

Development and Validation of a Meta-Instrument for Nursing Assessment in Adult Hospitalization Units (VALENF Instrument) (Part I)

 , , , ,
, , , ,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Participants and Sample
2.3. Variables and Instruments
- Barthel index: This assesses the functional capacity (or dependency level) to carry out basic activities of daily life. It comprises 10 items, with a total score range between 0 and 100, and groups the patients into four levels (total dependency = zero–15; severe dependency = 20–35; moderate dependency = 40–55; low dependency > 60 points) [35]. González et al. (2017) [36] validated this in a Spanish population over 65 years old admitted to hospitalization units with good internal consistency (α > 0.8) and good construct validity (RMSEA < 0.08; LI > 0.9).
- Braden index: This assesses the risk of pressure injuries. It comprises six items with four response categories. Its scores range from six to 23 points, and it is classified into four categories (high risk = 6–12; moderate risk = 13–14; low risk = 15–18; no risk = 19–23). According to Moreno Pina et al. (2007) [37], it is considered the most appropriate instrument to assess the risk of pressure injuries in the context of the study (sensitivity = 0.27–1; specificity = 0.26–0.92; positive predictive value = 0.08–0.77, negative predictive value = 0.71–1).
- Downton scale: This assesses the risk of falls and comprises five items that score zero or one points. Higher scores indicate higher risk of falls, and scores above two points indicate a high risk of falls (sensitivity = 0.58; specificity = 0.62) [38].
2.4. Data Collection
2.5. Development and Data Analysis Procedures
2.6. Ethical Considerations
3. Results
3.1. Descriptive Analysis of the Sample
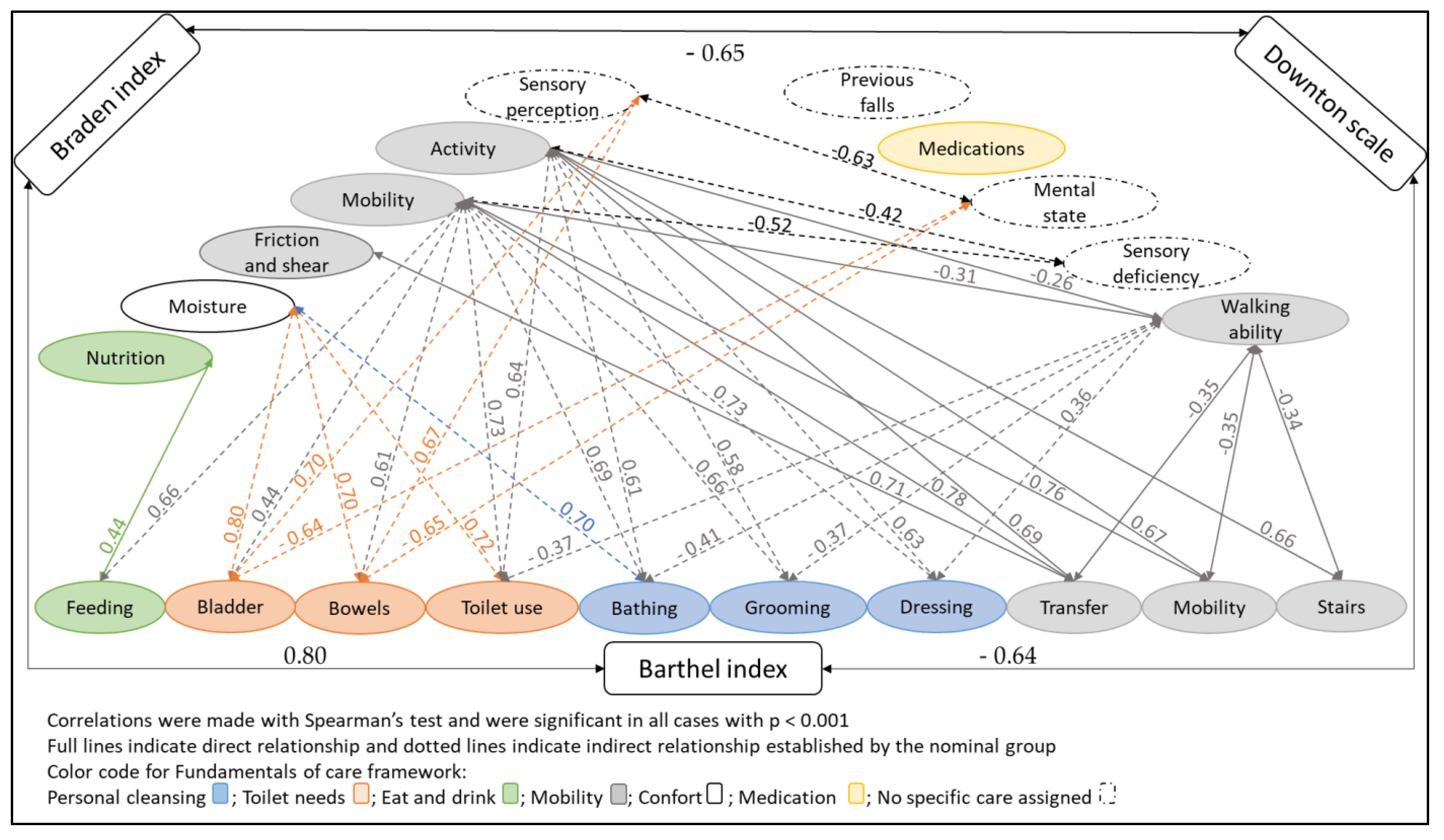
3.2. Bivariant Analysis of the Assessment Instruments
3.3. Development of the VALENF Instrument
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, J.A.; Cooper, A.L.; Albrecht, M.A. Development and content validation of the Burden of Documentation for Nurses and Midwives (BurDoNsaM) survey. J. Adv. Nurs. 2020, 76, 1273–1281. [Google Scholar] [CrossRef]
- Dunn Lopez, K.; Chin, C.L.; Leitão Azevedo, R.F.; Kaushik, V.; Roy, B.; Schuh, W.; Banks, K.; Sousa, V.; Morrow, D. Electronic health record usability and workload changes over time for provider and nursing staff following transition to new EHR. Appl. Ergon. 2021, 93, 103359. [Google Scholar] [CrossRef]
- Walker, R.M.; Burmeister, E.; Jeffrey, C.; Birgan, S.; Garrahy, E.; Andrews, J.; Hada, A.; Aitken, L.M. The impact of an integrated electronic health record on nurse time at the bedside: A pre-post continuous time and motion study. Collegian 2019, 27, 63–74. [Google Scholar] [CrossRef] [Green Version]
- Cooper, A.L.; Brown, J.A.; Eccles, S.P.; Cooper, N.; Albrecht, M.A. Is nursing and midwifery clinical documentation a burden? An empirical study of perception versus reality. J. Clin. Nurs. 2021, 30, 1645–1652. [Google Scholar] [CrossRef] [PubMed]
- Charalambous, L.; Goldberg, S. ‘Gaps, mishaps and overlaps’. Nursing documentation: How does it affect care? J. Res. Nurs. 2016, 21, 638–648. [Google Scholar] [CrossRef] [Green Version]
- Berman, A.; Snyder, S.; Frandsen, G. Kozier & Erb’s Fundamentals of Nursing: Concepts, Process and Practice, 9th ed.; Pearson: London, UK, 2016. [Google Scholar]
- Gray, L.C.; Beattie, E.; Boscart, V.M.; Henderson, A.; Hornby-Turner, Y.C.; Hubbard, R.E.; Wood, S.; Peel, N.M. Developrment and Testing of the interRAI Acute Care: A Standardized Assessment Administered by Nurses for Patients Admitted to Acute Care. Health Serv. Insights 2018, 111, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Gasperini, B.; Pelusi, G.; Frascati, A.; Sarti, D.; Dolcini, F.; Espinosa, E.; Prospero, E. Predictors of adverse outcomes using a multidimensional nursing assessment in an Italian community hospital. PLoS ONE 2021, 16, e0249630. [Google Scholar] [CrossRef]
- Lee, S.; Jeon, M.Y.; Kim, E.O. Implementation of Structured Documentation and Standard Nursing Statements: Perceptions of Nurses in Acute Care Settings. Comp. Inform. Nurs. 2019, 37, 266–275. [Google Scholar] [CrossRef]
- Swietlik, M.; Sengstack, P.P. An Evaluation of Nursing Admission Assessment Documentation to Identify Opportunities for Burden Reduction. J. Inform. Nurs. 2020, 5, 6–11. [Google Scholar]
- Muinga, N.; Abejirinde, I.O.; Paton, C.; English, M.; Zweekhorst, M. Designing paper-based records to improve the quality of nursing documentation in hospitals: A scoping review. J. Clin. Nurs. 2021, 30, 56–71. [Google Scholar] [CrossRef]
- Dante, A.; Mecugni, D.; Moga, M.M.; Graceffa, G.; Palese, A. Gli sprechi nella pratica clinica infermieristica: Risultati di uno studio fenomenologico. Ig. E Sanita Pubblica 2015, 71, 2015–2224. [Google Scholar]
- Palese, A.; Marini, E.; Guarnier, A.; Barelli, P.; Zambiasi, P.; Allegrini, E.; Bazoli, L.; Casson, P.; Grassetti, L. Overcoming redundancies in bedside nursing assessments by validating a parsimonious meta-tool: Findings from a methodological exercise study. J. Eval. Clin. Prac. 2016, 22, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Munroe, B.; Curtis, K.; Considine, J.; Buckley, T. The impact structured patient assessment frameworks have on patient care: An integrative review. J. Clin. Nurs. 2013, 22, 2991–3005. [Google Scholar] [CrossRef] [PubMed]
- Morales-Asencio, J.M.; Porcel-Gálvez, A.M.; Oliveros-Valenzuela, R.; Rodríguez-Gómez, S.; Sánchez-Extremera, L.; Serrano-López, F.A.; Aranda-Gallardo, M.; Canca-Sánchez, J.C.; Barrientos-Trigo, S. Design and validation of the INICIARE instrument, for the assessment of dependency level in acuteli ill hospitalised patients. J. Clin. Nurs. 2015, 24, 761–777. [Google Scholar] [CrossRef]
- Gengo E Silva Butcher, R.C.; Jones, D.A. An integrative review of comprehensive nursing assessment tools developed based on Gordon’s Eleven Functional Health Patterns. Int. J. Nurs. Know. 2021, 32, 294–307. [Google Scholar] [CrossRef]
- Douglas, C.; Booker, C.; Fox, R.; Windsor, C.; Osborne, S.; Gardner, G. Nursing physical assessment for patient safety in general wards: Reaching consensus on core skills. J. Clin. Nurs. 2016, 25, 1890–1900. [Google Scholar] [CrossRef] [Green Version]
- Buurman, B.M.; van Munster, B.C.; Korevaar, J.C.; de Hann, R.J.; de Rooij, S.E. Variability in measuring (instrumental) activities of daily living functioning and functional decline in hospitalized older medical patients: A systematic review. J. Clin. Epidemiol. 2011, 64, 619–627. [Google Scholar] [CrossRef] [Green Version]
- Arndt, J.V.; Kelechi, T.J. An overview of instruments for wound and skin assessment and healing. J. Wound Ostomy Cont. Nurs. 2014, 42, 17–23. [Google Scholar] [CrossRef]
- Aranda-Gallardo, M.; Morales-Asencio, J.M.; Canca-Sanchez, J.C.; Barrero-Sojo, S.; Perez-Jimenez, C.; Morales-Fernandez, A.; de Luna-Rodriguez, M.E.; Moya-Suarez, A.B.; Mora-Banderas, A.M. Instruments for assessing the risk of falls in acute hospitalized patients: A systematic review and meta-analysis. BMC Health Serv. Res. 2013, 13, 122. [Google Scholar] [CrossRef] [Green Version]
- Moore, E.C.; Tolley, C.L.; Bates, D.W.; Slight, S.P. A systematic review of the impact of health information technology on nurse’s time. J. Am. Med. Inf. Assoc. 2020, 27, 798–807. [Google Scholar] [CrossRef]
- Paans, W.; Sermeus, W.; Nieweg, R.M.; van der Schans, C.P. Prevalence of accurate nursing documentation in patient records. J. Adv. Nurs. 2010, 66, 2481–2489. [Google Scholar] [CrossRef] [PubMed]
- Lindo, J.; Stennett, R.; Stephenson-Wilson, K.; Barrett, K.A.; Bunnaman, D.; Anderson-Johnson, P.; Waugh-Brown, V.; Wint, Y. An Audit of Nursing Documentation at Three Public Hospitals in Jamaica. J. Nurs. Scholarsh. 2016, 48, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Iula, A.; Ialungo, C.; De Waure, C.; Raponi, M.; Burgazzoli, M.; Zega, M.; Galleti, C.; Damiani, G. Quality of Care: Ecological Study for the Evaluation of Completeness and Accuracy in Nursing Assessment. Int. J. Environ. Res. Public Health. 2020, 17, 3259. [Google Scholar] [CrossRef] [PubMed]
- Asmirajanti, M.; Hamid, A.; Hariyati, R. Nursing care activities based on documentation. BMC Nurs. 2019, 18, 32. [Google Scholar] [CrossRef] [PubMed]
- Bååth, C.; Hall-Lord, M.L.; Johansson, I.; Larsson, B.W. Nursing assessment documentation and care of hip fracture patients’ skin. J. Orthop. Nurs. 2007, 11, 4–14. [Google Scholar] [CrossRef]
- Bail, K.; Merrick, E.; Bridge, C.; Redley, B. Documenting patient risk and nursing interventions: Record audit. Asust. J. Adv. Nurs. 2021, 38, 32–37. [Google Scholar] [CrossRef]
- Redley, B.; Raggatt, M. Use of standard risk screening and assessment forms to prevent farm to older people in Australian hospitals: A mixed methods study. BMJ Qual. Saf. 2017, 26, 704–713. [Google Scholar] [CrossRef]
- Needleman, J. Increasing acuity, increasing technology, and the changing demands on nurses. Nurs. Econ. 2013, 31, 200–202. [Google Scholar]
- De Groot, K.; Triemstra, M.; Paans, W.; Francke, A.L. Quality criteria, instruments, and requirements for nursing documentation: A systematic review of systematic reviews. J. Adv. Nurs. 2019, 75, 1379–1393. [Google Scholar] [CrossRef] [Green Version]
- Palese, A.; Colognese, S.; Pellicciari, C.; Mecugni, D.; VISPA’s group. Implemetation strategies of measurement instruments and their validity as adopted in Italian hsopital nursing practice: An Italian cross-sectional study. Int. J. Nurs. Knowl. 2012, 23, 75–85. [Google Scholar] [CrossRef]
- Palestini, L.; Anzivino, F.; Nicoli, M.A. La Valutazione Multidimensionale Dle Paziente Anziano. Applicazione Di Strumenti Nei Percorsi Di Continuità Assistenziale. 2012. Available online: https://assr.regione.emilia-romagna.it/pubblicazioni/dossier/doss218 (accessed on 22 August 2022).
- Anthoine, E.; Moret, L.; Regnault, A.; Sébille, V.; Hardouin, J.B. Sample size used to validate a scale: A review of publications on newly-developed patient reported outcomes measures. Health Qual. Life Outcomes 2014, 12, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Formiga, F.; Moreno-Gonzalez, R.; Chivite, D. High comorbidity, measured by the Charlson Comorbidity Index, associates with higher 1-year mortality risks in elderly patients experiencing a first acute heart failure hospitalization. Aging Clin. Exp. Res. 2018, 30, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Baztán, J.J.; Pérez, J.; Alarcón, T.; San Crsitóbal, E.; Izquierdo, G.; Manzarbeitia, J. Índice de Barthel: Instrumento válido para la valoración funcional de pacientes con enfermedad cerebrovascular. Rev. Esp. Geriatr. Gerontol. 1993, 28, 32–40. [Google Scholar]
- González, N.; Bilbao, A.; Forjaz, M.J.; Ayala, A.; Orive, M.; Garcia-Gutierrez, S.; Hayas, C.L.; Quintana, J.M.; OFF (Older Falls Fracture)-IRYSS group. Psychometric characteristics of the Spanish version of the Barthel Index. Aging Clin. Exp. Res. 2018, 30, 489–497. [Google Scholar] [CrossRef]
- Moreno-Pina, J.P.; Richart-Martínez, M.; Guirao-Goris, J.A.; Duarte-Climents, G. Análisis de las escalas de valoración del riesgo de desarrollar una úlcera por presión. Enferm. Clin. 2007, 17, 186–197. [Google Scholar] [CrossRef]
- Bueno-García, M.J.; Roldán-Chicano, M.T.; Rodríguez-Tello, J.; Meroño-Rivera, M.D.; Dávila-Martínez, R.; Berenguer-García, N. Características de la escala Downton en la valoración del riesgo de caídas en pacientes hospitalizados. Enferm. Clin. 2017, 27, 227–234. [Google Scholar] [CrossRef]
- Hinkle, D.E.; Wiersma, W.; Jurs, S.G. Applied Statistics for the Behavioral Sciences, 5th ed.; CENGAGE Learning; Houghton Mifflin: Boston, MA, USA, 2002. [Google Scholar]
- Feo, R.; Conroy, T.; Jangland, E.; Muntlin Athlin, Å.; Brovall, M.; Parr, J.; Blomberb, K.; Kitson, A. Towards a standardised definition for fundamental care: A modified Delphi study. J. Clin. Nurs. 2017, 27, 2285–2299. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 8th ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2021. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- De Raadt, A.; Warrens, M.J.; Bosker, R.J.; Kiers, H.A.L. A Comparison of Reliability Coefficients for Ordinal Rating Scales. J. Classif. 2021, 38, 519–543. [Google Scholar] [CrossRef]
- Palese, A.; Cuel, M.; Zanella, P.; Zambiasi, P.; Guarnier, A.; Allegrini, E.; Saiani, L. Nursing care received by older patients in Italian medical units: Findings from an explorative study. Aging Clin. Exp. Res. 2013, 25, 707–710. [Google Scholar] [CrossRef]
- De Morton, N.A.; Keating, J.L.; Davidson, M. Rasch analysis of the barthel index in the assessment of hospitalized older patients after admission for an acute medical condition. Arch. Phys. Med. Rehabil. 2008, 89, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Mannucci, P.M.; Nobili, A.; Reposi, I.; Barbagallo, M.; Dominguez, L.J. Multimorbidity and polypharmacy in the elderly: Lessons from REPOSI. Intern. Emerg. Med. 2014, 9, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Paans, W.; Sermeus, W.; Nieweg, R.M.; Krijnen, W.P.; van der Schans, C.P. Do knowledge, knowledge sources and reasoning skills affect the accuracy of nursing diagnoses? A randomised study. BMC Nurs. 2012, 11, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frigstad, S.A.; Nøst, T.H.; André, B. Implementation of Free Text Format Nursing Diagnoses at a University Hospital’s Medical Department. Exploring Nurses’ and Nursing Students’ Experiences on Use and Usefulness. A Qualitative Study. Nurs. Res. Pract. 2015, 2015, 179275. [Google Scholar] [CrossRef]
- Conley, D.; Schultz, A.A.; Selvin, R. The challenge of predicting patients at risk for falling: Development of the Conley Scale. Medsurg. Nurs. 1999, 8, 348–354. [Google Scholar]
- Ruggieri, M.; Palmisano, B.; Fratocchi, G.; Santilli, V.; Mollica, R.; Berardi, A.; Galeoto, G. Validated Fall Risk Assessment Tools for Use with Older Adults: A Systematic Review. Phys. Occup. Ther. Geriatr. 2018, 36, 331–353. [Google Scholar] [CrossRef]
- Aranda-Gallardo, M.; Enriquez de Luna-Rodriguez, M.; Vazquez-Blanco, M.J.; Canca-Sanchez, J.C.; Moya-Suarez, A.B.; Morales-Asencio, J.M. Diagnostic validity of the STRATIFY and Downton instruments for evaluating the risk of falls by hospitalised acute-care patients: A multicentre longitudinal study. BMC Health Serv. Res. 2017, 17, 277. [Google Scholar] [CrossRef] [Green Version]
- Strini, V.; Schiavolin, R.; Prendin, A. Fall Risk Assessment Scales: A Systematic Literature Review. Nurs. Rep. 2022, 11, 430–443. [Google Scholar] [CrossRef]
- Blaylock, A.; Cason, C.L. Discharge planning predicting patients’ needs. J. Gerontol. Nurs. 1992, 18, 5–10. [Google Scholar] [CrossRef]
- Ladios-Martín, M.; Cabañero-Martínez, M.J.; Fernández-de-Maya, J.; Ballesta-López, F.J.; Belso-Garzas, A.; Zamora-Aznar, F.M.; Cabrero-García, J. Development of a predictive inpatient falls risk model usinng machine learning. J. Nurs. Manag. 2022, 1–10. [Google Scholar] [CrossRef]
- Galvao, Y.M.; Ferreira, J.; Albuquerque, V.A.; Barros, P.; Fernandes, B.J.T. A multimodal approach using deep learning for fall detection. Expert Syst. Appl. 2022, 168, 114226. [Google Scholar] [CrossRef]
- Ferrús, L.; Honrado, G.; Pintado, D. Grupos relacionados con el diagnóstico e intensidad de cuidados de enfermería: Variabilidad y homogeneidad de los cuidados enfermeros. Enf. Clín. 2001, 11, 239–246. [Google Scholar] [CrossRef]
- Pirson, M.; Delo, C.; Di Pierdomenico, L.; Laport, N.; Biloque, V.; Leclercq, P. Variability of nursing care by APR-DRG and by severity of illness in a sample of nine Belgian hospitals. BMC Nurs. 2013, 12, 26. [Google Scholar] [CrossRef] [Green Version]
- Hopfe, M.; Stucki, G.; Marshall, R.; Twomey, C.D.; Üstün, T.B.; Prodinger, B. Capturing patients’ needs in casemix: A systematic literature review on the value of adding functioning information in reimbursement systems. BMC Health Serv. Res. 2016, 16, 40. [Google Scholar] [CrossRef] [Green Version]
- Gluckman, T.J.; Spinelli, K.J.; Wang, M.; Yazdani, A.; Grunkemeier, G.; Bradley, S.M.; Wasfy, J.H.; Goyal, A.; Oseran, A.; Joynt Maddox, K.E. Trends in Diagnosis Related Groups for Inpatient Admissions and Associated Changes in Payment from 2012 to 2016. JAMA Netw. Open 2020, 3, e2028470. [Google Scholar] [CrossRef]
- Laake, K.; Laake, P.; Ranhoff, A.H.; Sveen, U.; Wyller, T.B.; Bautz-Holter, E. The Barthel ADL Index: Factor Structure depends upon the Category of Patient. Age Ageing 1995, 24, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Sardo, P.; Guedes, J.; Alvarelhão, J.; Machado, P.; Melo, E. Pressure ulcer incidence and Braden subscales: Retrospective cohort analysis in general wards of a Portuguese hospital. J. Tissue Viability 2018, 27, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Cabañero-Martínez, M.J.; Cabrero-García, J.; Richart-Martínez, M.; Muñoz-Mendoza, C.L. The Spanish versions of the Barthel index (BI) and the Katz index (KI) of activities of daily living (ADL): A structured review. Arch. Gerontol. Geriatr. 2009, 49, e77–e84. [Google Scholar] [CrossRef]
- Huang, C.; Ma, Y.; Wang, C.; Jiang, M.; Yuet Foon, L.; Lv, L.; Han, L. Predictive validity of the braden scale for pressure injury risk assessment in adults: A systematic review and meta-analysis. Nurs. Open 2021, 8, 2194–2207. [Google Scholar] [CrossRef]
- Nadeau, C.; Bengio, Y. Inference for the Generalization Error. Mach. Learn. 2003, 52, 239–281. [Google Scholar] [CrossRef]


{kind=link}
| Variable | m (ds) 1 | |
|---|---|---|
| Age | 67.69 (17.92) | |
| Charlson index | 3.68 (2.5) | |
| Barthel index | 78.38 (33.77) | |
| Braden index | 18.97 (3.86) | |
| Downton scale | 1.15 (1.23) | |
| % (n) 2 | ||
| Sex | Male | 52.1 (705) |
| Female | 47.9 (647) | |
| Process type | Medical | 66.9 (905) |
| Surgical | 33.1 (447) | |
| Admission type | Emergency | 83.4 (1128) |
| Scheduled | 16.6 (224) | |
| Hospitalization unit | Traumatology | 26.6 (359) |
| Surgery and gynecology | 20.7 (280) | |
| Cardio/gastroenterology | 14.3 (194) | |
| Neuro/pulmonology | 13.1 (177) | |
| General surgery | 2.3 (31) | |
| Otolaryngo/urology | 9 (122) | |
| Internal medicine | 14 (189) | |
| Variables | Barthel Index | Braden Index | Downton Scale | ||||
|---|---|---|---|---|---|---|---|
| m (ds) 1 | p 2 | m (ds) 1 | p 2 | m (ds) 1 | p 2 | ||
| Sex | Male | 81.83 (31.98) | <0.001 * | 19.19 (3.78) | 0.063 | 1.07 (1.21) | <0.001 * |
| Female | 74.62 35.28) | 18.74 (3.95) | 1.25 (1.24) | ||||
| Process type | Medical | 73.5 (36.8) | <0.001 * | 18.34 (4.18) | <0.001 * | 1.3 (1.28) | <0.001 * |
| Surgical | 88.26 (23.76) | 20.25 (2.73) | 0.85 (1.05) | ||||
| Admission type | Scheduled | 94.71 (16.05) | <0.001 * | 21.09 (1.76) | <0.001 * | 0.66 (0.863) | <0.001 * |
| Emergency | 75.14 (35.4) | 18.55 (4.03) | 1.25 (1.27) | ||||
| Hospitalization unit | Traumatology | 74.33 (34.92) | <0.001 ** | 18.57 (4.03) | <0.001 ** | 1.26 (1.15) | <0.001 ** |
| Surgery and gynecology | 82.21 (31.35) | 19.52 (3.63) | 0.99 (1.32) | ||||
| Cardio/gastroenterology | 77.52 (36.13) | 18.32 (3.91) | 1.11 (1.31) | ||||
| Neuro/pulmonology | 68.27 (37.92) | 17.92 (4.03) | 1.68 (1.29) | ||||
| General surgery | 82.74 (26.73) | 19.54 (3.22) | 0.77 (1.17) | ||||
| Otolaryngo/urology | 86.63 (26.72) | 19.94 (3.41) | 1.09 (1.08) | ||||
| Internal medicine | 84.68 (30.30) | 19.82 (3.63) | 0.82 (0.96) | ||||
| Variables | Barthel Index | Braden Index | Downton Scale | |
|---|---|---|---|---|
| Coefficient | β (IC95%) 1 t (p) 2 β SE 3 | −19.839 (−16.326–−11.077) −11.077 (<0.001) 1.791 | 2.042 (1.602–2.482) 9.105 (<0.001) 0.224 | 1.632 (1.487–1.776) 22.18 (<0.001) 0.073 |
| Barthel | β (IC95%) 1 | 4.416 (4.26–4.571) | 0.095 (0.076–0.114) | −0.018 (−0.025–−0.012) |
| Mobility | t (p) 2 | 56.4 (<0.001) | 9.712 (<0.001) | −5.82 (<0.001) |
| (VIF = 3.35) 4 | β SE 3 | 0.08 | 0.009 | 0 |
| Braden | β (IC95%) 1 | 4.484 (3.45–5.516) | 1.149 (1.29–1.548) | −0.215 (−0.257–−0.172) |
| Sensory perception | t (p) 2 | 8.532(<0.001) | 21.57 (<0.001) | −9.965 (<0.001) |
| (VIF = 3.09) 4 | β SE 3 | 0.53 | 0.065 | 0 |
| Braden | β (IC95%) 1 | 6.196 (5.27–7.12) | 1.326 (1.209–1.442) | −0.136 (−0.175–−0.098) |
| Moisture | t (p) 2 | 13.07 (<0.001) | 22.341 (<0.001) | −7.033 (<0.001) |
| (VIF = 2.69) 4 | β SE 3 | 0.47 | 0.059 | 0 |
| Braden | β (IC95%) 1 | 2.804 (1.83–3.778) | 1.847 (1.725–1.696) | 0.003 (−0.036–0.042) |
| Mobility | t (p) 2 | 5.653 (<0.001) | 29.731 (<0.001) | 0.156 (0.876) |
| (VIF = 3.19) 4 | β SE 3 | 0.5 | 0.062 | 0 |
| Downton | β (IC95%) 1 | −0.816 (−2.08–0.448) | 0.019 (−0.138–0.178) | 1.015 (0.958–1.062) |
| Previous fall | t (p) 2 | −1.267 (0.205) | 0.244 (0.807) | 38.136 (<0.001) |
| (VIF = 1.13) 4 | β SE 3 | 0.64 | 0.081 | 0 |
| Downton | β (IC95%) 1 | −0.076 (−1.03–0.872) | −0.131 (−0.25–−0.012) | 1.074 (1.035–1.113) |
| Medication | t (p) 2 | −0.159 (0.874) | −2.174 (0.03) | 54.065 (<0.001) |
| (VIF = 1.12) 4 | β SE 3 | 0.48 | 0.061 | 0 |
| Downton | β (IC95%) 1 | −2.688 (−3.93–−1.447) | 0.082 (−0.073–−0.237) | 1.008 (0.957–1.0598) |
| Sensory deficiency | t (p) 2 | −4.249 (<0.001) | 1.034 (0.302) | 38.8 (<0.001) |
| (VIF = 1.62) 4 | β SE 3 | 0.63 | 0.079 | 0 |
| Summarized model | R2 * R2 adjusted ANOVA (p) | 0.939 0.938 2937 (<0.001) | 0.927 0.926 2424 (<0.001) | 0.922 0.921 2266 (<0.001) |
| Predicted Categories | Original Categories | |||||
|---|---|---|---|---|---|---|
| Total | Severe | Moderate | Slight | Total | ||
| Total | n | 151 (86.3%) * | 12 | 0 | 0 | 163 |
| Severe | n | 21 | 9 (25%) * | 12 | 10 | 52 |
| Moderate | n | 3 | 15 | 23 (42.6%) * | 49 | 90 |
| Slight | n | 0 | 0 | 19 | 1028 (94.6%) * | 1047 |
| Total | n | 175 | 36 | 54 | 1087 | 1352 (89.6%) * |
| Predicted Categories | Original Categories | |||||
|---|---|---|---|---|---|---|
| High | Moderate | Low | No Risk | Total | ||
| High | n | 68 (70.8%) * | 31 | 0 | 9 | 99 |
| Moderate | n | 26 | 64 (58.7%) * | 32 | 0 | 122 |
| Low | n | 2 | 14 | 185 (70.3%) * | 66 | 267 |
| No risk | n | 0 | 0 | 46 | 818 (92.5%) * | 864 |
| Total | n | 96 | 109 | 263 | 884 | 1352 (83.94%) * |
| Predicted Categories | Original Categories | |||
|---|---|---|---|---|
| No Risk | Risk | Total | ||
| No risk | n | 1139 (99.7%) * | 82 | 1221 |
| Risk | n | 3 | 128 (61%) * | 131 |
| Total | n | 1142 | 210 | 1352 (93.71%) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luna-Aleixos, D.; Llagostera-Reverter, I.; Castelló-Benavent, X.; Aquilué-Ballarín, M.; Mecho-Montoliu, G.; Cervera-Gasch, Á.; Valero-Chillerón, M.J.; Mena-Tudela, D.; Andreu-Pejó, L.; Martínez-Gonzálbez, R.; et al. Development and Validation of a Meta-Instrument for Nursing Assessment in Adult Hospitalization Units (VALENF Instrument) (Part I). Int. J. Environ. Res. Public Health 2022, 19, 14622. https://doi.org/10.3390/ijerph192214622
Luna-Aleixos D, Llagostera-Reverter I, Castelló-Benavent X, Aquilué-Ballarín M, Mecho-Montoliu G, Cervera-Gasch Á, Valero-Chillerón MJ, Mena-Tudela D, Andreu-Pejó L, Martínez-Gonzálbez R, et al. Development and Validation of a Meta-Instrument for Nursing Assessment in Adult Hospitalization Units (VALENF Instrument) (Part I). International Journal of Environmental Research and Public Health. 2022; 19(22):14622. https://doi.org/10.3390/ijerph192214622
Chicago/Turabian StyleLuna-Aleixos, David, Irene Llagostera-Reverter, Ximo Castelló-Benavent, Marta Aquilué-Ballarín, Gema Mecho-Montoliu, Águeda Cervera-Gasch, María Jesús Valero-Chillerón, Desirée Mena-Tudela, Laura Andreu-Pejó, Rafael Martínez-Gonzálbez, and et al. 2022. "Development and Validation of a Meta-Instrument for Nursing Assessment in Adult Hospitalization Units (VALENF Instrument) (Part I)" International Journal of Environmental Research and Public Health 19, no. 22: 14622. https://doi.org/10.3390/ijerph192214622