

Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Inflammatory Markers
- -
- MLR = monocytes/lymphocytes
- -
- NLR = neutrophils/lymphocytes
- -
- PLR = platelets/lymphocytes
- -
- SII = (neutrophils * platelets)/lymphocytes
- -
- SIRI = (monocytes * platelets)/lymphocytes
- -
- AISI = (neutrophils * monocytes * platelets)/lymphocytes
2.4. Surgical Technique
2.5. Study Outcomes
2.6. Follow-Up Strategy
2.7. Histopathological and Morphometrical Analysis
2.8. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, Regional, and National Burden of Stroke and Its Risk Factors, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Yi, X.; Zhu, L.; Sui, G.; Li, J.; Luo, H.; Yu, M.; Wang, C.; Chen, X.; Wei, W.; Bao, S. Inflammation and Endothelial Function Relevant Genetic Polymorphisms and Carotid Plaque in Chinese Population. J. Atheroscler. Thromb. 2020, 27, 978–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, M.; Wang, L.; Xia, Y.; Tao, L.; Liu, Y.; Huang, F.; Li, S.; Gong, X.; Liu, X.; Xu, G. High Dietary Inflammatory Index Is Associated with Increased Plaque Vulnerability of Carotid in Patients with Ischemic Stroke. Stroke 2020, 51, 2983–2989. [Google Scholar] [CrossRef]
- Fabiani, I.; Palombo, C.; Caramella, D.; Nilsson, J.; De Caterina, R. Imaging of the Vulnerable Carotid Plaque: Role of Imaging Techniques and a Research Agenda. Neurology 2020, 94, 922–932. [Google Scholar] [CrossRef]
- Willey, J.Z.; Pasterkamp, G. The Role of the Vulnerable Carotid Plaque in Embolic Stroke of Unknown Source. J. Am. Coll. Cardiol. 2022, 79, 2200–2202. [Google Scholar] [CrossRef]
- Whooley, J.L.; David, B.C.; Woo, H.H.; Hoh, B.L.; Raftery, K.B.; Hussain Siddiqui, A.; Westerveld, M.; Amin-Hanjani, S.; Ghogawala, Z. Carotid Revascularization and Its Effect on Cognitive Function: A Prospective Nonrandomized Multicenter Clinical Study. J. Stroke Cerebrovasc. Dis. 2020, 29, 104702. [Google Scholar] [CrossRef] [Green Version]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline from the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef]
- Brott, T.G.; Halperin, J.L.; Abbara, S.; Bacharach, J.M.; Barr, J.D.; Bush, R.L.; Cates, C.U.; Creager, M.A.; Fowler, S.B.; Friday, G.; et al. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients with Extracranial Carotid and Vertebral Artery Disease: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery. J. Am. Coll. Cardiol. 2011, 57, 1002–1044. [Google Scholar] [CrossRef] [Green Version]
- Howell, S.J. Carotid Endarterectomy. Br. J. Anaesth. 2007, 99, 119–131. [Google Scholar] [CrossRef]
- DeGroote, R.D.; Lynch, T.G.; Jamil, Z.; Hobson, R.W. Carotid Restenosis: Long-Term Noninvasive Follow-up after Carotid Endarterectomy. Stroke 1987, 18, 1031–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lattimer, C.R.; Burnand, K.G. Recurrent Carotid Stenosis after Carotid Endarterectomy. Br. J. Surg. 1997, 84, 1206–1219. [Google Scholar] [PubMed]
- Keagy, B.A.; Edrington, R.D.; Poole, M.A.; Johnson, G. Incidence of Recurrent or Residual Stenosis after Carotid Endarterectomy. Am. J. Surg. 1985, 149, 722–725. [Google Scholar] [CrossRef]
- Herder, M.; Johnsen, S.H.; Arntzen, K.A.; Mathiesen, E.B. Risk Factors for Progression of Carotid Intima-Media Thickness and Total Plaque Area: A 13-Year Follow-up Study: The Tromsø Study. Stroke 2012, 43, 1818–1823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunelli, N.; Altamura, C.; Costa, C.M.; Altavilla, R.; Palazzo, P.; Maggio, P.; Marcosano, M.; Vernieri, F. Carotid Artery Plaque Progression: Proposal of a New Predictive Score and Role of Carotid Intima-Media Thickness. Int. J. Environ. Res. Public Health 2022, 19, 758. [Google Scholar] [CrossRef]
- Nguyen, D.T.; Bérczi, Á.; Nyárády, B.B.; Szőnyi, Á.; Philippovich, M.; Dósa, E. Short- and Mid-Term Outcomes of Stenting in Patients with Isolated Distal Internal Carotid Artery Stenosis or Post-Surgical Restenosis. J. Clin. Med. 2022, 11, 5640. [Google Scholar] [CrossRef]
- Arbănași, E.M.; Mureșan, A.V.; Coșarcă, C.M.; Kaller, R.; Bud, T.I.; Hosu, I.; Voidăzan, S.T.; Arbănași, E.M.; Russu, E. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Impact on Predicting Outcomes in Patients with Acute Limb Ischemia. Life 2022, 12, 822. [Google Scholar] [CrossRef]
- Russu, E.; Mureșan, A.V.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Voidăzan, S.; Arbănași, E.M.; Coșarcă, C.M. The Predictive Role of NLR and PLR in Outcome and Patency of Lower Limb Revascularization in Patients with Femoropopliteal Disease. J. Clin. Med. 2022, 11, 2620. [Google Scholar] [CrossRef]
- Taurino, M.; Aloisi, F.; Del Porto, F.; Nespola, M.; Dezi, T.; Pranteda, C.; Rizzo, L.; Sirignano, P. Neutrophil-to-Lymphocyte Ratio Could Predict Outcome in Patients Presenting with Acute Limb Ischemia. J. Clin. Med. 2021, 10, 4343. [Google Scholar] [CrossRef]
- Drugescu, A.; Roca, M.; Zota, I.M.; Costache, A.-D.; Gavril, O.I.; Gavril, R.S.; Vasilcu, T.F.; Mitu, O.; Esanu, I.M.; Roca, I.-C.; et al. Value of the Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio in Predicting CPET Performance in Patients with Stable CAD and Recent Elective PCI. Med. Kaunas Lith. 2022, 58, 814. [Google Scholar] [CrossRef]
- Efros, O.; Beit Halevi, T.; Meisel, E.; Soffer, S.; Barda, N.; Cohen, O.; Kenet, G.; Lubetsky, A. The Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Patients Hospitalized with Acute Pulmonary Embolism. J. Clin. Med. 2021, 10, 4058. [Google Scholar] [CrossRef] [PubMed]
- Strazzulla, A.; Abroug Ben Halima, S.; Chouchane, I.; Rezek, M.; Pinto Stiebler, M.; Hamrouni, S.; Maalaoui, M.; Ghriss, N.; Guedec-Ghelfi, R.; Moini, C.; et al. The Predictive Value of Cell Blood Count Parameters to Diagnose Pulmonary Embolism in Patients with SARS-CoV-2 Infection: A Case Control Study. Antibiotics 2022, 11, 60. [Google Scholar] [CrossRef] [PubMed]
- Arbănași, E.M.; Mureșan, A.V.; Arbănași, E.M.; Kaller, R.; Cojocaru, I.I.; Coșarcă, C.M.; Russu, E. The Neutrophil-to-Lymphocyte Ratio’s Predictive Utility in Acute Pulmonary Embolism: Systematic Review. J. Cardiovasc. Emergencies 2022, 8, 25–30. [Google Scholar] [CrossRef]
- Tomioka-Inagawa, R.; Nakane, K.; Enomoto, T.; Tomioka, M.; Taniguchi, T.; Ishida, T.; Ozawa, K.; Takagi, K.; Ito, H.; Takeuchi, S.; et al. The Impact of Neutrophil-to-Lymphocyte Ratio after Two Courses of Pembrolizumab for Oncological Outcomes in Patients with Metastatic Urothelial Carcinoma. Biomedicines 2022, 10, 1609. [Google Scholar] [CrossRef] [PubMed]
- Ginesu, G.C.; Paliogiannis, P.; Feo, C.F.; Cossu, M.L.; Scanu, A.M.; Fancellu, A.; Fois, A.G.; Zinellu, A.; Perra, T.; Veneroni, S.; et al. Inflammatory Indexes as Predictive Biomarkers of Postoperative Complications in Oncological Thoracic Surgery. Curr. Oncol. 2022, 29, 3425–3432. [Google Scholar] [CrossRef]
- Iinuma, K.; Enomoto, T.; Kawada, K.; Fujimoto, S.; Ishida, T.; Takagi, K.; Nagai, S.; Ito, H.; Kawase, M.; Nakai, C.; et al. Utility of Neutrophil-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, and Systemic Immune Inflammation Index as Prognostic, Predictive Biomarkers in Patients with Metastatic Renal Cell Carcinoma Treated with Nivolumab and Ipilimumab. J. Clin. Med. 2021, 10, 5325. [Google Scholar] [CrossRef]
- Gawiński, C.; Michalski, W.; Mróz, A.; Wyrwicz, L. Correlation between Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Tumor-Infiltrating Lymphocytes (TILs) in Left-Sided Colorectal Cancer Patients. Biology 2022, 11, 385. [Google Scholar] [CrossRef]
- Pasqui, E.; de Donato, G.; Lazzeri, E.; Molino, C.; Galzerano, G.; Giubbolini, M.; Palasciano, G. High Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios Are Associated with a Higher Risk of Hemodialysis Vascular Access Failure. Biomedicines 2022, 10, 2218. [Google Scholar] [CrossRef]
- Kaller, R.; Arbănași, E.M.; Mureșan, A.V.; Voidăzan, S.; Arbănași, E.M.; Horváth, E.; Suciu, B.A.; Hosu, I.; Halmaciu, I.; Brinzaniuc, K.; et al. The Predictive Value of Systemic Inflammatory Markers, the Prognostic Nutritional Index, and Measured Vessels’ Diameters in Arteriovenous Fistula Maturation Failure. Life 2022, 12, 1447. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Russu, E.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Arbănași, E.M.; Voidăzan, S.T. The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients. Biomedicines 2022, 10, 1272. [Google Scholar] [CrossRef]
- Halmaciu, I.; Arbănași, E.M.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Bacalbasa, N.; Suciu, B.A.; Cojocaru, I.I.; Runcan, A.I.; Grosu, F.; et al. Chest CT Severity Score and Systemic Inflammatory Biomarkers as Predictors of the Need for Invasive Mechanical Ventilation and of COVID-19 Patients’ Mortality. Diagnostics 2022, 12, 2089. [Google Scholar] [CrossRef] [PubMed]
- Arbănași, E.M.; Halmaciu, I.; Kaller, R.; Mureșan, A.V.; Arbănași, E.M.; Suciu, B.A.; Coșarcă, C.M.; Cojocaru, I.I.; Melinte, R.M.; Russu, E. Systemic Inflammatory Biomarkers and Chest CT Findings as Predictors of Acute Limb Ischemia Risk, Intensive Care Unit Admission, and Mortality in COVID-19 Patients. Diagnostics 2022, 12, 2379. [Google Scholar] [CrossRef] [PubMed]
- Parthasarathi, A.; Padukudru, S.; Arunachal, S.; Basavaraj, C.K.; Krishna, M.T.; Ganguly, K.; Upadhyay, S.; Anand, M.P. The Role of Neutrophil-to-Lymphocyte Ratio in Risk Stratification and Prognostication of COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1233. [Google Scholar] [CrossRef] [PubMed]
- Citu, C.; Gorun, O.M.; Motoc, A.; Citu, I.M.; Gorun, F.; Malita, D. Correlation of Lung Damage on CT Scan with Laboratory Inflammatory Markers in COVID-19 Patients: A Single-Center Study from Romania. J. Clin. Med. 2022, 11, 4299. [Google Scholar] [CrossRef]
- Cocoş, R.; Mahler, B.; Turcu-Stiolica, A.; Stoichiță, A.; Ghinet, A.; Shelby, E.-S.; Bohîlțea, L.C. Risk of Death in Comorbidity Subgroups of Hospitalized COVID-19 Patients Inferred by Routine Laboratory Markers of Systemic Inflammation on Admission: A Retrospective Study. Viruses 2022, 14, 1201. [Google Scholar] [CrossRef]
- Regolo, M.; Vaccaro, M.; Sorce, A.; Stancanelli, B.; Colaci, M.; Natoli, G.; Russo, M.; Alessandria, I.; Motta, M.; Santangelo, N.; et al. Neutrophil-to-Lymphocyte Ratio (NLR) Is a Promising Predictor of Mortality and Admission to Intensive Care Unit of COVID-19 Patients. J. Clin. Med. 2022, 11, 2235. [Google Scholar] [CrossRef]
- Kudlinski, B.; Zgoła, D.; Stolińska, M.; Murkos, M.; Kania, J.; Nowak, P.; Noga, A.; Wojciech, M.; Zaborniak, G.; Zembron-Lacny, A. Systemic Inflammatory Predictors of In-Hospital Mortality in COVID-19 Patients: A Retrospective Study. Diagnostics 2022, 12, 859. [Google Scholar] [CrossRef]
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; Farb, A.; Schwartz, S.M. Lessons from Sudden Coronary Death: A Comprehensive Morphological Classification Scheme for Atherosclerotic Lesions. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1262–1275. [Google Scholar] [CrossRef] [Green Version]
- Libby, P.; Ridker, P.M.; Maseri, A. Inflammation and Atherosclerosis. Circulation 2002, 105, 1135–1143. [Google Scholar] [CrossRef]
- Santo Signorelli, S.; Anzaldi, M.; Fiore, V.; Catanzaro, S.; Simili, M.; Torrisi, B.; Neri, S. Study on Unrecognized Peripheral Arterial Disease (PAD) by Ankle/Brachial Index and Arterial Comorbidity in Catania, Sicily, Italy. Angiology 2010, 61, 524–529. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An Inflammatory Disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.H.; Croal, B.L.; Cuthbertson, B.H.; Small, G.R.; Ifezulike, A.I.; Gibson, G.; Jeffrey, R.R.; Buchan, K.G.; El-Shafei, H.; Hillis, G.S. Preoperative Neutrophil-Lymphocyte Ratio and Outcome from Coronary Artery Bypass Grafting. Am. Heart J. 2007, 154, 995–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamhane, U.U.; Aneja, S.; Montgomery, D.; Rogers, E.-K.; Eagle, K.A.; Gurm, H.S. Association between Admission Neutrophil to Lymphocyte Ratio and Outcomes in Patients with Acute Coronary Syndrome. Am. J. Cardiol. 2008, 102, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Duffy, B.K.; Gurm, H.S.; Rajagopal, V.; Gupta, R.; Ellis, S.G.; Bhatt, D.L. Usefulness of an Elevated Neutrophil to Lymphocyte Ratio in Predicting Long-Term Mortality after Percutaneous Coronary Intervention. Am. J. Cardiol. 2006, 97, 993–996. [Google Scholar] [CrossRef]
- Sadeghi, F.; Sarkady, F.; Zsóri, K.S.; Szegedi, I.; Orbán-Kálmándi, R.; Székely, E.G.; Vasas, N.; Berényi, E.; Csiba, L.; Bagoly, Z.; et al. High Neutrophil–Lymphocyte Ratio and Low Lymphocyte–Monocyte Ratio Combination after Thrombolysis Is a Potential Predictor of Poor Functional Outcome of Acute Ischemic Stroke. J. Pers. Med. 2022, 12, 1221. [Google Scholar] [CrossRef]
- Lee, S.-H.; Jang, M.U.; Kim, Y.; Park, S.Y.; Kim, C.; Kim, Y.J.; Sohn, J.-H. The Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios Predict Reperfusion and Prognosis after Endovascular Treatment of Acute Ischemic Stroke. J. Pers. Med. 2021, 11, 696. [Google Scholar] [CrossRef]
- Lattanzi, S.; Norata, D.; Broggi, S.; Meletti, S.; Świtońska, M.; Słomka, A.; Silvestrini, M. Neutrophil-to-Lymphocyte Ratio Predicts Early Neurological Deterioration after Endovascular Treatment in Patients with Ischemic Stroke. Life 2022, 12, 1415. [Google Scholar] [CrossRef]
- Świtońska, M.; Piekuś-Słomka, N.; Słomka, A.; Sokal, P.; Żekanowska, E.; Lattanzi, S. Neutrophil-to-Lymphocyte Ratio and Symptomatic Hemorrhagic Transformation in Ischemic Stroke Patients Undergoing Revascularization. Brain Sci. 2020, 10, E771. [Google Scholar] [CrossRef]
- Kotfis, K.; Bott-Olejnik, M.; Szylińska, A.; Rotter, I. Could Neutrophil-to-Lymphocyte Ratio (NLR) Serve as a Potential Marker for Delirium Prediction in Patients with Acute Ischemic Stroke? A Prospective Observational Study. J. Clin. Med. 2019, 8, 1075. [Google Scholar] [CrossRef] [Green Version]
- Dai, Z.; Li, R.; Zhao, N.; Han, Y.; Wang, M.; Zhang, S.; Bai, Y.; Li, Z.; Liang, M.; Xiao, L.; et al. Neutrophil to Lymphocyte Ratio as a Predictor of Restenosis after Angioplasty and Stenting for Asymptomatic Carotid Stenosis. Angiology 2019, 70, 160–165. [Google Scholar] [CrossRef]
- Halazun, H.J.; Mergeche, J.L.; Mallon, K.A.; Connolly, E.S.; Heyer, E.J. Neutrophil-Lymphocyte Ratio as a Predictor of Cognitive Dysfunction in Carotid Endarterectomy Patients. J. Vasc. Surg. 2014, 59, 768–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.H.; Kim, A.H.; Kwan, S.; Lee, J.; Schmaier, A.H.; Kumins, N.H.; Harth, K.C.; Wong, V.L.; Colvard, B.D.; Kashyap, V.S.; et al. Elevated Neutrophil to Lymphocyte Ratio Is Associated with Worse Outcomes after Carotid Endarterectomy in Asymptomatic Patients. J. Stroke Cerebrovasc. Dis. 2021, 30, 106120. [Google Scholar] [CrossRef] [PubMed]
- Deşer, S.B.; Yucel, S.M.; Demirag, M.K.; Guclu, M.M.; Kolbakir, F.; Keceligil, H.T. The Association between Platelet/Lymphocyte Ratio, Neutrophil/Lymphocyte Ratio, and Carotid Artery Stenosis and Stroke Following Carotid Endarterectomy. Vascular 2019, 27, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Casanova, N.; Diaz-Duran, C.; Nieto, L.; Llort, C.; Elosua, R.; Clara, A. Predictive Value of Complete Blood Count-Derived Inflammatory Markers for 5-Year Survival After Carotid Endarterectomy: Implications for Practice. Angiology 2022, 73, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Bao, X.; Zhou, G.; Xu, W.; Liu, X.; Ye, Z.; Jiang, F. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: Novel Markers for the Diagnosis and Prognosis in Patients with Restenosis Following CAS. Biomark. Med. 2020, 14, 271–282. [Google Scholar] [CrossRef]
- Fluri, F.; Hatz, F.; Voss, B.; Lyrer, P.A.; Engelter, S.T. Restenosis after Carotid Endarterectomy: Significance of Newly Acquired Risk Factors. Eur. J. Neurol. 2010, 17, 493–498. [Google Scholar] [CrossRef]
- Texakalidis, P.; Tzoumas, A.; Giannopoulos, S.; Jonnalagadda, A.K.; Jabbour, P.; Rangel-Castilla, L.; Machinis, T.; Rivet, D.J.; Reavey-Cantwell, J. Risk Factors for Restenosis After Carotid Revascularization: A Meta-Analysis of Hazard Ratios. World Neurosurg. 2019, 125, 414–424. [Google Scholar] [CrossRef]
- Zhou, F.; Hua, Y.; Ji, X.; Jia, L. A Systemic Review into Carotid Plaque Features as Predictors of Restenosis after Carotid Endarterectomy. J. Vasc. Surg. 2021, 73, 2179–2188.e4. [Google Scholar] [CrossRef]
- Hellings, W.E.; Moll, F.L.; De Vries, J.-P.P.M.; Ackerstaff, R.G.A.; Seldenrijk, K.A.; Met, R.; Velema, E.; Derksen, W.J.M.; De Kleijn, D.P.V.; Pasterkamp, G. Atherosclerotic Plaque Composition and Occurrence of Restenosis After Carotid Endarterectomy. JAMA 2008, 299, 547–554. [Google Scholar] [CrossRef] [Green Version]
- Lattanzi, S.; Norata, D.; Divani, A.A.; Di Napoli, M.; Broggi, S.; Rocchi, C.; Ortega-Gutierrez, S.; Mansueto, G.; Silvestrini, M. Systemic Inflammatory Response Index and Futile Recanalization in Patients with Ischemic Stroke Undergoing Endovascular Treatment. Brain Sci. 2021, 11, 1164. [Google Scholar] [CrossRef]
- Scicchitano, P.; Marzullo, A.; Santoro, A.; Zito, A.; Cortese, F.; Galeandro, C.; Ciccone, A.S.; Angiletta, D.; Manca, F.; Pulli, R.; et al. The Prognostic Role of ST2L and SST2 in Patients Who Underwent Carotid Plaque Endarterectomy: A Five-Year Follow-Up Study. J. Clin. Med. 2022, 11, 3142. [Google Scholar] [CrossRef] [PubMed]
- Marzullo, A.; Ambrosi, F.; Inchingolo, M.; Manca, F.; Devito, F.; Angiletta, D.; Zito, A.; Scicchitano, P.; Ciccone, M.M. ST2L Transmembrane Receptor Expression: An Immunochemical Study on Endarterectomy Samples. PLoS ONE 2016, 11, e0156315. [Google Scholar] [CrossRef] [PubMed]
- Scicchitano, P.; Cameli, M.; Maiello, M.; Modesti, P.A.; Muiesan, M.L.; Novo, S.; Palmiero, P.; Saba, P.S.; Pedrinelli, R.; Ciccone, M.M. Nutraceuticals and Dyslipidaemia: Beyond the Common Therapeutics. J. Funct. Foods 2014, 6, 11–32. [Google Scholar] [CrossRef]
- Ciccone, M.M.; Cortese, F.; Gesualdo, M.; Carbonara, S.; Zito, A.; Ricci, G.; De Pascalis, F.; Scicchitano, P.; Riccioni, G. Dietary Intake of Carotenoids and Their Antioxidant and Anti-Inflammatory Effects in Cardiovascular Care. Mediat. Inflamm. 2013, 2013, 782137. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | All Patients n = 369 | No Stenosis n = 294 | Restenosis n = 75 | p-Value (OR; CI 95%) |
|---|---|---|---|---|
| Age mean ± SD (min–max) | 71.33 ± 11.61 (39–94) | 69.91 ± 11.35 (39–91) | 76.90 ± 10.97 (44–94) | <0.0001 |
| Male/Female sex no. (%) | 190 (51.49%) 179 (48.51%) | 157 (53.30%) 137 (46.60%) | 33 (44.00%) 42 (56.00%) | 0.14 (1.45; 0.87–2.42) |
| Comorbidities and Risk factors | ||||
| AH, no. (%) | 240 (65.04%) | 181 (61.56%) | 59 (78.67%) | 0.006 (2.30; 1.26–4.19) |
| IHD, no. (%) | 146 (39.57%) | 104 (35.37%) | 42 (56.00%) | 0.001 (2.32; 1.38–3.89) |
| AF, no. (%) | 105 (28.46%) | 68 (23.13%) | 37 (49.33%) | <0.0001 (3.23; 1.90–5.48) |
| CHF, no. (%) | 84 (22.76%) | 66 (22.45%) | 18 (24.00%) | 0.77 (1.09; 0.60–1.98) |
| MI, no. (%) | 88 (23.85%) | 56 (19.05%) | 32 (42.67%) | <0.0001 (3.16; 1.83–5.44) |
| DM, no. (%) | 108 (29.27%) | 82 (27.89%) | 26 (34.67%) | 0.25 (1.37; 0.79–2.35) |
| CKD, no. (%) | 69 (18.70%) | 54 (18.37%) | 15 (20.00%) | 0.74 (1.11; 0.58–2.10) |
| PAD, no. (%) | 86 (23.31%) | 67 (22.79%) | 19 (25.33%) | 0.64 (1.14; 0.63–2.06) |
| Tobacco, no. (%) | 80 (21.68%) | 53 (18.03%) | 27 (36.00%) | 0.001 (2.55; 1.46–4.46) |
| Obesity, no. (%) | 94 (25.47%) | 67 (22.79%) | 27 (36.00%) | 0.02 (1.90; 1.10–3.28) |
| Dyslipidemia, no. (%) | 114 (30.89%) | 68 (23.13%) | 46 (61.33%) | <0.0001 (5.27; 3.07–9.02) |
| Ipsilateral ICA Stenosis | ||||
| 70–90%, no. (%) | 268 (72.62%) | 242 (82.31%) | 26 (34.67%) | <0.0001 (8.77; 4.99–15.38) |
| 90–99%, no. (%) | 101 (27.37%) | 52 (17.68%) | 49 (65.33%) | |
| Contralateral ICA Stenosis | ||||
| <50%, no. (%) | 218 (59.07%) | 176 (59.86%) | 42 (56%) | 0.54 (0.85; 0.51–1.42) |
| 50–70%, no. (%) | 89 (24.11%) | 69 (23.46%) | 20 (26.67%) | 0.56 (1.18; 0.66–2.11) |
| >70%, no. (%) | 62 (16.80%) | 49 (16.67%) | 13 (17.33%) | 0.89 (1.04; 0.53–2.05) |
| Histological Type of Carotid Plaque | ||||
| Stable Plaques, no. (%) | 213 (57.72%) | 169 (57.48%) | 44 (58.66%) | 0.85 (1.04; 0.62–1.75) |
| Fibroatheroma, no. (%) | 88 (23.85%) | 65 (22.10%) | 23 (30.67%) | 0.12 (1.55; 0.88–2.73) |
| Fibrocalcific, no. (%) | 125 (33.88%) | 104 (35.37%) | 21 (28%) | 0.22 (0.71; 0.40–1.24) |
| Unstable Plaques, no. (%) | 156 (42.28%) | 109 (37.07%) | 47 (62.67%) | 0.0001 (2.84; 1.68–4.81) |
| Thrombotic Plaque, no. (%) | 73 (19.78%) | 47 (15.98%) | 26 (34.67%) | 0.0004 (2.78; 1.57–4.92) |
| With A Thrombus in Organization, no. (%) | 41 (11.11%) | 30 (10.20%) | 11 (14.67%) | 0.27 (1.51; 0.71–3.17) |
| Thin-Cap Fibro-Atheroma, no. (%) | 26 (7.05%) | 20 (6.80%) | 6 (8%) | 0.71 (1.19; 0.46–3.07) |
| Calcified Nodule, no. (%) | 16 (4.34%) | 12 (4.08%) | 4 (5.33%) | 0.63 (1.32; 0.41–4.22) |
| Pre-Operative Drug Therapy | ||||
| Anticoagulant, no. (%) | 95 (25.75%) | 78 (26.53%) | 17 (22.67%) | 0.49 (0.81; 0.44–1.47) |
| Antiplatelet, no. (%) | 178 (48.24%) | 153 (52.04%) | 25 (33.33%) | 0.004 (0.46; 0.27–0.78) |
| Statins, no. (%) | 222 (60.16%) | 184 (62.59%) | 38 (50.67%) | 0.06 (0.61; 0.36–1.02) |
| Ezetimibe, no. (%) | 77 (20.86%) | 68 (23.12%) | 9 (12%) | 0.03 (0.45; 0.21–0.95) |
| PCSK9I, no. (%) | 21 (5.69%) | 18 (6.12%) | 3 (4%) | 0.48 (0.63; 0.18–2.22) |
| Laboratory data | ||||
| Hemoglobin g/dL median (Q1–Q3) | 13.7 (12.5–14.86) | 13.81 (12.75–14.99) | 13.2 (10.96–14.4) | 0.0004 |
| Hematocrit % median (Q1–Q3) | 41.9 (38.2–45) | 42.0 (39.02–45.01) | 41.23 (34.27–44.5) | 0.003 |
| Glucose mg/dL median (Q1–Q3) | 115 (95–145.8) | 110 (94–133.7) | 146 (120.75–173.75) | <0.0001 |
| Cholesterol mg/dL median (Q1–Q3) | 178.2 (146.4–215.2) | 177.75 (148.02–214.07) | 180.1 (146–239.25) | 0.09 |
| Triglyceride mg/dL median (Q1–Q3) | 119.1 (90.7–165.3) | 117.35 (93.55–163.67) | 123.1 (81.4–170.15) | 0.22 |
| GFR (mL/min/1.73 m2) median (Q1–Q3) | 76.06 (57.47–92.24) | 77.93 (63.28–93.46) | 62.44 (37.42–86.08) | <0.0001 |
| BUN mg/dL median (Q1–Q3) | 41.1 (31.2–54.8) | 39.15 (30.05–50.6) | 51.2 (37.75–97.2) | <0.0001 |
| Creatinine mg/dL median (Q1–Q3) | 0.90 (0.76–1.12) | 0.89 (0.75–1.08) | 1.10 (0.78–1.52) | 0.0003 |
| Neutrophils ×10³/µL median (Q1–Q3) | 4.78 (3.47–7.12) | 4.33 (3.33–6.04) | 7.79 (5.43–9.85) | <0.0001 |
| Lymphocytes ×10³/µL median (Q1–Q3) | 2.10 (1.48–2.87) | 2.35 (1.70–3.19) | 1.36 (0.79–1.72) | <0.0001 |
| Monocyte ×10³/µL median (Q1–Q3) | 0.53 (0.4–0.72) | 0.51 (0.4–0.68) | 0.60 (0.4–0.92) | 0.003 |
| PLT ×10³/µL median (Q1–Q3) | 234 (189.4–280) | 234 (188.62–277.57) | 240.9 (199–323.85) | 0.03 |
| MLR, median (Q1–Q3) | 0.24 (0.16–0.41) | 0.22 (0.15–0.31) | 0.50 (0.32–0.73) | <0.0001 |
| NLR, median (Q1–Q3) | 2.37 (1.25–4.68) | 1.82 (1.15–3.19) | 6.38 (4.39–9.06) | <0.0001 |
| PLR, median (Q1–Q3) | 106.49 (79.95–160.84) | 97.01 (74.88–134.3) | 206.77 (128.17–307.96) | <0.0001 |
| SII, median (Q1–Q3) | 528.57 (302.95–1089.97) | 433.84 (265.83–744.45) | 1635.22 (1039.23–2795.66) | <0.0001 |
| SIRI, median (Q1–Q3) | 1.06 (0.62–2.80) | 0.92 (0.56–1.74) | 4.31 (2.69–5.66) | <0.0001 |
| AISI, median (Q1–Q3) | 265.39 (136.85–666.86) | 209.2 (125.01–419.96) | 1095.2 (593.47–1721.68) | <0.0001 |
| Outcomes | ||||
| Mortality, no. (%) | 38 (10.30%) | 18 (6.12%) | 20 (26.67%) | <0.0001 (5.57; 2.77–11.22) |
| Length of hospital stay, mean ± SD | 3.93 ± 0.85 | 3.93 ± 0.79 | 4.07 ± 1.06 | 0.054 |
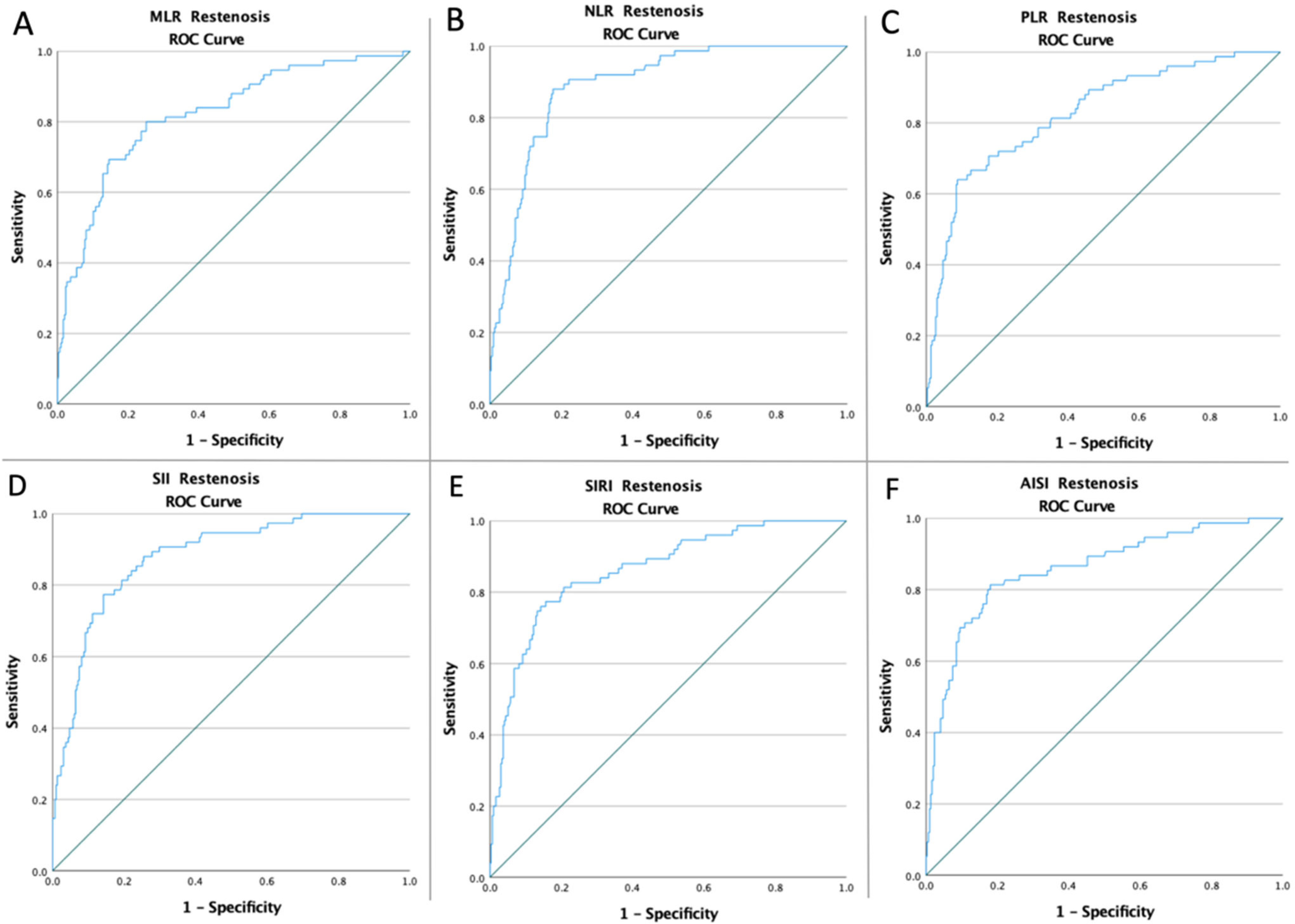
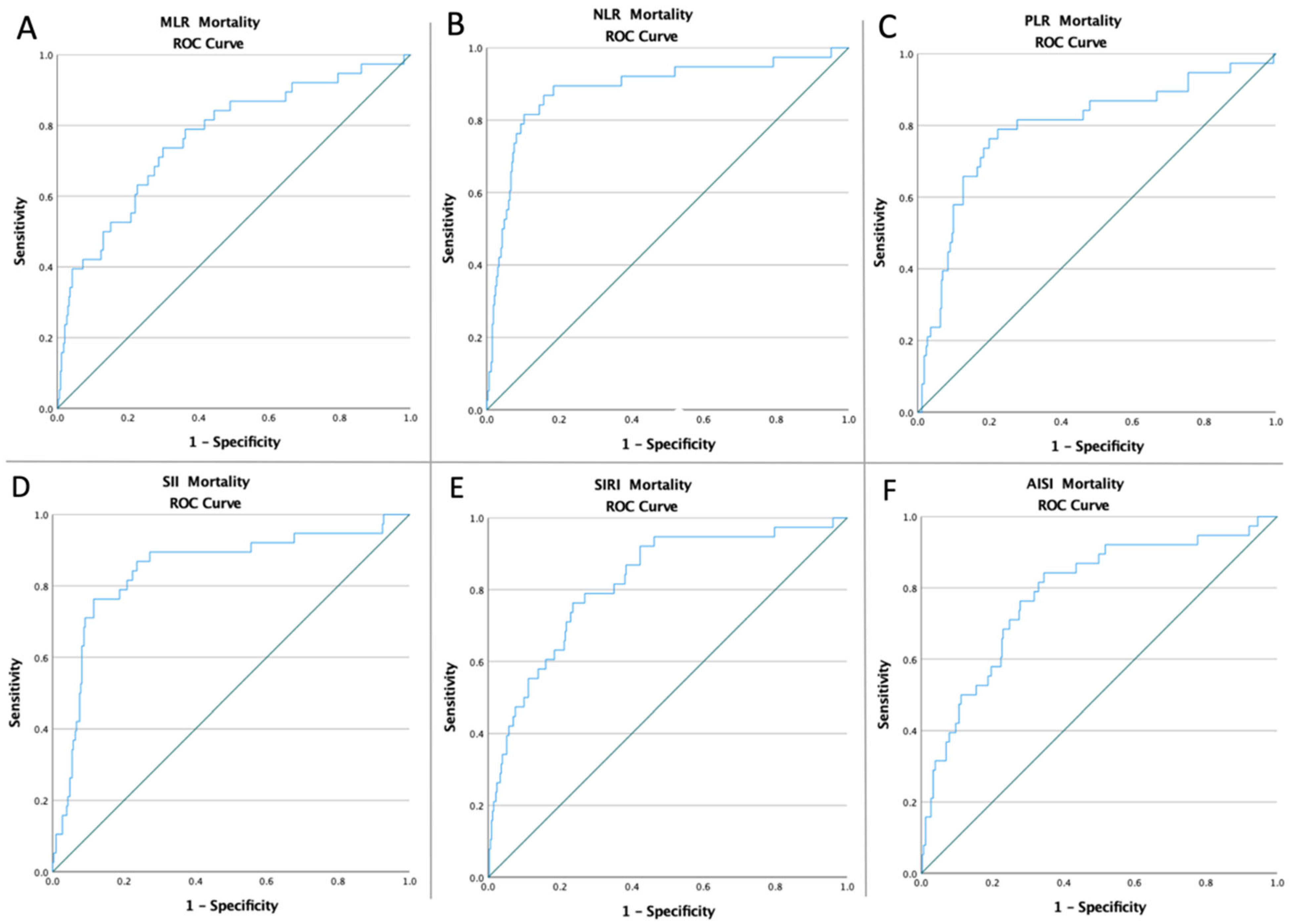
| Variables | Cut-Off | AUC | Std. Error | 95% CI | Sensitivity | Specificity | p-Value |
|---|---|---|---|---|---|---|---|
| Restenosis | |||||||
| MLR | 0.30 | 0.822 | 0.028 | 0.767–0.878 | 80% | 74.8% | <0.0001 |
| NLR | 3.47 | 0.890 | 0.019 | 0.854–0.927 | 90.7% | 77.9% | <0.0001 |
| PLR | 143.05 | 0.825 | 0.028 | 0.771–0.879 | 72% | 79.6% | <0.0001 |
| SII | 881.55 | 0.880 | 0.021 | 0.839–0.921 | 81.3% | 80.6% | <0.0001 |
| SIRI | 2.01 | 0.861 | 0.024 | 0.814–0.908 | 81.3% | 79.3% | <0.0001 |
| AISI | 465.42 | 0.857 | 0.026 | 0.806–0.908 | 82.7% | 77.9% | <0.0001 |
| Mortality | |||||||
| MLR | 0.31 | 0.765 | 0.044 | 0.679–0.850 | 73.7% | 70.1% | <0.0001 |
| NLR | 4.41 | 0.885 | 0.034 | 0.818–0.953 | 89.5% | 81.6% | <0.0001 |
| PLR | 155.07 | 0.794 | 0.044 | 0.708–0.880 | 78.9% | 77.6% | <0.0001 |
| SII | 921.47 | 0.844 | 0.038 | 0.769–0.919 | 86.8% | 76.4% | <0.0001 |
| SIRI | 2.17 | 0.819 | 0.037 | 0.747–0.891 | 78.9% | 73.1% | <0.0001 |
| AISI | 504.97 | 0.784 | 0.041 | 0.704–0.864 | 76.3% | 72.2% | <0.0001 |
| Restenosis | Mortality | |
|---|---|---|
| Low-MLR vs. high-MLR | 15/225 (6.67%) vs. 60/144 (41.67%) p < 0.0001 | 10/237 (4.22%) vs. 28/132 (21.21%) p < 0.0001 |
| Low-NLR vs. high-NLR | 7/236 (2.97%) vs. 68/133 (51.13%) p < 0.0001 | 4/274 (1.46%) vs. 34/95 (57.36%) p < 0.0001 |
| Low-PLR vs. high-PLR | 21/255 (8.24%) vs. 54/114 (47.37%) p < 0.0001 | 8/265 (3.02%) vs. 30/104 (28.85%) p < 0.0001 |
| Low-SII vs. high-SII | 14/251 (5.58%) vs. 61/118 (51.69%) p < 0.0001 | 5/258 (1.94%) vs. 33/111 (29.73%) p < 0.0001 |
| Low-SIRI vs. high-SIRI | 14/247 (5.67%) vs. 61/122 (50%) p < 0.0001 | 8/248 (3.23%) vs. 30/121 (24.79%) p < 0.0001 |
| Low-AISI vs. high-AISI | 13/242 (5.37%) vs. 62/127 (48.82%) p < 0.0001 | 9/247 (3.64%) vs. 29/122 (23.77%) p < 0.0001 |
| Restenosis | Mortality | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age > 70 | 3.26 | 1.79–5.93 | <0.001 | 5.44 | 1.59–18.60 | 0.007 |
| AH | 2.30 | 1.26–4.19 | 0.006 | 2.13 | 0.77–5.85 | 0.14 |
| IHD | 1.42 | 0.95–2.10 | 0.08 | 1.11 | 0.71–1.73 | 0.64 |
| AF | 1.74 | 1.06–2.87 | 0.02 | 1.26 | 0.85–1.87 | 0.24 |
| MI | 3.16 | 1.83–5.44 | <0.001 | 2.83 | 1.37–5.85 | 0.005 |
| Tobacco | 2.55 | 1.46–4.46 | <0.001 | 2.31 | 0.97–5.50 | 0.058 |
| Obesity | 1.90 | 1.10–3.28 | 0.02 | 1.94 | 0.93–4.05 | 0.07 |
| Dyslipidemia | 5.27 | 3.07–9.02 | <0.001 | 2.80 | 1.37–5.71 | 0.005 |
| Unstable Plaques | 2.83 | 1.67–4.78 | <0.001 | 2.40 | 1.02–5.63 | 0.04 |
| Thrombotic Plaques | 2.77 | 1.57–4.90 | <0.001 | 1.73 | 0.69–4.35 | 0.24 |
| Antiplatelet | 0.46 | 0.27–0.78 | 0.004 | 1.07 | 0.47–2.46 | 0.85 |
| Statins | 0.59 | 0.35–0.78 | 0.04 | 0.75 | 0.32–1.72 | 0.50 |
| Ezetimibe | 0.45 | 0.21–0.95 | 0.03 | 0.74 | 0.24–2.24 | 0.74 |
| high-MLR | 10.37 | 5.38–18.58 | <0.001 | 6.11 | 2.86–13.04 | <0.001 |
| high-NLR | 34.22 | 14.99–78.12 | <0.001 | 37.62 | 12.87–109.97 | <0.001 |
| high-PLR | 12.02 | 6.62–17.88 | <0.001 | 16.06 | 5.78–44.61 | <0.001 |
| high-SII | 18.11 | 9.46–34.66 | <0.001 | 31.70 | 10.37–96.84 | <0.001 |
| high-SIRI | 16.64 | 8.72–31.74 | <0.001 | 9.89 | 4.37–22.37 | <0.001 |
| high-AISI | 16.80 | 8.69–32.45 | <0.001 | 8.24 | 3.76–18.08 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niculescu, R.; Russu, E.; Arbănași, E.M.; Kaller, R.; Arbănași, E.M.; Melinte, R.M.; Coșarcă, C.M.; Cocuz, I.G.; Sabău, A.H.; Tinca, A.C.; et al. Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy. Int. J. Environ. Res. Public Health 2022, 19, 13934. https://doi.org/10.3390/ijerph192113934
Niculescu R, Russu E, Arbănași EM, Kaller R, Arbănași EM, Melinte RM, Coșarcă CM, Cocuz IG, Sabău AH, Tinca AC, et al. Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy. International Journal of Environmental Research and Public Health. 2022; 19(21):13934. https://doi.org/10.3390/ijerph192113934
Chicago/Turabian StyleNiculescu, Raluca, Eliza Russu, Emil Marian Arbănași, Réka Kaller, Eliza Mihaela Arbănași, Răzvan Marian Melinte, Cătălin Mircea Coșarcă, Iuliu Gabriel Cocuz, Adrian Horațiu Sabău, Andreea Cătălina Tinca, and et al. 2022. "Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy" International Journal of Environmental Research and Public Health 19, no. 21: 13934. https://doi.org/10.3390/ijerph192113934