
Musculoskeletal Ultrasound Shows Muscle Mass Changes during Post-Acute Care Hospitalization in Older Men: A Prospective Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Eligibility Criteria
2.3. Study Variables
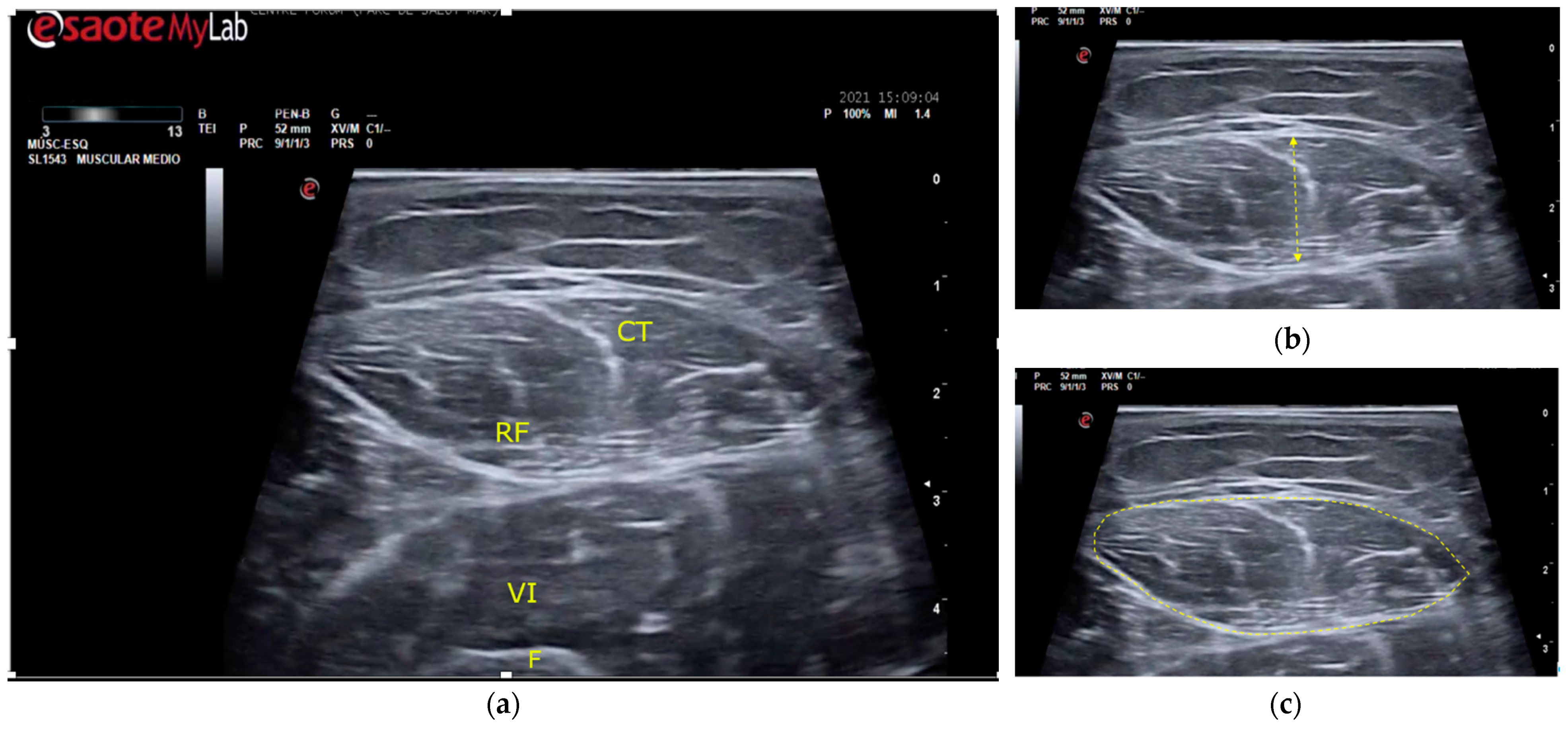
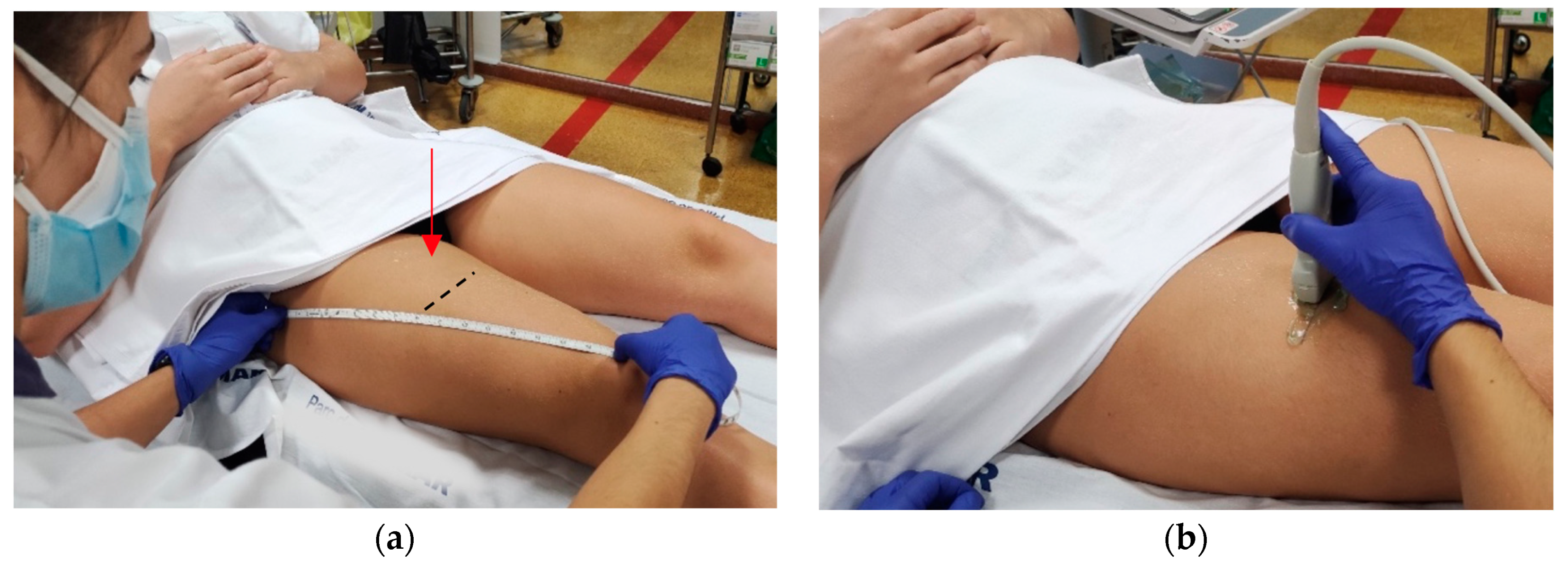
2.3.1. Muscle Thickness and Cross-Sectional Area
2.3.2. Muscle Strength
2.3.3. Muscle Mass

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | |
|---|---|
| Muscle to assess | Rectus femoris of quadriceps |
| Patient position | Patient lying supine, hips and knees in a neutral position |
| Patient condition | The patient had to maintain the same position for at least 30 min before the assessment, measuring the muscle in a relaxed state and before any functional testing. |
| Ultrasound and probe characteristics | B-mode ultrasound, 12 MHz, with a 5 cm-linear transducer probe. |
| Probe position | The probe in neutral/perpendicular to the skin, with a generous amount of transmission gel, maintaining the minimal pressure possible between the transducer and the skin. |
| Anatomical landmarks | Proximal landmark: greater trochanter. Distal landmark: proximal border of the patella. |
| Measuring point | The middle point of distance between anatomical landmarks, marking this point with a demographic pencil. |
| Measurements procedures | With the transducer probe in the measuring point. The measure of Muscle Thickness:
|
| Final value | The investigator repeated each measurement three times and used the mean value. |
2.3.4. Physical Performance
2.3.5. Sarcopenia Risk
2.3.6. Sarcopenia


2.3.7. Frailty Status
2.3.8. Nutritional Risk
2.3.9. Laboratory Values
2.3.10. Pharmacological Treatment
2.3.11. Demographic and Clinical Characteristics
2.4. Study Procedures
2.5. Sample Size Calculation
2.6. Statistics
3. Results
| Baseline | 1st Week Follow-Up | 2nd Week Follow-Up | |||
|---|---|---|---|---|---|
| Mean (SD) | Mean Difference | p | Mean Difference | p | |
| (95%CI) | (95%CI) | ||||
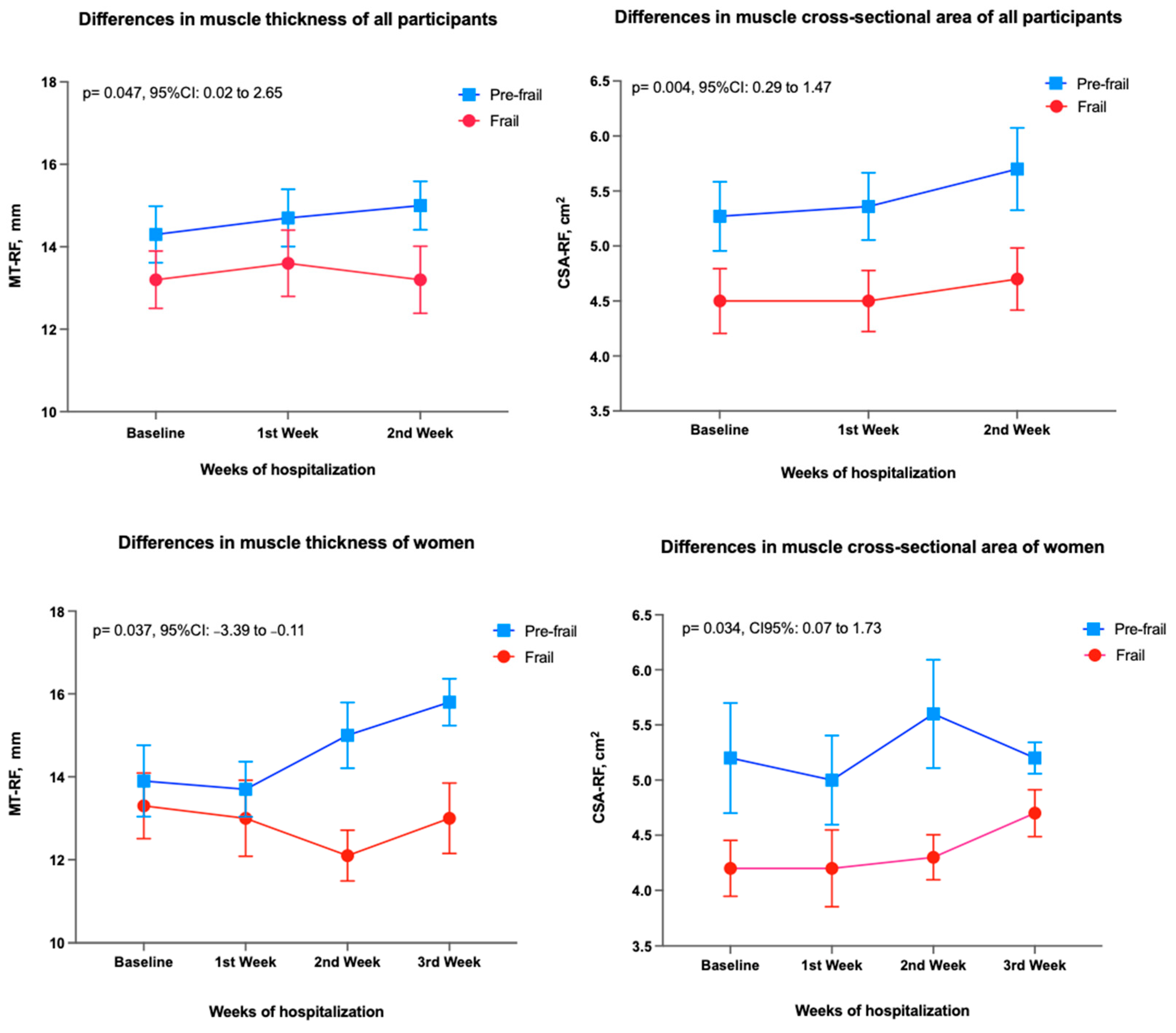
| Muscle thickness, mm | |||||
| Women | 13.2 (2.9) | 0.2 (−0.8 to 1.2) | 0.932 | 0.5 (−1.4 to 2.3) | 0.847 |
| Men | 14.9 (3.4) | 0.9 (0.3 to 1.4) | 0.003 | 0.7 (0.1 to 1.4) | 0.036 |
| Cross-sectional area, cm2 | |||||
| Women | 4.7 (1.5) | −0.1 (−0.5 to 0.3) | 0.926 | 0.2 (−0.5 to 0.9) | 0.752 |
| Men | 5.3 (1.3) | 0.4 (0.1 to 0.6) | 0.007 | 0.6 (0.01 to 1.2) | 0.048 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nascimento, C.M.; Ingles, M.; Salvador-Pascual, A.; Cominetti, M.R.; Gomez-Cabrera, M.C.; Viña, J. Sarcopenia, frailty and their prevention by exercise. Free Radic. Biol. Med. 2019, 132, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Proietti, M.; Cesari, M. Frailty: What Is It? Adv. Exp. Med. Biol. 2020, 1216, 1–7. [Google Scholar] [CrossRef]
- Tabue-Teguo, M.; Simo, N.; Gonzalez-Colaço Harmand, M.; Cesari, M.; Avila-Funes, J.A.; Féart, C.; Amiéva, H.; Dartigues, J.F. Frailty in elderly: A brief review. Gériatrie Et Psychol. Neuropsychiatr. Du Vieil. 2017, 15, 127–137. [Google Scholar] [CrossRef]
- Tanner, R.E.; Brunker, L.B.; Agergaard, J.; Barrows, K.M.; Briggs, R.A.; Kwon, O.S.; Young, L.M.; Hopkins, P.N.; Volpi, E.; Marcus, R.L.; et al. Age-related differences in lean mass, protein synthesis and skeletal muscle markers of proteolysis after bed rest and exercise rehabilitation. J. Physiol. 2015, 593, 4259–4273. [Google Scholar] [CrossRef] [Green Version]
- Witteveen, E.; Wieske, L.; Verhamme, C.; Schultz, M.J.; van Schaik, I.N.; Horn, J. Muscle and nerve inflammation in intensive care unit-acquired weakness: A systematic translational review. J. Neurol. Sci. 2014, 345, 15–25. [Google Scholar] [CrossRef]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. JAMA 2007, 297, 1772–1774. [Google Scholar] [CrossRef]
- Alley, D.E.; Koster, A.; Mackey, D.; Cawthon, P.; Ferrucci, L.; Simonsick, E.M.; Yu, B.; Hardy, S.; Goodpaster, B.; Sarkisian, C.; et al. Hospitalization and change in body composition and strength in a population-based cohort of older persons. J. Am. Geriatr. Soc. 2010, 58, 2085–2091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- English, K.L.; Paddon-Jones, D. Protecting muscle mass and function in older adults during bed rest. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 34–39. [Google Scholar] [CrossRef]
- Reidy, P.T.; Lindsay, C.C.; McKenzie, A.I.; Fry, C.S.; Supiano, M.A.; Marcus, R.L.; LaStayo, P.C.; Drummond, M.J. Aging-related effects of bed rest followed by eccentric exercise rehabilitation on skeletal muscle macrophages and insulin sensitivity. Exp. Gerontol. 2018, 107, 37–49. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Ferrillo, M.; Lippi, L.; Agostini, F.; de Sire, R.; Ferrara, P.E.; Raguso, G.; Riso, S.; Roccuzzo, A.; Ronconi, G.; et al. Sarcopenic Dysphagia, Malnutrition, and Oral Frailty in Elderly: A Comprehensive Review. Nutrients 2022, 14, 982. [Google Scholar] [CrossRef]
- Lee, H.; Lee, E.; Jang, I.Y. Frailty and Comprehensive Geriatric Assessment. J. Korean Med. Sci. 2020, 35, e16. [Google Scholar] [CrossRef] [PubMed]
- Schippinger, W. Comprehensive geriatric assessment. Wien. Med. Wochenschr. 2022, 172, 122–125. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaudart, C.; McCloskey, E.; Bruyere, O.; Cesari, M.; Rolland, Y.; Rizzoli, R.; Araujo de Carvalho, I.; Amuthavalli Thiyagarajan, J.; Bautmans, I.; Bertiere, M.C.; et al. Sarcopenia in daily practice: Assessment and management. BMC Geriatr. 2016, 16, 170. [Google Scholar] [CrossRef] [PubMed]
- Nijholt, W.; Scafoglieri, A.; Jager-Wittenaar, H.; Hobbelen, J.S.M.; van der Schans, C.P. The reliability and validity of ultrasound to quantify muscles in older adults: A systematic review. J. Cachexia Sarcopenia Muscle 2017, 8, 702–712. [Google Scholar] [CrossRef]
- Van den Broeck, J.; Buzzatti, L.; Jager-Wittenaar, H.; Perkisas, S.; Scafoglieri, A. The validity of ultrasound-derived equation models to predict whole-body muscle mass: A systematic review. Clin. Nutr. ESPEN 2021, 46, 133–141. [Google Scholar] [CrossRef]
- Sponbeck, J.K.; Frandsen, C.R.; Ridge, S.T.; Swanson, D.A.; Swanson, D.C.; Johnson, A.W. Leg muscle cross-sectional area measured by ultrasound is highly correlated with MRI. J. Foot Ankle Res. 2021, 14, 5. [Google Scholar] [CrossRef]
- Perkisas, S.; Bastijns, S.; Baudry, S.; Bauer, J.; Beaudart, C.; Beckwée, D.; Cruz-Jentoft, A.; Gasowski, J.; Hobbelen, H.; Jager-Wittenaar, H.; et al. Application of ultrasound for muscle assessment in sarcopenia: 2020 SARCUS update. Eur. Geriatr. Med. 2021, 12, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Perkisas, S.; Baudry, S.; Bauer, J.; Beckwée, D.; De Cock, A.-M.; Hobbelen, H.; Jager-Wittenaar, H.; Kasiukiewicz, A.; Landi, F.; Marco, E.; et al. Application of ultrasound for muscle assessment in sarcopenia: Towards standardized measurements. Eur. Geriatr. Med. 2018, 9, 739–757. [Google Scholar] [CrossRef] [PubMed]
- Leigheb, M.; de Sire, A.; Colangelo, M.; Zagaria, D.; Grassi, F.A.; Rena, O.; Conte, P.; Neri, P.; Carriero, A.; Sacchetti, G.M.; et al. Sarcopenia Diagnosis: Reliability of the Ultrasound Assessment of the Tibialis Anterior Muscle as an Alternative Evaluation Tool. Diagnostics 2021, 11, 2158. [Google Scholar] [CrossRef] [PubMed]
- Hammond, K.; Mampilly, J.; Laghi, F.A.; Goyal, A.; Collins, E.G.; McBurney, C.; Jubran, A.; Tobin, M.J. Validity and reliability of rectus femoris ultrasound measurements: Comparison of curved-array and linear-array transducers. J. Rehabil. Res. Dev. 2014, 51, 1155–1164. [Google Scholar] [CrossRef] [PubMed]
- Meza-Valderrama, D.; Sánchez-Rodríguez, D.; Perkisas, S.; Duran, X.; Bastijns, S.; Dávalos-Yerovi, V.; Da Costa, E.; Marco, E. The feasibility and reliability of measuring forearm muscle thickness by ultrasound in a geriatric inpatient setting: A cross-sectional pilot study. BMC Geriatr. 2022, 22, 137. [Google Scholar] [CrossRef]
- Pirri, C.; Pirri, N.; Porzionato, A.; Boscolo-Berto, R.; De Caro, R.; Stecco, C. Inter- and Intra-Rater Reliability of Ultrasound Measurements of Superficial and Deep Fasciae Thickness in Upper Limb. Diagnostics 2022, 12, 2195. [Google Scholar] [CrossRef]
- Fukumoto, Y.; Ikezoe, T.; Taniguchi, M.; Yamada, Y.; Sawano, S.; Minani, S.; Asai, T.; Kimura, M.; Ichihashi, N. Cut-off Values for Lower Limb Muscle Thickness to Detect Low Muscle Mass for Sarcopenia in Older Adults. Clin. Interv. Aging 2021, 16, 1215–1222. [Google Scholar] [CrossRef]
- Berger, J.; Bunout, D.; Barrera, G.; de la Maza, M.P.; Henriquez, S.; Leiva, L.; Hirsch, S. Rectus femoris (RF) ultrasound for the assessment of muscle mass in older people. Arch. Gerontol. Geriatr. 2015, 61, 33–38. [Google Scholar] [CrossRef]
- Ozturk, Y.; Koca, M.; Burkuk, S.; Unsal, P.; Dikmeer, A.; Oytun, M.G.; Bas, A.O.; Kahyaoglu, Z.; Deniz, O.; Coteli, S.; et al. The role of muscle ultrasound to predict sarcopenia. Nutrition 2022, 101, 111692. [Google Scholar] [CrossRef]
- Wilkinson, T.J.; Gore, E.F.; Vadaszy, N.; Nixon, D.G.D.; Watson, E.L.; Smith, A.C. Utility of Ultrasound as a Valid and Accurate Diagnostic Tool for Sarcopenia: Sex-Specific Cutoff Values in Chronic Kidney Disease. J. Ultrasound Med. 2021, 40, 457–467. [Google Scholar] [CrossRef]
- Barotsis, N.; Galata, A.; Hadjiconstanti, A.; Panayiotakis, G. The ultrasonographic measurement of muscle thickness in sarcopenia. A prediction study. Eur. J. Phys. Rehabil. Med. 2020, 56, 427–437. [Google Scholar] [CrossRef]
- Lin, X.; Chen, Z.; Huang, H.; Zhong, J.; Xu, L. Diabetic kidney disease progression is associated with decreased lower-limb muscle mass and increased visceral fat area in T2DM patients. Front. Endocrinol. (Lausanne) 2022, 13, 1002118. [Google Scholar] [CrossRef]
- Sahathevan, S.; Khor, B.H.; Singh, B.K.S.; Sabatino, A.; Fiaccadori, E.; Daud, Z.A.M.; Ali, M.S.; Narayanan, S.S.; Tallman, D.; Chinna, K.; et al. Association of Ultrasound-Derived Metrics of the Quadriceps Muscle with Protein Energy Wasting in Hemodialysis Patients: A Multicenter Cross-Sectional Study. Nutrients 2020, 12, 3597. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.R.J.; Kong, K.H. Ultrasound Measurements of Rectus Femoris and Locomotor Outcomes in Patients with Spinal Cord Injury. Life 2022, 12, 1073. [Google Scholar] [CrossRef]
- Mueller, N.; Murthy, S.; Tainter, C.R.; Lee, J.; Riddell, K.; Fintelmann, F.J.; Grabitz, S.D.; Timm, F.P.; Levi, B.; Kurth, T.; et al. Can Sarcopenia Quantified by Ultrasound of the Rectus Femoris Muscle Predict Adverse Outcome of Surgical Intensive Care Unit Patients as well as Frailty? A Prospective, Observational Cohort Study. Ann. Surg. 2016, 264, 1116–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rustani, K.; Kundisova, L.; Capecchi, P.L.; Nante, N.; Bicchi, M. Ultrasound measurement of rectus femoris muscle thickness as a quick screening test for sarcopenia assessment. Arch. Gerontol. Geriatr. 2019, 83, 151–154. [Google Scholar] [CrossRef] [PubMed]
- McKendry, J.; Thomas, A.C.Q.; Phillips, S.M. Muscle Mass Loss in the Older Critically Ill Population: Potential Therapeutic Strategies. Nutr. Clin. Pract. 2020, 35, 607–616. [Google Scholar] [CrossRef]
- Dirks, M.L.; Wall, B.T.; van de Valk, B.; Holloway, T.M.; Holloway, G.P.; Chabowski, A.; Goossens, G.H.; van Loon, L.J. One Week of Bed Rest Leads to Substantial Muscle Atrophy and Induces Whole-Body Insulin Resistance in the Absence of Skeletal Muscle Lipid Accumulation. Diabetes 2016, 65, 2862–2875. [Google Scholar] [CrossRef] [Green Version]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [Green Version]
- Crum, R.M.; Anthony, J.C.; Bassett, S.S.; Folstein, M.F. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef]
- Lukaski, H.C. Requirements for clinical use of bioelectrical impedance analysis (BIA). Ann. N. Y. Acad. Sci. 1999, 873, 72–76. [Google Scholar] [CrossRef]
- Větrovská, R.; Vilikus, Z.; Klaschka, J.; Stránská, Z.; Svačina, Š.; Svobodová, Š.; Matoulek, M. Does impedance measure a functional state of the body fat? Physiol. Res. 2014, 63, S309–S320. [Google Scholar] [CrossRef]
- Schutz, Y.; Kyle, U.U.; Pichard, C. Fat-free mass index and fat mass index percentiles in Caucasians aged 18-98 y. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 953–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Wang, Y.C. Four-Meter Gait Speed: Normative Values and Reliability Determined for Adults Participating in the NIH Toolbox Study. Arch. Phys. Med. Rehabil. 2019, 100, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, D.; Marco, E.; Dávalos-Yerovi, V.; López-Escobar, J.; Messaggi-Sartor, M.; Barrera, C.; Ronquillo-Moreno, N.; Vázquez-Ibar, O.; Calle, A.; Inzitari, M.; et al. Translation and Validation of the Spanish Version of the SARC-F Questionnaire to Assess Sarcopenia in Older People. J. Nutr. Health Aging 2019, 23, 518–524. [Google Scholar] [CrossRef]
- Abellan van Kan, G.; Rolland, Y.M.; Morley, J.E.; Vellas, B. Frailty: Toward a clinical definition. J. Am. Med. Dir. Assoc. 2008, 9, 71–72. [Google Scholar] [CrossRef]
- Woo, J.; Yu, R.; Wong, M.; Yeung, F.; Wong, M.; Lum, C. Frailty Screening in the Community Using the FRAIL Scale. J. Am. Med. Dir. Assoc. 2015, 16, 412–419. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Liu, H.; Jiao, J.; Zhu, M.; Wen, X.; Jin, J.; Wang, H.; Lv, D.; Zhao, S.; Sun, X.; Wu, X.; et al. Nutritional Status According to the Short-Form Mini Nutritional Assessment (MNA-SF) and Clinical Characteristics as Predictors of Length of Stay, Mortality, and Readmissions Among Older Inpatients in China: A National Study. Front. Nutr. 2022, 9, 815578. [Google Scholar] [CrossRef] [PubMed]
- Martín, A.I.; Priego, T.; López-Calderón, A. Hormones and Muscle Atrophy. In Muscle Atrophy; Xiao, J., Ed.; Springer: Singapore, 2018; pp. 207–233. [Google Scholar] [CrossRef]
- Ferrando, B.; Olaso-Gonzalez, G.; Sebastia, V.; Viosca, E.; Gomez-Cabrera, M.C.; Viña, J. Alopurinol y su papel en el tratamiento de la sarcopenia. Rev. Española De Geriatría Y Gerontol. 2014, 49, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Sartiani, L.; Spinelli, V.; Laurino, A.; Blescia, S.; Raimondi, L.; Cerbai, E.; Mugelli, A. Pharmacological perspectives in sarcopenia: A potential role for renin-angiotensin system blockers? Clin. Cases Miner. Bone Metab. 2015, 12, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.P.; Josse, R.G. 2002 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada. Cmaj 2002, 167, S1–S34. [Google Scholar]
- Borgström, F.; Karlsson, L.; Ortsäter, G.; Norton, N.; Halbout, P.; Cooper, C.; Lorentzon, M.; McCloskey, E.V.; Harvey, N.C.; Javaid, M.K.; et al. Fragility fractures in Europe: Burden, management and opportunities. Arch. Osteoporos. 2020, 15, 59. [Google Scholar] [CrossRef] [Green Version]
- Portney, L.G. Foundations of Clinical Research: Applications to Evidence-Based Practice, 4th ed.; McGraw Hill: Philadelphia, PA, USA, 2020; Available online: https://fadavispt.mhmedical.com/book.aspx?bookID=2885 (accessed on 10 October 2022).
- Liu, K.; Shibata, J.; Fukuchi, K.; Takahashi, K.; Sonoo, T.; Ogura, T.; Goto, T. Optimal timing of introducing mobilization therapy for ICU patients with sepsis. J. Intensive Care 2022, 10, 22. [Google Scholar] [CrossRef]
- Fisher, S.R.; Kuo, Y.-f.; Graham, J.E.; Ottenbacher, K.J.; Ostir, G.V. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch. Intern. Med. 2010, 170, 1942–1943. [Google Scholar] [CrossRef] [Green Version]
- Ticinesi, A.; Meschi, T.; Narici, M.V.; Lauretani, F.; Maggio, M. Muscle Ultrasound and Sarcopenia in Older Individuals: A Clinical Perspective. J. Am. Med. Dir. Assoc. 2017, 18, 290–300. [Google Scholar] [CrossRef]
- Minetto, M.A.; Caresio, C.; Menapace, T.; Hajdarevic, A.; Marchini, A.; Molinari, F.; Maffiuletti, N.A. Ultrasound-Based Detection of Low Muscle Mass for Diagnosis of Sarcopenia in Older Adults. PMR 2016, 8, 453–462. [Google Scholar] [CrossRef]
- Flores, D.F.; Gentil, P.; Brown, L.E.; Pinto, R.S.; Carregaro, R.L.; Bottaro, M. Dissociated time course of recovery between genders after resistance exercise. J. Strength Cond Res. 2011, 25, 3039–3044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, K.; Asai, H.; Toyama, H.; Kunita, K.; Yaguchi, C.; Kiyota, N.; Tomita, H.; Jacobs, J.V. Changes in muscle thickness of gastrocnemius and soleus associated with age and sex. Aging Clin. Exp. Res. 2010, 22, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Chen, H.C.; Huang, S.W.; Liou, T.H. The Role of Muscle Mass Gain Following Protein Supplementation Plus Exercise Therapy in Older Adults with Sarcopenia and Frailty Risks: A Systematic Review and Meta-Regression Analysis of Randomized Trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef] [Green Version]
- Pilotto, A.; Cella, A.; Daragjati, J.; Veronese, N.; Musacchio, C.; Mello, A.M.; Logroscino, G.; Padovani, A.; Prete, C.; Panza, F. Three Decades of Comprehensive Geriatric Assessment: Evidence Coming From Different Healthcare Settings and Specific Clinical Conditions. J. Am. Med. Dir. Assoc. 2017, 18, 192.e1. [Google Scholar] [CrossRef] [PubMed]
- Distefano, G.; Goodpaster, B.H. Effects of Exercise and Aging on Skeletal Muscle. Cold Spring Harb. Perspect. Med. 2018, 8, a029785. [Google Scholar] [CrossRef] [PubMed]


| Total Sample (n = 40) | |
|---|---|
| Demographics: | |
| Age, years (SD) | 79.5 (9.5) |
| Sex, female, n (%) | 23 (57.5) |
| Ultrasound assessment: | |
| Muscle thickness, mm (SD) | |
| Women | 13.2 (2.9) |
| Men | 14.9 (3.4) |
| Cross-sectional area, mm2 (SD) | |
| Women | 4.8 (1.5) |
| Men | 5.3 (1.4) |
| Body composition: | |
| Body mass index, Kg/m2 (SD) | 29.1 (6.0) |
| Fat-free mass, Kg (SD) | |
| Women | 38.3 (6.7) |
| Men | 51.1 (10.0) |
| Fat mass, Kg (SD) | |
| Women | 34.6 (9.6) |
| Men | 26.6 (8.3) |
| Muscle strength, | |
| Handgrip, Kg (SD): | |
| Women | 18.1 (3.8) |
| Men | 24.9 (6.1) |
| Physical performance: | |
| 4 m gait speed test, m/s (SD) | 0.12 (0.2) |
| Sarcopenia assessment: | |
| SARC-F/10 (SD) | 6 (3) |
| Sarcopenia (EWGSOP2), n (%) | 7 (17.5) |
| FRAIL scale, /5 | |
| Frailty (3–5), n (%) | 14 (35) |
| Pre-frailty (1–2), n (%) | 26 (65) |
| Robust (0), n (%) | 0 |
| Malnutrition risk | |
| MNA-SF, /14 (SD) | 10 (2) |
| Comorbidity | |
| Charlson Index, /36 (SD) | 3 (4) |
| Laboratory test | |
| Vitamin D, ngmL (SD) | 18.2 (10.1) |
| Albumin, gdL (SD) | 3.4 (0.3) |
| Prealbumin, mgdL (SD) | 18.3 (6.6) |
| C Reactive Protein, mgdL (SD) | 5.1 (4.7) |
| Falls in the last year, n (%) | |
| 0 falls | 12 (30) |
| 1–3 falls | 22 (55) |
| 4 or more falls | 6 (15) |
| Fragility fractures, n (%) | 19 (47.5%) |
| Pharmacologic treatment, n (%) | |
| Glucocorticoids | 23 (57.5) |
| Allopurinol | 6 (15) |
| Statin | 14 (35) |
| Insulin | 10 (25) |
| ARBs | 9 (22.5) |
| NSAIDs | 38 (95) |
| Muscle Thickness | Cross-Sectional Area | |
|---|---|---|
| r (p) | r (p) | |
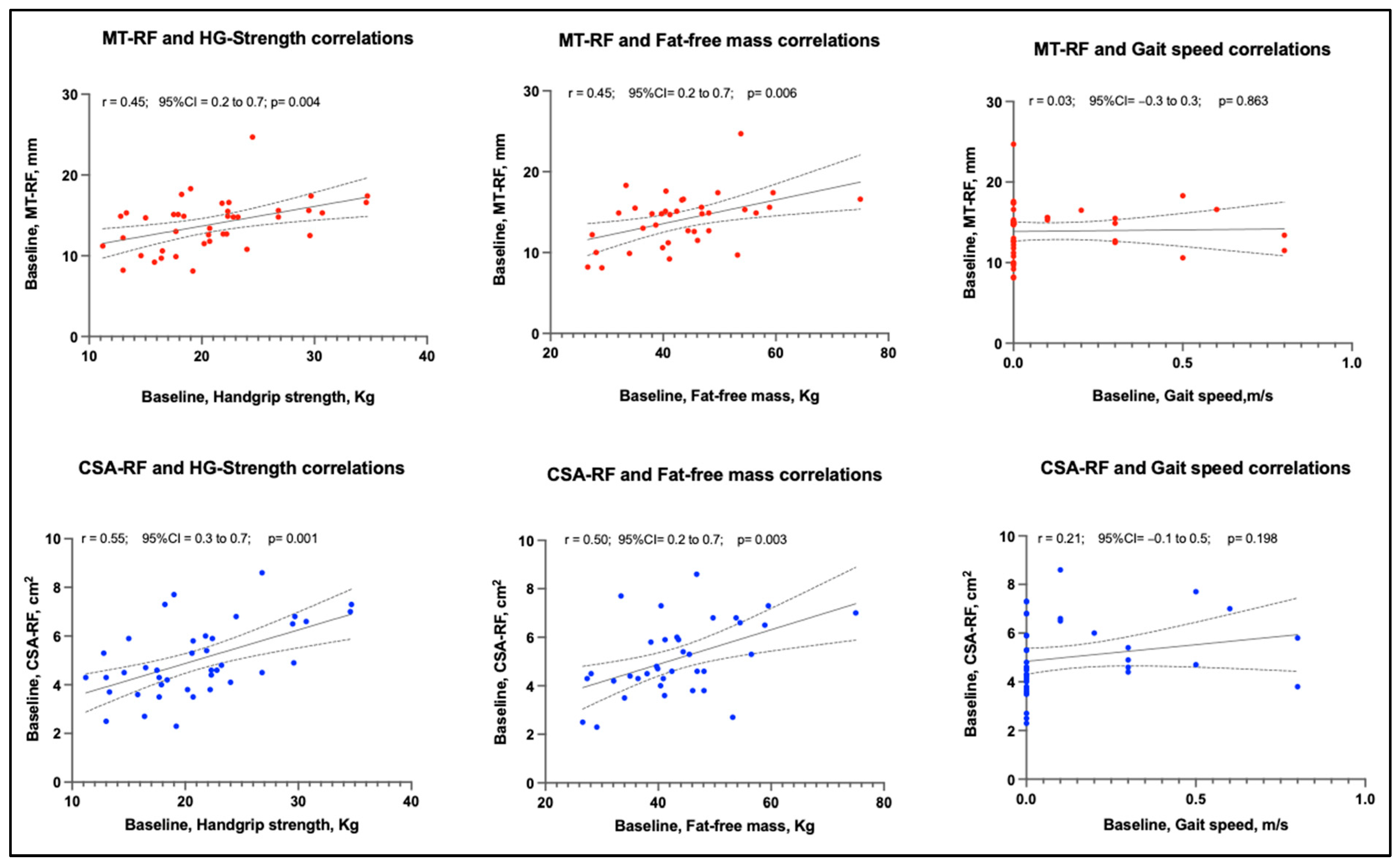
| Baseline | ||
| Handgrip | 0.45 (0.004) | 0.56 (0.001) |
| Fat-free mass | 0.45 (0.006) | 0.50 (0.003) |
| Gait speed | 0.03 (0.863) | 0.21 (0.198) |
| 1st week | ||
| Handgrip | 0.42 (0.011) | 0.58 (0.001) |
| Fat-free mass | 0.42 (0.015) | 0.57 (0.001) |
| Gait speed | 0.03 (0.974) | 0.38 (0.027) |
| 2nd week | ||
| Handgrip | 0.38 (0.080) | 0.34 (0.124) |
| Fat-free mass | 0.31 (0.192) | 0.44 (0.060) |
| Gait speed | 0.26 (0.238) | 0.38 (0.085) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meza-Valderrama, D.; Marco, E.; Muñoz-Redondo, E.; Morgado-Pérez, A.; Sánchez, M.T.; Curbelo Peña, Y.; De Jaime, E.; Canchucaja, L.; Meza Concepción, F.; Perkisas, S.; et al. Musculoskeletal Ultrasound Shows Muscle Mass Changes during Post-Acute Care Hospitalization in Older Men: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 15150. https://doi.org/10.3390/ijerph192215150
Meza-Valderrama D, Marco E, Muñoz-Redondo E, Morgado-Pérez A, Sánchez MT, Curbelo Peña Y, De Jaime E, Canchucaja L, Meza Concepción F, Perkisas S, et al. Musculoskeletal Ultrasound Shows Muscle Mass Changes during Post-Acute Care Hospitalization in Older Men: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(22):15150. https://doi.org/10.3390/ijerph192215150
Chicago/Turabian StyleMeza-Valderrama, Delky, Ester Marco, Elena Muñoz-Redondo, Andrea Morgado-Pérez, Marta Tejero Sánchez, Yulibeth Curbelo Peña, Elisabeth De Jaime, Lizzeth Canchucaja, Frank Meza Concepción, Stany Perkisas, and et al. 2022. "Musculoskeletal Ultrasound Shows Muscle Mass Changes during Post-Acute Care Hospitalization in Older Men: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 22: 15150. https://doi.org/10.3390/ijerph192215150