
Maxillofacial Injuries Sustained by Riders of Electric-Powered Bikes and Electric-Powered Scooters
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
- Minor injuries (dentoalveolar injuries and facial lacerations);
- Mandibular fractures (symphysis/parasymphysis, angle/body, condylar/subcondylar);
- Midface fractures (orbit, naso-orbito-ethmoidal [NOE], zygomatic complex/arch, LeFort I/II/III, maxilla);
- Skull base and cranial vault fractures (frontal bone and sinus).
- The surgical interventions were subdivided into:
- Suturing;
- Splinting;
- Closed reduction approaches (either intermaxillary fixation or Gillies approach);
- Open reduction and internal fixation (ORIF).
2.3. Statistical Analysis
3. Results
3.1. Rider Characteristics
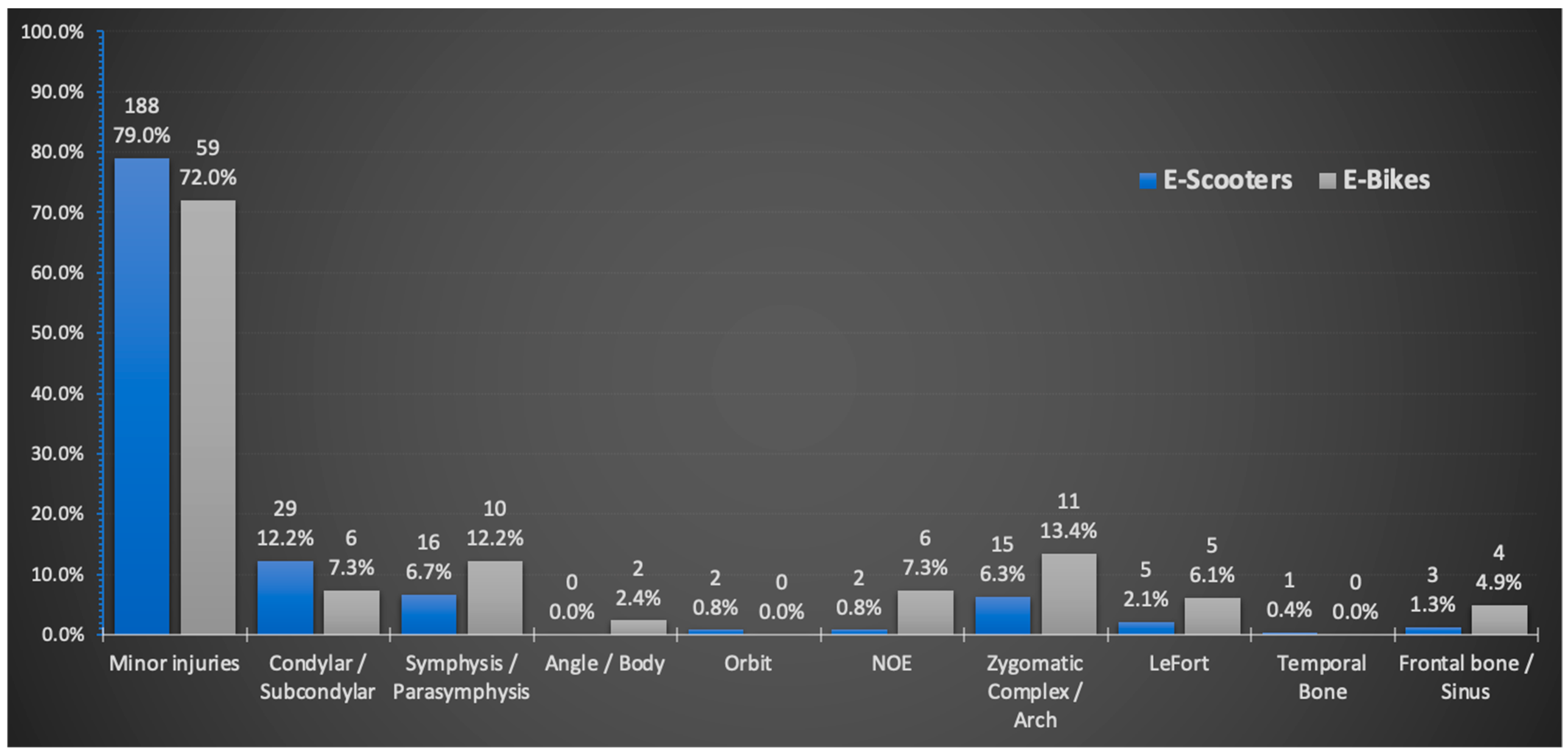
3.2. Type of Injuries and Treatment
3.3. Protective Headgear Use
3.4. Driving under the Influence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hadar, Y. Electronic Bike Accidents—Data, Risk Factors, Behaviors and Means for Dealing with Phenomenon. Israeli National Road Safety Authority. October 2018. Available online: https://www.gov.il/BlobFolder/reports/ebikes_2018/he/research_ebikes_2018.pdf (accessed on 25 August 2021).
- Soroker, G. Electronic Scooters—Data, Risk Factors and Mode of Actions. Israeli National Road Safety Authority. August 2020. Available online: https://www.gov.il/BlobFolder/reports/202008_electric_scooters_review/he/reports_202008_electric_scooters_review.pdf (accessed on 25 August 2021).
- DiMaggio, C.J.; Bukur, M.; Wall, S.P.; Frangos, S.G.; Wen, A.Y. Injuries associated with electric powered bikes and scooters: Analysis of US Consumer Product Data. Inj. Prev. 2019, 26, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Cui, M.; Gu, Y.; Stallones, L.; Xiang, H. Trends in electric bike–related injury in China, 2004–2010. Asia Pac. J. Public Health 2015, 27, NP1819–NP1826. [Google Scholar] [CrossRef] [PubMed]
- Siman-Tov, M.; Radomislensky, I.; Israel Trauma Group; Peleg, K. The casualties from electric bike and motorized scooter road accidents. Traffic Inj. Prev. 2017, 18, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Goh, S.S.; Leong, X.Y.; Cheng, J.Y.; Teo, L.T. Electronic bicycles and scooters: Convenience at the expense of danger? Ann. Acad. Med. Singapore 2019, 48, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Goldman, S.; Peleg, K.; Levin, L. With support of the Israel Trauma Group. Dental and maxillofacial injuries associated with electric-powered bikes and scooters in Israel: A report for 2014–2019. Dent. Traumatol. 2020, 36, 533–537. [Google Scholar] [PubMed]
- Craniomaxillofacial AO Surgery Reference—AO CMF Fracture Classification. Available online: https://surgeryreference.aofoundation.org/cmf/trauma (accessed on 16 November 2021).
- Bresler, A.Y.; Hanba, C.; Svider, P.; Carron, M.A.; Hsueh, W.D.; Paskhover, B. Craniofacial injuries related to motorized scooter use: A rising epidemic. Am. J. Otolaryngol. 2019, 40, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Grill, F.D.; Roth, C.; Zyskowski, M.; Fichter, A.; Kollmuss, M.; Stimmer, H.; Deppe, H.; Wolff, K.D.; Nieberler, M. E-scooter-related craniomaxillofacial injuries compared with bicycle-related injuries—A retrospective study. J. Craniomaxillofac. Surg. 2022, 50, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Cicchino, J.B.; Kulie, P.E.; McCarthy, M.L. Injuries related to electric scooter and bicycle use in a Washington, DC, emergency department. Traffic Inj. Prev. 2021, 22, 401–406. [Google Scholar] [CrossRef]
- Shiffler, K.; Mancini, K.; Wilson, M.; Huang, A.; Mejia, E.; Yip, F.K. Intoxication is a Significant Risk Factor for Severe Craniomaxillofacial Injuries in Standing Electric Scooter Accidents. J. Oral Maxillofac. Surg. 2021, 79, 1084–1090. [Google Scholar] [CrossRef]
- Nelson, N.G.; McKenzie, L.B. Mountain biking–related injuries treated in emergency departments in the United States, 1994–2007. Am. J. Sports Med. 2011, 39, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Boffano, P.; Roccia, F.; Zavattero, E.; Dediol, E.; Uglešić, V.; Kovačič, Ž; Vesnaver, A.; Konstantinović, V.S.; Petrović, M.; Stephens, J.; et al. European Maxillofacial Trauma (EURMAT) project: A multicentre and prospective study. J. Craniomaxillofac. Surg. 2015, 43, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Hamzani, Y.; Bar Hai, D.; Cohen, N.; Drescher, M.J.; Chaushu, G.; Yahya, B.H. The impact of helmet use on oral and maxillofacial injuries associated with electric-powered bikes or powered scooter: A retrospective cross-sectional study. Head Face Med. 2021, 17, 36. [Google Scholar] [CrossRef] [PubMed]
- Tefft, B.C. Impact speed and a pedestrian’s risk of severe injury or death. Accid. Anal. Prev. 2013, 50, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Almannaa, M.H.; Ashqar, H.I.; Elhenawy, M.; Masoud, M.; Rakotonirainy, A.; Rakha, H. A comparative analysis of escooter and e-bike usage patterns: Findings from the City of Austin, TX. Int. J. Sustain. Transp. 2021, 15, 571–579. [Google Scholar] [CrossRef]
- van der Zaag, P.D.; Rozema, R.; Poos, H.P.; Kleinbergen, J.Y.; van Minnen, B.; Reininga, I.H.; Doff, M.H.; de Vries, G.T.; El Moumni, M.; Verbeek, R.; et al. Maxillofacial Fractures in Electric and Conventional Bicycle-Related Accidents. J. Oral Maxillofac. Surg. 2022, 80, 1361–1370. [Google Scholar] [CrossRef] [PubMed]
- Gülses, A.; Klingauf, L.; Emmert, M.; Karayürek, F.; Naujokat, H.; Acil, Y.; Wiltfang, J.; Spille, J. Injury patterns and outcomes in bicycle-related maxillofacial traumata: A retrospective analysis of 162 cases. J. Craniomaxillofac. Surg. 2022, 50, 70–75. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| E-Scooters | E-Bikes | p-Value | |
|---|---|---|---|
| Patients (%) | 238 (74.4%) | 82 (25.6%) | - |
| Age (years) # | 27.66 (8) | 32.28 (18) | 0.008 |
| X-ray (%) | 153 (64.3%) | 58 (70.7%) | 0.288 |
| Protractive helmet (%) | 62 (34.1%) | 26 (40.6%) | 0.346 |
| Blood alcohol levels above normal (%) | 31 (20.4%) | 8 (14%) | 0.293 |
| Additional injuries (%) | |||
| TBI | 14 (5.9%) | 4 (4.9%) | >0.999 |
| Orthopedic | 112 (47.1%) | 44 (53.7%) | 0.302 |
| Chest | 3 (1.3%) | 1 (1.2%) | >0.999 |
| Combinations | 3 (1.3%) | 1 (1.2%) | >0.999 |
| Need for hospitalization (%) | 55 (23.1%) | 29 (35.4%) | 0.03 |
| Surgical intervention (%) | |||
| Suturing or Wire splinting | 71 (29.8%) | 22 (26.8%) | 0.606 |
| Closed treatment (IMF/Gillies) | 26 (10.9%) | 8 (9,8%) | 0.767 |
| ORIF | 21 (8.8%) | 14 (17.1%) | 0.039 |
| Combinations | 11 (4.6%) | 5 (6.1%) | 0.567 |
| Follow-up (%) | 81 (34%) | 35 (42.7%) | 0.16 |
| Headgear Wearers | Non-Headgear- Wearers | p-Value | |
|---|---|---|---|
| Patients (%) | 88 (35.77%) | 158 (64.23%) | - |
| Age (years) # | 29.05 (11.75) | 27.78 (10) | 0.485 |
| X-ray (%) | 58 (65.9%) | 109 (69%) | 0.62 |
| Blood alcohol levels above normal (%) | 6 (10.5%) | 30 (28%) | 0.01 |
| Additional injuries (%) | 49 (55.7%) | 74 (46.8%) | 0.231 |
| Need for hospitalization (%) | 22 (25%) | 47 (29.7%) | 0.427 |
| Intervention (%) | |||
| Suturing or Wire splinting | 27 (30.7%) | 47 (29.7%) | 0.878 |
| Closed treatment (IMF/Gillies) | 12 (13.6%) | 20 (12.7%) | 0.827 |
| ORIF | 8 (9.1%) | 22 (13.9%) | 0.267 |
| Combinations | 6 (6.8%) | 9 (5.7%) | 0.724 |
| Drunk Drivers | Sober Drivers | p-Value | |
|---|---|---|---|
| Patients (%) | 39 (18.67%) | 170 (81.33%) | - |
| Age (years) # | 29.87 (10) | 29.3 (13) | 0.635 |
| Injury Location (%) | |||
| Minor injuries * | 21 (53.8%) | 134 (78.8%) | 0.002 |
| Condylar/subcondylar | 4 (10.3%) | 20 (11.8%) | 0.79 |
| Symphysis/parasymphysis | 4 (10.3%) | 13 (7.6%) | 0.591 |
| Angle/body | 0 (0%) | 1 (0.6%) | 0.631 |
| Orbit | 1 (2.6%) | 1 (0.06%) | 0.253 |
| Frontal sinus | 3 (7.7%) | 3 (1.8%) | 0.046 |
| Zygomatic complex | 6 (15.4%) | 10 (5.9%) | 0.044 |
| LeFort | 1 (2.6%) | 5 (2.9%) | 0.899 |
| NOE | 3 (7.7%) | 4 (2.4%) | 0.095 |
| Protractive helmet (%) | 6 (16.7%) | 51 (39.8%) | 0.01 |
| Need for hospitalization (%) | 18 (46.2%) | 40 (23.5%) | 0.004 |
| Intervention (%) | |||
| Suturing or Wire splinting | 8 (20.5%) | 49 (28.8%) | 0.327 |
| Closed treatement (IMF/Gillies) | 8 (20.5%) | 15 (8.8%) | 0.047 |
| ORIF | 8 (20.5%) | 12 (7.1%) | 0.016 |
| Combinations | 4 (10.3%) | 6 (3.5%) | 0.093 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arbel, S.; Zrifin, E.; Mahmoud, R.; Mijiritsky, E.; Groysman, L.; Shuster, A.; Rahima, H.; Kleinman, S.; Ianculovici, C.; Peleg, O. Maxillofacial Injuries Sustained by Riders of Electric-Powered Bikes and Electric-Powered Scooters. Int. J. Environ. Res. Public Health 2022, 19, 15183. https://doi.org/10.3390/ijerph192215183
Arbel S, Zrifin E, Mahmoud R, Mijiritsky E, Groysman L, Shuster A, Rahima H, Kleinman S, Ianculovici C, Peleg O. Maxillofacial Injuries Sustained by Riders of Electric-Powered Bikes and Electric-Powered Scooters. International Journal of Environmental Research and Public Health. 2022; 19(22):15183. https://doi.org/10.3390/ijerph192215183
Chicago/Turabian StyleArbel, Shimrit, Elad Zrifin, Reema Mahmoud, Eitan Mijiritsky, Leonid Groysman, Amir Shuster, Heled Rahima, Shlomi Kleinman, Clariel Ianculovici, and Oren Peleg. 2022. "Maxillofacial Injuries Sustained by Riders of Electric-Powered Bikes and Electric-Powered Scooters" International Journal of Environmental Research and Public Health 19, no. 22: 15183. https://doi.org/10.3390/ijerph192215183