

First-Trimester Biochemical Serum Markers in Female Kidney Transplant Recipients—The Impact of Graft Function
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murray, J.E.; Reid, D.E.; Harrison, J.H.; Merrill, J.P. Successful pregnancies after human renal transplantation. N. Engl. J. Med. 1963, 269, 341–343. [Google Scholar] [CrossRef]
- Transplant Pregnancy Registry International-Gift of Life Institute. 2018 Annual Report. Available online: https://www.transplantpregnancyregistry.org/ (accessed on 11 July 2022).
- Durst, J.K.; Rampersad, R.M. Pregnancy in Women with Solid-Organ Transplants: A Review. Obstet. Gynecol. Surv. 2015, 70, 408–418. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Cabiddu, G.; Attini, R.; Gerbino, M.; Todeschini, P.; Perrino, M.L.; Manzione, A.M.; Piredda, G.B.; Gnappi, E.; Caputo, F.; et al. Outcomes of Pregnancies After Kidney Transplantation: Lessons Learned From CKD. A Comparison of Transplanted, Nontransplanted Chronic Kidney Disease Patients and Low-Risk Pregnancies: A Multicenter Nationwide Analysis. Transplantation 2017, 101, 2536–2544. [Google Scholar] [CrossRef] [PubMed]
- Pandya, P.P.; Snijders, R.J.; Johnson, S.P.; De Lourdes Brizot, M.; Nicolaides, K.H. Screening for fetal trisomies by maternal age and fetal nuchal translucency thickness at 10 to 14 weeks of gestation. Br. J. Obstet. Gynaecol. 1995, 102, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, K.H. Screening for fetal aneuploidies at 11 to 13 weeks. Prenat. Diagn. 2011, 31, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.; Silva, M.; Papadopoulos, S.; Wright, A.; Nicolaides, K.H. Serum pregnancy-associated plasma protein-A in the three trimesters of pregnancy: Effects of maternal characteristics and medical history. Ultrasound Obstet. Gynecol. 2015, 46, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Amiri, F.S. Serum tumor markers in chronic kidney disease: As clinical tool in diagnosis, treatment and prognosis of cancers. Ren. Fail. 2016, 38, 530–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soni, S.; Menon, M.C.; Bhaskaran, M.; Jhaveri, K.D.; Molmenti, E.; Muoio, V. Elevated human chorionic gonadotropin levels in patients with chronic kidney disease: Case series and review of literature. Indian J. Nephrol. 2013, 23, 424–427. [Google Scholar] [PubMed]
- Coskun, A.; Duran, S.; Apaydin, S.; Bulut, I.; Sariyar, M. Pregnancy-associated plasma protein-A: Evaluation of a new biomarker in renal transplant patients. Transplant. Proc. 2007, 39, 3072–3076. [Google Scholar] [CrossRef] [PubMed]
- Kagan, K.O.; Hoopmann, M.; Abele, H.; Alkier, R.; Lüthgens, K. First-trimester combined screening for trisomy 21 with different combinations of placental growth factor, free β-human chorionic gonadotropin and pregnancy-associated plasma protein-A. Ultrasound Obstet. Gynecol. 2012, 40, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Grande, M.; Cararach, V.; Casals, E.; Borrell, A. First-trimester Down syndrome screening in renal-transplanted pregnant women: A model for adjusting the false-positives rates. Prenat. Diagn. 2013, 33, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Cararach, V.; Casals, E.; Martínez, S.; Carmona, F.; Aibar, C.; Quintó, L.I.; Alonso, P.; Fortuny, A. Abnormal renal function as a cause of false-positive biochemical screening for Down’s syndrome. Lancet 1997, 350, 1295. [Google Scholar] [CrossRef] [PubMed]
- Karidas, C.N.; Michailidis, G.D.; Spencer, K.; Economides, D.L. Biochemical screening for Down syndrome in pregnancies following renal transplantation. Prenat. Diagn. 2002, 22, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Spencer, K.; Enofe, O.; Cowans, N.J.; Stamatopoulou, A. Is maternal renal disease a cause of elevated free beta-hCG in first trimester aneuploidy screening? Prenat. Diagn. 2009, 29, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Valentin, M.; Muller, F.; Beaujard, M.P.; Dreux, S.; Czerkiewicz, I.; Meyer, V.; Leruez, M.; Ville, Y.; Salomon, L.J. First-trimester combined screening for trisomy 21 in women with renal disease. Prenat. Diagn. 2015, 35, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Meloni, P.; D’Angeli, I.; Piazze, J.; Cerekya, A.; Simari, T.; Pala, A.; Anceschi, M.M.; Guglietta, M.; Izzo, P.; Izzo, L. First Trimester PAPP-A Levels Associated with Early Prediction of Pregnancy Induced Hypertension. Hypertens. Pregnancy 2009, 28, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Kalousová, M.; Tesaíř, V.; Muravská, A.; Zima, T. Pregnancy-associated plasma protein A: Spotlight on kidney diseases. Clin. Chem. Lab. Med. 2012, 50, 1183–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippone, E.J.; Farber, J.L. The Monitoring of Donor-derived Cell-free DNA in Kidney Transplantation. Transplantation 2021, 105, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Attini, R.; Grati, F.R.; Menato, G.; Todros, T.; Colla, L.; Rossetti, M.; Malvestiti, B.; Alemanno, M.G.; Masturzo, B.; Piccoli, G.B.; et al. Pregnancy on dialysis and with a failing kidney graft: A double challenge for non-invasive prenatal testing. Prenat. Diagn. 2020, 40, 387–389. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Study Group (n = 27) | Control Group (n = 110) | p |
|---|---|---|---|
| Maternal characteristics: | |||
| Age (years) | 35.0 ± 3.5 | 34.1 ± 4.3 | 0.31 |
| BMI (kg/m2) | 24.7 ± 4.2 | 23.9 ± 7.6 | 0.19 |
| Nulliparous (%) | 13 (48.1) | 68 (61.8) | <0.0001 |
| Hypertension before pregnancy (%) | 21 (77.8) | 0 | <0.001 |
| Pregnancy complications: | |||
| Pregnancy-induced hypertension (%) | 6 (22.2) | 9 (8.2) | 0.047 |
| Gestational diabetes (%) | 5 (18.5) | 7 (6.4) | 0.06 |
| Anemia (%) | 11 (40.7) | 11 (10.0) | <0.0001 |
| Proteinuria (%) | 12 (44.4) | 3 (2.7) | <0.0001 |
| Intrahepatic cholestasis (%) | 0 | 2 (1.8) | 0.98 |
| HCV infection (%) | 1 (3.7) | 0 | 0.197 |
| HBV infection (%) | 1 (3.7) | 1 (0.9) | 0.356 |
| Perinatal outcomes: | |||
| Gestational age at delivery (weeks) | 34.8 ± 4.2 | 39.1 ± 1.6 | <0.0001 |
| Cesarean section (%) | 21 (77.8) | 37 (33.6) | <0.0001 |
| Birth weight (g) | 2350 ± 878.36 | 3404 ± 488.37 | 0.001 |
| Birth weight centiles | 38.63 ± 23.47 | 45.97 ± 27.76 | 0.171 |
| SGA (<10 percentile) (%) | 4 (14.8) | 8 (7.3) | 0.252 |
| Variables (Mean ± SD) | Study Group (n = 27) |
|---|---|
| Prepregnancy laboratory values: | |
| SCr (mg/dL) | 1.03 ± 0.24 |
| eGFR (mL/min/1.73 m2) | 65.5 ± 23.8 |
| Pregnancy (I trimester) laboratory values | |
| SCr (mg/dL) | 1.14 ± 0.38 |
| ALT (U/L) | 18.9 ± 0.11 |
| AST (U/L) | 17.04 ± 0.83 |
| Hgb (g/dL) | 10.84 ± 1.27 |
| Urea (mg/dL) | 7.24 ± 1.91 |
| Postpartum Scr (mg/dL) | 1.17 ± 0.40 |
| Variable | Study Group (n = 27) | Control Group (n = 110) | p-Value |
|---|---|---|---|
| free β-hCG (mIU/L) | 123.06 ± 76.54 | 50.76 ± 32.71 | 0.047 |
| free β-hCG MoM | 3.47 ± 2.08 | 1.38 ± 0.85 | 0.035 |
| PAPP-A (mIU/L) | 5.25 ± 4.20 | 2.48 ± 1.16 | 0.016 |
| PAPP-A MoM | 1.46 ± 0.81 | 0.98 ± 0.57 | 0.007 |
| NT (mm) | 1.77 ± 0.43 | 1.70 ± 0.47 | 0.687 |
| UtA PI | 1.06 ± 0.23 | 1.28 ± 0.53 | 0.052 |
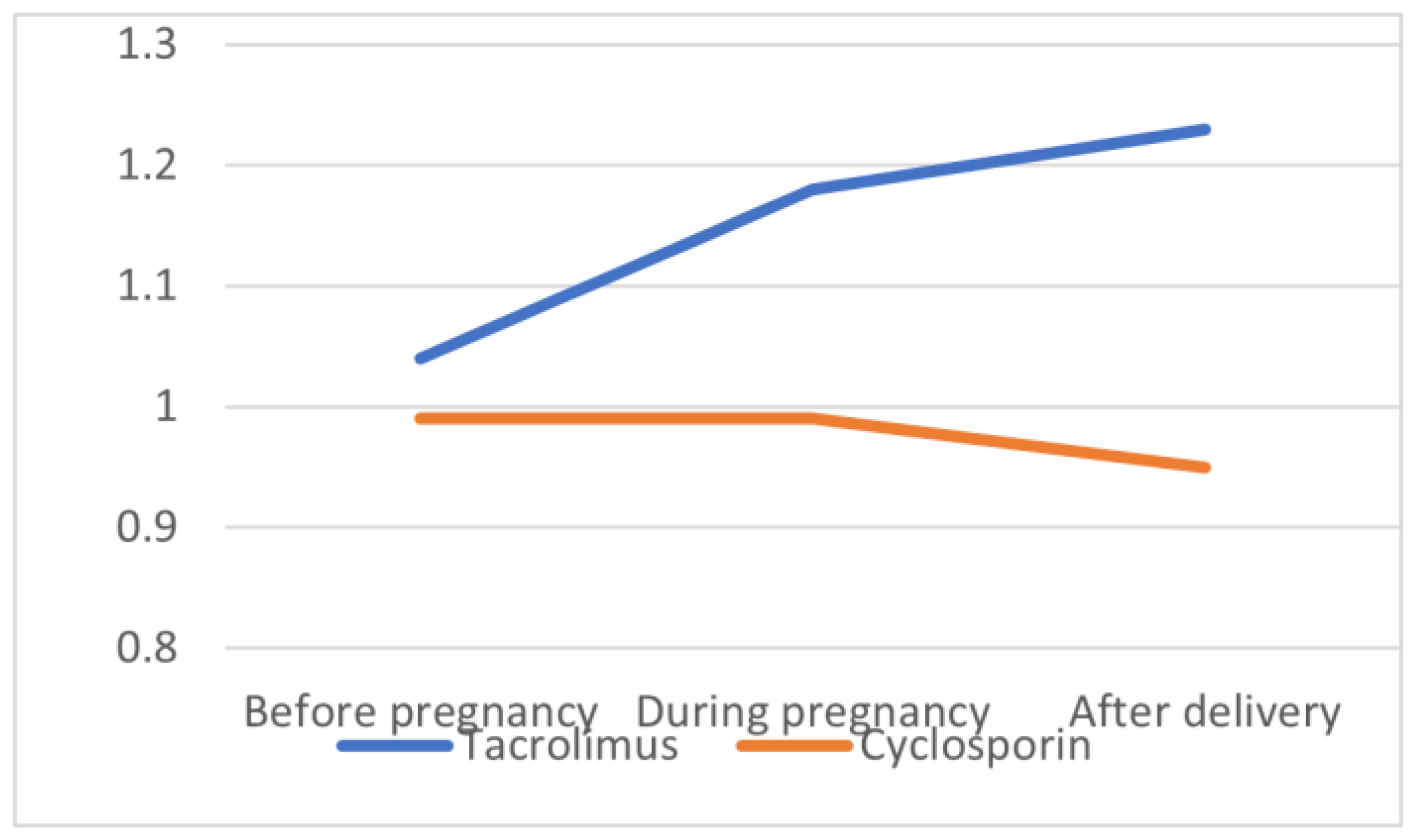
| Variables | Tacrolimus (n = 19) | Cyclosporin (n = 7) | p-Value |
|---|---|---|---|
| NT (mm) | 1.91 ± 0.36 | 1.96 ± 0.31 | 0.75 |
| UtA PI | 1.13 ± 0.37 | 1.12 ± 0.29 | 0.95 |
| free β-hCG (mIU/L) | 101.01 ± 68.10 | 157.32 ± 80.50 | 0.18 |
| free β-hCG MoM | 2.87 ± 1.76 | 3.40 ± 1.30 | 0.47 |
| PAPP-A (mIU/L) | 4.44 ± 3.25 | 7.88 ± 6.31 | 0.16 |
| PAPP-A MoM | 1.28 ± 0.64 | 2.02 ± 1.07 | 0.12 |
| GA at delivery (weeks) | 34.16 ± 4.60 | 36.00 ± 2.70 | 0.33 |
| Birthweight (g) | 2266.05 ± 937.35 | 2401.43 ± 654.08 | 0.73 |
| Birthweight percentile | 40.79 ± 23.26 | 26.71 ± 14.49 | 0.16 |
| SCr before pregnancy (mg/dL) | 1.04 ± 0.28 | 0.99 ± 0.11 | 0.70 |
| SCr during pregnancy (md/dL) | 1.18 ± 0.39 | 0.99 ± 0.32 | 0.29 |
| SCr after delivery (mg/dL) | 1.23 ± 0.44 | 0.95 ± 0.16 | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazanowska, N.; Jarmużek-Orska, P.; Pietrzak, B.; Pazik, J.; Jabiry-Zieniewicz, Z.; Kosiński, P. First-Trimester Biochemical Serum Markers in Female Kidney Transplant Recipients—The Impact of Graft Function. Int. J. Environ. Res. Public Health 2022, 19, 16352. https://doi.org/10.3390/ijerph192316352
Mazanowska N, Jarmużek-Orska P, Pietrzak B, Pazik J, Jabiry-Zieniewicz Z, Kosiński P. First-Trimester Biochemical Serum Markers in Female Kidney Transplant Recipients—The Impact of Graft Function. International Journal of Environmental Research and Public Health. 2022; 19(23):16352. https://doi.org/10.3390/ijerph192316352
Chicago/Turabian StyleMazanowska, Natalia, Patrycja Jarmużek-Orska, Bronisława Pietrzak, Joanna Pazik, Zoulikha Jabiry-Zieniewicz, and Przemysław Kosiński. 2022. "First-Trimester Biochemical Serum Markers in Female Kidney Transplant Recipients—The Impact of Graft Function" International Journal of Environmental Research and Public Health 19, no. 23: 16352. https://doi.org/10.3390/ijerph192316352