


COVID-19—Infections and Immunization of Inmates in Penitentiary Institutions in Poland in 2021
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Snowden, F.M. Epidemics and Society: From the Black Death to the Present; Yale University Press: New Haven, CT, USA; London, UK, 2020. [Google Scholar]
- Word Health Organization Regional Office for Europe. Preparedness, Prevention and Control of COVID-19 in Prisons and Other Places of Detention; Word Health Organization Regional Office for Europe: Copenhagen, Denmark, 2021. [Google Scholar]
- Walmsley, R. World Prison Population List, 12th ed.; World Prison Brief, Institute for Criminal Policy Research: London, UK, 2015. [Google Scholar]
- Fazel, S.; Hayes, A.J.; Bartellas, K.; Clerici, M.; Trestman, R. Mental health of prisoners, prevalence, adverse outcomes and interventions. Lancet Psychiatry 2016, 3, 871–878. [Google Scholar] [CrossRef] [Green Version]
- Niełaczna, M. COVID-19 a funkcjonowanie polskiego więziennictwa [COVID-19 and the functioning of the Polish prison system]. Nowa Kodyfikacja Prawa Karnego 2020, 57, 87–104. [Google Scholar] [CrossRef]
- Wallace, M.; Marlow, M.; Simonson, S.; Walker, M.; Christophe, N.; Dominguez, O.; Kleamenakis, L.; Orellana, A.; Pagan-Pena, D.; Singh, C.; et al. Public health response to COVID-19 cases in correctional and detention facilities—Louisiana. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Hawks, L.; Woolhandler, S.; McCormick, D. COVID-19 in prisons and jails in the United States. JAMA Intern. Med. 2020, 180, 1041–1042. [Google Scholar] [CrossRef] [PubMed]
- Maruschak, L.M.; Berzofsky, M.; Unangst, J. Medical Problems of State and Federal Prisoners and Jail Inmates, 2011–2012; Special Report; Department of Justice, Bureau of Justice Statistics: Washington, DC, USA, 2015.
- Heard, C. Commentary: Assessing Global Impact of the COVOD-19 Pandemic on Prison Populations. In the Global Impact of the COVID-19 Pandemic on Institutional and Community Corrections; Byrne, J.M., Hammer, D., Rapisarda, S., Eds.; Routledge: London, UK; New York, NY, USA, 2022. [Google Scholar]
- Dunkel, F.; Harrendorf, S.; van Zyl Smit, D. The Impact of COVID-19 on Prison Conditions and Penal Policy; Routledge: London, UK, 2022. [Google Scholar]
- Aebi, M.E.; Cocco, E.; Molnar, L.; Tiago, M.M. Prisons and Prisoners in Europe 2021: Key Findings of the SPACE; Series UNILCRIM 2022/3; Council of Europe and University of Lausanne: Lausanne, Switzerland, 2022. [Google Scholar]
- Stańdo-Kawecka, B. Populacja więzienna w Polsce w pierwszym roku pandemii COVID-19 [The prison population in Poland in the first year of the COVID-19 pandemic]. Arch. Kryminol. 2021, 43, 127–149. [Google Scholar]
- Act of March 2, 2020 on Special Solutions Related to the Prevention, Counteraction and Combating of COVID-19, Other Infectious Diseases and Crisis Situations Caused by Them (Journal of Laws of 2021, Item 2095, as Amended). Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20200000374 (accessed on 5 May 2022).
- Augustynowicz, A.; Wójcik, M.; Bachurska, B.; Opolski, J.; Czerw, A.; Raczkiewicz, D.; Pinkas, J. COVID-1–Infection prevention in prisons and jails in Poland. Ann. Agric. Environ. Med. 2021, 28, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Seguera, V.G.; Garcia-Basteiro, A.I.; Bayas, J.M. The role of vaccination in prisoners health. Expert Rev. Vaccines 2013, 12, 469–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarthy, C.V.; O’Mara, O.; van Leeuwen, E.; Jit, M.; Sandmann, F. The impact of COVID-19 in England and Wales: A metapopulation model. BMC Public Health 2022, 22, 1003. [Google Scholar] [CrossRef] [PubMed]
- Brinkley-Rubinstein, L.; Peteron, M.; Martin, R.; Chan, P.; Berk, J. Breakthrough SARS CoV-2 infections in prisons after vaccination. N. Engl. J. Med. 2021, 385a, 1051–1052. [Google Scholar] [CrossRef] [PubMed]
- The Act of 6 September 2001 on Access to Public Information. Available online: https://www.global-regulation.com/translation/poland/7049976/the-act-of-6-september-2001-on-access-to-public-information.html (accessed on 4 May 2020).
- Regulation of the Minister of Health of February 25, 2021 on Infectious Diseases Resulting in the Obligation of Hospitalization, Isolation or Isolation at Home, and the Obligation of Quarantine or Epidemiological Supervision (Journal of Laws of 2021, item 351, as Amended). Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20210000351 (accessed on 5 May 2020).
- World Health Organization. Antigen-detection in the diagnosis of SARS-CoV-2 infection using rapid immunoassays. In Interim Guidance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- National COVID-19 Immunization Program; National COVID-19 Immunization Program: Warsaw, Poland, 2020.
- Available online: https://www.gov.pl/web/koronawirus/wykaz-zarazen-koronawirusem-sars-cov-2 (accessed on 13 July 2022).
- Saloner, B.; Parish, K.; Ward, J.A.; Dilaura, G.; Dolovichet, S. COVID-19 cases and death in federal and state prisons. JAMA 2020, 324, 602–603. [Google Scholar] [CrossRef] [PubMed]
- Marquez, N.; Ward, J.A.; Parish, K.; Saloner, B.; Dolovich, S. COVID-19 incidence and mortality in federal state prisons compared with the US population. JAMA 2021, 325, 1865–1867. [Google Scholar] [CrossRef] [PubMed]
- Aebi, M.F.; Tiago, M.M. Prisons and Prisoners in Europe in Pandemic Times: An Evaluation of the Short-Term Impact of the COVID-19 on Prison Populations; Unil. Ecole de Sciences Criminalles, Council of Europe and University of Lausanne: Lausanne, Switzerland, 2020. [Google Scholar]
- Mazzilli, S.; Tavoschi, L.; Soria, A.; Fornili, M.; Cocca, G.; Sebastiani, T.; Scardina, G.; Cairone, C.; Arzilli, G.; Lapadula, G.; et al. COVID-19 Infection Among Incarcerated Individuals and Prison Staff in Lombardy. JAMA Netw. Open 2022, 5, e224862. [Google Scholar]
- Rapisarda, S.; Byrne, J.M.; Marmolejo, L. An Examination of COVID-19 Outbreaks in South American Prisons and Jails. Vict. Offenders 2020, 15, 1009–1018. [Google Scholar] [CrossRef]
- Penal Reform International, Harm Reduction International. COVID-19 Vaccinations for Prison Populations and Staff: Report on Global Scan; Harm Reduction International: London, UK, 2021. [Google Scholar]
- Word Health Organization. Updated WHO SAGE. Roadmap for Prioritizing Uses of COVID-19 Vaccines in the Context of Limited Supply; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Liu, E.Y.; Oto, J.; Will, J.; Liu, Y.E.; Oto, J.; Will, J.; LeBoa, C.; Doyle, A.; Rens, N.; Aggarwal, S.; et al. Factors associated with COVID-19 vaccine acceptance and hesitancy among residents of Northern California jails. Preventive Medicine Reports. Prev. Med. Rep. 2022, 27, 101771. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Paredes, D.; Varsaneux, O.; Worthington, J.; Park, H.; MacDonald, S.; Basta, N.; Lebouche, B.; Cox, J.; Ismail, S.; Kronfli, N. Reasons for COVID-19 vaccine refusal among people incarcerated in Canadian federal prisons. PLoS ONE 2022, 17, e0264145. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Month | Inmates | ||||
|---|---|---|---|---|---|
| Infected | Referred to Quarantine | Total Number of Inmates As of the Last Day of the Month | |||
| n | % | n | % | ||
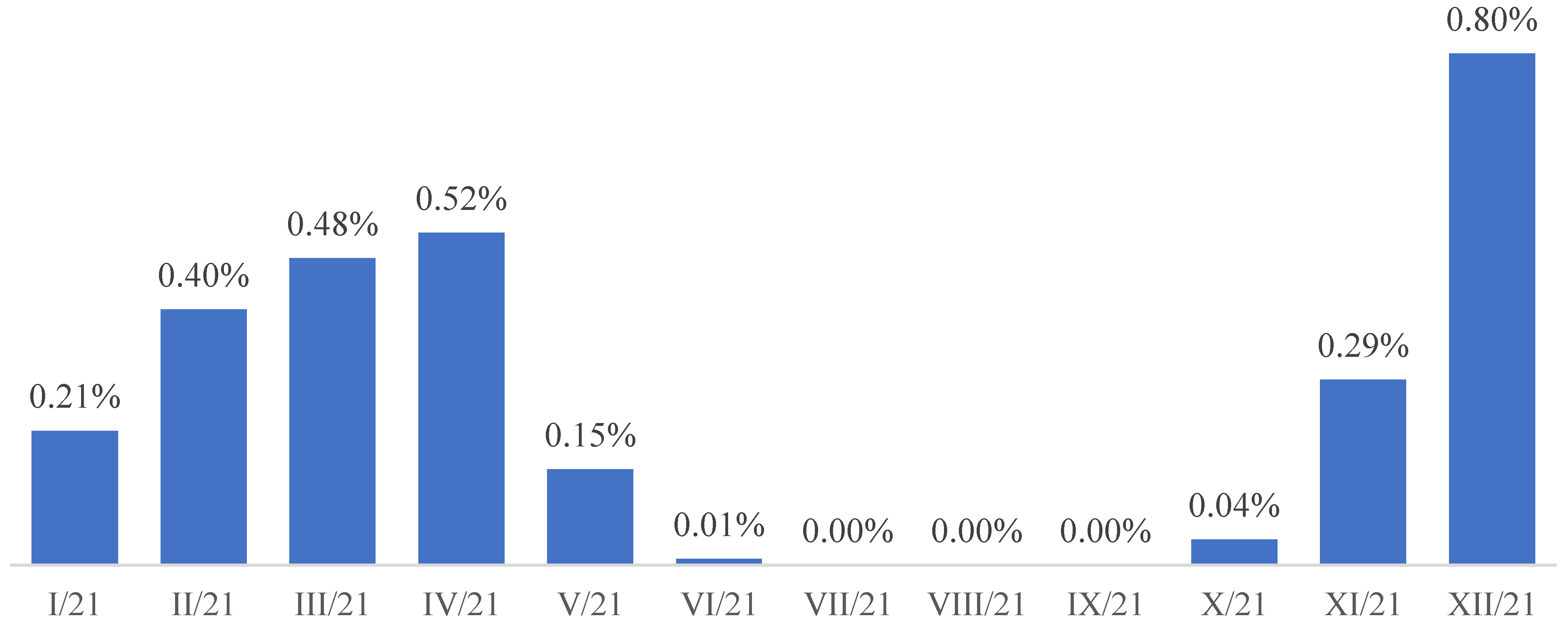
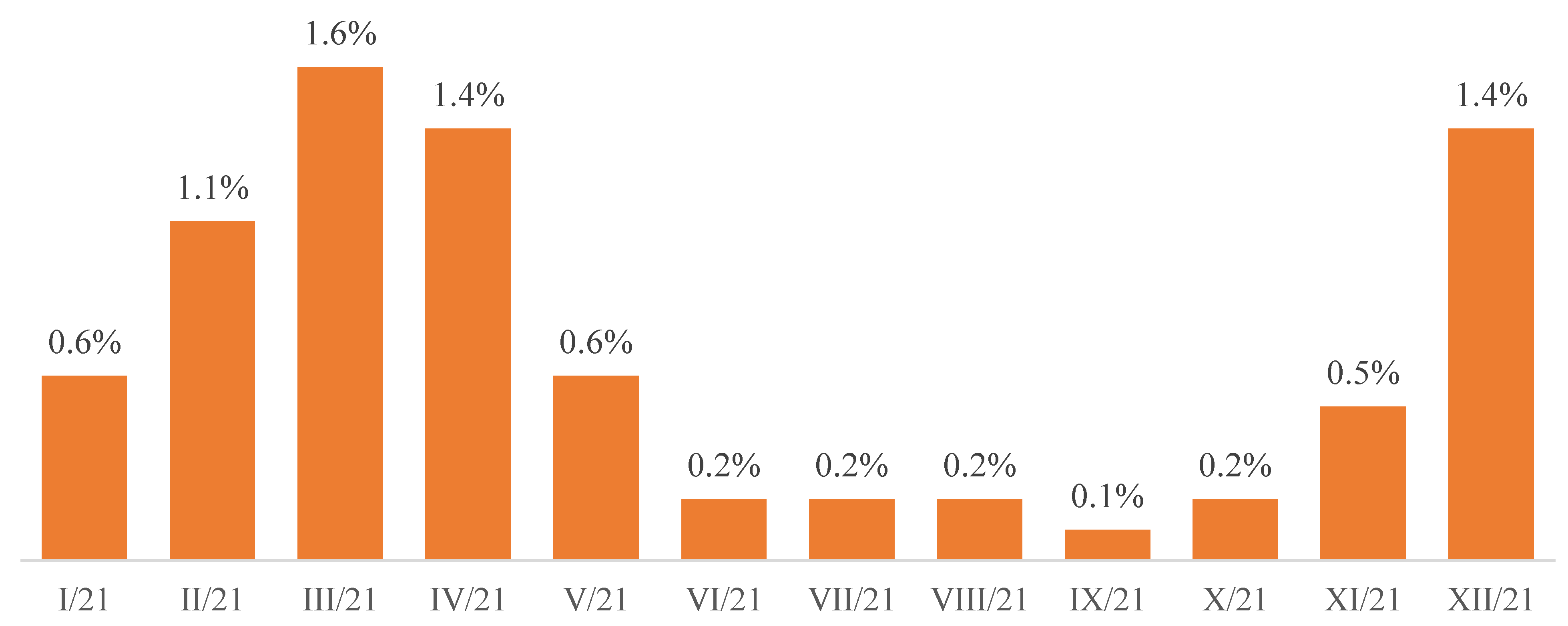
| January | 142 | 0.21% | 425 | 0.60% | 68,852 |
| February | 281 | 0.40% | 742 | 1.10% | 70,117 |
| March | 339 | 0.48% | 1162 | 1.60% | 71,297 |
| April | 374 | 0.52% | 985 | 1.40% | 71,258 |
| May | 105 | 0.15% | 441 | 0.60% | 71,375 |
| June | 9 | 0.01% | 157 | 0.20% | 71,640 |
| July | 0 | 0.00% | 113 | 0.20% | 71,960 |
| August | 2 | 0.00% | 115 | 0.20% | 71,907 |
| September | 0 | 0.00% | 87 | 0.10% | 71,291 |
| October | 29 | 0.04% | 119 | 0.20% | 71,391 |
| November | 209 | 0.29% | 342 | 0.50% | 71,546 |
| December | 575 | 0.80% | 1019 | 1.40% | 71,874 |
| District Inspectorate of the Prison Service | Number of Inmates Vaccinated with One Dose | Number of Inmates Vaccinated with Two Doses | Number of Inmates Vaccinated with a Single-Dose Product | % Inmates Fully Vaccinated |
|---|---|---|---|---|
| Białystok | 22 | 159 | 3626 | 2.6% |
| Bydgoszcz | 38 | 371 | 6153 | 4.5% |
| Gdańsk | 162 | 422 | 4378 | 3.3% |
| Katowice | 726 | 841 | 5817 | 4.6% |
| Koszalin | 832 | 463 | 2493 | 2.0% |
| Kraków | 20 | 474 | 4171 | 3.2% |
| Lublin | 14 | 285 | 3725 | 2.8% |
| Łódź | 1233 | 1114 | 3362 | 3.1% |
| Olsztyn | 779 | 752 | 3030 | 2.6% |
| Opole | 106 | 1123 | 2903 | 2.8% |
| Poznań | 320 | 612 | 4957 | 3.8% |
| Rzeszów | 2105 | 1947 | 1384 | 2.3% |
| Szczecin | 180 | 238 | 3749 | 2.7% |
| Warszawa | 308 | 282 | 6015 | 4.3% |
| Wrocław | 371 | 441 | 6296 | 4.6% |
| TOTAL | 7216 | 9524 | 62,059 | 49.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Augustynowicz, A.; Bachurska, B.; Wójcik, M.; Borowska, M.; Czerw, A.; Opolski, J.; Słabicka, K.; Pinkas, J. COVID-19—Infections and Immunization of Inmates in Penitentiary Institutions in Poland in 2021. Int. J. Environ. Res. Public Health 2022, 19, 13725. https://doi.org/10.3390/ijerph192113725
Augustynowicz A, Bachurska B, Wójcik M, Borowska M, Czerw A, Opolski J, Słabicka K, Pinkas J. COVID-19—Infections and Immunization of Inmates in Penitentiary Institutions in Poland in 2021. International Journal of Environmental Research and Public Health. 2022; 19(21):13725. https://doi.org/10.3390/ijerph192113725
Chicago/Turabian StyleAugustynowicz, Anna, Beata Bachurska, Michał Wójcik, Mariola Borowska, Aleksandra Czerw, Janusz Opolski, Karolina Słabicka, and Jarosław Pinkas. 2022. "COVID-19—Infections and Immunization of Inmates in Penitentiary Institutions in Poland in 2021" International Journal of Environmental Research and Public Health 19, no. 21: 13725. https://doi.org/10.3390/ijerph192113725