
Co-Design in Electrical Medical Beds with Caregivers
 , ,
, ,
Abstract
:1. Introduction
1.1. Human-Centred Design in Healthcare Environments
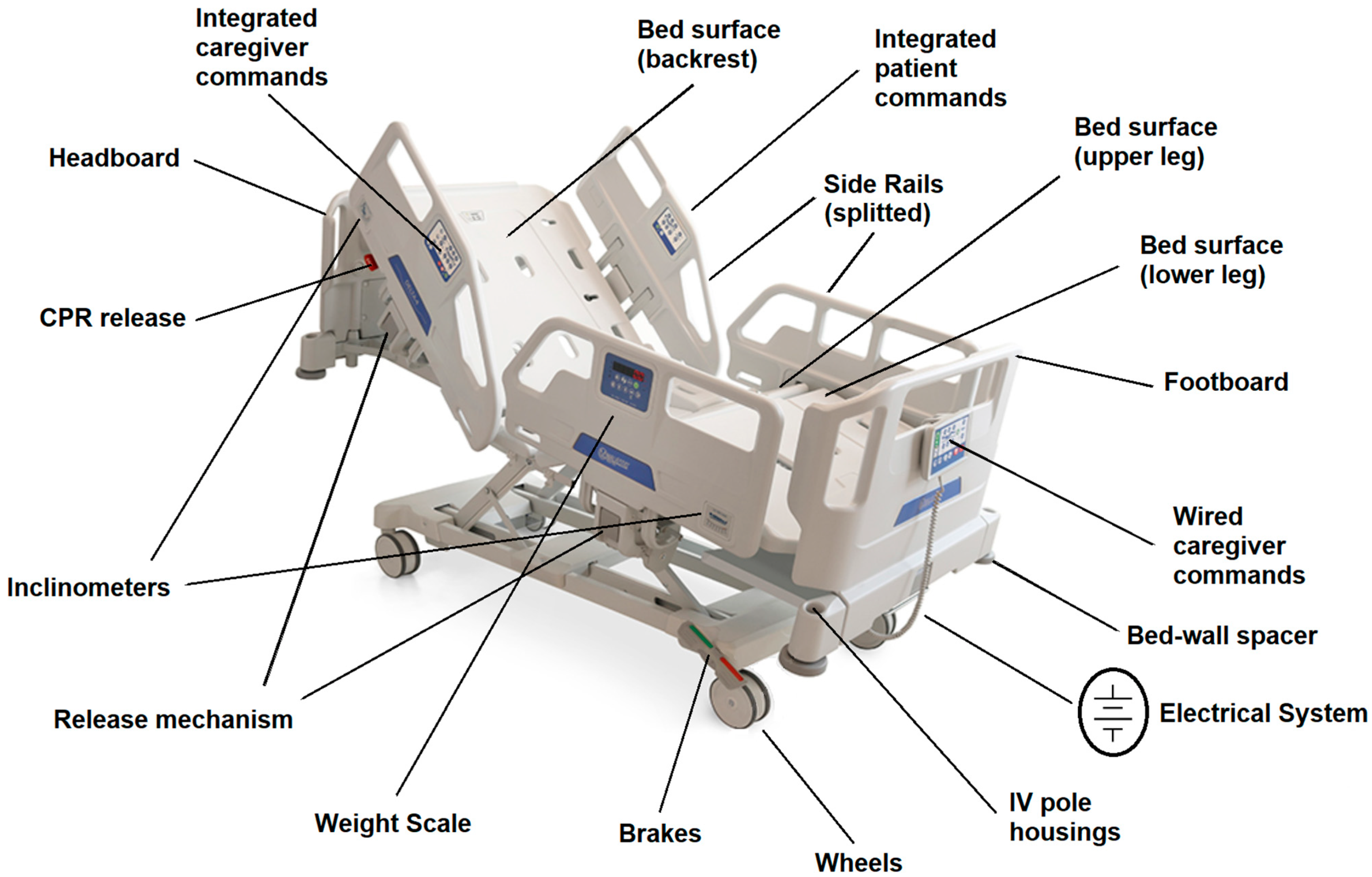
1.2. Medical Beds
1.3. Research Objective
2. Materials and Methods
2.1. Focus Group
2.2. Procedure
2.3. Participants
3. Results
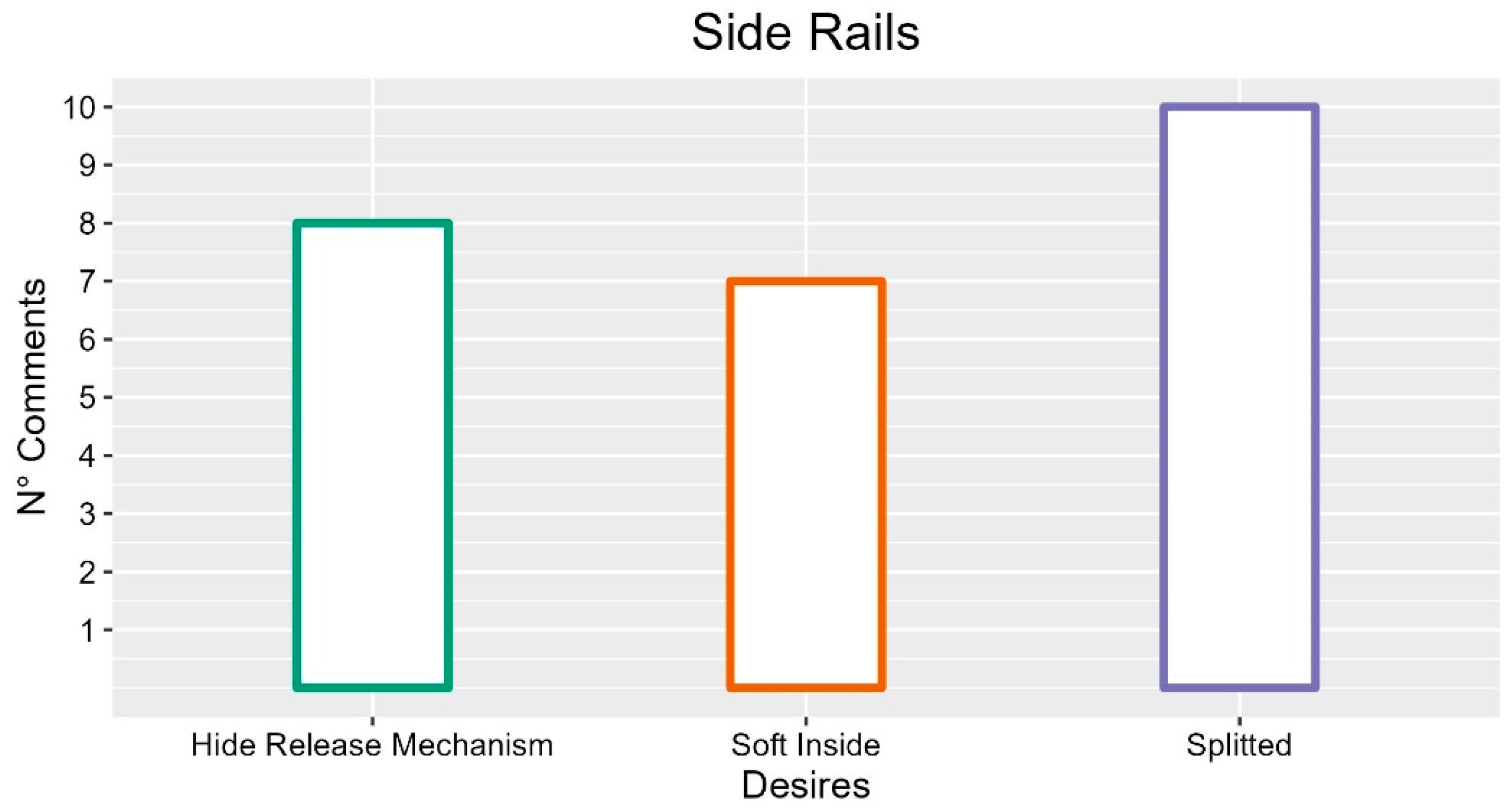
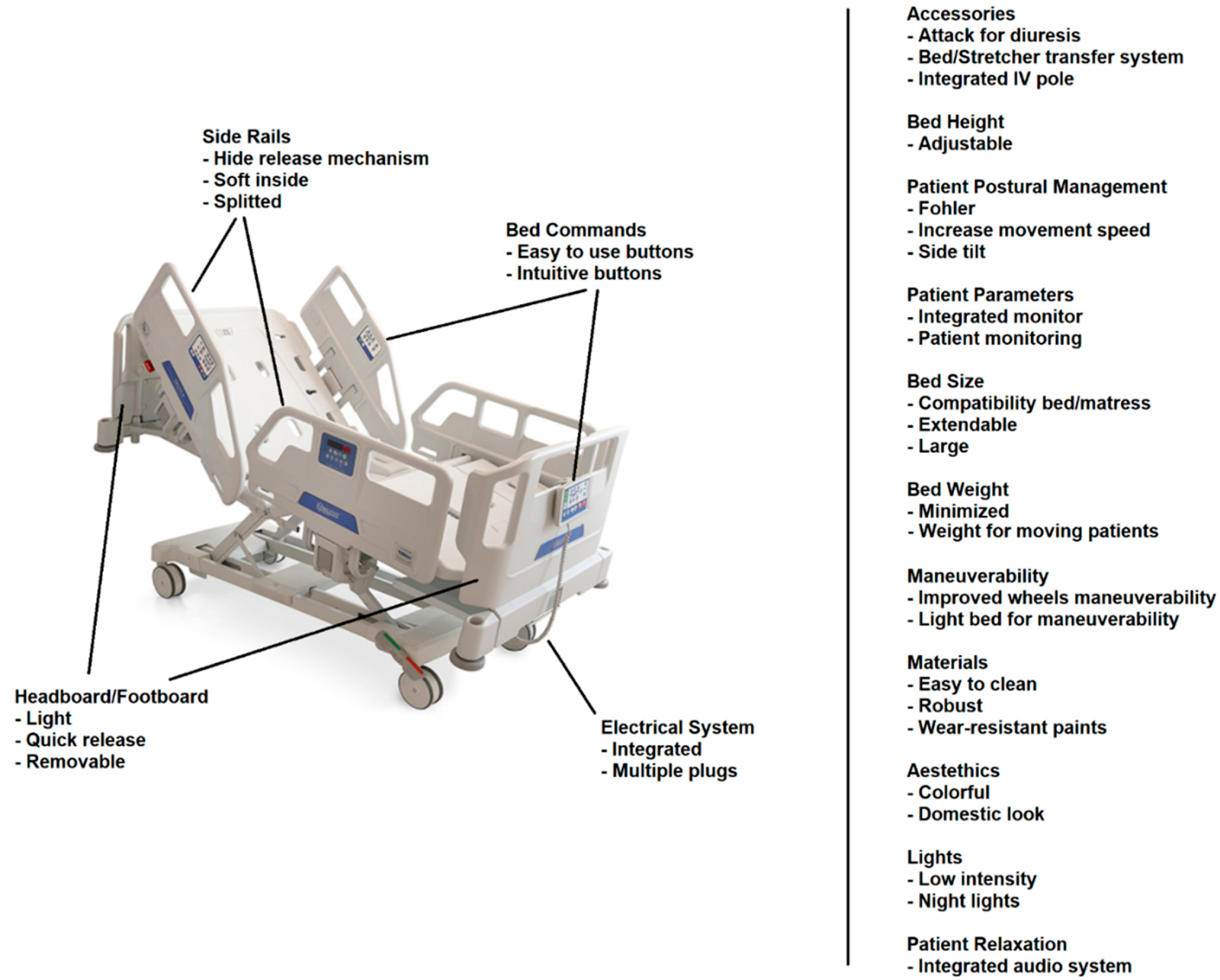
3.1. Side Rails
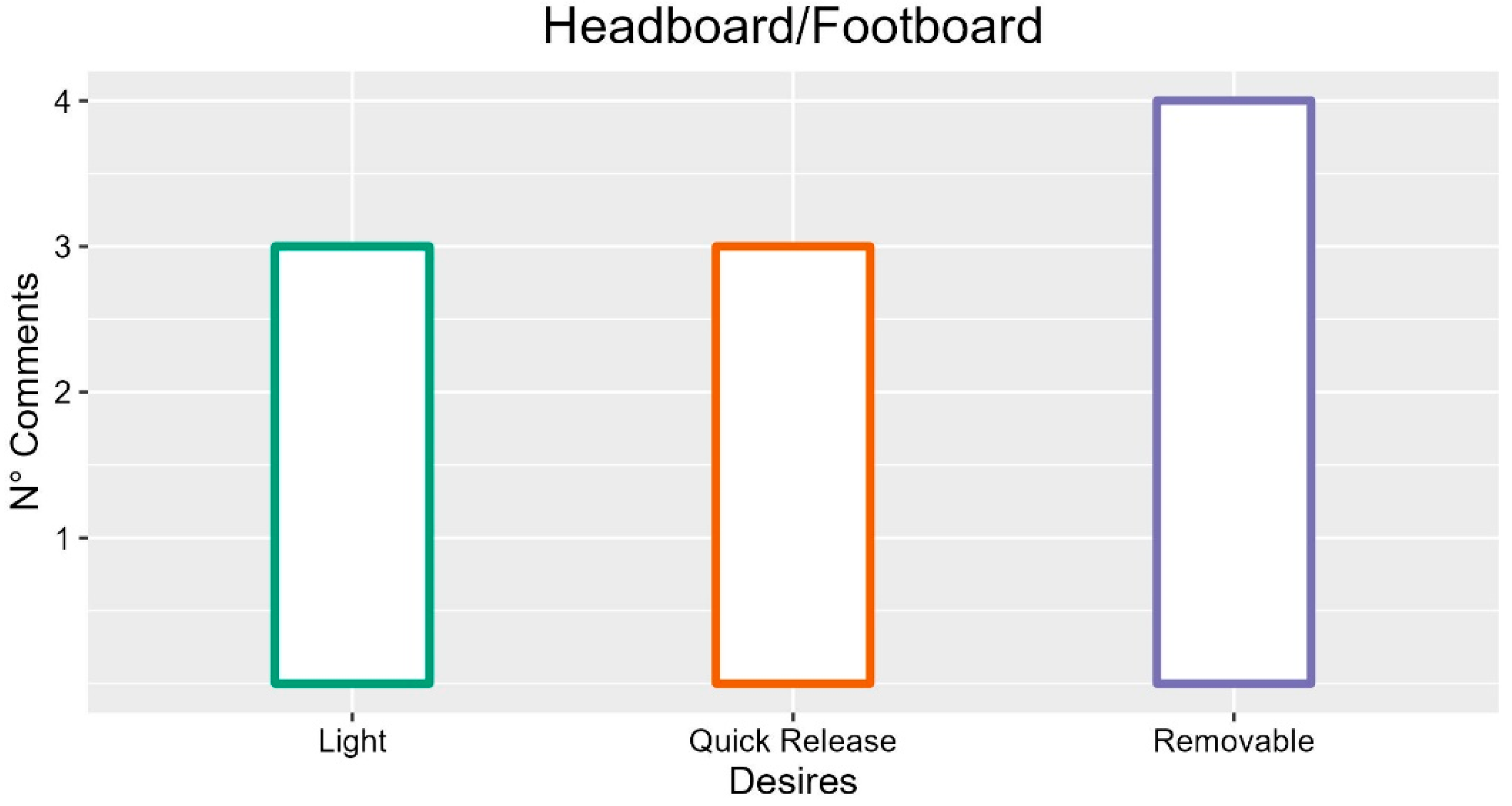
3.2. Headboard/Footboard
3.3. Bed Base Surface
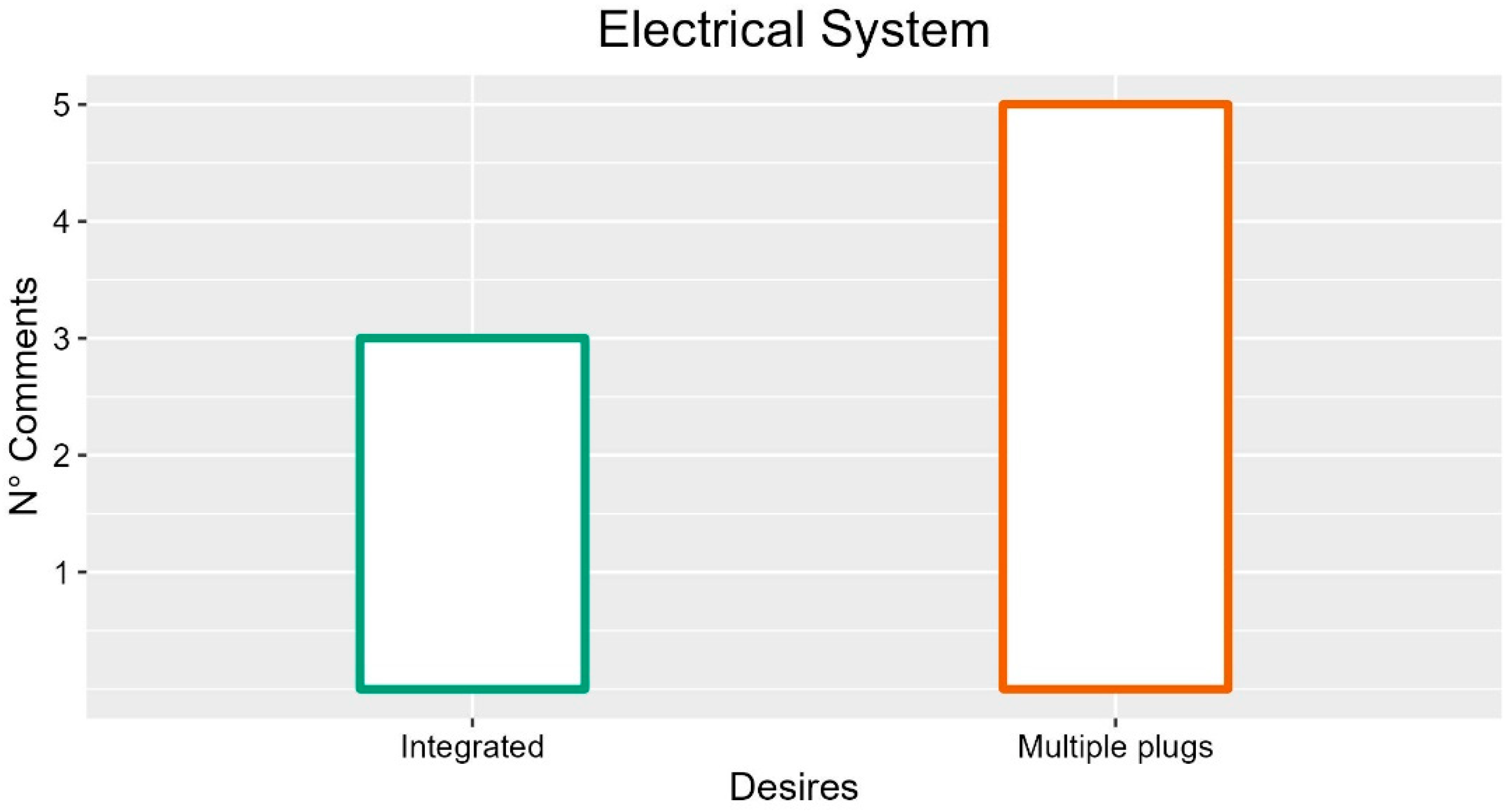
3.4. Electrical System
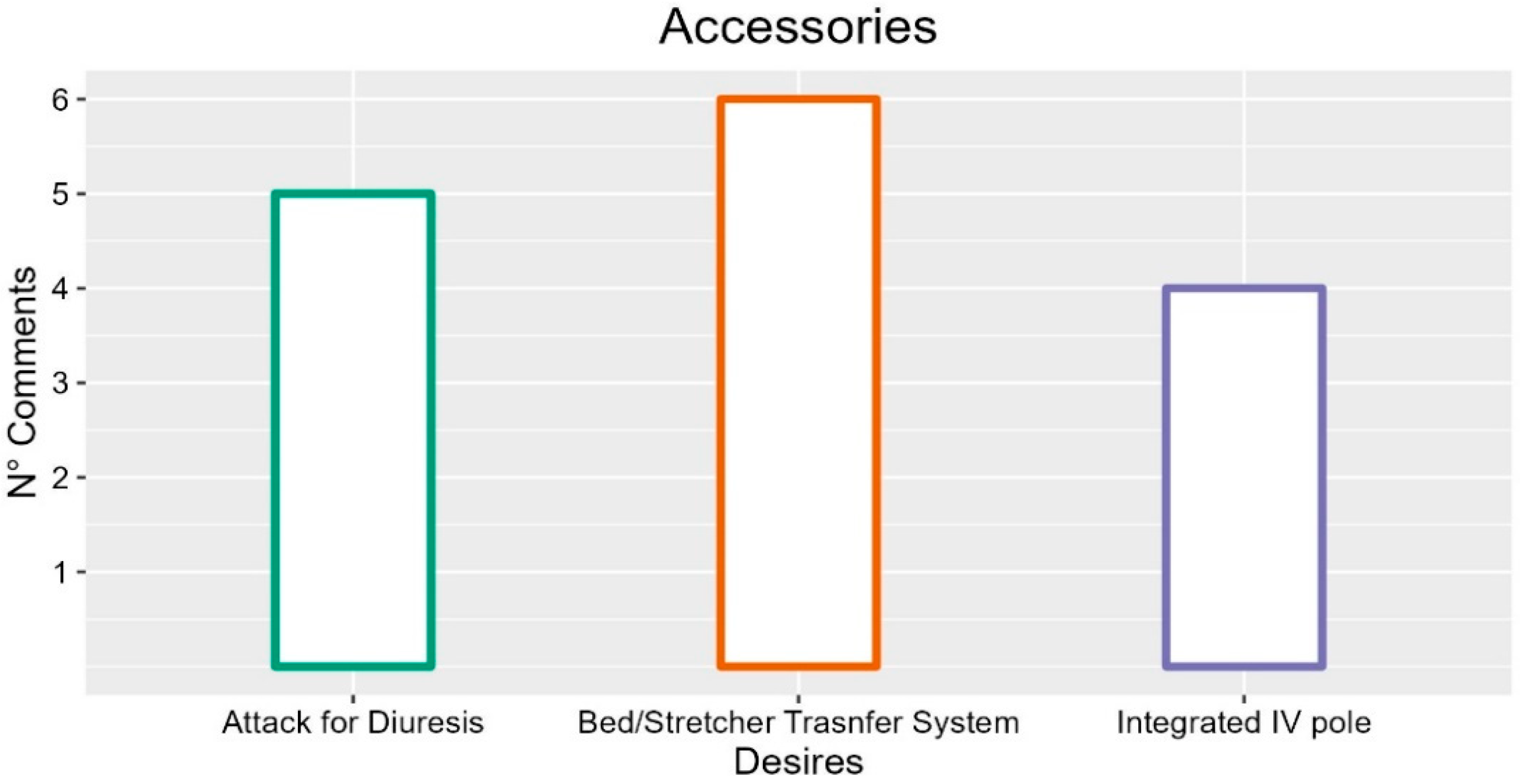
3.5. Accessories
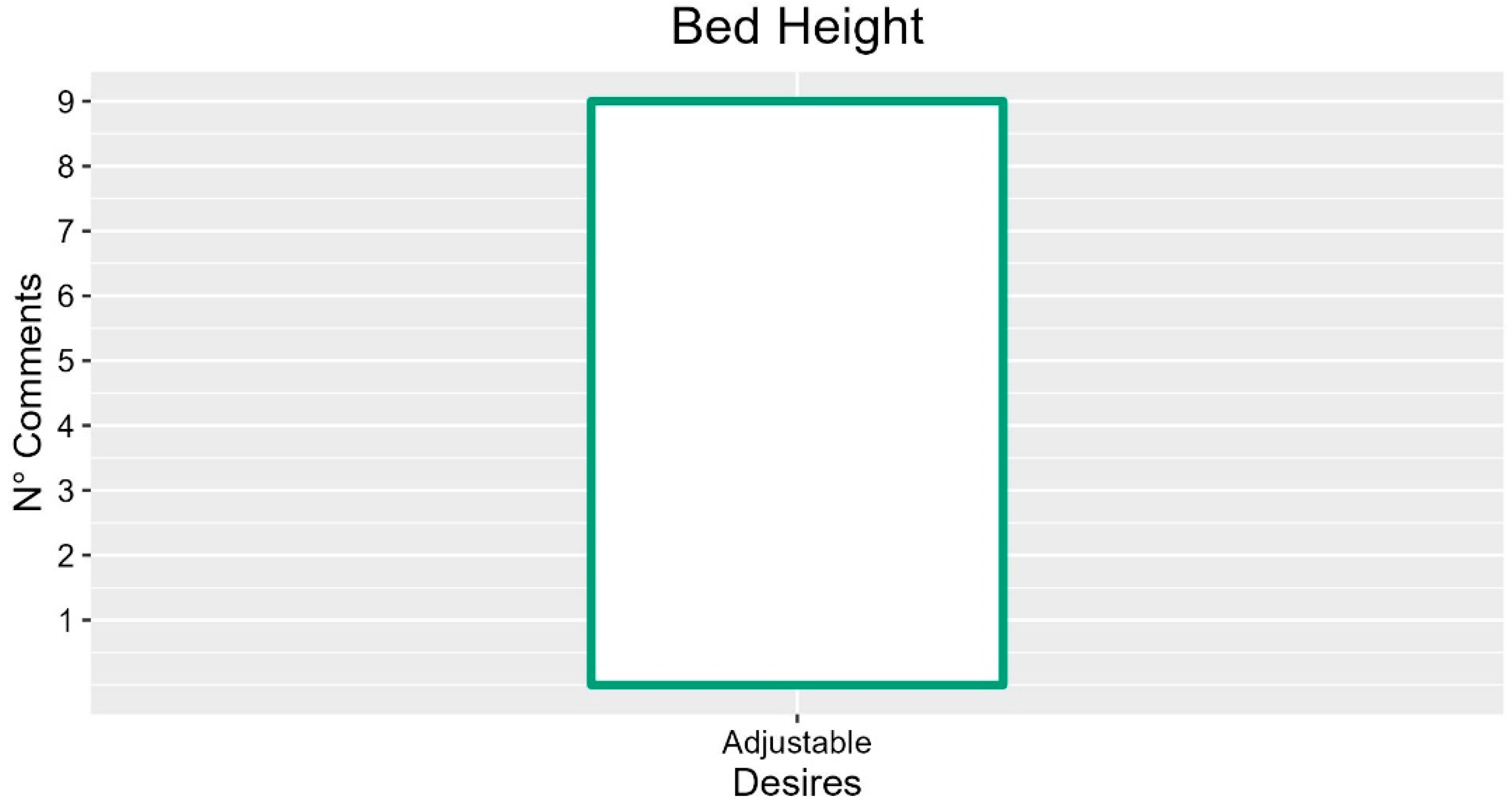
3.6. Bed Height
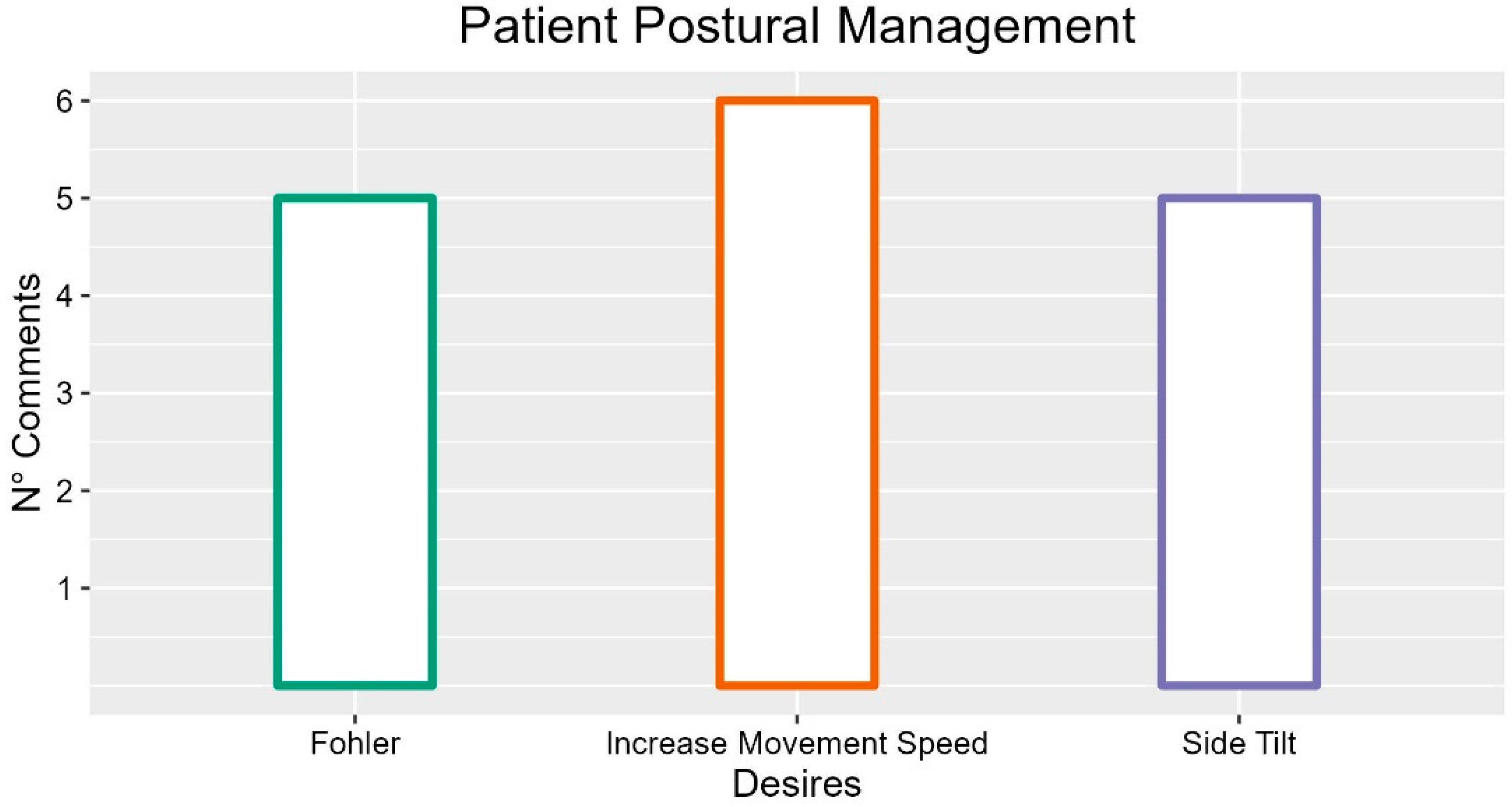
3.7. Patient Postural Management
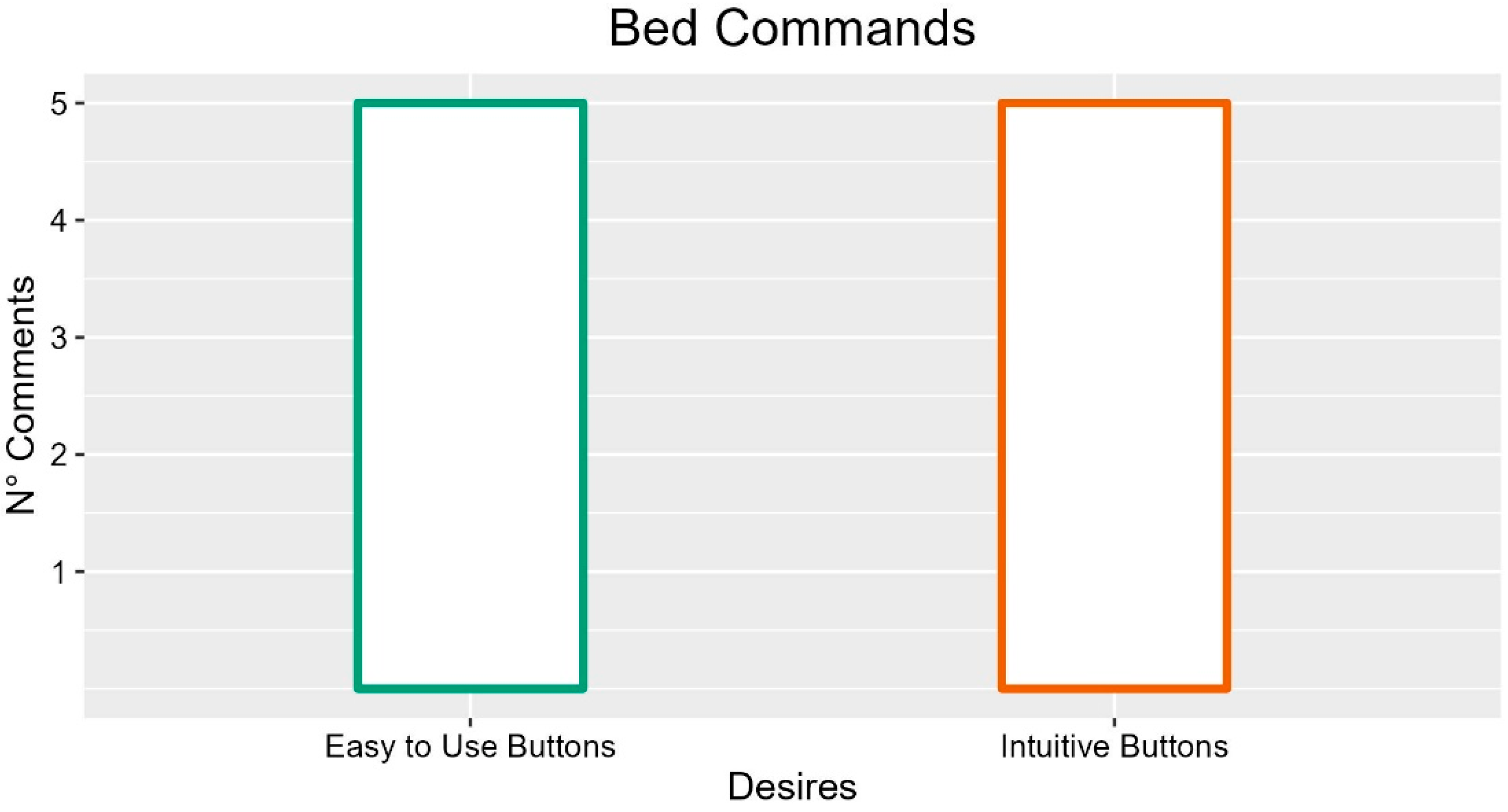
3.8. Bed Commands
3.9. Nurse Call
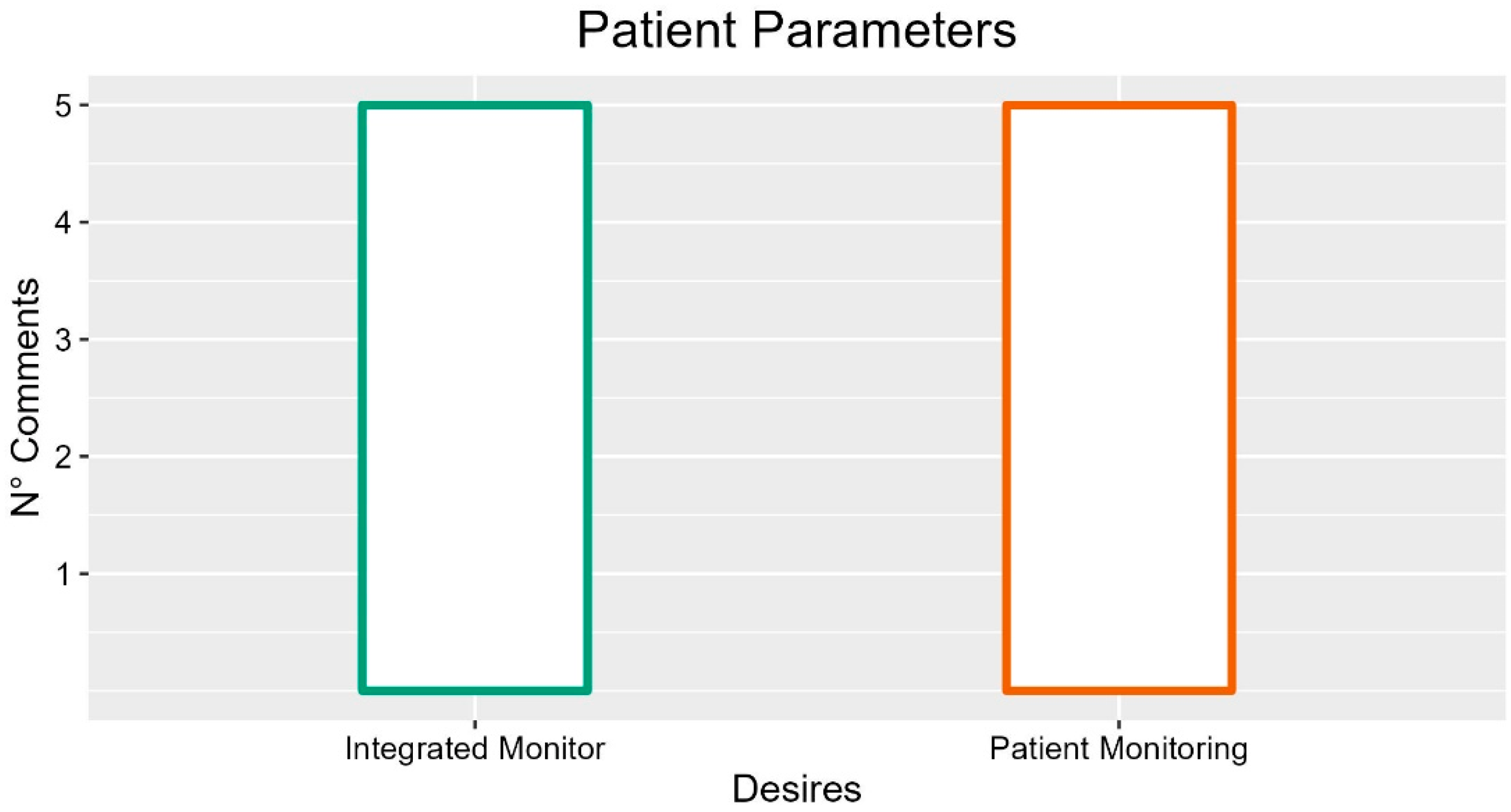
3.10. Patient Parameters
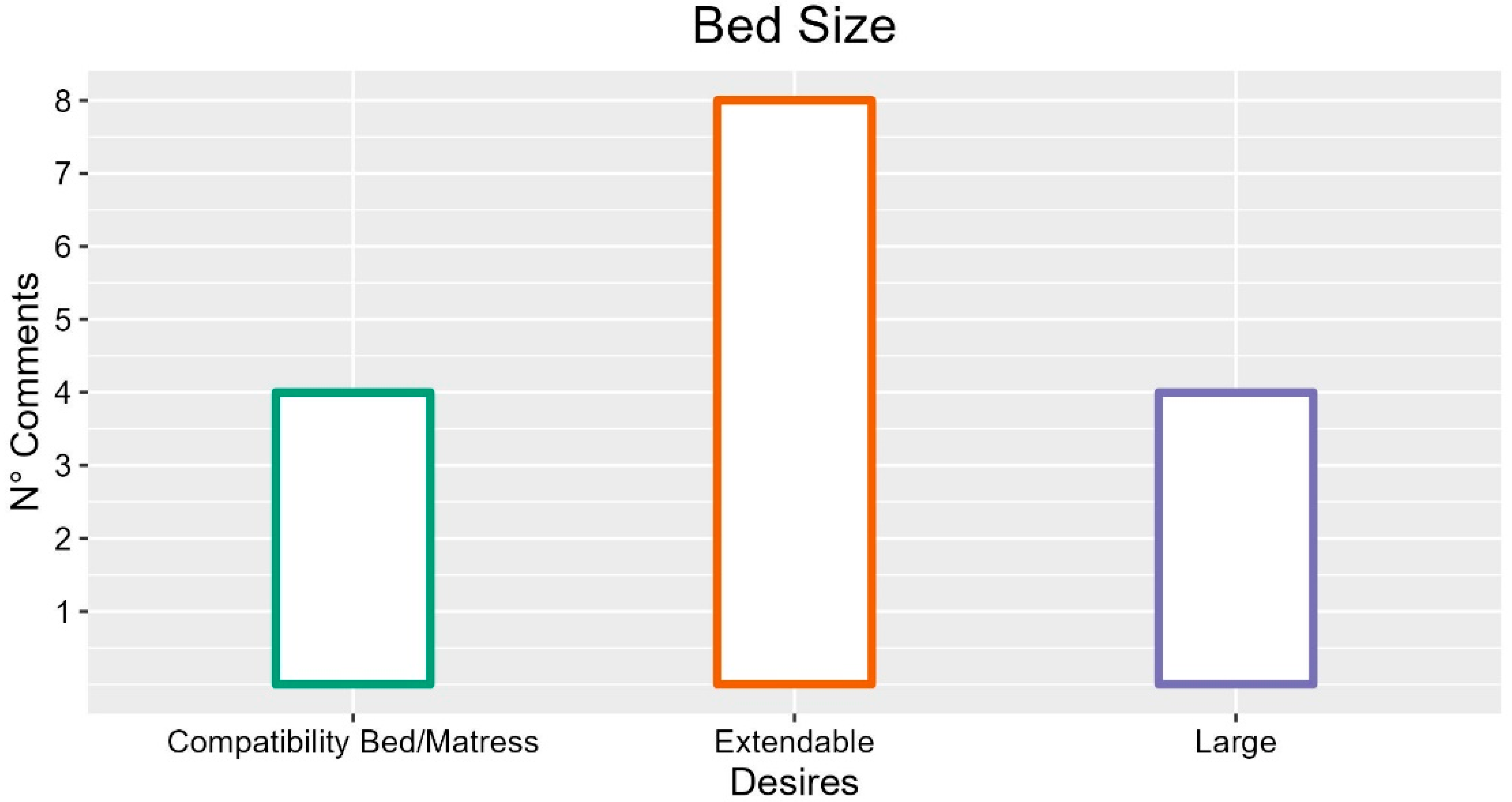
3.11. Bed Size
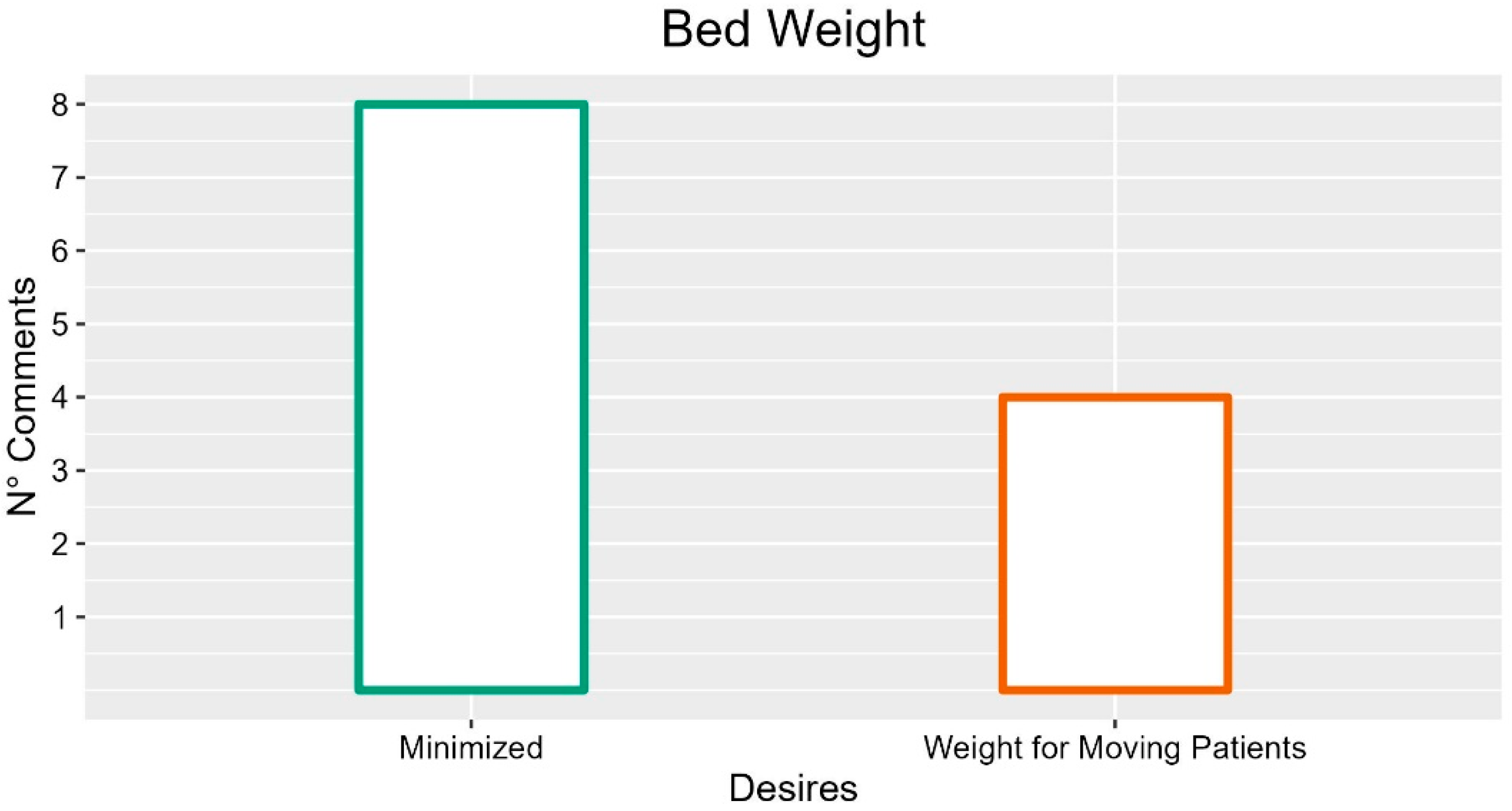
3.12. Bed Weight
3.13. Manoeuvrability
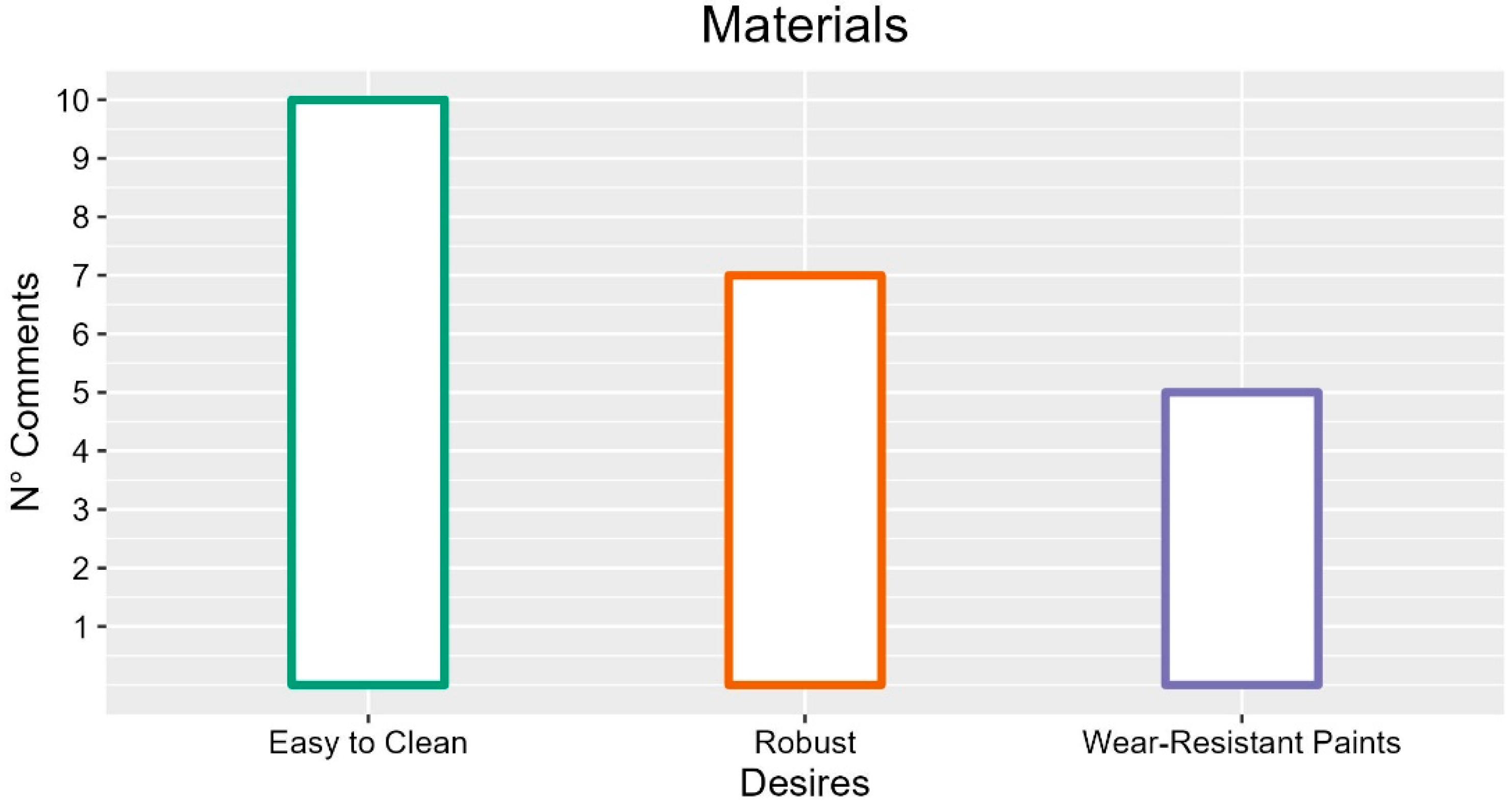
3.14. Materials
3.15. Maintenance
3.16. Aesthetics
3.17. Lights
3.18. Patient Relaxation
4. Discussion
4.1. Design for Physical Workload Reduction
4.2. Design for Bed Adaptability to Different Situations
4.3. Design for Patient Safety
4.4. Design for Easy-to-Clean Bed
4.5. Design for Aesthetics and Durability
4.6. Design for Patient Comfort
4.7. UX Design of Medical Beds
4.7.1. Emerging Factors for User Experience
Safety
Comfort
Ease of Use
Timesaving and Workload Reduction
Perceived Usefulness
Flexibility
Aesthetics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Bed Element | Desires | Description | N°of Occurrences during Interviews |
| Side Rails | |||
| Split into two sections | Pro: Easy to clean, escape routes for tubes and drains, less evident restraint, follow backrest movement. Cons: The patient can get stuck in empty spaces. | 10 | |
| Unique | Pro: Quickly lowered with a single gesture, avoid that cables and patient stuck between the said rails Cons: Possible patient joint between the side rails boards | 6 | |
| Low | Less dangerous falls | 5 | |
| Adjustable | Both electrically and manually | 4 | |
| Support points | To permit lean of the patient | 3 | |
| Curved, rounded | Less sense of restraint and suffocation | 6 | |
| Release mechanism that slides under the bed net | Avoid accidents, avoid creating gaps between the bed and other supports | 8 | |
| Easy to use and handy | They help in making the bed | 3 | |
| Single action to unlock | 4 | ||
| One-hand release | 3 | ||
| Quickly closable | 1 | ||
| Sides lowered alarm | 1 | ||
| Braked | Avoid pinching | 1 | |
| Light | 2 | ||
| Resistant | 5 | ||
| Soft inside / padded | Safe and comfortable | 7 | |
| Made of plastic | 1 | ||
| Fireproof | 1 | ||
| Smooth | 2 | ||
| Solid/Transparent sides and non-straight bars | They prevent patients’ feeling of imprisonment | 7 | |
| Headboard/Footboard | |||
| Not bulky | 2 | ||
| Flexible for accessories | 2 | ||
| Removable | Facilitate the positioning of bulky equipment, feature that gives comfort and safety | 4 | |
| Light | 3 | ||
| Soft | Avoid injury to the patient | 2 | |
| Quick to release | Comfortable for hygiene and therapies | 3 | |
| Bed Surface | |||
| Solid surface | Facilitating cleaning as it is a surface that tends to get dirty | 2 | |
| Waterproof | 1 | ||
| Smooth | 1 | ||
| Resistant | 1 | ||
| Solid | 1 | ||
| Electrical System | Multi-socket for instrumentation | Solve the cable jam problem | 5 |
| Internal multi-socket bed for the patient | 1 | ||
| Head side socket | 2 | ||
| Magnetic socket | 1 | ||
| Integrated anti-decubitus mattress plugs | 1 | ||
| Integrated electrical socket | 3 | ||
| Integrated USB port | 2 | ||
| Hidden electrical cables | They wear less and improve the aesthetics of the bed | 2 | |
| Socket bed disconnection alarm | 1 | ||
| Battery autonomy | It allows to use the functions of the bed even when you are disconnected from the socket | 1 | |
| Auxiliary Battery | Useful in case the bed runs out of current | 1 | |
| Accessories | |||
| Bed flexibility to accommodate different types of accessories | IV pole integrated into the bed and adaptable | 4 | |
| IV pole | |||
| IV pole | Comfortable and useful | 4 | |
| Integrated into the bed and adaptable | It can be used while on the move | 5 | |
| Robust | It would solve the problem of poles breaking too easily | 2 | |
| Attack for diuresis | |||
| Raised or adjustable connection | It would solve the problem of the pockets that touch the ground | 6 | |
| Support surfaces | |||
| Integrated support surface to support the instrumentation | 4 | ||
| storage compartment | |||
| Integrated | 4 | ||
| Restraint anchors | |||
| Integrated | Comfortable and remove the risk of harm to the patient | 4 | |
| Mattress | |||
| Adequate size to the bed | To cover empty spaces and prevent them from slipping | 4 | |
| Triangle pole | |||
| Removable | It would reduce the danger to the patient when this tool is not needed | 3 | |
| Headrest | |||
| Integrated | Help for patient hygiene but also an element of comfort | 2 | |
| Bed-wall spacer | |||
| Integrated | It would avoid bumps | 2 | |
| Blankets Lifter | |||
| Integrated | 3 | ||
| Electrically adjustable | 2 | ||
| Bumper wheels | |||
| Space-saving | 1 | ||
| Armrest | |||
| Integrated | 1 | ||
| Connection for the Anti-decubitus mattress | |||
| Integrated | 1 | ||
| Bed-stretcher transfer system | |||
| Systems to facilitate the movement of the patient from the bed and stretcher | They should avoid the empty space between the two | 5 | |
| Bed Base | |||
| Flexible | It would help with regards to the use of the patient lift trolley | 1 | |
| Bed Height | |||
| Ability to adjust the height | Indispensable for comfort and operator facilitation | 9 | |
| Minimum height | Important for patient safety | 2 | |
| Quite wide height adjustment range | 4 | ||
| Increased height adjustment speed | Pro: it helps the staff work Cons: may confuse the patient | 2 | |
| Automatic height adjustment | 1 | ||
| Autonomous height adjustment by the patient | Psychologically it makes the patient feel more involved | 1 | |
| Patient Postural Management | |||
| Handling support | Reduce patient discomfort | 1 | |
| An element of peace of mind for the operators | Adapt the tool to your needs | 1 | |
| Inclinometer | |||
| Useful | 0 ° indication | 1 | |
| Position | At the foot part of the bed | 1 | |
| Inclination of the entire bed | Avoid slipping (Trendelenburg) | 1 | |
| Degrees of inclination | Ability to accurately set the inclination, visible degrees (not just 30 °) | 1 | |
| Reliability | No ball, light by degrees of inclination | 1 | |
| Sections | |||
| Increase number | Adaptable to different stature, multiple postures, patient comfort | 3 | |
| Handling | Reduces fatigue, promotes patient independence | 3 | |
| Increase movement speed | Usage time reduction | 6 | |
| Accompanied movements | Avoid patient disorientation | 2 | |
| Trendelenburg | |||
| Useful | 4 | ||
| Patient movement | Towards the headboard or footboard, solve the sliding problem, reduction of staff fatigue | 4 | |
| Automatic | Automatic patient repositioning | 1 | |
| Minimum height | 1 | ||
| Side tilt | |||
| Lateral patient repositioning | Prevent pressure sores, facilitate the insertion of aids | 5 | |
| Fohler | |||
| Patient feeding | It favors autonomy and comfort | 5 | |
| Bed exit support | |||
| Method for straightening patient | 2 | ||
| Allow sitting position | Therapy, patient comfort, operator convenience | 3 | |
| Posture Alarm | |||
| Posture alarm | Report the need for posturing to staff | 1 | |
| Proposals for new functions | |||
| Standard | Preset position reset, via a button | 1 | |
| Electric leg movement | 1 | ||
| Wave movement of the sections | Patient re-positioning | 1 | |
| Bed Commands | |||
| Push-button panel integrated into the sides | Avoid wire stuck in the sides, avoid frequent falls (breakage of hooks) | 3 | |
| Patient control lock | Maintain posture for therapy | 4 | |
| Magnetic coupling | 1 | ||
| Unified tool | Same remote control for operator and patient, same remote control for all beds | 1 | |
| Wireless | 2 | ||
| Usable with feet | Avoid problem of busy hands | 1 | |
| Vocal commands | Hygiene | 1 | |
| Touch control panel | Avoid fret wear | 1 | |
| Controls on mobile app | 1 | ||
| Buttons | |||
| Easy to use | 5 | ||
| Intuitive | Lighter icons, help | 5 | |
| Familiars | Referable to a domestic context, highlighting potential bed | 1 | |
| Reliable | 2 | ||
| Readable | 1 | ||
| Big | 1 | ||
| Soft | 1 | ||
| Not too flat | 2 | ||
| Wear resistant | 3 | ||
| Command speed | Too slow | 2 | |
| Reduce number of keys per patient | 3 | ||
| Keyboard backlight | It does not have to bother | 2 | |
| Improve remote control grip | 3 | ||
| Sound feedback on pressure | 3 | ||
| Button panel materials | |||
| Wear resistant | Icon color, shock resistant | 3 | |
| Resistant to disinfectants | 1 | ||
| Rubber cover | 2 | ||
| Cleanable | 1 | ||
| Button panel functions | |||
| Distinction between operator and patient commands | 2 | ||
| Reduced number of commands per patient | 2 | ||
| Possibility of customization | 1 | ||
| Ability to use multiple functions at the same time | 3 | ||
| Replaceable | In case of maintenance | 1 | |
| Nurse Call | |||
| Microphone to speak to the guardhouse | Understanding call priorities, avoiding unnecessary interventions | 2 | |
| Video/monitor | 1 | ||
| Vocal command | 1 | ||
| Integrated | 1 | ||
| Urgency alarm for operators | 1 | ||
| Patient Parameters | |||
| Parameter monitoring through integrated tools | 5 | ||
| Integrated monitor | View vital signs | 4 | |
| Integrated scale (weighing) | 2 | ||
| Catheter bag weight sensor | 3 | ||
| Patient parameter alarms | |||
| Bed exit | 4 | ||
| Agitated patient | 1 | ||
| Bed Size | |||
| Extendable bed (or bed extension) | Adapt to the patient’s height | 8 | |
| Larger beds | Increase patient comfort, especially for obese patients | 4 | |
| Adaptable width (or bed spreader) | 1 | ||
| Narrower bed | To facilitate movement | 2 | |
| Avoid incompatibility between bed and mattress | Avoid gaps and reduce mattress wear | 4 | |
| Bed Weight | |||
| Minimized | Encourage travel | 8 | |
| Lightweight removable components | 1 | ||
| Importance of the weight lifted by the bed | Easier to lift heavy patients | 4 | |
| Maneuverability | |||
| Bed size proportionate to the environment (doors) | 1 | ||
| Lighter bed promotes maneuverability | 5 | ||
| Weight helps for displacements | 1 | ||
| Wheels | |||
| Improve maneuverability | 6 | ||
| Improve wear resistance | 1 | ||
| Double driving mode | Lock front wheel rotation | 1 | |
| Retractable wheels | Lower height, less hospital look | 2 | |
| Addition of a motorized wheel | Travel support | 2 | |
| Shockproof material | Comfort | 1 | |
| Brakes | |||
| Possibility of locking all the wheels with a single brake | 2 | ||
| Brake accessible for operator | 1 | ||
| Materials | |||
| Smooth | 2 | ||
| Robust | 7 | ||
| Easy to clean | 10 | ||
| Plastics | 4 | ||
| Light | For removable components | 1 | |
| Wear-resistant paints | For patient safety and aesthetic factor | 5 | |
| Reduce edges and cracks for hygiene | 4 | ||
| Maintenance | |||
| Manual controls in case of failure | To be able to use the bed in an emergency | 9 | |
| Ability to remove individual components for maintenance | Avoid replacing the entire bed in case of maintenance | 3 | |
| Maintenance alarms | |||
| Malfunctioning sensor | Failure reporting | 1 | |
| Automatic alarm in case of failure | Automatic call for assistance | 1 | |
| Aesthetics | |||
| Domestic look, less hospital | Patient comfort, familiar look | 4 | |
| Modern look | 1 | ||
| Roundish | 1 | ||
| Hidden mechanical parts | 1 | ||
| Retractable wheels | 1 | ||
| Colorful or oddly shaped beds for children | 4 | ||
| Colors | |||
| Warm and relaxing | Avoid strong colors | 8 | |
| Shades of color | 1 | ||
| Color that integrates with the room | 2 | ||
| Faux wood | 6 | ||
| White color (avoid) | Cons: More prone to getting dirty | 2 | |
| Lights | |||
| Night light | Patient wellbeing, support for operators | 5 | |
| Courtesy light | 2 | ||
| Catheter bag illumination | 2 | ||
| Bed exit light | 3 | ||
| Interior lights | More domestic and welcoming environment | 2 | |
| Low intensity lights | Avoid disturbing patients | 4 | |
| Patient Relaxation | |||
| Screen for video calls | 1 | ||
| Integrated TV stand | 1 | ||
| Integrated audio system | 4 | ||
| Intercom for children | 1 |
References
- Feder, S. The Surprising Origins of the Modern Hospital Bed—Scopes. Available online: https://www.zocdoc.com/blog/the-surprising-origins-of-the-modern-hospital-bed/ (accessed on 7 November 2022).
- Yeom, H.; Park, C.H.; Park, S. Medical Bed with Integrated Toilet: Design Considerations and Utilization by a Bedridden Patient. Health Technol. 2019, 9, 903–907. [Google Scholar] [CrossRef]
- Kim, J.; Lee, Y.; Seon, M.; Lim, J.-Y. The Medical Bed System for Preventing Pressure Ulcer Using the Two-Stage Control. Int. J. Adv. Smart Converg. 2021, 10, 151–158. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, H. Design and Application of a Medical Bed and Its Bedside Angle Measuring Device. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2019, 31, 493–494. [Google Scholar] [PubMed]
- Guo, Z.; Xiao, X.; Yu, H. Design and Evaluation of a Motorized Robotic Bed Mover with Omnidirectional Mobility for Patient Transportation. IEEE J. Biomed. Health Inform. 2018, 22, 1775–1785. [Google Scholar] [CrossRef] [PubMed]
- Dix, A.; Finlay, J.; Abowd, G.D.; Beale, R. Human-Computer Interaction: Pearson Prentice Hall; Prentice Hall Inc.: London, UK, 2004. [Google Scholar]
- Park, H.; McKilligan, S. A Systematic Literature Review for Human-Computer Interaction and Design Thinking Process Integration. In Design, User Experience, and Usability: Theory and Practice, Proceedings of the 7th International Conference, DUXU 2018, Held as Part of HCI International 2018, Las Vegas, NV, USA, 15–20 July 2018; Marcus, A., Wang, W., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 725–740. [Google Scholar]
- Nielsen, J. Ten Usability Heuristics. 2020. Available online: https://www.nngroup.com/articles/ten-usability-heuristics (accessed on 27 November 2022).
- Henderson, A. Interaction Design: Beyond Human-Computer Interaction. Ubiquity 2002, 2002, 2. [Google Scholar] [CrossRef]
- Caputo, F.; Greco, A.; D’Amato, E.; Notaro, I.; Spada, S. On the Use of Virtual Reality for a Human-Centered Workplace Design. Procedia Struct. Integr. 2018, 8, 297–308. [Google Scholar] [CrossRef]
- Adam, M.; McMahon, S.A.; Prober, C.; Bärnighausen, T. Human-Centered Design of Video-Based Health Education: An Iterative, Collaborative, Community-Based Approach. J. Med. Internet Res. 2019, 21, e12128. [Google Scholar] [CrossRef] [PubMed]
- Mincolelli, G.; Giacobone, G.A.; Marchi, M. Project PLEINAIR: Discovering User Needs Exploring a Non-Conventional Human-Centered Approach. In Advances in Industrial Design, Proceedings of the International Conference on Applied Human Factors and Ergonomics, Manhattan, NY, USA, 25–29 July 2021; Shin, C.S., Di Bucchianico, G., Fukuda, S., Ghim, Y.-G., Montagna, G., Carvalho, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 363–370. [Google Scholar]
- Ong, A.; Troncoso, J.; Yeung, A.; Kim, E.; Agogino, A.M. Towards Flexible Ridesharing Experiences: Human-Centered Design of Segmented Shared Spaces. In HCI International 2019—Posters, Proceedings of the 21st International Conference, HCII 2019, Orlando, FL, USA, 26–31 July 2019; Stephanidis, C., Ed.; Springer International Publishing: Cham, Switzerland, 2019; pp. 373–380. [Google Scholar]
- Giacobone, G.A.; Mincolelli, G. Human-Centered Design and Quality Function Deployment: Understanding Needs on a Multidisciplinary Automotive Research. In Advances in Design for Inclusion, Proceedings of the AHFE 2019 International Conference on Design for Inclusion and the AHFE 2019 International Conference on Human Factors for Apparel and Textile Engineering, Washington, DC, USA, 24–28 July 2019; Di Bucchianico, G., Ed.; Springer International Publishing: Cham, Switzerland, 2020; pp. 57–68. [Google Scholar]
- Volkmann, T.; Sengpiel, M.; Jochems, N. Historytelling: A Website for the Elderly A Human-Centered Design Approach. In Proceedings of the 9th Nordic Conference on Human-Computer Interaction; Association for Computing Machinery, New York, NY, USA, 23–27 October 2016; pp. 1–6. [Google Scholar]
- Bacchin, D.; Pluchino, P.; Grippaldi, A.Z.; Mapelli, D.; Spagnolli, A.; Zanella, A.; Gamberini, L. Smart Co-Housing for People With Disabilities: A Preliminary Assessment of Caregivers’ Interaction With the DOMHO System. Front. Psychol. 2021, 12, 734180. [Google Scholar] [CrossRef]
- Harte, R.; Glynn, L.; Rodríguez-Molinero, A.; Baker, P.M.; Scharf, T.; Quinlan, L.R.; ÓLaighin, G. A Human-Centered Design Methodology to Enhance the Usability, Human Factors, and User Experience of Connected Health Systems: A Three-Phase Methodology. JMIR Hum. Factors 2017, 4, e5443. [Google Scholar] [CrossRef]
- Bazzano, A.N.; Martin, J.; Hicks, E.; Faughnan, M.; Murphy, L. Human-Centred Design in Global Health: A Scoping Review of Applications and Contexts. PLoS ONE 2017, 12, e0186744. [Google Scholar] [CrossRef]
- Kirch, J.; Marquardt, G. Towards Human-Centred General Hospitals: The Potential of Dementia-Friendly Design. Archit. Sci. Rev. 2021, 1–9. [Google Scholar] [CrossRef]
- Cawood, T.; Saunders, E.; Drennan, C.; Cross, N.; Nicholl, D.; Kenny, A.; Meates, D.; Laing, R. Creating the Optimal Workspace for Hospital Staff Using Human Centred Design. Intern. Med. J. 2016, 46, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Parreira, P.; Sousa, L.B.; Marques, I.A.; Costa, P.; Cortez, S.; Carneiro, F.; Cruz, A.; Salgueiro-Oliveira, A. Development of an Innovative Double-Chamber Syringe for Intravenous Therapeutics and Flushing: Nurses’ Involvement through a Human-Centred Approach. PLoS ONE 2020, 15, e0235087. [Google Scholar] [CrossRef] [PubMed]
- Beede, E.; Baylor, E.; Hersch, F.; Iurchenko, A.; Wilcox, L.; Ruamviboonsuk, P.; Vardoulakis, L.M. A Human-Centered Evaluation of a Deep Learning System Deployed in Clinics for the Detection of Diabetic Retinopathy. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25–30 April 2020; Association for Computing Machinery: New York, NY, USA, 2020; pp. 1–12. [Google Scholar]
- Martin, J.L.; Clark, D.J.; Morgan, S.P.; Crowe, J.A.; Murphy, E. A User-Centred Approach to Requirements Elicitation in Medical Device Development: A Case Study from an Industry Perspective. Appl. Ergon. 2012, 43, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Poncette, A.-S.; Spies, C.; Mosch, L.; Schieler, M.; Weber-Carstens, S.; Krampe, H.; Balzer, F. Clinical Requirements of Future Patient Monitoring in the Intensive Care Unit: Qualitative Study. JMIR Med. Inform. 2019, 7, e13064. [Google Scholar] [CrossRef] [Green Version]
- Nodooshan, H.S.; Choobineh, A.; Razeghi, M.; Khales, T.S.N. Designing, Prototype Making and Evaluating a Mechanical Aid Device for Patient Transfer between Bed and Stretcher. Int. J. Occup. Saf. Ergon. 2017, 23, 491–500. [Google Scholar] [CrossRef]
- Kuroda, T.; Noma, H.; Naito, C.; Tada, M.; Yamanaka, H.; Takemura, T.; Nin, K.; Yoshihara, H. Prototyping Sensor Network System for Automatic Vital Signs Collection. Methods Inf. Med. 2013, 52, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Schertz, J.; Worton, H. Nurse Evaluation of the Redesigned Fertility Pen Injector: A Questionnaire-Based Observational Survey. Expert Opin. Drug Deliv. 2018, 15, 435–442. [Google Scholar] [CrossRef]
- Parreira, P.; Sousa, L.B.; Marques, I.A.; Santos-Costa, P.; Cortez, S.; Carneiro, F.; Cruz, A.; Salgueiro-Oliveira, A. Usability Assessment of an Innovative Device in Infusion Therapy: A Mix-Method Approach Study. Int. J. Environ. Res. Public Health 2020, 17, 8335. [Google Scholar] [CrossRef]
- Matinolli, H.-M.; Mieronkoski, R.; Salanterä, S. Health and Medical Device Development for Fundamental Care: Scoping Review. J. Clin. Nurs. 2020, 29, 1822–1831. [Google Scholar] [CrossRef]
- Ghersi, I.; Mariño, M.; Miralles, M.T. From Modern Push-Button Hospital-Beds to 20th Century Mechatronic Beds: A Review. In Journal of Physics: Conference Series, Volume 705, Proceedings of the 20th Argentinean Bioengineering Society Congress, SABI 2015 (XX Congreso Argentino de Bioingeniería y IX Jornadas de Ingeniería Clínica), San Nicolás de los Arroyos, Argentina, 28–30 October 2015; IOP Publishing: Bristol, UK, 2016; Volume 705, p. 012054. [Google Scholar]
- Ghersi, I.; Mariño, M.; Miralles, M.T. Smart Medical Beds in Patient-Care Environments of the Twenty-First Century: A State-of-Art Survey. BMC Med. Inform. Decis. Mak. 2018, 18, 63. [Google Scholar] [CrossRef] [PubMed]
- Who Invented Medical Beds—Medical Beds. Available online: http://www.medical-beds.co.uk/who-invented-medical-beds.html (accessed on 20 November 2022).
- Wiggermann, N.; Rempel, K.; Zerhusen, R.M.; Pelo, T.; Mann, N. Human-Centered Design Process for a Hospital Bed: Promoting Patient Safety and Ease of Use. Ergon. Des. 2019, 27, 4–12. [Google Scholar] [CrossRef] [Green Version]
- LeLaurin, J.H.; Shorr, R.I. Preventing Falls in Hospitalized Patients: State of the Science. Clin. Geriatr. Med. 2019, 35, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Hilbe, J.; Schulc, E.; Linder, B.; Them, C. Development and Alarm Threshold Evaluation of a Side Rail Integrated Sensor Technology for the Prevention of Falls. Int. J. Med. Inform. 2010, 79, 173–180. [Google Scholar] [CrossRef]
- Wolf, K.-H.; Hetzer, K.; Zu Schwabedissen, H.M.; Wiese, B.; Marschollek, M. Development and Pilot Study of a Bed-Exit Alarm Based on a Body-Worn Accelerometer. Z. Gerontol. Geriat. 2013, 46, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Wiggermann, N. Ergonomic Evaluation of Brake Pedal and Push Handle Locations on Hospital Beds. Appl. Ergon. 2017, 60, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Wiggermann, N. The Effects of Hospital Bed Features on Physical Stresses on Caregivers When Repositioning Patients in Bed. Appl. Ergon. 2021, 90, 103259. [Google Scholar] [CrossRef]
- Petzäll, K.; Berglund, B.; Lundberg, C. The Staff’s Satisfaction with the Hospital Bed. J. Nurs. Manag. 2001, 9, 51–57. [Google Scholar] [CrossRef]
- Cai, H.; Krebs, H.J.; Tao, Y.; Hansen, J.; Pan, R.; Cai, Y.; Toft, E.; Dinesen, B. A Qualitative Study on Implementation of the Intelligent Bed: Findings from a Rehabilitation Ward at a Large Chinese Tertiary Hospital. Wirel. Pers. Commun. 2016, 90, 399–420. [Google Scholar] [CrossRef]
- Esengün, G.G.; Alppay, E.C. A Study on Examining User Comfort in Hospital Beds. In Advances in Ergonomics in Design, Proceedings of the AHFE 2017 International Conference on Applied Human Factors and Ergonomics, Los Angeles, CA, USA, 17−21 July 2017; Rebelo, F., Soares, M., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 885–896. [Google Scholar]
- Soonthornkiti, S.; Jearanaisilawong, P. Design of Anti-Bedsore Hospital Bed. J. Res. Appl. Mech. Eng. 2013, 1, 15–20. [Google Scholar]
- Mehta, R.K.; Horton, L.M.; Agnew, M.J.; Nussbaum, M.A. Ergonomic Evaluation of Hospital Bed Design Features during Patient Handling Tasks. Int. J. Ind. Ergon. 2011, 41, 647–652. [Google Scholar] [CrossRef]
- Kim, S.; Barker, L.M.; Jia, B.; Agnew, M.J.; Nussbaum, M.A. Effects of Two Hospital Bed Design Features on Physical Demands and Usability during Brake Engagement and Patient Transportation: A Repeated Measures Experimental Study. Int. J. Nurs. Stud. 2009, 46, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Jia, B.; Barker, L.M.; Kim, S.; Agnew, M.J.; Nussbaum, M.A. Ergonomic Design in Hospital Beds: Comparison of Brake Pedal Design and Steering-Assistance Features. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2008, 52, 1040–1044. [Google Scholar] [CrossRef]
- Alenezi, A.M.; Aboshaiqah, A.; Baker, O. Work-Related Stress among Nursing Staff Working in Government Hospitals and Primary Health Care Centres. Int. J. Nurs. Pract. 2018, 24, e12676. [Google Scholar] [CrossRef] [PubMed]
- Kakemam, E.; Raeissi, P.; Raoofi, S.; Soltani, A.; Sokhanvar, M.; Visentin, D.C.; Cleary, M. Occupational Stress and Associated Risk Factors among Nurses: A Cross-Sectional Study. Contemp. Nurse 2019, 55, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, A.G.; Shepperd, J. The Use of Focus Groups in Health Research. Scand. J. Prim. Health Care Suppl. 1988, 1, 81–90. [Google Scholar]
- Maguire, M.; Delahunt, B. Doing a Thematic Analysis: A Practical, Step-by-Step Guide for Learning and Teaching Scholars. All Irel. J. High. Educ. 2017, 9, 3351–3354. [Google Scholar]
- Shieh, S.-H.; Sung, F.-C.; Su, C.-H.; Tsai, Y.; Hsieh, V.C.-R. Increased Low Back Pain Risk in Nurses with High Workload for Patient Care: A Questionnaire Survey. Taiwan. J. Obstet. Gynecol. 2016, 55, 525–529. [Google Scholar] [CrossRef] [Green Version]
- Diehl, E.; Rieger, S.; Letzel, S.; Schablon, A.; Nienhaus, A.; Pinzon, L.C.E.; Dietz, P. The Relationship between Workload and Burnout among Nurses: The Buffering Role of Personal, Social and Organisational Resources. PLoS ONE 2021, 16, e0245798. [Google Scholar] [CrossRef]
- Asamani, J.A.; Amertil, N.P.; Chebere, M. The Influence of Workload Levels on Performance in a Rural Hospital. Br. J. Healthc. Manag. 2015, 21, 577–586. [Google Scholar] [CrossRef]
- Sjöberg, A.; Pettersson-Strömbäck, A.; Sahlén, K.-G.; Lindholm, L.; Norström, F. The Burden of High Workload on the Health-Related Quality of Life among Home Care Workers in Northern Sweden. Int. Arch. Occup. Environ. Health 2020, 93, 747–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umansky, J.; Rantanen, E. Workload in Nursing. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2016, 60, 551–555. [Google Scholar] [CrossRef]
- Reed, L.; Fisher, J. A Comparison of the Opinions of Nurses and Emergency Medical Workers Regarding Medical Device Usability. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2002, 46, 1477–1481. [Google Scholar] [CrossRef]
- Nuamah, J.K.; Mehta, R.K. Chapter 11—Design for Stress, Fatigue, and Workload Management. In Design for Health; Sethumadhavan, A., Sasangohar, F., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 201–226. ISBN 978-0-12-816427-3. [Google Scholar]
- Lin, X.; Zhang, Z. Designing Remote Control of Medical Bed Based on Human Factors. In Proceedings of the 2020 IEEE 7th International Conference on Industrial Engineering and Applications (ICIEA), Bangkok, Thailand, 16–21 April 2020; pp. 838–841. [Google Scholar]
- Horton, L.M.; Mehta, R.K.; Kim, S.; Agnew, M.J.; Nussbaum, M.A. Effects of Alternative Hospital Bed Design Features on Physical Demands. IIE Annu. Conf. Proc. 2009, 937–942. [Google Scholar]
- Suresh, M.; Roobaswathiny, A.; Priyadarsini, S.L. A Study on the Factors That Influence the Agility of COVID-19 Hospitals. Int. J. Healthc. Manag. 2021, 14, 290–299. [Google Scholar] [CrossRef]
- Goh, C.H.; Muslimah, Y.; Ng, S.-C.; Subramanian, P.; Tan, M.P. The Use of the Self-Standing Turning Transfer Device to Perform Bed-To-Chair Transfers Reduces Physical Stress among Caregivers of Older Patients in a Middle-Income Developing Country. Front. Med. 2014, 1, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hignett, S.; Griffiths, P. Do Split-Side Rails Present an Increased Risk to Patient Safety? BMJ Qual. Saf. 2005, 14, 113–116. [Google Scholar] [CrossRef] [Green Version]
- Babatabar-Darzi, H.; Jafari-Iraqi, I.; Mahmoudi, H.; Ebadi, A. Overcrowding Management and Patient Safety: An Application of the Stabilization Model. Iran. J. Nurs. Midwifery Res. 2020, 25, 382–386. [Google Scholar] [CrossRef]
- Morse, J.M.; Gervais, P.; Pooler, C.; Merryweather, A.; Doig, A.K.; Bloswick, D. The Safety of Hospital Beds: Ingress, Egress, and In-Bed Mobility. Glob. Qual. Nurs. Res. 2015, 2, 2333393615575321. [Google Scholar] [CrossRef] [Green Version]
- Yasuhara, H.; Fukatsu, K.; Komatsu, T.; Obayashi, T.; Saito, Y.; Uetera, Y. Prevention of Medical Accidents Caused by Defective Surgical Instruments. Surgery 2012, 151, 153–161. [Google Scholar] [CrossRef]
- Taylor, M.L.; Thomas, E.E.; Snoswell, C.L.; Smith, A.C.; Caffery, L.J. Does Remote Patient Monitoring Reduce Acute Care Use? A Systematic Review. BMJ Open 2021, 11, e040232. [Google Scholar] [CrossRef] [PubMed]
- Poncette, A.-S.; Mosch, L.; Spies, C.; Schmieding, M.; Schiefenhövel, F.; Krampe, H.; Balzer, F. Improvements in Patient Monitoring in the Intensive Care Unit: Survey Study. J. Med. Internet Res. 2020, 22, e19091. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, M. Improving Patient Safety by Reducing Falls in Hospitals Among the Elderly: A Review of Successful Strategies. ICIMTH 2019, 262, 340–343. [Google Scholar]
- Bacchin, D.; Pernice, G.F.A.; Sardena, M.; Malvestio, M.; Gamberini, L. Caregivers’ Perceived Usefulness of an IoT-Based Smart Bed. In Distributed, Ambient and Pervasive Interactions. Smart Environments, Ecosystems, and Cities, Proceedings of the 10th International Conference, DAPI 2022, Held as Part of the 24th HCI International Conference, HCII 2022, Virtual Event, 26 June–1 July 2022; Proceedings, Part I.; Springer: Berlin/Heidelberg, Germany, 2022; pp. 247–265. [Google Scholar]
- Rus, S.; Grosse-Puppendahl, T.; Kuijper, A. Evaluating the Recognition of Bed Postures Using Mutual Capacitance Sensing. J. Ambient. Intell. Smart Environ. 2017, 9, 113–127. [Google Scholar] [CrossRef]
- Matar, G.; Lina, J.-M.; Kaddoum, G. Artificial Neural Network for In-Bed Posture Classification Using Bed-Sheet Pressure Sensors. IEEE J. Biomed. Health Inform. 2020, 24, 101–110. [Google Scholar] [CrossRef]
- Votruba, L.; Graham, B.; Wisinski, J.; Syed, A. Video Monitoring to Reduce Falls And Patient Companion Costs For Adult Inpatients. Nurs. Econ. 2016, 34, 185–189. [Google Scholar]
- Cournan, M.; Fusco-Gessick, B.; Wright, L. Improving Patient Safety through Video Monitoring. Rehabil. Nurs. 2018, 43, 111–115. [Google Scholar] [CrossRef]
- Kumar, N.; Panda, S.; Pradhan, P.; Kaushal, R. IoT Based Hybrid System for Patient Monitoring and Medication. EAI Endorsed Trans. Pervasive Health Technol. 2019, 5, e1. [Google Scholar] [CrossRef]
- Rahaman, A.; Islam, M.M.; Islam, M.R.; Sadi, M.S.; Nooruddin, S. Developing IoT Based Smart Health Monitoring Systems: A Review. Rev. d’Intelligence Artif. 2019, 33, 435–440. [Google Scholar] [CrossRef] [Green Version]
- Awais, M.; Raza, M.; Ali, K.; Ali, Z.; Irfan, M.; Chughtai, O.; Khan, I.; Kim, S.; Ur Rehman, M. An Internet of Things Based Bed-Egress Alerting Paradigm Using Wearable Sensors in Elderly Care Environment. Sensors 2019, 19, 2498. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-N.; Yang, S.-C.; Li, C.-K.; Liu, M.-Z.; Kuo, P.-C. Alarm System For Bed Exit And Prolonged Bed Rest. In Proceedings of the 2018 International Conference on Machine Learning and Cybernetics (ICMLC), Chengdu, China, 15–18 July 2018; Volume 2, pp. 439–443. [Google Scholar]
- Lee, Y.-L.; Chang, M.-C.; Chang, C.-L.; Chi, W.-Y. Validation of Agitated Patient Remote Monitoring Alarm System in the Intensive Care Unit. Stud. Health Technol. Inform. 2021, 284, 365–366. [Google Scholar] [CrossRef] [PubMed]
- Muñiz, R.; Díaz, J.; Martínez, J.A.; Nuño, F.; Bobes, J.; García-Portilla, M.P.; Sáiz, P.A. A Smart Band for Automatic Supervision of Restrained Patients in a Hospital Environment. Sensors 2020, 20, 5211. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, J. The Cause of Pressure Sores. In Prevention of Pressure Sores; CRC Press: Boca Raton, FL, USA, 1991; ISBN 978-0-367-81154-9. [Google Scholar]
- Carling, P.C. Optimizing Health Care Environmental Hygiene. Infect. Dis. Clin. 2016, 30, 639–660. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Sullivan, N.; Leas, B.F.; Pegues, D.A.; Kaczmarek, J.L.; Umscheid, C.A. Cleaning Hospital Room Surfaces to Prevent Health Care–Associated Infections: A Technical Brief. Ann. Intern. Med. 2015, 163, 598–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capolongo, S.; Gola, M.; Brambilla, A.; Morganti, A.; Mosca, E.I.; Barach, P. COVID-19 and Healthcare Facilities: A Decalogue of Design Strategies for Resilient Hospitals. Acta Biomed. 2020, 91, 50–60. [Google Scholar] [CrossRef]
- Xu, X.; Luo, M.; He, P.; Yang, J. Washable and Flexible Screen Printed Graphene Electrode on Textiles for Wearable Healthcare Monitoring. J. Phys. D Appl. Phys. 2020, 53, 125402. [Google Scholar] [CrossRef]
- Yang, C.Q. Elderly Home Nursing Bed Design. Adv. Mater. Res. 2012, 482–484, 643–646. [Google Scholar] [CrossRef]
- Levinson, R.; Salas, L.; Zanca, J.M. The Experience of Using a Hospital Bed Alternative at Home among Individuals with Spinal Cord Injury: A Case Series. J. Spinal Cord Med. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sobrino, J.A. Less and Better. Elements to Achieve Excellence in Bridge Design. Struct. Eng. Int. 2021, 31, 610–613. [Google Scholar] [CrossRef]
- Lombardo, V.; Vinatier, I.; Baillot, M.-L.; Franja, V.; Bourgeon-Ghittori, I.; Dray, S.; Jeune, S.; Mossadegh, C.; Reignier, J.; Souweine, B.; et al. How Caregivers View Patient Comfort and What They Do to Improve It: A French Survey. Ann. Intensive Care 2013, 3, 19. [Google Scholar] [CrossRef] [Green Version]
- Gillick, M.R. The Critical Role of Caregivers in Achieving Patient-Centered Care. JAMA 2013, 310, 575–576. [Google Scholar] [CrossRef] [PubMed]
- Bacchin, D.; Pluchino, P.; Orso, V.; Sardena, M.; Malvestio, M.; Gamberini, L. Development and Testing of a Usability Checklist for the Evaluation of Control Interfaces of Electrical Medical Beds. In Digital Human Modeling and Applications in Health, Safety, Ergonomics and Risk Management. AI, Product and Service, Proceedings of the 12th International Conference, DHM 2021, Held as Part of the 23rd HCI International Conference, HCII 2021, Virtual Event, 24–29 July 2021; Duffy, V.G., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 3–19. [Google Scholar]
- Jaffar, N.; Abdul-Tharim, A.H.; Mohd-Kamar, I.F.; Lop, N.S. A Literature Review of Ergonomics Risk Factors in Construction Industry. Procedia Eng. 2011, 20, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Tao, D.; Yuan, J.; Liu, S.; Qu, X. Effects of Button Design Characteristics on Performance and Perceptions of Touchscreen Use. Int. J. Ind. Ergon. 2018, 64, 59–68. [Google Scholar] [CrossRef]
- Yeh, P.; Hsu, Y. Operation of Button Feedback Design within TV Remote Control Applications for Middle-Aged and Older Adult. J. Soc. Inf. Disp. 2021, 29, 247–253. [Google Scholar] [CrossRef]
- Gelsema, T.I.; van der Doef, M.; Maes, S.; Janssen, M.; Akerboom, S.; Verhoeven, C. A Longitudinal Study of Job Stress in the Nursing Profession: Causes and Consequences. J. Nurs. Manag. 2006, 14, 289–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurses, A.P.; Carayon, P. Exploring Performance Obstacles of Intensive Care Nurses. Appl. Ergon. 2009, 40, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Sauer, J.; Sonderegger, A.; Schmutz, S. Usability, User Experience and Accessibility: Towards an Integrative Model. Ergonomics 2020, 63, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Bitkina, O.V.; Kim, H.K.; Park, J. Usability and User Experience of Medical Devices: An Overview of the Current State, Analysis Methodologies, and Future Challenges. Int. J. Ind. Ergon. 2020, 76, 102932. [Google Scholar] [CrossRef]
- Bevan, N.; Carter, J.; Harker, S. ISO 9241-11 Revised: What Have We Learnt about Usability since 1998? In Human-Computer Interaction: Design and Evaluation, Proceedings of the 17th International Conference on Human-Computer Interaction 2015, Los Angeles, CA, USA, 2–7 August 2015; Springer: Cham, Switzerland, 2015; pp. 143–151. [Google Scholar]
- 14:00–17:00 ISO/IEC DIS 25010. Available online: https://www.iso.org/standard/78176.html (accessed on 22 November 2022).
- Kucukusta, D.; Law, R.; Besbes, A.; Legohérel, P. Re-Examining Perceived Usefulness and Ease of Use in Online Booking: The Case of Hong Kong Online Users. Int. J. Contemp. Hosp. Manag. 2015, 27, 185–198. [Google Scholar] [CrossRef]
- SO 9241-171:2008. Available online: https://www.iso.org/standard/39080.html (accessed on 23 November 2022).
- Feinberg, S.; Murphy, M. Applying Cognitive Load Theory to the Design of Web-Based Instruction. In Proceedings of the 18th Annual Conference on Computer Documentation. ipcc sigdoc 2000, Technology and Teamwork, Proceedings, IEEE Professional Communication Society International Professional Communication Conference and ACM Special Interest Group on Documentation Conference, Cambridge, MA, USA, 24–27 September 2000; pp. 353–360. [Google Scholar]
- Lah, U.; Lewis, J.R.; Šumak, B. Perceived Usability and the Modified Technology Acceptance Model. Int. J. Hum.–Comput. Interact. 2020, 36, 1216–1230. [Google Scholar] [CrossRef]
- Vermeeren, A.; Kort, J.; Cremers, A.; Fokker, J. Comparing UX Measurements, a Case Study. In Proceedings of the International Workshop on Meaningful Measures: Valid Useful Experience Measurement, Reykjavik, Iceland, 18 June 2008; Volume 18, pp. 72–78. [Google Scholar]
- Tcha-Tokey, K.; Christmann, O.; Loup-Escande, E.; Richir, S. Proposition and Validation of a Questionnaire to Measure the User Experience in Immersive Virtual Environments. Int. J. Virtual Real. 2016, 16, 33–48. [Google Scholar] [CrossRef]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FG Code | Current Work Organization | Age | Gender | Healthcare Experience (years) | Past Experience in Different Healthcare Facilities | Electrical Bed Experience (years) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | F | M | Mean | SD | Yes | No | Mean | SD | ||
| FG1 | Hospital | 38.83 | 12.34 | 5 | 1 | 15 | 9.78 | 6 | 0 | 1.5 | 0.55 |
| FG2 | Hospital | 41 | 9.93 | 2 | 2 | 16.8 | 13.62 | 3 | 1 | 15.25 | 9.81 |
| FG3 | Elderly Retirement Home | 41.8 | 7.33 | 4 | 1 | 20.4 | 8.59 | 4 | 1 | 9.4 | 6.84 |
| FG4 | Institution for people with disabilities | 33.6 | 70.69 | 4 | 1 | 8.4 | 5.13 | 1 | 4 | 8.4 | 5.13 |
| FG5 | Hospital | 44 | 8.19 | 2 | 1 | 7 | 7.81 | 3 | 0 | 7 | 7.81 |
| FG6 | Domiciliary home care | 35 | 4.82 | 2 | 4 | 11 | 5.06 | 5 | 1 | 9.33 | 5.65 |
| Safety [97] | Refer to the users’ perception to minimize the levels of risk using the system |
| Comfort [98] | The extent to which the user is satisfied with physical comfort using the system |
| Ease of Use [99] | Refers to the degree to which the user believes s/he can use the system effortlessly |
| Timesaving [100] | The degree to which a person perceived itself as able to accomplish her/his objectives in a reasonable amount of time using the system |
| Workload [101] | The total cognitive load, or amount of mental processing power needed to use a system |
| Perceived Usefulness [102] | The degree to which a person believes that use of a particular system would enhance his or her job performance |
| Flexibility [98] | Measure of the extent to which the system is usable in all potential contexts of use |
| Aesthetic [103] | Refer to the capacity of a system to pleased one or more of our sensory modalities. |
| Reliability [104] | Refer to the users’ perception that the tool assesses the consistency |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bacchin, D.; Pernice, G.F.A.; Pierobon, L.; Zanella, E.; Sardena, M.; Malvestio, M.; Gamberini, L. Co-Design in Electrical Medical Beds with Caregivers. Int. J. Environ. Res. Public Health 2022, 19, 16353. https://doi.org/10.3390/ijerph192316353
Bacchin D, Pernice GFA, Pierobon L, Zanella E, Sardena M, Malvestio M, Gamberini L. Co-Design in Electrical Medical Beds with Caregivers. International Journal of Environmental Research and Public Health. 2022; 19(23):16353. https://doi.org/10.3390/ijerph192316353
Chicago/Turabian StyleBacchin, Davide, Gabriella Francesca Amalia Pernice, Leonardo Pierobon, Elena Zanella, Marcello Sardena, Marino Malvestio, and Luciano Gamberini. 2022. "Co-Design in Electrical Medical Beds with Caregivers" International Journal of Environmental Research and Public Health 19, no. 23: 16353. https://doi.org/10.3390/ijerph192316353