
Predictors of the Quality of Life of University Students: A Cross-Sectional Study
 ,
,  , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
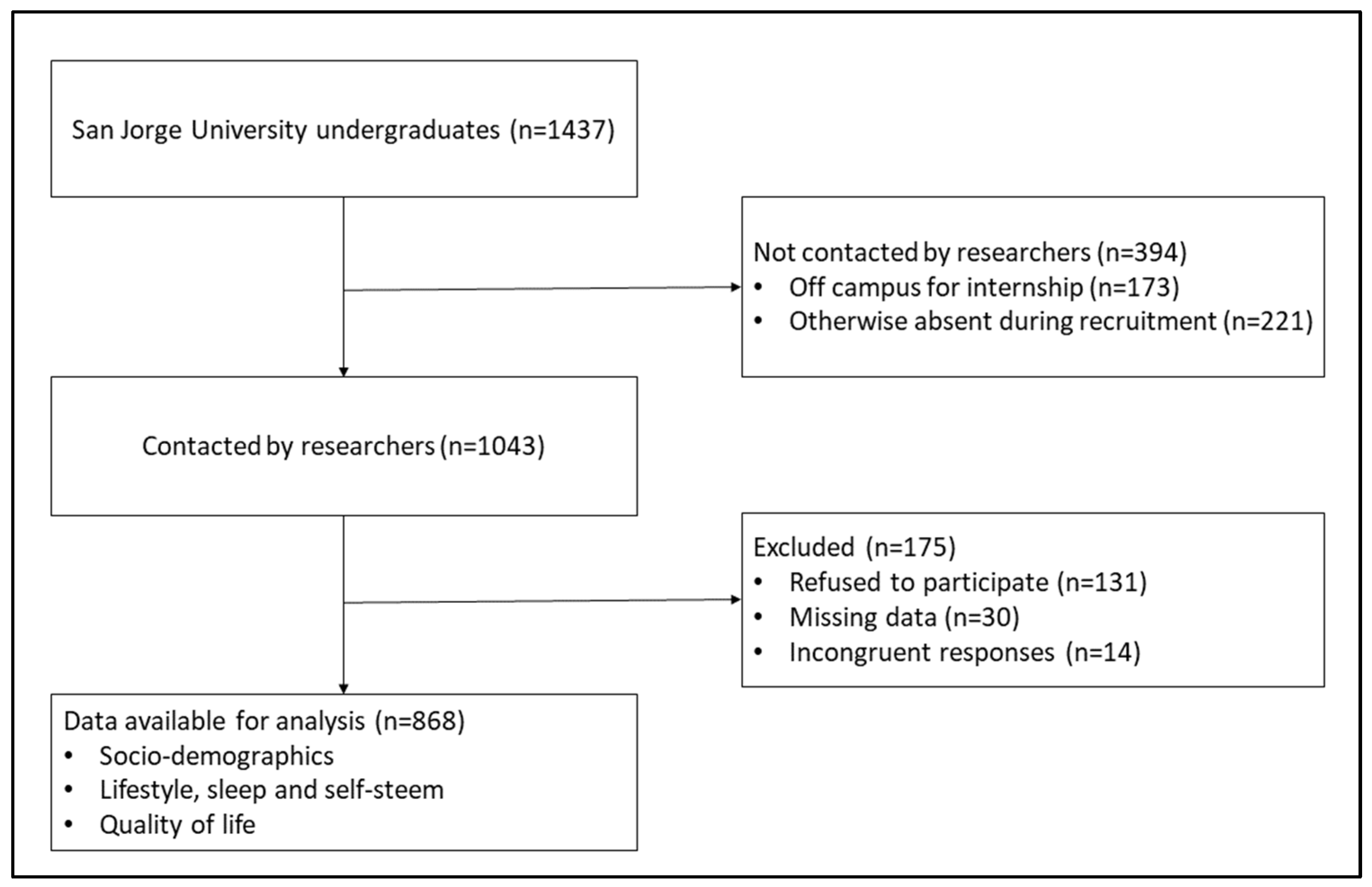
2.1. Procedure and Participants
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Demographic Characteristics
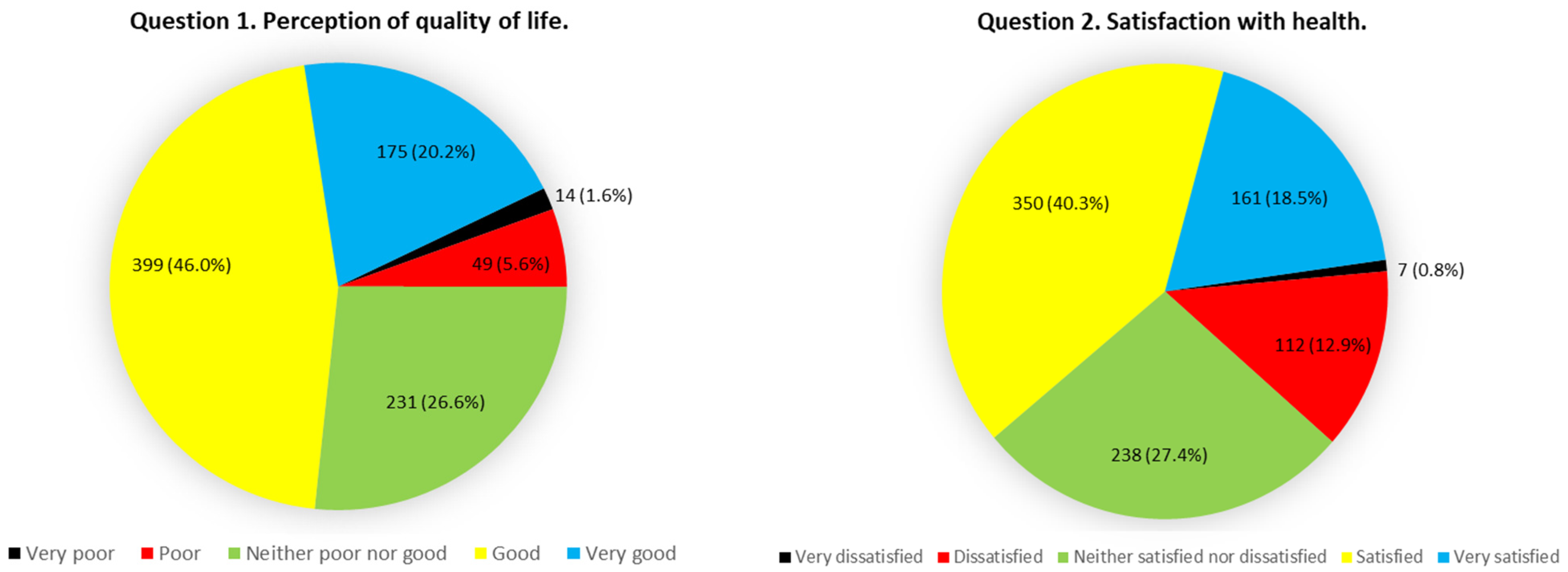
3.2. WHOQOL-BREF scores and their reliability
3.3. The Relationship between Sociodemographic Variables and QOL: Multivariant Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? PharmacoEconomics 2016, 34, 645–649. [Google Scholar] [CrossRef]
- Moons, P.; Budts, W.; De Geest, S. Critique on the conceptualisation of quality of life: A review and evaluation of different conceptual approaches. Int. J. Nurs. Stud. 2006, 43, 891–901. [Google Scholar] [CrossRef] [PubMed]
- The WHOQOL Group. The World Health Organization Quality of Life assessment (WHOQOL):Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Faílde Garrido, J.M.; Ruiz Soriano, L.; Pérez Fernández, M.R.; Lameiras Fernández, M.; Rodríguez Castro, Y. Evolution of quality of life and health-related behaviors among Spanish university students. Int. J. Health Plan. Manag. 2019, 34, e789–e801. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.M.; Squeglia, L.M. Research Review: What have we learned about adolescent substance use? J. Child Psychol. Psychiatry Allied Discip. 2018, 59, 618–627. [Google Scholar] [CrossRef]
- Ramón-Arbués, E.; Abadía, B.M.; López, J.M.G.; Serrano, E.E.; García, B.P.; Vela, R.J.; Portillo, S.G.; Guinoa, M.S. Eating behavior and relationships with stress, anxiety, depression and insomnia in university students. Nutr. Hosp. 2019, 36, 1339–1345. [Google Scholar] [CrossRef]
- Nur, N.; Kıbık, A.; Kılıç, E.; Sümer, H. Health-related Quality of Life and Associated Factors Among Undergraduate University Students. Oman Med. J. 2017, 32, 329–334. [Google Scholar] [CrossRef]
- Ghassab-Abdollahi, N.; Shakouri, S.K.; Aghdam, A.T.; Farshbaf-Khalili, A.; Abdolalipour, S.; Farshbaf-Khalili, A. Association of quality of life with physical activity, depression, and demographic characteristics and its predictors among medical students. J. Educ. Health Promot. 2020, 9, 147. [Google Scholar] [CrossRef]
- Messina, G.; Quercioli, C.; Troiano, G.; Russo, C.; Barbini, E.; Nisticò, F.; Nante, N. Italian medical students quality of life: Years 2005–2015. Ann. Di Ig. Med. Prev. E Di Comunita 2016, 28, 245–251. [Google Scholar] [CrossRef]
- Serinolli, M.I.; Novaretti, M.C.Z. A cross-sectional study of sociodemographic factors and their influence on quality of life in medical students at Sao Paulo, Brazil. PLoS ONE 2017, 12, e0180009. [Google Scholar] [CrossRef] [Green Version]
- Shareef, M.A.; AlAmodi, A.A.; Al-Khateeb, A.A.; Abudan, Z.; Alkhani, M.A.; Zebian, S.I.; Qannita, A.S.; Tabrizi, M.J. The interplay between academic performance and quality of life among preclinical students. BMC Med. Educ. 2015, 15, 193. [Google Scholar] [CrossRef] [PubMed]
- Solis, A.C.; Lotufo-Neto, F. Predictors of quality of life in Brazilian medical students: A systematic review and meta-analysis. Braz. J. Psychiatry 2019, 41, 556–567. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, Y.; Kilic, S.P.; Akyol, A.D. Relationship between life satisfaction and quality of life in Turkish nursing school students. Nurs. Health Sci. 2013, 15, 415–422. [Google Scholar] [CrossRef]
- Al-Shibani, N.; Al-Kattan, R. Evaluation of quality of life among dental students using WHOQOL-BREF questionnaire in Saudi Arabia: A cross sectional study. Pak. J. Med. Sci. 2019, 35, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Pillay, N.; Ramlall, S.; Burns, J.K. Spirituality, depression and quality of life in medical students in KwaZulu-Natal. South Afr. J. Psychiatry SAJP J. Soc. Psychiatr. South Afr. 2019, 22, 731. [Google Scholar] [CrossRef] [PubMed]
- Seo, E.J.; Ahn, J.-A.; Hayman, L.L.; Kim, C.-J. The Association Between Perceived Stress and Quality of Life in University Students: The Parallel Mediating Role of Depressive Symptoms and Health-Promoting Behaviors. Asian Nurs. Res. 2018, 12, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; McEnroe-Petitte, D.M.; Papathanasiou, I.V.; Edet, O.; Tsaras, K.; Christos, K.F.; Fradelos, E.C.; Rosales, R.A.; Cruz, J.; Leocadio, M.; et al. A cross-country comparative study on stress and quality of life in nursing students. Perspect. Psychiatr. Care 2018, 54, 469–476. [Google Scholar] [CrossRef]
- Kwon, S.J.; Kim, Y.; Kwak, Y. Relationship of sleep quality and attention deficit hyperactivity disorder symptoms with quality of life in college students. J. Am. Coll. Health 2020, 68, 536–542. [Google Scholar] [CrossRef]
- Rezaei, O.; Mokhayeri, Y.; Haroni, J.; Rastani, M.J.; Sayadnasiri, M.; Ghisvand, H.; Noroozi, M.; Armoon, B. Association between sleep quality and quality of life among students: A cross sectional study. Int. J. Adolesc. Med. Health 2017, 32. [Google Scholar] [CrossRef]
- Wanden-Berghe, C.; Martín-Rodero, H.; Rodríguez-Martín, A.; Ruiz, J.P.N.; De Victoria, E.M.; Sanz-Valero, J.; García-González, Á.; Vila, A.; Alonso, M.V.; Marí, J.A.T.; et al. Quality of life and its determinants in Spanish university students of health sciences factors. Nutr. Hosp. 2014, 31, 952–958. [Google Scholar] [CrossRef] [Green Version]
- Feasel-Aklilu, S.; Marcus, A.; Parrott, J.S.; Peters, E.; Byham-Gray, L. Is Nutrition Specific Quality of Life Associated With Nutritional Status? J. Ren. Nutr. 2018, 28, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Kanesarajah, J.; Waller, M.; Whitty, J.A.; Mishra, G.D. Physical activity and body mass shape quality of life trajectories in mid-age women. Aust. N. Z. J. Public Health 2018, 42, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, M.; Danovitch, I.; IsHak, W.W. Quality of life and smoking. Am. J. Addict. 2014, 23, 540–562. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.V.F.D.; Campos, M.R.; Fortes, S.L.C.L. Relationship of alcohol consumption and mental disorders common with the quality of life of patients in primary health care. Cienc. Saude Coletiva 2019, 24, 1051–1063. [Google Scholar] [CrossRef]
- Verma, A.K.; Schulte, P.J.; Bittner, V.; Keteyian, S.J.; Fleg, J.L.; Piña, I.L.; Swank, A.M.; Fitz-Gerald, M.; Ellis, S.J.; Kraus, W.E.; et al. Socioeconomic and partner status in chronic heart failure: Relationship to exercise capacity, quality of life, and clinical outcomes. Am. Heart J. 2017, 183, 54–61. [Google Scholar] [CrossRef]
- Almojali, A.I.; Almalki, S.A.; Alothman, A.S.; Masuadi, E.M.; Alaqeel, M.K. The prevalence and association of stress with sleep quality among medical students. J. Epidemiol. Glob. Health 2017, 7, 169–174. [Google Scholar] [CrossRef]
- Pulido-Martos, M.; Augusto-Landa, J.M.; Lopez-Zafra, E. Sources of stress in nursing students: A systematic review of quantitative studies. Int. Nurs. Rev. 2012, 59, 15–25. [Google Scholar] [CrossRef]
- Fernández-Martínez, E.; Onieva-Zafra, M.D.; Parra-Fernández, M.L. The Impact of Dysmenorrhea on Quality of Life Among Spanish Female University Students. Int. J. Environ. Res. Public Health 2019, 16, E713. [Google Scholar] [CrossRef]
- Franquelo-Morales, P.; Sánchez-López, M.; Notario-Pacheco, B.; Miota-Ibarra, J.; Lahoz-García, N.; Gómez-Marcos, M.Á.; Martínez-Vizcaíno, V. Association Between Health-Related Quality of Life, Obesity, Fitness, and Sleep Quality in Young Adults: The Cuenca Adult Study. Behav. Sleep Med. 2018, 16, 347–355. [Google Scholar] [CrossRef]
- Latorre-Román, P.Á.; Gallego-Rodríguez, M.; Mejía-Meza, J.A.; García-Pinillos, F. Alcohol, and tobacco consumption and sports practice in Mexican and Spanish university students and the association between quality of life and health and sensation seeking. Gac. Med. De Mex. 2015, 151, 197–205. [Google Scholar]
- Martín-Espinosa, N.M.; Garrido-Miguel, M.; Martínez-Vizcaíno, V.; González-García, A.; Redondo-Tébar, A.; Cobo-Cuenca, A.I. The Mediating and Moderating Effects of Physical Fitness of the Relationship between Adherence to the Mediterranean Diet and Health-Related Quality of Life in University Students. Nutrients 2020, 12, E3578. [Google Scholar] [CrossRef] [PubMed]
- The International Physical Activity Questionnaire Group. The International Physical Activity Questionnaire Group Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire. Available online: http://www.ipaq.ki.se/scoring.pdf (accessed on 21 June 2022).
- Norte Navarro, A.I.; Ortiz Moncada, R. Spanish diet quality according to the healthy eating index. Nutr. Hosp. 2011, 26, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1995. [Google Scholar] [CrossRef]
- Vázquez-Morejón, A.; Jiménez-García, R.; Vázquez-Morejón, R. Escala de autoestima de Rosenberg. Fiabilidad y validez en población clínica española. Apunt. De Psicol. 2004, 22, 247–255. [Google Scholar]
- Rodríguez Martos, A.; Navarro, R.; Vecino, C.; Pérez, R. Validación de los cuestionarios KFA (CBA) y CAGE para el diagnóstico del alcoholismo. Drog. -Alcohol. 1986, 11, 132–139. [Google Scholar]
- Morales-Rueda, A.; Rubio-Valladolid, G. Diagnóstico y tratamiento de los problemas relacionados con el alcohol en atención primaria. MEDIFAM 1997, 7, 211–225. [Google Scholar]
- Royuela-Rico, A.; Macías-Fernández, J. Propiedades clinimétricas de la versión castellana del cuestionario de Pittsburgh. Vigilia-Sueño 1997, 9, 81–94. [Google Scholar]
- Jiménez-Genchi, A.; Monteverde-Maldonado, E.; Nenclares-Portocarrero, A.; Esquivel-Adame, G.; de la Vega-Pacheco, A. Reliability and factorial analysis of the Spanish version of the Pittsburg Sleep Quality Index among psychiatric patients. Gac. Med. De Mex. 2008, 144, 491–496. [Google Scholar]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A.; WHOQOL Group. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef]
- World Health Organization; Division of Mental Health. WHOQOL-BREF: Introduction, Administration, Scoring and Generic Version of the Assessment: Field trial Version, December 1996. (No. WHOQOL-BREF). World Health Organization. 1996. Available online: https://apps.who.int/iris/handle/10665/63529 (accessed on 14 June 2022).
- Ridner, S.L.; Keith, R.J.; Walker, K.L.; Hart, J.L.; Newton, K.S.; Crawford, T.N. Differences in quality of life among college student electronic cigarette users. AIMS Public Health 2018, 5, 454–462. [Google Scholar] [CrossRef]
- Victor, F.F.; Souza, A.I.; Barreiros, C.D.T.; de Barros, J.L.N.; da Silva, F.A.C.; Ferreira, A.L.C.G. Quality of Life among University Students with Premenstrual Syndrome. Rev. Bras. De Ginecol. E Obstet. Rev. Da Fed. Bras. Das Soc. De Ginecol. E Obstet. 2019, 41, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Pedrero-Pérez, E.J.; Barreda-Marina, M.A.; Bartolomé-Gil, C.; Bosque-Coro, S.; Callejo-Escobar, J.; Ema-López, I.; Dominguez-Aranda, M.A.; Ferrero-Herreros, Y.E.; Galera-García, Ó.; Garrido-Ureña, B.; et al. Quality of life in patients treated with methadone: The WHOQOL-BREF, psychometric study and application results. An. De Psicol. 2018, 34, 251–257. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Encuesta Nacional de Salud de España (ENSE). Portal Estadístico Área de Inteligencia de Gestión. Available online: https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/S/ense (accessed on 16 June 2022).
- Kupcewicz, E.; Grochans, E.; Kadučáková, H.; Mikla, M.; Jóźwik, M. Analysis of the Relationship between Stress Intensity and Coping Strategy and the Quality of Life of Nursing Students in Poland, Spain and Slovakia. Int. J. Environ. Res. Public Health 2020, 17, 4536. [Google Scholar] [CrossRef] [PubMed]
- Ilić, I.; Šipetić, S.; Grujičić, J.; Mačužić, I.Ž.; Kocić, S.; Ilić, M. Psychometric Properties of the World Health Organization’s Quality of Life (WHOQOL-BREF) Questionnaire in Medical Students. Medicina 2019, 55, E772. [Google Scholar] [CrossRef] [PubMed]
- Irribarra, T.L.; Mery, I.P.; Lira, S.M.J.; Campos, D.M.; González, L.F.; Irarrázaval, D.S. Quality of life scores among 411 medical students. Rev. Med. De Chile 2018, 146, 1294–1303. [Google Scholar] [CrossRef] [Green Version]
- Backhaus, I.; D’Egidio, V.; Saulle, R.; Masala, D.; Firenze, A.; De Vito, E.; Mannocci, A.; La Torre, G. Health-related quality of life and its associated factors: Results of a multi-center cross-sectional study among university students. J. Public Health 2020, 42, 285–293. [Google Scholar] [CrossRef]
- Cruz, J.P.; Felicilda-Reynaldo, R.F.D.; Lam, S.C.; Contreras, F.A.M.; Cecily, H.S.J.; Papathanasiou, I.V.; Fouly, H.A.; Kamau, S.M.; Valdez, G.F.D.; Adams, K.A.; et al. Quality of life of nursing students from nine countries: A cross-sectional study. Nurse Educ. Today 2018, 66, 135–142. [Google Scholar] [CrossRef]
- Ramos-Dias, J.C.; Libardi, M.C.; Zillo, C.M.; Igarashi, M.H.; Senger, M.H. Qualidade de vida em cem alunos do curso de Medicina de Sorocaba-PUC/SP. Rev. Bras. De Educ. Médica 2010, 34, 116–123. [Google Scholar] [CrossRef]
- Lins, L.; Carvalho, F.M.; Menezes, M.S.; Porto-Silva, L.; Damasceno, H. Health-related quality of life of medical students in a Brazilian student loan programme. Perspect. Med. Educ. 2016, 5, 197–204. [Google Scholar] [CrossRef]
- Torres, G.C.S.; Paragas, E.D. Social determinants associated with the quality of life of baccalaureate nursing students: A cross-sectional study. Nurs. Forum 2019, 54, 137–143. [Google Scholar] [CrossRef]
- Meira, T.M.; Paiva, S.M.; Antelo, O.M.; Guimarães, L.K.; Bastos, S.Q.; Tanaka, O.M. Perceived stress and quality of life among graduate dental faculty. J. Dent. Educ. 2020, 84, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Moutinho, I.L.D.; Lucchetti, A.L.G.; da Ezequiel, O.S.; Lucchetti, G. Mental health and quality of life of Brazilian medical students: Incidence, prevalence, and associated factors within two years of follow-up. Psychiatry Res. 2019, 274, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Blázquez Abellán, G.; López-Torres Hidalgo, J.D.; Rabanales Sotos, J.; López-Torres López, J.; Val Jiménez, C.L. Healthy eating and self-perception of health. Aten. Primaria 2016, 48, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Govindaraju, T.; Sahle, B.W.; McCaffrey, T.A.; McNeil, J.J.; Owen, A.J. Dietary Patterns and Quality of Life in Older Adults: A Systematic Review. Nutrients 2018, 10, E971. [Google Scholar] [CrossRef] [PubMed]
- Antonopoulou, M.; Mantzorou, M.; Serdari, A.; Bonotis, K.; Vasios, G.; Pavlidou, E.; Trifonos, C.; Vadikolias, K.; Petridis, D.; Giaginis, C. Evaluating Mediterranean diet adherence in university student populations: Does this dietary pattern affect students’ academic performance and mental health? Int. J. Health Plan. Manag. 2020, 35, 5–21. [Google Scholar] [CrossRef]
- Ramón-Arbués, E.; Gea-Caballero, V.; Granada-López, J.M.; Juárez-Vela, R.; Pellicer-García, B.; Antón-Solanas, I. The Prevalence of Depression, Anxiety and Stress and Their Associated Factors in College Students. Int. J. Environ. Res. Public Health 2020, 17, 7001. [Google Scholar] [CrossRef]
- Ge, Y.; Xin, S.; Luan, D.; Zou, Z.; Liu, M.; Bai, X.; Gao, Q. Association of physical activity, sedentary time, and sleep duration on the health-related quality of life of college students in Northeast China. Health Qual. Life Outcomes 2019, 17, 124. [Google Scholar] [CrossRef]
- Tao, K.; Liu, W.; Xiong, S.; Ken, L.; Zeng, N.; Peng, Q.; Yan, X.; Wang, J.; Wu, Y.; Lei, M.; et al. Associations between Self-Determined Motivation, Accelerometer-Determined Physical Activity, and Quality of Life in Chinese College Students. Int. J. Environ. Res. Public Health 2019, 16, E2941. [Google Scholar] [CrossRef]
- Yarmohammadi, S.; Ghaffari, M.; Yarmohammadi, H.; Hosseini Koukamari, P.; Ramezankhani, A. Relationship between Quality of Life and Body Image Perception in Iranian Medical Students: Structural Equation Modeling. Int. J. Prev. Med. 2020, 11, 159. [Google Scholar] [CrossRef]
- Yun, E.K.; Lee, H.; Lee, J.U.; Park, J.H.; Noh, Y.M.; Song, Y.G.; Park, J.H. Longitudinal Effects of Body Mass Index and Self-Esteem on Adjustment From Early to Late Adolescence: A Latent Growth Model. J. Nurs. Res. 2019, 27, 1–7. [Google Scholar] [CrossRef]
- Nguyen, D.T.; Wright, E.P.; Dedding, C.; Pham, T.T.; Bunders, J. Low Self-Esteem and Its Association With Anxiety, Depression, and Suicidal Ideation in Vietnamese Secondary School Students: A Cross-Sectional Study. Front. Psychiatry 2019, 10, 698. [Google Scholar] [CrossRef]
- van Tuijl, L.A.; Bennik, E.C.; Penninx, B.W.J.H.; Spinhoven, P.; de Jong, P.J. Predictive value of implicit and explicit self-esteem for the recurrence of depression and anxiety disorders: A 3-year follow-up study. J. Abnorm. Psychol. 2020, 129, 788–798. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, S.; Aleem, A.; Nadeem, M.A. Health Related Quality of Life (HRQOL) and its correlation with academic performance of medical students. Pak. J. Med. Sci. 2019, 35, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Chattu, V.K.; Sahu, P.K.; Seedial, N.; Seecharan, G.; Seepersad, A.; Seunarine, M.; Sieunarine, S.; Seymour, K.; Simboo, S.; Singh, A. An Exploratory Study of Quality of Life and Its Relationship with Academic Performance among Students in Medical and other Health Professions. Med. Sci. 2020, 8, E23. [Google Scholar] [CrossRef] [PubMed]
- Keating, X.D.; Castelli, D.; Ayers, S.F. Association of weekly strength exercise frequency and academic performance among students at a large university in the United States. J. Strength Cond. Res. 2013, 27, 1988–1993. [Google Scholar] [CrossRef] [Green Version]
- Álvarez-Bueno, C.; Pesce, C.; Cavero-Redondo, I.; Sánchez-López, M.; Garrido-Miguel, M.; Martínez-Vizcaíno, V. Academic Achievement and Physical Activity: A Meta-analysis. Pediatrics 2017, 140, e20171498. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef] [PubMed]
- Hershner, S.D.; Chervin, R.D. Causes and consequences of sleepiness among college students. Nat. Sci. Sleep 2014, 6, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Bíró, É. Determinants of sleep quality in college students: A literature review. Explore 2021, 17, 170–177. [Google Scholar] [CrossRef]
- Alotaibi, A.D.; Alosaimi, F.M.; Alajlan, A.A.; Bin Abdulrahman, K.A. The relationship between sleep quality, stress, and academic performance among medical students. J. Fam. Community Med. 2020, 27, 23–28. [Google Scholar] [CrossRef]
- Bolin, D.J. Sleep Deprivation and Its Contribution to Mood and Performance Deterioration in College Athletes. Curr. Sports Med. Rep. 2019, 18, 305–310. [Google Scholar] [CrossRef]
- Short, M.A.; Booth, S.A.; Omar, O.; Ostlundh, L.; Arora, T. The relationship between sleep duration and mood in adolescents: A systematic review and meta-analysis. Sleep Med. Rev. 2020, 52, 101311. [Google Scholar] [CrossRef] [PubMed]
- Al Shammari, M.A.; Al Amer, N.A.; Al Mulhim, S.N.; Al Mohammedsaleh, H.N.; AlOmar, R.S. The quality of sleep and daytime sleepiness and their association with academic achievement of medical students in the eastern province of Saudi Arabia. J. Fam. Community Med. 2020, 27, 97–102. [Google Scholar] [CrossRef] [PubMed]
- El Hangouche, A.J.; Jniene, A.; Aboudrar, S.; Errguig, L.; Rkain, H.; Cherti, M.; Dakka, T. Relationship between poor quality sleep, excessive daytime sleepiness and low academic performance in medical students. Adv. Med. Educ. Pract. 2018, 9, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Villalbí, J.R.; Bosque-Prous, M. Policies to prevent the harm caused by alcohol: Priorities for Spain. Rev. Esp. De Salud Publica 2020, 94, e202011168. [Google Scholar]
- Villalb, J.R.; Suelves, J.M.; Martínez, C.; Valverde, A.; Cabezas, C.; Fernández, E. Smoking control in Spain: Current situation and priorities. Rev. Esp. De Salud Publica 2019, 93, e201907044. [Google Scholar]
- Strack, J.; Esteves, F. Exams? Why worry? Interpreting anxiety as facilitative and stress appraisals. Anxiety Stress Coping 2015, 28, 205–214. [Google Scholar] [CrossRef]
- Ringeisen, T.; Lichtenfeld, S.; Becker, S.; Minkley, N. Stress experience and performance during an oral exam: The role of self-efficacy, threat appraisals, anxiety, and cortisol. Anxiety Stress Coping 2019, 32, 50–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Physical Health Domain | Psychological Health Domain | Social Relationships Domain | Environmental Health Domain | ||
|---|---|---|---|---|---|
| Number (%) / Average ± SD | Average ± SD / Correlation Coefficient | Average ± SD / Correlation Coefficient | Average ± SD / Correlation Coefficient | Average ± SD / Correlation Coefficient | |
| Age | 22.84 ± 7.51 | −0.112 * | −0.084 ** | −0.014 | −0.138 * |
| Under 21 | 525 (60.5%) | 77.48 ± 13.15 | 67.09 ± 16.18 | 74.29 ± 19.00 | 75.40 ± 13.77 |
| Between 21 and 29 | 231 (26.6%) | 72.82 ± 14.37 | 6315 ± 14.97 | 70.21 ± 18.09 | 70.73 ± 12.54 |
| 30 or older | 112 (12.9%) | 76.25 ± 17.13 * | 66.13 ± 15.03 * | 69.19 ± 25.53 * | 72.44 ± 11.98 * |
| Degree in health sciences | 532 (61.3%) | 75.77 ± 12.90 | 65.83 ± 15.33 | 73.55 ± 19.57 | 73.65 ± 13.66 |
| Other degrees | 336 (38.7%) | 76.57 ± 15.99 | 66.07 ± 16.52 | 70.96 ± 20.16 | 73.97 ± 12.92 |
| First-year students | 456 (52.5%) | 76.071 ± 3.73 | 67.79 ± 13.90 | 74.32 ± 20.36 | 74.85 ± 12.46 |
| Other years | 412 (47.5%) | 76.09 ± 14.67 | 63.85 ± 17.45 * | 70.59 ± 19.06 * | 72.58 ± 14.24 ** |
| Male | 189 (21.8%) | 80.41 ± 13.55 | 71.11 ± 12.77 | 73.41 ± 19.82 | 77.44 ± 13.76 |
| Female | 679 (78.2%) | 74.88 ± 14.12 * | 64.47 ± 16.26 * | 72.31 ± 19.84 | 72.75 ± 13.10 * |
| BMI | 22.20 ± 3.18 | 0.032 | −0.052 | −0.191 * | −0.077 ** |
| Low body weight (<18.5) | 84 (9.7%) | 70.42 ± 17.09 | 65.67 ± 20.59 | 77.58 ± 16.03 | 70.00 ± 14.66 |
| Healthy body weight (18.5–24.9) | 672 (77.4%) | 77.40 ± 13.67 | 67.23 ± 14.95 | 73.00 ± 19.38 | 75.40 ± 12.98 |
| Overweight (25–29.9) | 70 (8.1%) | 73.30 ± 12.13 | 56.90 ± 12.22 | 64.40 ± 18.73 | 66.30 ± 13.16 |
| obese (≥30) | 42 (4.8%) | 71.00 ± 14.81 * | 60.50 ± 17.78 | 68.83 ± 29.56 | 67.83 ± 9.85 * |
| Lives alone | 42 (4.8%) | 84.50 ± 14.19 | 61.67 ± 13.75 | 72.00 ± 27.42 | 76.00 ± 15.19 |
| Lives with flat mates | 224 (25.8%) | 73.16 ± 14.69 | 69.25 ± 15.52 | 73.81 ± 22.19 | 72.19 ± 13.18 |
| Lives with parents/family members | 602 (69.4%) | 76.58 ± 13.70 * | 64.98 ± 15.86 * | 72.12 ± 18.24 | 74.21 ± 13.28 |
| Single | 476 (54.8%) | 75.43 ± 14.38 | 64.15 ± 16.63 | 67.78 ± 19.76 | 72.81 ± 14.40 |
| In a stable relationship | 392 (45.2%) | 76.88 ± 13.89 | 68.07 ± 14.47 * | 78.34 ± 18.34 * | 74.95 ± 11.93 ** |
| Satisfaction with academic performance (min. 1–max. 5) | 3.35 ± 0.86 | 0.140 * | 0.243 * | 0.033 | 0.078 ** |
| Low levels of physical activity | 231 (26.6%) | 74.33 ± 15.94 | 64.70 ± 15.90 | 74.27 ± 21.53 | 73.82 ± 14.58 |
| Moderate levels of physical activity | 371 (42.7%) | 77.81 ± 13.74 | 65.77 ± 15.86 | 72.43 ± 18.72 | 71.62 ± 13.55 |
| High levels of physical activity | 266 (30.6%) | 75.18 ± 12.86 * | 67.18 ± 15.59 | 71.21 ± 19.76 | 76.74 ± 11.38 * |
| Screen time (not work/school related) | 3.40 ± 1.72 | 0.055 | −0.005 | 0.037 | 0.062 |
| Screen time < 3 h per day | 329 (37.9%) | 76.28 ± 15.96 | 65.91 ± 16.66 | 70.34 ± 19.92 | 73.66 ± 12.83 |
| Screen time ≥ 3 h per day | 539 (62.1%) | 75.96 ± 12.97 | 65.92 ± 15.27 | 73.90 ± 19.67 ** | 73.84 ± 13.71 |
| Nonsmoker | 588 (67.7%) | 76.54 ± 14.97 | 66.36 ± 16.85 | 70.05 ± 19.50 | 73.56 ± 13.61 |
| Smoker | 280 (32.3%) | 75.13 ± 12.32 | 65.00 ± 13.30 | 77.80 ± 19.53 * | 74.23 ± 12.89 |
| CAGE score | 0.62 ± 0.91 | −0.042 | −0.098 * | 0.073 ** | −0.024 |
| Responsible alcohol consumption (CAGE < 2) | 742 (85.5%) | 76.41 ± 14.24 | 66.48 ± 16.43 | 71.90 ± 20.46 | 73.96 ± 13.41 |
| Risky alcohol consumption (CAGE ≥ 2) | 126 (14.5%) | 74.17 ± 13.68 | 62.61 ± 10.86 * | 76.39 ± 15.15 * | 72.67 ± 13.18 |
| Rosenberg scale score | 31.48 ± 5.93 | 0.489 * | 0.682 * | 0.494 * | 0.471 * |
| High self-esteem | 560 (64.5%) | 80.84 ± 12.12 | 73.14 ± 10.73 | 77.69 ± 18.43 | 77.63 ± 12.40 |
| Moderate self-esteem | 168 (19.4%) | 68.83 ± 11.31 | 58.21 ± 12.31 | 66.42 ± 17.73 | 67.04 ± 10.78 |
| Low self-esteem | 140 (16.1%) | 65.75 ± 15.70 * | 46.30 ± 15.57 * | 59.35 ± 19.54 * | 66.45 ± 13.78 * |
| Pittsburgh Sleep Quality Index score | 6.39 ± 3.58 | −0.555 * | −0.519 * | −0.310 * | −0.332 * |
| Without sleep problems | 420 (48.4%) | 82.37 ± 11.85 | 73.50 ± 12.25 | 78.40 ± 18.62 | 79.10 ± 13.09 |
| Poor sleep quality | 448 (51.6%) | 70.19 ± 13.64 * | 58.81 ± 15.45 * | 67.06 ± 19.38 * | 68.78 ± 11.61 * |
| SHEI score | 69.88 ± 11.29 | −0.051 | 0.116 * | 0.037 | 0.232 * |
| Unhealthy diet | 49 (5.6%) | 70.43 ± 16.79 | 60.86 ± 17.08 | 63.43 ± 23.13 | 64.29 ± 10.01 |
| Diet needing changes | 665 (76.6%) | 76.98 ± 14.73 | 65.51 ± 16.39 | 73.17 ± 20.11 | 73.36 ± 13.32 |
| Healthy diet | 154 (17.7%) | 74.00 ± 9.50 * | 69.32 ± 11.67 * | 72.77 ± 16.66 * | 78.59 ± 12.65 * |
| Average ± SD | Minimum and Maximum Scores Possible | Minimum and Maximum Scores Obtained | Cronbach’s Alpha | |
|---|---|---|---|---|
| Item 1. Perception of QOL | 3.77 ± 0.88 | 1–5 | 1–5 | ----- |
| Item 2. Overall health | 3.63 ± 0.95 | 1–5 | 1–5 | ----- |
| Physical health domain | 76.08 ± 14.17 | 0–100 | 31–100 | 0.71 |
| Psychological health domain | 65.92 ± 15.79 | 0–100 | 6–94 | 0.79 |
| Social relationship domain | 72.55 ± 19.83 | 0–100 | 19–100 | 0.76 |
| Environmental health domain | 73.77 ± 13.37 | 0–100 | 44–100 | 0.72 |
| Item 1: Perceived QOL | Item 2: Overall Health | Physical Health Domain | Psychological Health Domain | Social Relationships Domain | |
|---|---|---|---|---|---|
| Item 1: Perception of QOL | ----- | 0.539 * | ----- | ----- | ----- |
| Physical health domain | 0.468 * | 0.421 * | ----- | ----- | ----- |
| Psychological health domain | 0.472 * | 0.377 * | 0.553 * | ----- | ----- |
| Social relationships domain | 0.302 * | 0.128 * | 0.312 * | 0.542 * | ----- |
| Environmental health domain | 0.478 * | 0.315 * | 0.502 * | 0.538 * | 0.419 * |
| Physical Health Domain B (95% CI) | Psychological Health Domain B (95% CI) | Social Relationships Domain B (95% CI) | Environmental Health Domain B (95% CI) | |
|---|---|---|---|---|
| Age (years) (log) | ----- | −0.120 (−0.219, −0.020) ** | −0.477 (−0.641, −0.313) * | −0.151 (−0.271, −0.031) ** |
| Year of study (Ref. first year) | ||||
| Other years | ----- | ----- | ----- | −2.049 (−3.918, −0.180) ** |
| Gender (Ref. Male) | ||||
| Female | ----- | −1.493 (−3.227, 0.241) | ----- | ----- |
| BMI (Ref. healthy body weight, 18.5–24.9 kg/m2) | ||||
| Low body weight (<18.5) | −6.051 (−8.810, −3.291) * | 3.044 (0.641, 5.447) ** | 5.792 (2.037, 9.547)* | −2.976 (−5.610, −0.343) ** |
| Overweight (25–29.9) | ----- | −4.049 (−6.704, −1.394) * | ----- | −3.233 (−6.118, −0.348) ** |
| Obese (≥30) | −6.159 (−9.801, −2.517) * | −4.297 (−7.645, −0.950) ** | ----- | −5.227 (−8.868, −1.585) ** |
| Living situation (Ref. lives alone) | ||||
| Lives with flat mates | −8.341 (−12.238, −4.444) * | 9.887 (6.361, 13.414) * | ----- | −2.800 (−4.914, −0.685) * |
| Lives with parents/family | −3.407 (−7.164, 0.350) | 6.808 (3.370, 10.246) * | ----- | ----- |
| Relationship status (Ref. single) | ||||
| In a stable relationship | ----- | ----- | 9.904 (7.678, 12.130) * | 1.869 (0.300, 3.437) ** |
| Satisfaction with academic performance | 1.189 (0.142, 2.236) ** | 2.355 (1.508, 3.202) * | ---- | ----- |
| Physical activity (Ref. moderate physical activity) | ||||
| Low physical activity | ----- | 2.450 (0.715, 4.185) * | 4.586 (2.112, 7.060) * | 4.172 (2.326, 6.019) * |
| High physical activity | −2.057 (−3.830, −0.284) ** | 1.852 (0.160, 3.544) ** | ----- | 4.918 (2.995, 6.841) * |
| Screen time (hours) | 0.579 (0.090, 1.069) ** | ----- | −0.641 (−1.392, 0.110) | 0.706 (0.172, 1.241) ** |
| Smoking (Ref. Nonsmoker) | ||||
| Smoker | ----- | ----- | 5.256 (2.779, 7.733) * | ----- |
| CAGE score (log) | −1.688 (−2.573, −0.802) * | −0.916 (−1.679, −0.153) ** | 1.770 (0.570, 2.970) * | −0.753 (−1.593, 0.086) |
| Rosenberg scale score | 0.846 (0.705, 0.987) * | 1.543 (1.417, 1.668) * | 1.457 (1.261, 1.652) * | 0.773 (0.637, 0.908) * |
| Sleep (Ref. without sleep problems) | ||||
| Poor sleep quality | −7.600 (−9.261, −5.940) * | −8.032 (−9.509, −6.555) * | −6.290 (−8.607, −3.972) * | −6.476 (−8.062, −4.889) * |
| SHEI score | ----- | ----- | 0.115 (0.018, 0.212) ** | 0.105 (0.037, 0.173) * |
| R2 (R2 corrected) | 0.359 (0.351) | 0.601 (0.595) | 0.385 (0.377) | 0.350 (0.339) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramón-Arbués, E.; Echániz-Serrano, E.; Martínez-Abadía, B.; Antón-Solanas, I.; Cobos-Rincón, A.; Santolalla-Arnedo, I.; Juárez-Vela, R.; Adam Jerue, B. Predictors of the Quality of Life of University Students: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 12043. https://doi.org/10.3390/ijerph191912043
Ramón-Arbués E, Echániz-Serrano E, Martínez-Abadía B, Antón-Solanas I, Cobos-Rincón A, Santolalla-Arnedo I, Juárez-Vela R, Adam Jerue B. Predictors of the Quality of Life of University Students: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12043. https://doi.org/10.3390/ijerph191912043
Chicago/Turabian StyleRamón-Arbués, Enrique, Emmanuel Echániz-Serrano, Blanca Martínez-Abadía, Isabel Antón-Solanas, Ana Cobos-Rincón, Iván Santolalla-Arnedo, Raúl Juárez-Vela, and Benjamin Adam Jerue. 2022. "Predictors of the Quality of Life of University Students: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 19: 12043. https://doi.org/10.3390/ijerph191912043