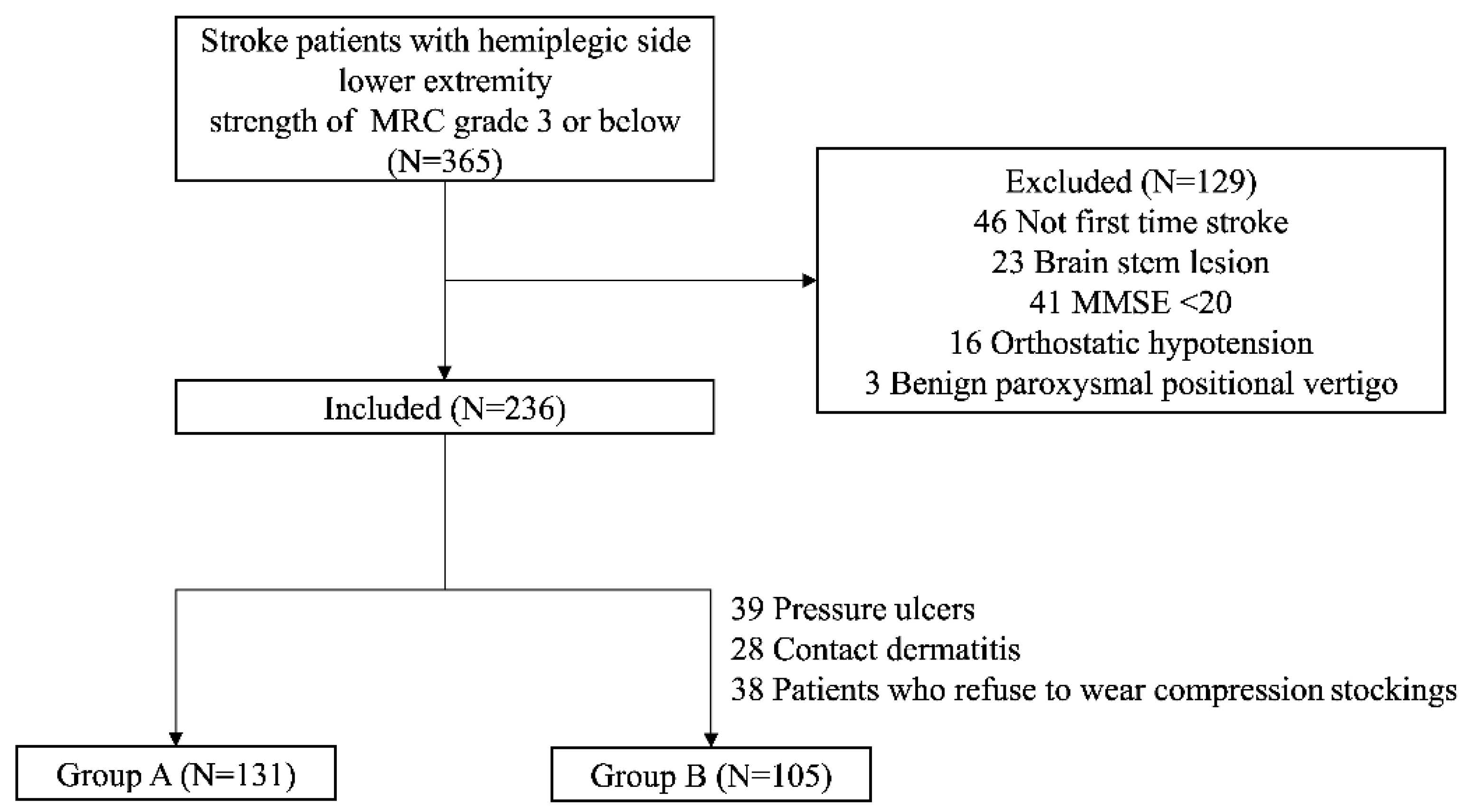
2.1. Subjects
2.2. Procedure
2.3. The Berg Balance Scale
2.4. The Trunk Control Test Score
2.5. The Trunk Impairment Scale
2.6. Modified Barthel Index
2.7. Statistical Analysis
3. Results
3.1. Subjects
3.2. Comparison of Balance Function before and after Treatment
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int. J. Stroke 2022, 17, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Venketasubramanian, N.; Yoon, B.W.; Pandian, J.; Navarro, J.C. Stroke Epidemiology in South, East, and South-East Asia: A Review. J. Stroke 2017, 19, 286–294, Erratum in J. Stroke 2018, 20, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansfield, A.; Inness, E.L.; McIlroy, W.E. Stroke. Handb. Clin. Neurol. 2018, 159, 205–228. [Google Scholar] [PubMed]
- Szopa, A.; Domagalska-Szopa, M.; Lasek-Bal, A.; Żak, A. The link between weight shift asymmetry and gait disturbances in chronic hemiparetic stroke patients. Clin. Interv. Aging 2017, 12, 2055–2062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denissen, S.; Staring, W.; Kunkel, D.; Pickering, R.M.; Lennon, S.; Geurts, A.C.; Weerdesteyn, V.; Verheyden, G.S. Interventions for preventing falls in people after stroke. Cochrane Database Syst. Rev. 2019, 10, Cd008728. [Google Scholar] [CrossRef] [Green Version]
- Wei, W.E.; De Silva, D.A.; Chang, H.M.; Yao, J.; Matchar, D.B.; Young, S.H.Y.; See, S.J.; Lim, G.H.; Wong, T.H.; Venketasubramanian, N. Post-stroke patients with moderate function have the greatest risk of falls: A National Cohort Study. BMC Geriatr. 2019, 19, 373. [Google Scholar] [CrossRef] [Green Version]
- Goto, Y.; Otaka, Y.; Suzuki, K.; Inoue, S.; Kondo, K.; Shimizu, E. Incidence and circumstances of falls among community-dwelling ambulatory stroke survivors: A prospective study. Geriatr. Gerontol. Int. 2019, 19, 240–244. [Google Scholar] [CrossRef]
- Romli, M.H.; Tan, M.P.; Mackenzie, L.; Lovarini, M.; Suttanon, P.; Clemson, L. Falls amongst older people in Southeast Asia: A scoping review. Public Health 2017, 145, 96–112. [Google Scholar] [CrossRef]
- Kim, E.J.; Arai, H.; Chan, P.; Chen, L.-K.; Hill, K.D.; Kong, B.; Poi, P.; Tan, M.P.; Yoo, H.J.; Won, C.W. Strategies on fall prevention for older people living in the community: A report from a round-table meeting in IAGG 2013. J. Clin. Gerontol. Geriatr. 2015, 6, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Whitney, D.G.; Dutt-Mazumder, A.; Peterson, M.D.; Krishnan, C. Fall risk in stroke survivors: Effects of stroke plus dementia and reduced motor functional capacity. J. Neurol. Sci. 2019, 401, 95–100. [Google Scholar] [CrossRef]
- Samuelsson, C.M.; Hansson, P.O.; Persson, C.U. Early prediction of falls after stroke: A 12-month follow-up of 490 patients in The Fall Study of Gothenburg (FallsGOT). Clin. Rehabil. 2019, 33, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Gramont, B.; Chalayer, É.; Savall, A.; Killian, M.; Celarier, T.; Tardy, B. Graduated compression stockings in prevention of venous thromboembolism among acutely ill medical patients aged over 75 years: A French national survey. Clin. Interv. Aging 2019, 14, 1153–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, B. DVT in acute stroke--the use of graduated compression stockings. Aust. Fam. Physician 2010, 39, 485–487. [Google Scholar] [PubMed]
- Mota, G.R.; Simim, M.A.M.; Dos Santos, I.A.; Sasaki, J.E.; Marocolo, M. Effects of Wearing Compression Stockings on Exercise Performance and Associated Indicators: A Systematic Review. Open Access J. Sport. Med. 2020, 11, 29–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, W.-C.; Tseng, L.-W.; Chen, F.-C.; Wang, L.-C.; Yang, W.-W.; Lin, Y.-J.; Liu, C. Effects of compression garments on surface EMG and physiological responses during and after distance running. J. Sport Health Sci. 2020, 9, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Montoye, A.H.K.; Mithen, A.A.; Westra, H.L.; Besteman, S.S.; Rider, B.C. The Effect of Compression Socks on Maximal Exercise Performance and Recovery in Insufficiently Active Adults. Int. J. Exerc. Sci. 2021, 14, 1036–1051. [Google Scholar]
- Leabeater, A.J.; James, L.P.; Driller, M.W. Tight Margins: Compression Garment Use during Exercise and Recovery—A Systematic Review. Textiles 2022, 2, 395–421. [Google Scholar] [CrossRef]
- Sun, Y.; Munro, B.; Zehr, E.P. Compression socks enhance sensory feedback to improve standing balance reactions and reflex control of walking. BMC Sport. Sci. Med. Rehabil. 2021, 13, 61. [Google Scholar] [CrossRef]
- Zehr, E.P.; Hesketh, K.L.; Chua, R. Differential regulation of cutaneous and H-reflexes during leg cycling in humans. J. Neurophysiol. 2001, 85, 1178–1184. [Google Scholar] [CrossRef]
- Zehr, E.P.; Nakajima, T.; Barss, T.; Klarner, T.; Miklosovic, S.; Mezzarane, R.A.; Nurse, M.; Komiyama, T. Cutaneous stimulation of discrete regions of the sole during locomotion produces “sensory steering” of the foot. BMC Sport. Sci. Med. Rehabil. 2014, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Duysens, J.; Tax, A.A.; Trippel, M.; Dietz, V. Phase-dependent reversal of reflexly induced movements during human gait. Exp. Brain Res. 1992, 90, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Derby, H.; Conner, N.O.; Talukder, A.; Griffith, A.; Freeman, C.; Burch, R.; Simpson, J.D.; Goble, D.J.; Knight, A.C.; Chander, H. Impact of Sub-Clinical and Clinical Compression Socks on Postural Stability Tasks among Individuals with Ankle Instability. Healthcare 2022, 10, 1271. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.; Jaszczak, S.L.T.; Steffensen, A.K.S.; Debrabant, B. Using 4+ to grade near-normal muscle strength does not improve agreement. Chiropr. Man. Ther. 2017, 25, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pathak, A.; Gyanpuri, V.; Dev, P.; Dhiman, N.R. The Bobath Concept (NDT) as rehabilitation in stroke patients: A systematic review. J. Fam. Med. Prim. Care 2021, 10, 3983–3990. [Google Scholar]
- Yoon, H.S.; Cha, Y.J.; You, J.S.H. The effects of dynamic core-postural chain stabilization on respiratory function, fatigue and activities of daily living in subacute stroke patients: A randomized control trial. NeuroRehabilitation 2020, 47, 471–477. [Google Scholar] [CrossRef]
- Apriliyasari, R.W.; Van Truong, P.; Tsai, P.S. Effects of proprioceptive training for people with stroke: A meta-analysis of randomized controlled trials. Clin. Rehabil. 2022, 36, 431–448. [Google Scholar] [CrossRef]
- Lee, N.G.; You, J.H.; Yi, C.H.; Jeon, H.S.; Choi, B.S.; Lee, D.R.; Park, J.M.; Lee, T.H.; Ryu, I.T.; Yoon, H.S. Best Core Stabilization for Anticipatory Postural Adjustment and Falls in Hemiparetic Stroke. Arch. Rehabil. Res. Clin. Transl. 2018, 99, 2168–2174. [Google Scholar] [CrossRef]
- Chen, S.-C.; Lin, C.-H.; Su, S.-W.; Chang, Y.-T.; Lai, C.-H. Feasibility and effect of interactive telerehabilitation on balance in individuals with chronic stroke: A pilot study. J. Neuroeng. Rehabil. 2021, 18, 71. [Google Scholar] [CrossRef]
- Kudlac, M.; Sabol, J.; Kaiser, K.; Kane, C.; Phillips, R.S. Reliability and Validity of the Berg Balance Scale in the Stroke Population: A Systematic Review. Phys. Occup. Ther. Geriatr. 2019, 37, 196–221. [Google Scholar] [CrossRef]
- Park, S.H.; Lee, Y.S. The Diagnostic Accuracy of the Berg Balance Scale in Predicting Falls. West. J. Nurs. Res. 2017, 39, 1502–1525. [Google Scholar] [CrossRef]
- Fil Balkan, A.; Salcı, Y.; Keklicek, H.; Çetin, B.; Adın, R.M.; Armutlu, K. The trunk control: Which scale is the best in very acute stroke patients? Top Stroke Rehabil. 2019, 26, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Quinzaños-Fresnedo, J.; Fratini-Escobar, P.C.; Almaguer-Benavides, K.M.; Aguirre-Güemez, A.V.; Barrera-Ortíz, A.; Pérez-Zavala, R.; Villa-Romero, A.R. Prognostic validity of a clinical trunk control test for independence and walking in individuals with spinal cord injury. J. Spinal Cord Med. 2020, 43, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Parlak Demir, Y.; Yıldırım, S.A. Reliability and validity of Trunk Control Test in patients with neuromuscular diseases. Physiother. Theory Pr. 2015, 31, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; An, S.; Lee, G. Clinical utility of the modified trunk impairment scale for stroke survivors. Disabil. Rehabil. 2018, 40, 1200–1205. [Google Scholar] [CrossRef]
- Lee, K.; Lee, D.; Hong, S.; Shin, D.; Jeong, S.; Shin, H.; Choi, W.; An, S.; Lee, G. The relationship between sitting balance, trunk control and mobility with predictive for current mobility level in survivors of sub-acute stroke. PLoS ONE 2021, 16, e0251977. [Google Scholar] [CrossRef]
- Lee, M.J.; Lee, S.; Park, D.-S. A Systematic Review on Trunk Impairment Scale for Stroke Patients. Phys. Ther. Rehabil. Sci. 2021, 10, 379–386. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, D.Y.; Sohn, M.K.; Lee, J.; Lee, S.G.; Shin, Y.I.; Kim, S.Y.; Oh, G.J.; Lee, Y.H.; Lee, Y.S.; et al. Determining the cut-off score for the Modified Barthel Index and the Modified Rankin Scale for assessment of functional independence and residual disability after stroke. PLoS ONE 2020, 15, e0226324. [Google Scholar] [CrossRef] [Green Version]
- Rasman, B.G.; Forbes, P.A.; Tisserand, R.; Blouin, J.S. Sensorimotor Manipulations of the Balance Control Loop-Beyond Imposed External Perturbations. Front. Neurol. 2018, 9, 899. [Google Scholar] [CrossRef] [Green Version]
- Heiss, R.; Hotfiel, T.; Kellermann, M.; May, M.S.; Wuest, W.; Janka, R.; Nagel, A.M.; Uder, M.; Hammon, M. Effect of Compression Garments on the Development of Edema and Soreness in Delayed-Onset Muscle Soreness (DOMS). J. Sport. Sci. Med. 2018, 17, 392–401. [Google Scholar]
- Roijezon, U.; Clark, N.C.; Treleaven, J. Proprioception in musculoskeletal rehabilitation. Part 1: Basic science and principles of assessment and clinical interventions. Man. Ther. 2015, 20, 368–377. [Google Scholar] [CrossRef]
- Clark, N.C.; Roijezon, U.; Treleaven, J. Proprioception in musculoskeletal rehabilitation. Part 2: Clinical assessment and intervention. Man. Ther. 2015, 20, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Pasma, J.H.; Boonstra, T.A.; Campfens, S.F.; Schouten, A.C.; Van der Kooij, H. Sensory reweighting of proprioceptive information of the left and right leg during human balance control. J. Neurophysiol. 2012, 108, 1138–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Q.; Zhang, X.; Mao, M.; Sun, W.; Zhang, C.; Chen, Y.; Li, L. Relationship of proprioception, cutaneous sensitivity, and muscle strength with the balance control among older adults. J. Sport Health Sci. 2021, 10, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.J.; Kidgell, D.J.; Grikepelis, L.A.; Carlson, J.S. Wearing a sports compression garment on the performance of visuomotor tracking following eccentric exercise: A pilot study. J. Sci. Med. Sport 2009, 12, 500–502. [Google Scholar] [CrossRef] [PubMed]
- Orth, D.; Davids, K.; Wheat, J.; Seifert, L.; Liukkonen, J.; Jaakkola, T.; Ashford, D.; Kerr, G. The role of textured material in supporting perceptual-motor functions. PLoS ONE 2013, 8, e60349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davids, K.; Shuttleworth, R.; Button, C.; Renshaw, I.; Glazier, P. Essential noise—Enhancing variability of informational constraints benefits movement control: A comment on Waddington and Adams (2003). Br. J. Sport. Med. 2004, 38, 601–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Son, B.; Han, I.; Lee, W. Effect of Cutaneous Feedback on the Perception of Virtual Object Weight during Manipulation. Sci. Rep. 2020, 10, 1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barss, T.S.; Pearcey, G.E.P.; Munro, B.; Bishop, J.L.; Zehr, E.P. Effects of a compression garment on sensory feedback transmission in the human upper limb. J. Neurophysiol. 2018, 120, 186–195. [Google Scholar] [CrossRef] [Green Version]
- Born, D.P.; Sperlich, B.; Holmberg, H.C. Bringing light into the dark: Effects of compression clothing on performance and recovery. Int. J. Sports. Physiol. Perform. 2013, 8, 4–18. [Google Scholar] [CrossRef] [Green Version]
- Chang, L.; Fu, S.; Wu, S.; Witchalls, J.; Adams, R.; Waddington, G.; Han, J. Effects of graduated compression socks on ankle inversion proprioception of half-marathon runners at different running distances. J. Sci. Med. Sport 2022, 25, 529–534. [Google Scholar] [CrossRef]
- Woo, M.T.; Davids, K.; Chow, J.Y.; Jaakkola, T. Acute effects of wearing compression knee-length socks on ankle joint position sense in community-dwelling older adults. PLoS ONE 2021, 16, e0245979. [Google Scholar] [CrossRef] [PubMed]
- Schinkel-Ivy, A.; Inness, E.L.; Mansfield, A. Relationships between fear of falling, balance confidence, and control of balance, gait, and reactive stepping in individuals with sub-acute stroke. Gait. Posture. 2016, 43, 154–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alghadir, A.H.; Al-Eisa, E.S.; Anwer, S.; Sarkar, B. Reliability, validity, and responsiveness of three scales for measuring balance in patients with chronic stroke. BMC Neurol. 2018, 18, 141. [Google Scholar] [CrossRef]
- Park, S.-H. Tools for assessing fall risk in the elderly: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2018, 30, 1–16. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Value |
|---|---|
| Age (years) | 69.55 ± 12.92 |
| Sex | |
| Male | 115 (48.70) |
| Female | 121 (51.30) |
| Type of stroke | |
| Ischemic | 126 (53.40) |
| Hemorrhagic | 110 (46.60) |
| MBI | 55.31 ± 8.79 |
| MMSE | 22.99 ± 3.22 |
| BBS | 22.00 ± 4.57 |
| TCT | 40.13 ± 6.11 |
| TIS | 10.56 ± 1.65 |
| Variables | Group A (N = 131) | Group B (N = 105) | p-Value |
|---|---|---|---|
| Age (years) | 70.79 ± 12.41 | 68.75 ± 13.06 | 0.24 |
| Sex | 0.13 | ||
| Male | 58 (44.30) | 57 (54.30) | |
| Female | 73 (55.70) | 48 (45.70) | |
| Type of stroke | 0.99 | ||
| Ischemic | 70 (53.40) | 56 (53.30) | |
| Hemorrhagic | 61 (46.60) | 49 (47.70) | |
| MBI | 55.87 ± 8.82 | 54.60 ± 8.74 | 0.27 |
| MMSE | 22.89 ± 3.15 | 23.11 ± 3.32 | 0.32 |
| BBS | 21.89 ± 4.44 | 22.13 ± 4.74 | 0.68 |
| TCT | 40.05 ± 6.35 | 40.23 ± 5.82 | 0.82 |
| TIS | 10.54 ± 1.72 | 10.57 ± 1.57 | 0.89 |
| Variables | Group A (N = 131) | Group B (N = 105) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | p-Value | Pre | Post | p-Value | |
| BBS | 21.89 ± 4.44 | 31.97 ± 5.86 | 0.031 * | 22.13 ± 4.74 | 27.30 ± 5.92 | 0.027 * |
| TCT | 40.05 ± 6.35 | 55.37 ± 9.90 | <0.001 ** | 40.23 ± 5.82 | 48.06 ± 8.83 | <0.001 ** |
| TIS | 10.54 ± 1.72 | 14.86 ± 3.20 | 0.015 * | 10.57 ± 1.57 | 12.98 ± 1.89 | 0.031 * |
| Variables | Group A (N = 131) | Group B (N = 105) | p-Value |
|---|---|---|---|
| ΔBBS | 10.08 ± 6.94 | 5.17 ± 7.32 | 0.015 * |
| ΔTCT | 15.31 ± 11.58 | 7.82 ± 10.69 | <0.001 ** |
| ΔTIS | 4.32 ± 3.47 | 2.40 ± 2.56 | 0.032 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, E.J. Effects of Compression Stockings on Body Balance in Hemiplegic Patients with Subacute Stroke. Int. J. Environ. Res. Public Health 2022, 19, 16212. https://doi.org/10.3390/ijerph192316212
Park EJ. Effects of Compression Stockings on Body Balance in Hemiplegic Patients with Subacute Stroke. International Journal of Environmental Research and Public Health. 2022; 19(23):16212. https://doi.org/10.3390/ijerph192316212
Chicago/Turabian StylePark, Eo Jin. 2022. "Effects of Compression Stockings on Body Balance in Hemiplegic Patients with Subacute Stroke" International Journal of Environmental Research and Public Health 19, no. 23: 16212. https://doi.org/10.3390/ijerph192316212