
Type D Personality and Health Behaviors in People Living with Obesity
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Ethics Approval
2.3. Research Tools
2.3.1. The Authors’ Survey
2.3.2. The Inventory of Health Behaviors (IZZ)
- Proper Eating Habits (PN1)—a dimension related to the type of food consumed;
- Positive Mental Attitude (PN2)—a dimension that includes psychological factors such as susceptibility to stress;
- Health Practices (PZ)—a dimension related to daily sleep or physical activity habits;
- Preventive Behaviors (ZP)—a dimension relating to respect for health recommendations and self-inquiry about health and disease.
2.3.3. The Multidimensional Health Locus of Control Scale, Version A (MHLC-A)
- Internal Dimension—control over one’s health depends on the individual;
- Powerful Others Dimension—self-health is the result of the influence of other people, especially medical personnel (External Dimension);
- Chance Dimension—the individual’s health is the result of chance and other factors of an external nature (External Dimension).
2.3.4. Type D Scale-14 (DS-14)
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
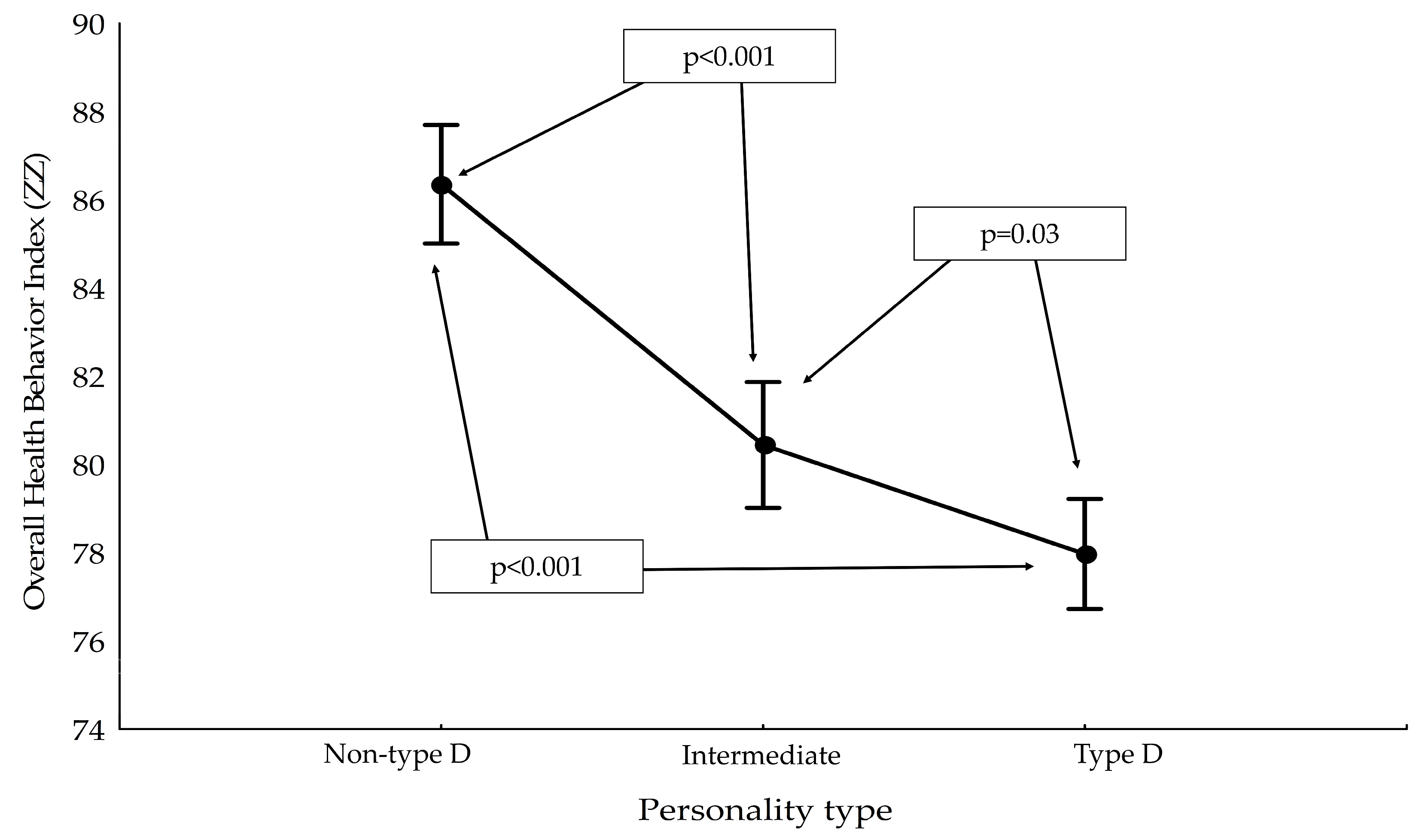
3.2. Health Behaviors Occurring among Obese Patients Due to Type D Personality
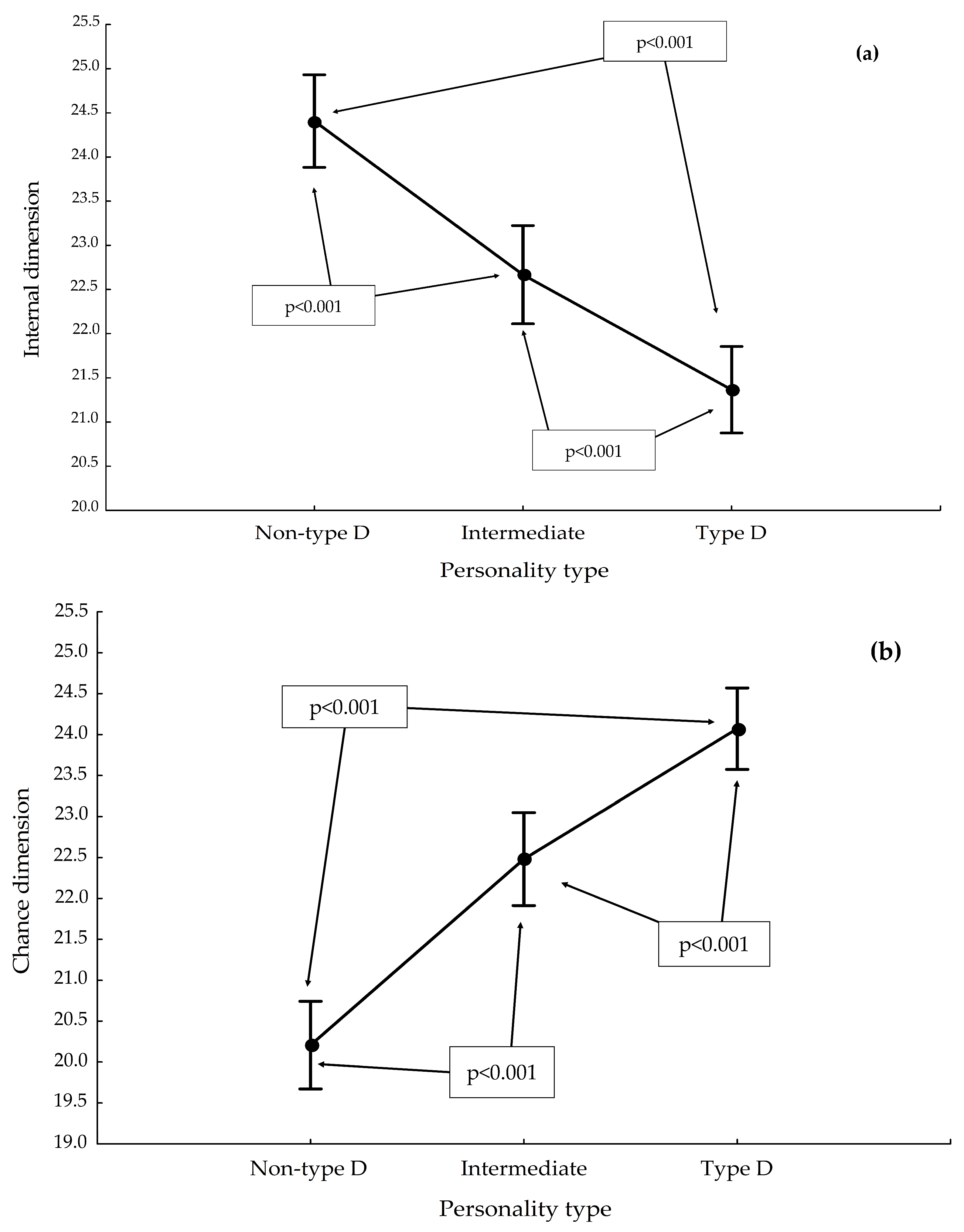
3.3. Health Locus of Control among the Obese Due to Type D Personality
3.4. Evaluation of the Correlation between MHLC-A and IZZ Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arroyo-Johnson, C.; Mincey, K.D. Obesity Epidemiology Worldwide. Gastroenterol. Clin. 2016, 45, 571–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hecker, J.; Freijer, K.; Hiligsmann, M.; Evers, S.M.A.A. Burden of Disease Study of Overweight and Obesity; the Societal Impact in Terms of Cost-of-Illness and Health-Related Quality of Life. BMC Public Health 2022, 22, 46. [Google Scholar] [CrossRef] [PubMed]
- Tremmel, M.; Gerdtham, U.-G.; Nilsson, P.M.; Saha, S. Economic Burden of Obesity: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2017, 14, 435. [Google Scholar] [CrossRef] [PubMed]
- Viinikainen, J.; Böckerman, P.; Pehkonen, J. Economic Costs of Obesity in Europe. In International Handbook of the Demography of Obesity; Garcia-Alexander, G., Poston Dudley, L., Jr., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 39–55. ISBN 978-3-031-10936-2. [Google Scholar]
- World Health Organization. WHO Fact Sheet: Obesity and Overweight. Available online: http://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 18 September 2022).
- OECD. The Heavy Burden of Obesity: The Economics of Prevention. In OECD Health Policy Studies; OECD Publishing: Paris, France, 2019; ISBN 9789264330047. [Google Scholar]
- Sala, M.; Rochefort, C.; Lui, P.P.; Baldwin, A.S. Trait Mindfulness and Health Behaviours: A Meta-Analysis. Health Psychol. Rev. 2020, 14, 345–393. [Google Scholar] [CrossRef]
- Statistics Poland. Health Status of Population in Poland in 2019; Statistics Poland: Warsaw, Poland, 2021.
- Gerlach, G.; Herpertz, S.; Loeber, S. Personality Traits and Obesity: A Systematic Review. Obes. Rev. 2015, 16, 32–63. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Shikora, S. Fighting Weight Bias and Obesity Stigma: A Call for Action. Obes. Surg. 2020, 30, 1623–1624. [Google Scholar] [CrossRef]
- Lunn, T.E.; Nowson, C.A.; Worsley, A.; Torres, S.J. Does Personality Affect Dietary Intake? Nutrition 2014, 30, 403–409. [Google Scholar] [CrossRef] [Green Version]
- Makara-Studzińska, M.; Zaborska, A. Otyłość a Obraz Własnego Ciała. Psychiatr. Pol. 2009, 43, 109–114. [Google Scholar]
- Jokela, M.; Hintsanen, M.; Hakulinen, C.; Batty, G.D.; Nabi, H.; Singh-Manoux, A.; Kivimäki, M. Association of Personality with the Development and Persistence of Obesity: A Meta-Analysis Based on Individual–Participant Data. Obes. Rev. 2013, 14, 315–323. [Google Scholar] [CrossRef]
- Sutin, A.R.; Terracciano, A. Personality and the Social Experience of Body Weight. Personal. Individ. Differ. 2019, 137, 76–79. [Google Scholar] [CrossRef]
- Bagnjuk, J.; König, H.-H.; Hajek, A. Personality Traits and Obesity. Int. J. Environ. Res. Public Health 2019, 16, 2675. [Google Scholar] [CrossRef] [PubMed]
- Sutin, A.R.; Terracciano, A. Five-Factor Model Personality Traits and the Objective and Subjective Experience of Body Weight. J. Personal. 2016, 84, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Armon, G.; Melamed, S.; Shirom, A.; Shapira, I.; Berliner, S. Personality Traits and Body Weight Measures: Concurrent and Across–Time Associations. Eur. J. Personal. 2013, 27, 398–408. [Google Scholar] [CrossRef]
- Sutin, A.R.; Ferrucci, L.; Zonderman, A.B.; Terracciano, A. Personality and Obesity across the Adult Life Span. J. Personal. Soc. Psychol. 2011, 101, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, R.J. Psychological Correlates of Habitual Diet in Healthy Adults. Psychol. Bull. 2017, 143, 53. [Google Scholar] [CrossRef]
- Worsley, A.; Wang, W.C.; Farragher, T. The Associations of Vegetable Consumption with Food Mavenism, Personal Values, Food Knowledge and Demographic Factors. Appetite 2016, 97, 29–36. [Google Scholar] [CrossRef]
- Horwood, S.; Anglim, J.; Tooley, G. Statistically modelling the relationships between Type D personality and social support, health behaviors and symptom severity in chronic illness groups. Psychol. Health 2016, 31, 1047–1063. [Google Scholar] [CrossRef] [Green Version]
- Denollet, J.; Sys, S.U.; Stroobant, N.; Rombouts, H.; Gillebert, T.C.; Brutsaert, D.L. Personality as Independent Predictor of Long-Term Mortality in Patients with Coronary Heart Disease. Lancet 1996, 347, 417–421. [Google Scholar] [CrossRef]
- Horwood, S.; Anglim, J.; Tooley, G. Type D Personality and the Five-Factor Model: A Facet-Level Analysis. Personal. Individ. Differ. 2015, 83, 50–54. [Google Scholar] [CrossRef]
- Stevenson, C.; Williams, L. Type D Personality, Quality of Life and Physical Symptoms in the General Population: A Dimensional Analysis. Psychol Health 2014, 29, 365–373. [Google Scholar] [CrossRef]
- Simson, U.; Nawarotzky, U.; Porck, W.; Friese, G.; Schottenfeld-Naor, Y.; Hahn, S.; Scherbaum, W.A.; Kruse, J. [Depression, anxiety, quality of life and type D pattern among inpatients suffering from diabetic foot syndrome]. Psychother. Psychosom. Med. Psychol. 2008, 58, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.D.; Ledoux, T.; Garcini, L.M.; Baker, J. Type D Personality and Chronic Pain: Construct and Concurrent Validity of the DS14. J. Clin. Psychol. Med. Settings 2009, 16, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Wiencierz, S.; Williams, L. Type D Personality and Physical Inactivity: The Mediating Effects of Low Self-Efficacy. J. Health Psychol. 2016, 22, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, S.; Zhang, G.; Yu, B.; Gao, X.; Dai, Z.; Yang, X.; Qiu, X.; Qiao, Z.; Zhou, J.; et al. Association between Type D Personality and In-Stent Restenosis in Patients Treated with Percutaneous Coronary Intervention: A Mediation Analysis of Dietary Patterns. J. Psychosom. Res. 2020, 138, 110244. [Google Scholar] [CrossRef] [PubMed]
- Booth, L.; Williams, L. Type D Personality and Dietary Intake: The Mediating Effects of Coping Style. J. Health Psychol 2015, 20, 921–927. [Google Scholar] [CrossRef]
- Timmermans, I.; Versteeg, H.; Duijndam, S.; Graafmans, C.; Polak, P.; Denollet, J. Social Inhibition and Emotional Distress in Patients with Coronary Artery Disease: The Type D Personality Construct. J. Health Psychol. 2017, 24, 1929–1944. [Google Scholar] [CrossRef]
- Mommersteeg, P.M.C.; Kupper, N.; Denollet, J. Type D Personality Is Associated with Increased Metabolic Syndrome Prevalence and an Unhealthy Lifestyle in a Cross-Sectional Dutch Community Sample. BMC Public Health 2010, 10, 714. [Google Scholar] [CrossRef]
- Cheng, F.; Lin, P.; Wang, Y.; Liu, G.; Li, L.; Yu, H.; Yu, B.; Zhao, Z.; Gao, X. Type D Personality and Coronary Atherosclerotic Plaque Vulnerability: The Potential Mediating Effect of Health Behavior. J. Psychosom. Res. 2018, 108, 54–60. [Google Scholar] [CrossRef]
- Yağcı, İ.; Taşdelen, Y.; Koç, O.; Kıvrak, Y. Type D Personality and Predictive Factors of Body Mass Index in Bariatric Surgery Candidates. J. Clin. Psychiatry 2021, 24, 334–341. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on Cardiovascular Disease Prevention in Clinical Practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (Constituted by Representatives of 10 Societies and by Invited Experts) Developed with the Special Contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [Green Version]
- Grande, G.; Romppel, M.; Barth, J. Association Between Type D Personality and Prognosis in Patients with Cardiovascular Diseases: A Systematic Review and Meta-Analysis. Ann. Behav. Med. 2012, 43, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Kupper, N.; Denollet, J. Type D Personality as a Risk Factor in Coronary Heart Disease: A Review of Current Evidence. Curr. Cardiol. Rep. 2018, 20, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina-Leyva, A.; Caparros-delMoral, I.; Ruiz-Carrascosa, J.C.; Naranjo-Sintes, R.; Jimenez-Moleon, J.J. Elevated Prevalence of Type D (Distressed) Personality in Moderate to Severe Psoriasis Is Associated with Mood Status and Quality of Life Impairment: A Comparative Pilot Study. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1710–1717. [Google Scholar] [CrossRef] [PubMed]
- Pasha, A.; Bahrainian, S.A.; Farahani, H. The Relationship between Type D Personality and the Stress Level of Life Events, Personality Traits and Anxiety Sensitivity in People with Breast Cancer. Ann. Médico Psychol. Rev. Psychiatr. 2022, 180, 527–532. [Google Scholar] [CrossRef]
- Husson, O.; Vissers, P.A.J.; Denollet, J.; Mols, F. The Role of Personality in the Course of Health-Related Quality of Life and Disease-Specific Health Status among Colorectal Cancer Survivors: A Prospective Population-Based Study from the PROFILES Registry. Acta Oncol. 2015, 54, 669–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mols, F.; Oerlemans, S.; Denollet, J.; Roukema, J.A.; van de Poll-Franse, L.V. Type D Personality Is Associated with Increased Comorbidity Burden and Health Care Utilization among 3080 Cancer Survivors. Gen. Hosp. Psychiatry 2012, 34, 352–359. [Google Scholar] [CrossRef]
- Horwood, S.; Chamravi, D.; Tooley, G. Examining the Prevalence of Type-D Personality in an Australian Population. Aust. Psychol. 2015, 50, 212–218. [Google Scholar] [CrossRef]
- Schoormans, D.; Husson, O.; Denollet, J.; Mols, F. Is Type D Personality a Risk Factor for All-Cause Mortality? A Prospective Population-Based Study among 2625 Colorectal Cancer Survivors from the PROFILES Registry. J. Psychosom. Res. 2017, 96, 76–83. [Google Scholar] [CrossRef]
- Kupper, N.; Denollet, J. Type D Personality as a Prognostic Factor in Heart Disease: Assessment and Mediating Mechanisms. J. Personal. Assess. 2007, 89, 265–276. [Google Scholar] [CrossRef]
- Slepecky, M.; Kotianova, A.; Prasko, J.; Majercak, I.; Kotian, M.; Gyorgyova, E.; Zatkova, M.; Chupacova, M.; Ociskova, M.; Sollar, T. Relation of Personality Factors and Life Events to Waist/Height Ratio and Percentage of Visceral Fat in Women and Men. Psychol. Res. Behav. Manag. 2019, 12, 499. [Google Scholar] [CrossRef] [Green Version]
- Martinac, M.; Babić, D.; Pavlović, M. Type D Personality and Metabolic Syndrome in Patients with Depression. Eur. Psychiatry 2017, 41, S533. [Google Scholar] [CrossRef]
- Villarroel, P.; Ortiz, M.S. Social Negativity and Obesity: Role of Negative Affectivity. Rev. Argent. De Clin. Psicol. 2019, 28, 744. [Google Scholar] [CrossRef]
- Harding, J.L.; Backholer, K.; Williams, E.D.; Peeters, A.; Cameron, A.J.; Hare, M.J.; Shaw, J.E.; Magliano, D.J. Psychosocial Stress Is Positively Associated with Body Mass Index Gain Over 5 Years: Evidence from the Longitudinal AusDiab Study. Obesity 2014, 21, 277–286. [Google Scholar] [CrossRef]
- Tomiyama, A.J. Stress and Obesity. Annu Rev. Psychol 2019, 70, 703–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohd-Sidik, S.; Lekhraj, R.; Foo, C.N. Prevalence, Associated Factors and Psychological Determinants of Obesity among Adults in Selangor, Malaysia. Int. J. Environ. Res. Public Health 2021, 18, 868. [Google Scholar] [CrossRef] [PubMed]
- Kleinridders, A.; Korosi, A.; Chattipakorn, S.C.; Sripetchwandee, J.; Chattipakorn, N. Links Between Obesity-Induced Brain Insulin Resistance, Brain Mitochondrial Dysfunction, and Dementia. Front. Endocrinol. 2018, 1, 496. [Google Scholar] [CrossRef] [Green Version]
- Rhea, E.M.; Salameh, T.S.; Logsdon, A.F.; Hanson, A.J.; Erickson, M.A.; Banks, W.A. Blood-Brain Barriers in Obesity. AAPS J. 2017, 19, 921–930. [Google Scholar] [CrossRef]
- Longo, M.; Zatterale, F.; Naderi, J.; Parrillo, L.; Formisano, P.; Raciti, G.A.; Beguinot, F.; Miele, C. Molecular Sciences Adipose Tissue Dysfunction as Determinant of Obesity-Associated Metabolic Complications. Int. J. Environ. Res. Public Health 2019, 20, 2358. [Google Scholar] [CrossRef] [Green Version]
- Roy, P.; Martinelli, I.; Moruzzi, M.; Maggi, F.; Amantini, C.; Micioni, M.V.; Bonaventura, D.; Cifani, C.; Amenta, F.; Tayebati, S.K.; et al. Ion Channels Alterations in the Forebrain of High-Fat Diet Fed Rats. Eur. J. Histochem. 2021, 65, 3305. [Google Scholar] [CrossRef]
- Martinelli, I.; Khosrow Tayebati, S.; Roy, P.; Micioni, M.V.; Bonaventura, D.; Moruzzi, M.; Cifani, C.; Amenta, F.; Tomassoni, D. Obesity-Related Brain Cholinergic System Impairment in High-Fat-Diet-Fed Rats. Int. J. Environ. Res. Public Health 2022, 14, 1243. [Google Scholar] [CrossRef]
- Marconcin, P.; Ihle, A.; Werneck, A.O.; Gouveia, E.R.; Ferrari, G.; Peralta, M.; Marques, A. The Association of Healthy Lifestyle Behaviors with Overweight and Obesity among Older Adults from 21 Countries. Nutrients 2021, 13, 315. [Google Scholar] [CrossRef] [PubMed]
- Gochman, D.S. Labels, Systems and Motives: Some Perspectives for Future Research and Programs. Health Educ. Q. 1982, 9, 167–174. [Google Scholar] [CrossRef]
- Parkerson, G.R., Jr.; Connis, R.T.; Broadhead, W.E.; Patrick, D.L.; Taylor, T.R.; Tse, C.-K.J. Disease-Specific versus Generic Measurement of Health-Related Quality of Life in Insulin-Dependent Diabetic Patients. Med. Care 1993, 31, 629–639. Available online: https://www.jstor.org/stable/3766113 (accessed on 31 October 2022). [CrossRef] [PubMed]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior: Theory, Research, and Practice, 5th ed.; John Wiley & Sons: San Francisco, CA, USA, 2015; ISBN 1118629000. [Google Scholar]
- Kasl, S.V.; Cobb, S. Health Behavior, Illness Behavior and Sick Role Behavior. Arch. Environ. Health Int. J. 1966, 12, 246–266. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Fuchs, R. Self-Efficacy and Health Behaviours. In Predicting Health Behavior: Research and Practice with Social Cognition Models; Conner, M., Norman, P., Eds.; Open University Press: Buckingham, UK, 1996; pp. 163–196. [Google Scholar]
- Juczyński, Z.; Ogińska, N. Zasoby Osobiste i Społeczne Sprzyjające Zdrowiu Jednostki; Wydawnictwo Uniwersytetu Łódzkiego: Łódź, Poland, 2003; ISBN 8371715870. [Google Scholar]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; John Wiley & Sons: San Francisco, CA, USA, 2008; ISBN 0470432489. [Google Scholar]
- Lee, K.M.; Hunger, J.M.; Tomiyama, A.J. Weight Stigma and Health Behaviors: Evidence from the Eating in America Study. Int. J. Obes. 2021, 45, 1499–1509. [Google Scholar] [CrossRef]
- Hashemi, N.; Sebar, B.; Harris, N. The Relationship between Cultural Capital and Lifestyle Health Behaviours in Young People: A Systematic Review. Public Health 2018, 164, 57–67. [Google Scholar] [CrossRef]
- Hagger, M.S.; Hamilton, K. Effects of Socio-Structural Variables in the Theory of Planned Behavior: A Mediation Model in Multiple Samples and Behaviors. Psychol. Health 2021, 36, 307–333. [Google Scholar] [CrossRef]
- Leman, M.A.; Claramita, M.; Rahayu, G.R. Predicting Factors on Modeling Health Behavior: A Systematic Review. Am. J. Health Behav. 2021, 45, 268–278. [Google Scholar] [CrossRef]
- Kim, J. Personality, Health Behaviours and Physical Health in Young Adulthood. Psychol. Health 2022, 37, 1164–1183. [Google Scholar] [CrossRef]
- Gilmour, J.; Williams, L. Type D Personality Is Associated with Maladaptive Health-Related Behaviours. J. Health Psychol. 2011, 17, 471–478. [Google Scholar] [CrossRef]
- Ginting, H.; van de Ven, M.; Becker, E.S.; Näring, G. Type D Personality Is Associated with Health Behaviors and Perceived Social Support in Individuals with Coronary Heart Disease. J. Health Psychol. 2014, 21, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.; Abbott, C.; Kerr, R. Health Behaviour Mediates the Relationship between Type D Personality and Subjective Health in the General Population. J. Health Psychol. 2015, 21, 2148–2155. [Google Scholar] [CrossRef] [Green Version]
- Gruszczyńska, M.; Bąk-Sosnowska, M.; Plinta, R. Zachowania Zdrowotne Jako Istotny Element Aktywności Życiowej Człowieka. Stosunek Polaków Do Własnego Zdrowia. Hygeia Public Health 2015, 50, 558–565. Available online: http://www.h-ph.pl/pdf/hyg-2015/hyg-2015-4-558.pdf (accessed on 31 October 2022).
- Ogińska-Bulik, N. Osobowość Typu D a Konsekwencje Stresu Zawodowego. Czas. Psychol. 2005, 11, 69–79. Available online: http://www.czasopismopsychologiczne.pl/files/articles/2005-11-osobowo-typu-d-a-konsekwencje-stresu-zawodowego.pdf (accessed on 31 October 2022).
- Juczyński, Z. Narzędzia Pomiaru w Promocji i Psychologii Zdrowia, 2nd ed.; Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warszawa, Poland, 2012; ISBN 978-83-60733-43-1. [Google Scholar]
- Wallston, K.A.; Strudler Wallston, B.; DeVellis, R. Development of the Multidimensional Health Locus of Control (MHLC) Scales. Health Educ. Monogr. 1978, 6, 160–170. [Google Scholar] [CrossRef]
- Denollet, J. DS14: Standard Assessment of Negative Affectivity, Social Inhibition, and Type D Personality. Psychosom. Med. 2005, 67, 89–97. [Google Scholar] [CrossRef]
- Juczyński, Z.; Ogińska-Bulik, N. Narzędzia Pomiaru Stresu i Radzenia Sobie Ze Stresem; Pracownia Testów Psychologicznych Polskiego Towarzystw Psychologicznego: Warszawa, Poland, 2012; ISBN 978-83-60733-47-9. [Google Scholar]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Levene, H. Robust Tests for Equality of Variances. In Contributions to Probability and Statistics: Essays in Honor of Harold Hotelling; Olkin, I., Ed.; Stanford University Press: Redwood City, CA, USA, 1960; pp. 278–292. [Google Scholar]
- Tukey, J.W. Comparing Individual Means in the Analysis of Variance. Biometrics 1949, 5, 99–114. [Google Scholar] [CrossRef]
- Spearman, C. The Proof and Measurement of Association between Two Things. Am. J. Psychol. 1904, 15, 72–101. [Google Scholar] [CrossRef]
- Stanisz, A. Przystępny Kurs Statystyki z Zastosowaniem STATISTICA PL Na Przykładach z Medycyny, 3rd ed.; StatSoft Polska: Kraków, Poland, 2007; Volume 1, ISBN 978-83-88724-18-3. [Google Scholar]
- Stanisz, A. Przystępny Kurs Statystyki z Zastosowaniem STATISTICA PL Na Przykładach z Medycyny, 2nd ed.; StatSoft Polska: Kraków, Poland, 2007; Volume 2, ISBN 978-83-88724-30-5. [Google Scholar]
- Chatterjee, A.; Gerdes, M.W.; Martinez, S.G. Identification of Risk Factors Associated with Obesity and Overweight—A Machine Learning Overview. Sensors 2020, 20, 2734. [Google Scholar] [CrossRef]
- Petridou, A.; Siopi, A.; Mougios, V. Exercise in the Management of Obesity. Metabolism 2019, 92, 163–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekuła, M.; Boniecka, I.; Paśnik, K. Ocena Zachowań Zdrowotnych, Żywieniowych i Poczucia Własnej Skuteczności Chorych z Otyłością Olbrzymią. Psychiatr. Pol. 2018, 105, 1125–1137. [Google Scholar] [CrossRef]
- Kawalec-Kajstura, E.; Reczek, A.; Porębska, A.; Brzostek, T.; Malinowska-Lipień, I. Zachowania Zdrowotne Pacjentów z Otyłością i Nadwagą. Pielęgniarstwo XXI Wieku 2011, 35, 27–33. Available online: https://ruj.uj.edu.pl/xmlui/bitstream/handle/item/165687/kawalec_et-al_zachowania_zdrowotne_pacjentow_z_otyloscia_i_nadwaga_2011.pdf?sequence=1&isAllowed=y (accessed on 31 October 2022).
- Moon, T.S.; Fox, P.E.; Somasundaram, A.; Minhajuddin, A.; Gonzales, M.X.; Pak, T.J.; Ogunnaike, B. The Influence of Morbid Obesity on Difficult Intubation and Difficult Mask Ventilation. J. Anesth. 2019, 33, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Gawlik, D. Diagnoza Zachowań Zdrowotnych Mieszkańców Województwa Śląskiego (Na Podstawie Badania Inwentarzem Zachowań Zdrowotnych Z. Juczyńskiego). Chowanna 2018, 51, 99–117. Available online: https://rebus.us.edu.pl/bitstream/20.500.12128/11215/1/Gawlik_diagnoza_zachowan_zdrowotnych_mieszkancow.pdf (accessed on 31 October 2022).
- Taboada-Vázquez, A.; Gonzalez-Rodriguez, R.; Gandoy-Crego, M.; Clemente, M. Personality Variables as Predictors of Health Services Consumption. Int. J. Environ. Res. Public Health 2021, 18, 5161. [Google Scholar] [CrossRef]
- Williams, L.; O’Connor, R.C.; Howard, S.; Hughes, B.M.; Johnston, D.W.; Hay, J.L.; O’Connor, D.B.; Lewis, C.A.; Ferguson, E.; Sheehy, N.; et al. Type-D Personality Mechanisms of Effect: The Role of Health-Related Behavior and Social Support. J. Psychosom. Res. 2008, 64, 63–69. [Google Scholar] [CrossRef]
- Wilson, K.E.; Dishman, R.K. Personality and Physical Activity: A Systematic Review and Meta-Analysis. Personal. Individ. Differ. 2015, 72, 230–242. [Google Scholar] [CrossRef]
- Svansdottir, E.; van den Broek, K.C.; Karlsson, H.D.; Gudnason, T.; Denollet, J. Type D Personality Is Associated with Impaired Psychological Status and Unhealthy Lifestyle in Icelandic Cardiac Patients: A Cross-Sectional Study. BMC Public Health 2012, 12, 42. [Google Scholar] [CrossRef] [Green Version]
- Kupper, N.; Pedersen, S.S.; Höfer, S.; Saner, H.; Oldridge, N.; Denollet, J. Cross-Cultural Analysis of Type D (Distressed) Personality in 6222 Patients with Ischemic Heart Disease: A Study from the International HeartQoL Project. Int. J. Cardiol. 2013, 166, 327–333. [Google Scholar] [CrossRef]
- Bruce, G.; Curren, C.; Williams, L. Type D Personality, Alcohol Dependence, and Drinking Motives in the General Population. J. Stud. Alcohol Drugs 2013, 74, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.; Bruce, G.; Knapton, C. Type D Personality Is Associated with Increased Desire for Alcohol in Response to Acute Stress. Stress Health 2018, 34, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.; Kang, J. Mediating Effect of Illness Perception on the Relationship between Type D Personality and Health Behaviors among Coronary Artery Disease Patients. Health Psychol. Open 2018, 5, 2055102918817228. [Google Scholar] [CrossRef] [PubMed]
- Conner, M.; Norman, P. Health Behaviour: Current Issues and Challenges. Psychol. Health 2017, 32, 895–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spring, B.; Moller, A.C.; Coons, M.J. Multiple Health Behaviours: Overview and Implications. J. Public Health 2012, 34, i3–i10. [Google Scholar] [CrossRef]
- Ek, S. Gender Differences in Health Information Behaviour: A Finnish Population-Based Survey. Health Promot. Int. 2015, 30, 736–745. [Google Scholar] [CrossRef] [Green Version]
- Hart, P.D.; Benavidez, G.; Erickson, J. Meeting Recommended Levels of Physical Activity in Relation to Preventive Health Behavior and Health Status Among Adults Corresponding Author. J. Prev. Med. Public Health 2017, 50. [Google Scholar] [CrossRef] [Green Version]
- Perissinotto, C.; Holt-Lunstad, J.; Periyakoil, V.S.; Covinsky, K. A Practical Approach to Assessing and Mitigating Loneliness and Isolation in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 657–662. [Google Scholar] [CrossRef]
- Lindsay Smith, G.; Banting, L.; Eime, R.; O’Sullivan, G.; van Uffelen, J.G.Z. The Association between Social Support and Physical Activity in Older Adults: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 56. [Google Scholar] [CrossRef] [Green Version]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An Overview of Systematic Reviews on the Public Health Consequences of Social Isolation and Loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef] [Green Version]
- Dogonchi, M.; Mohammadzadeh, F.; Moshki, M. Investigating the Relationship between Health Locus of Control and Health Behaviors: A Systematic Review. Open Public Health J. 2022, 15, e187494452208010. [Google Scholar] [CrossRef]
- Lindström, M.; Rosvall, M. Health Locus of Control and Mortality: A Population-Based Prospective Cohort Study. Public Health 2020, 185, 209–211. [Google Scholar] [CrossRef] [PubMed]
- Gore, J.S.; Griffin, D.P.; McNierney, D. Does Internal or External Locus of Control Have a Stronger Link to Mental and Physical Health? Psychol. Stud. 2016, 61, 181–196. [Google Scholar] [CrossRef]
- Náfrá, L.; Nakamoto, K.; Schulz, P.J. Is Patient Empowerment the Key to Promote Adherence? A Systematic Review of the Relationship between Self-Efficacy, Health Locus of Control and Medication Adherence. PLoS ONE 2017, 12, e0186458. [Google Scholar] [CrossRef] [Green Version]
- Grotz, M.; Hapke, U.; Lampert, T.; Baumeister, H. Health Locus of Control and Health Behaviour: Results from a Nationally Representative Survey. Psychol. Health Med. 2011, 16, 129–140. [Google Scholar] [CrossRef]
- Jacobs-Lawson, J.M.; Waddell, E.L.; Webb, A.K. Predictors of Health Locus of Control in Older Adults. Curr. Psychol. 2011, 30, 173. [Google Scholar] [CrossRef]
- Sargent-Cox, K.; Anstey, K.J. The Relationship between Age-Stereotypes and Health Locus of Control across Adult Age-Groups. Psychol. Health 2015, 30, 652–670. [Google Scholar] [CrossRef]
- Bailis, D.S.; Segall, A.; Chipperfield, J.G. Age, Relative Autonomy and Change in Health Locus of Control Beliefs: A Longitudinal Study of Members of a Health-Promotion Facility. J. Health Psychol. 2010, 15, 326–338. [Google Scholar] [CrossRef]
- Nowicki, S.; Ellis, G.; Iles-Caven, Y.; Gregory, S.; Golding, J. Events Associated with Stability and Change in Adult Locus of Control Orientation over a Six-Year Period. Personal. Individ. Differ. 2018, 126, 85–92. [Google Scholar] [CrossRef]
- Rafa, G.; Czyżowska, D. Kontrola Zdrowia a Wsparcie Społeczne i Satysfakcja z Życia w Okresie Późnej Dorosłości. Psychol. Rozw. 2020, 25, 87–106. [Google Scholar] [CrossRef]
- Awaworyi Churchill, S.; Munyanyi, M.E.; Prakash, K.; Smyth, R. Locus of Control and the Gender Gap in Mental Health. J. Econ. Behav. Organ. 2020, 178, 740–758. [Google Scholar] [CrossRef]
- Schmitt, D.P.; Long, A.E.; McPhearson, A.; O’Brien, K.; Remmert, B.; Shah, S.H. Personality and Gender Differences in Global Perspective. Int. J. Psychol. 2017, 52, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Cheung, M.W.-L.; Lo, B.C.Y. Relationship of Health Locus of Control with Specific Health Behaviours and Global Health Appraisal: A Meta-Analysis and Effects of Moderators. Health Psychol. Rev. 2016, 10, 460–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowicki, G.J.; Ślusarska, B.; Młynarsk, M.; Rudnicka-Drożak, E.; Chemperek, E.; Gawroński, M. The Health Locus of Control and the Declared Health Behaviour in a Group of HealthCare Professionals and People Working in Non-MediCal Professions. Pol. Przegląd Nauk. Zdrowiu 2017, 1, 38–48. [Google Scholar] [CrossRef]
- Deluga, A.; Bogdańska, P.; Dobrowolska, B.; Ślusarska, B.; Bartoszek, A.; Szczekala, K. The Health Locus of Control and Health Behaviours Declared by Students of Health Sciences. Pielegniarstwo XXI Wieku/Nurs. 21st Century 2018, 17, 10–17. [Google Scholar] [CrossRef]
- Marr, J.; Wilcox, S. Self-Efficacy and Social Support Mediate the Relationship Between Internal Health Locus of Control and Health Behaviors in College Students. Am. J. Health Educ. 2015, 46, 122–131. [Google Scholar] [CrossRef]
- Iskandarsyah, A.; de Klerk, C.; Suardi, D.R.; Sadarjoen, S.S.; Passchier, J. Health Locus of Control in Indonesian Women with Breast Cancer: A Comparison with Healthy Women. Asian Pac. J. Cancer Prev. 2014, 15, 9191–9197. [Google Scholar] [CrossRef] [Green Version]
- Afsahi, F.; Kachooei, M. Comparison of Health-Promoting Lifestyle and Health Locus of Control in Individuals with Hypertension and Healthy Individuals. Int. J. Behav. Sci. 2019, 13, 1111–1116. Available online: http://www.behavsci.ir/&url=http://www.behavsci.ir/article_97405_1cb434ec7aed309cd678414edd9c3727.pdf (accessed on 31 October 2022).
- Bąk-Sosnowska, M.; Gruszczyńska, M.; Wyszomirska, J.; Daniel-Sielańczyk, A. The Influence of Selected Psychological Factors on Medication Adherence in Patients with Chronic Diseases. Healthcare 2022, 10, 426. [Google Scholar] [CrossRef]
- Anastasiou, C.A.; Fappa, E.; Karfopoulou, E.; Gkza, A.; Yannakoulia, M. Weight Loss Maintenance in Relation to Locus of Control: The MedWeight Study. Behav. Res. Ther. 2015, 71, 40–44. [Google Scholar] [CrossRef]
- Radcliff, Z.; al Ghriwati, N.; Derlan, C.L.; Velazquez, E.; Halfond, R.; Corona, R. The Relationship between Latina/o Youth’s Internal Health Locus of Control, Cultural Factors, and Body Mass Index. J. Lat. Psychol 2018, 6, 190–203. [Google Scholar] [CrossRef]
- Montesi, L.; el Ghoch, M.; Brodosi, L.; Calugi, S.; Marchesini, G.; Dalle Grave, R. Long-Term Weight Loss Maintenance for Obesity: A Multidisciplinary Approach. Diabetes Metab. Syndr. Obes. Targets Ther. 2016, 9, 37. [Google Scholar] [CrossRef] [Green Version]
- Kamody, R.C.; Thurston, I.B.; Thomaseo Burton, E. Adolescent Engagement in a Binge-Eating Behavioral Health Intervention: Influence of Perceptions of Physical Appearance and Locus of Control. Children 2021, 8, 102. [Google Scholar] [CrossRef] [PubMed]
- Neymotin, F.; Nemzer, L.R.; Leon, M.; Cirulli, F. Locus of Control and Obesity. Front. Endocrinol. 2014, 5, 159. [Google Scholar] [CrossRef] [Green Version]
- Bares, C.B.; Gelman, S.A. Knowledge of Illness during Childhood: Making Distinctions between Cancer and Colds. Int. J. Behav. Dev. 2008, 32, 443–450. [Google Scholar] [CrossRef]
- Golding, J.; Iles-Caven, Y.; Ellis, G.; Gregory, S.; Nowicki, S. The Relationship between Parental Locus of Control and Adolescent Obesity: A Longitudinal Pre-Birth Cohort. Int. J. Obes. 2019, 43, 724–734. [Google Scholar] [CrossRef]
- Groth, N.; Schnyder, N.; Kaess, M.; Markovic, A.; Rietschel, L.; Moser, S.; Michel, C.; Schultze-Lutter, F.; Schmidt, S.J. Coping as a Mediator between Locus of Control, Competence Beliefs, and Mental Health: A Systematic Review and Structural Equation Modelling Meta-Analysis. Behav. Res. Ther. 2019, 121, 103442. [Google Scholar] [CrossRef]
- Wu, J.R.; Song, E.K.; Moser, D.K. Type D Personality, Self-Efficacy, and Medication Adherence in Patients with Heart Failure—A Mediation Analysis. Heart Lung 2015, 44, 276–281. [Google Scholar] [CrossRef] [Green Version]
- Sahoo, S.; Padhy, S.K.; Padhee, B.; Singla, N.; Sarkar, S. Role of Personality in Cardiovascular Diseases: An Issue That Needs to Be Focused Too! Indian Heart J. 2018, 70, S471–S477. [Google Scholar] [CrossRef]
- Xenaki, N.; Bacopoulou, F.; Kokkinos, A.; Nicolaides, N.C.; Chrousos, G.P.; Darviri, C. Impact of a Stress Management Program on Weight Loss, Mental Health and Lifestyle in Adults with Obesity: A Randomized Controlled Trial. J. Mol. Biochem. 2018, 7, 78. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6296480/ (accessed on 31 October 2022).




{kind=link}
{kind=link}
{kind=link}
| Male | Sten Scores | Female |
|---|---|---|
| ZZ (Score) | ZZ (Score) | |
| 24–50 | 1 | 24–53 |
| 51–58 | 2 | 54–62 |
| 59–65 | 3 | 63–70 |
| 66–71 | 4 | 71–77 |
| 72–78 | 5 | 78–84 |
| 79–86 | 6 | 85–91 |
| 87–93 | 7 | 92–98 |
| 94–101 | 8 | 99–104 |
| 102–108 | 9 | 105–111 |
| 109–120 | 10 | 112–120 |
| Personality Type | Total Scores for the Subscale | |
|---|---|---|
| Negative Affectivity | Social Inhibition | |
| Type D personality | ≥10 | ≥10 |
| Intermediate personality | ≥10 | <10 |
| <10 | ≥10 | |
| Non-type D personality | <10 | <10 |
| IZZ | Value from This Study X ± SD | 95% CI of the Mean (X) | Normative Value X ± SD | t | pt |
|---|---|---|---|---|---|
| Overall Health Behavior Index (ZZ) | 81.4 ± 9.0 | 80.6–82.3 | 81.82 ± 14.16 | −0.91 | >0.05 |
| Proper Eating Habits | 3.5 ± 0.6 | 3.4–3.5 | 3.22 ± 0.76 | 10.84 | <0.0001 |
| Preventive Behaviors | 3.1 ± 0.5 | 3.0–3.1 | 3.42 ± 0.78 | −10.94 | <0.0001 |
| Positive Mental Attitude | 3.4 ± 0.5 | 3.3–3.4 | 3.52 ± 0.66 | −4.16 | <0.0001 |
| Health Practices | 3.4 ± 0.4 | 3.4–3.5 | 3.32 ± 0.85 | 6.97 | <0.0001 |
| Dependent Variable—Health Behavior | Factor—Predictor | Predictor Characteristics | OR (95% CI) |
|---|---|---|---|
| The undertaking of health-promoting behaviors | Age (years) | <36 | 1 |
| 31–40 | 0.64 (0.25–1.64) | ||
| 41–50 | 0.19 (0.08–0.48) | ||
| 51–60 | 0.12 (0.05–0.29) | ||
| 61–70 | 0.09 (0.03–0.23) | ||
| >71 | 0.04 (0.01–0.13) | ||
| Personality type | Non-type D | 1 | |
| Intermediate | 0.32 (0.18–0.56) | ||
| Type D | 0.18 (0.10–0.32) |
| Internal Dimension Me (Q1–Q3) | Powerful Others Dimension Me (Q1–Q3) | Chance Dimension Me (Q1–Q3) | |
|---|---|---|---|
| Gender | |||
| Female | 22.0 (21.0–24.0) | 23.0 (22.0–25.0) | 23.0 (19.0–24.0) |
| Male | 22.0 (21.0–25.0) | 22.0 (20.0–24.0) | 23.0 (21.0–25.0) |
| pM-W | 0.9 | <0.0001 | 0.1 |
| Age (years) | |||
| ≤30 | 26.0 (23.0–28.0) | 22.0 (21.0–24.0) | 23.0 (19.0–24.0) |
| 31–40 | 24.0 (22.0–27.0) | 22.0 (21.0–24.0) | 22.0 (19.0–24.0) |
| 41–50 | 23.0 (22.0–25.0) | 23.0 (21.0–24.0) | 22.0 (18.0–24.0) |
| 51–60 | 22.0 (20.0–23.0) | 23.0 (22.0–25.0) | 23.0 (21.0–25.0) |
| 61–70 | 21.0 (20.0–22.0) | 23.5 (22.0–25.0) | 24.0 (22.0–26.0) |
| >70 | 20.0 (18.0–22.0) | 22.0 (20.0–26.0) | 23.0 (22.0–26.0) |
| Wartość pK-W | 0.0001 1 | 0.07 | 0.003 2 |
| Place of residence | |||
| Village | 23.0 (21.0–25.0) | 22.0 (20.0–24.0) | 23.0 (19.0–25.0) |
| City, with populations <50,000 | 23.0 (17.0–25.0) | 22.0 (21.0–23.0) | 24.0 (22.0–25.0) |
| City, with populations 50,000–100,000 | 22.0 (19.5–23.0) | 22.0 (21.0–24.0) | 23.0 (20.0–24.0) |
| City, with populations 100,000–250,000 | 22.0 (20.0–24.0) | 23.0 (22.0–25.0) | 23.0 (20.0–25.0) |
| City, with populations >250,000 | 23.0 (21.0–25.0) | 23.0 (21.0–25.0) | 22.0 (20.0–24.0) |
| Wartość pK-W | 0.051 | 0.07 | 0.5 |
| Educational level | |||
| Primary education | 22.0 (20.0–23.0) | 23.0 (21.0–25.0) | 23.0 (21.0–25.0) |
| Professional education | 22.0 (21.0–24.0) | 23.0 (21.0–24.0) | 23.0 (20.0–25.0) |
| Secondary education | 22.0 (21.0–24.0) | 23.0 (21.0–25.0) | 23.0 (21.0–25.0) |
| Higher education | 23.0 (21.0–25.0) | 23.0 (21.0–25.0) | 22.0 (19.0–24.0) |
| Wartość pK-W | 0.4 | 1.0 | 0.3 |
| Classes of obesity | |||
| Obese class I (BMI: 30.0–34.9 kg/m2) | 22.0 (21.0–24.0) | 23.0 (21.0–25.0) | 22.0 (20.0–25.0) |
| Obese class II (BMI: 35.0–39.9 kg/m2) | 22.0 (21.0–25.0) | 23.0 (21.0–24.0) | 22.0 (20.0–25.0) |
| Obese class III (BMI: ≥40.0 kg/m2) | 22.0 (21.0–24.0) | 23.0 (21.0–24.0) | 23.0 (20.0–25.0) |
| Wartość pK-W | 0.4 | 0.9 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buczkowska, M.; Górski, M.; Domagalska, J.; Buczkowski, K.; Nowak, P. Type D Personality and Health Behaviors in People Living with Obesity. Int. J. Environ. Res. Public Health 2022, 19, 14650. https://doi.org/10.3390/ijerph192214650
Buczkowska M, Górski M, Domagalska J, Buczkowski K, Nowak P. Type D Personality and Health Behaviors in People Living with Obesity. International Journal of Environmental Research and Public Health. 2022; 19(22):14650. https://doi.org/10.3390/ijerph192214650
Chicago/Turabian StyleBuczkowska, Marta, Michał Górski, Joanna Domagalska, Krzysztof Buczkowski, and Przemysław Nowak. 2022. "Type D Personality and Health Behaviors in People Living with Obesity" International Journal of Environmental Research and Public Health 19, no. 22: 14650. https://doi.org/10.3390/ijerph192214650