
Correlation between Endophthalmitis and Stroke Development in Ankylosing Spondylitis Patients: A Population-Based Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
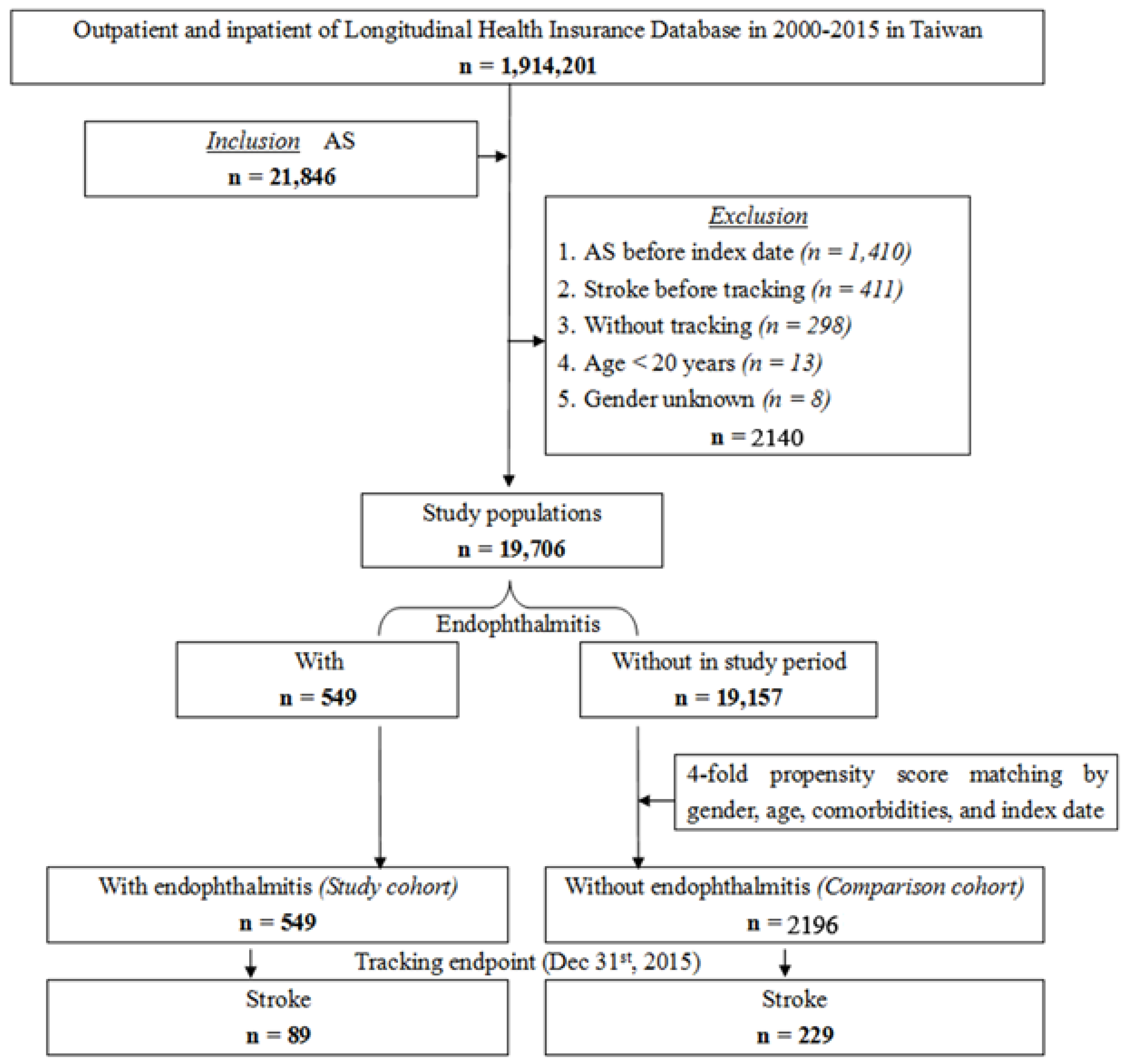
2.1. Research Database
2.2. Study Participants
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Han, C.; Robinson, D.W., Jr.; Hackett, M.V.; Paramore, L.C.; Fraeman, K.H.; Bala, M.V. Cardiovascular disease and risk factors in patients with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis. J. Rheumatol. 2006, 33, 2167–2172. [Google Scholar] [PubMed]
- Szabo, S.M.; Levy, A.R.; Rao, S.R.; Kirbach, S.E.; Lacaille, D.; Cifaldi, M.; Maksymowych, W.P. Increased risk of cardiovascular and cerebrovascular diseases in individuals with ankylosing spondylitis: A population-based study. Arthritis Rheum. 2011, 63, 3294–3304. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.J.; Hsu, J.L.; Lin, S.M.; Chou, C.C.; Wang, L.H.; Wang, J.; Bai, C.H.; Chiou, H.Y. Increased risk of stroke among patients with ankylosing spondylitis: A population-based matched-cohort study. Rheumatol. Int. 2014, 34, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Ma, W.; Liu, H.; Li, C.; Zhang, Y.; Liu, J.; Liang, Y.; Zhang, S.; Wu, Z.; Zang, C.; et al. Stroke risk in arthritis: A systematic review and meta-analysis of cohort studies. PLoS ONE 2021, 16, e0248564. [Google Scholar] [CrossRef]
- Sherer, Y.; Shoenfeld, Y. Mechanisms of disease: Atherosclerosis in autoimmune diseases. Nat. Clin. Pract. Rheumatol. 2006, 2, 99–106. [Google Scholar] [CrossRef]
- Hankey, G.J. Stroke. Lancet 2017, 389, 641–654. [Google Scholar] [CrossRef]
- Josef, A.; Costantino, I. Inflammation and Stroke: An Overview. Neurotherapeutics 2016, 13, 661–670. [Google Scholar]
- Grau, A.; Urbanek, C.; Palm, F. Common infections and the risk of stroke. Nat. Rev. Neurol. 2010, 6, 681–694. [Google Scholar] [CrossRef]
- Pokharel, D.; Doan, A.P.; Lee, A.G. Group B streptococcus endogenous endophthalmitis presenting as septic arthritis and a homonymous hemianopsia due to embolic stroke. Am. J. Ophthalmol. 2004, 138, 300–302. [Google Scholar] [CrossRef]
- Christy, C.; Jered, W.; Veena, R. Endophthalmitis. Disease-a-Month 2017, 63, 45–48. [Google Scholar]
- Gopalamurugan, A.B.; Wheatcroft, S.; Hunter, P.; Thomas, M.R. Bilateral Endophthalmitis and ARDS Complicating Group G Streptococcal Endocarditis. Lancet 2005, 366, 2062. [Google Scholar] [CrossRef]
- Yin, W.; Zhou, H.; Li, C. Endogenous Klebsiella Pneumoniae Endophthalmitis. Am. J. Emerg. Med. 2014, 32, 1300.e3–1300.e5. [Google Scholar] [CrossRef]
- Brophy, S.; Cooksey, R.; Atkinson, M.; Zhou, S.M.; Husain, M.J.; Macey, S.; Rahman, M.A.; Siebert, S. No increased rate of acute myocardial infarction or stroke among patients with ankylosing spondylitis-a retrospective cohort study using routine data. Semin. Arthritis Rheum. 2012, 42, 140–145. [Google Scholar] [CrossRef]
- Kang, J.H.; Chen, Y.H.; Lin, H.C. Comorbidity profiles among patients with ankylosing spondylitis: A nationwide population-based study. Ann. Rheum. Dis. 2010, 69, 1165–1168. [Google Scholar] [CrossRef]
- Wang, W.; Jiang, B.; Sun, H.; Ru, X.; Sun, D.; Wang, L.; Wang, L.; Jiang, Y.; Li, Y.; Wang, Y.; et al. Prevalence, Incidence, and Mortality of Stroke in China: Results from a Nationwide Population-Based Survey of 480 687 Adults. Circulation 2017, 135, 759–771. [Google Scholar] [CrossRef]
- Wen, L.Y.; Ni, H.; Li, K.S.; Yang, H.H.; Cheng, J.; Wang, X.; Zhao, D.S.; Xie, M.Y.; Su, H. Asthma and risk of stroke: A systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 2016, 25, 497–503. [Google Scholar] [CrossRef]
- Son, M.K.; Lim, N.K.; Kim, H.W.; Park, H.Y. Risk of ischemic stroke after atrial fibrillation diagnosis: A national sample cohort. PLoS ONE 2017, 12, e0179687. [Google Scholar] [CrossRef] [Green Version]
- Morgan, A.D.; Sharma, C.; Rothnie, K.J.; Potts, J.; Smeeth, L.; Quint, J.K. Chronic obstructive pulmonary disease and the risk of stroke. Ann. Am. Thorac. Soc. 2017, 14, 754–765. [Google Scholar] [CrossRef]
- Kang, S.H.; Kim, J.; Park, J.J.; Oh, I.Y.; Yoon, C.H.; Kim, H.J.; Kim, K.; Choi, D.J. Risk of stroke in congestive heart failure with and without atrial fibrillation. Int. J. Cardiol. 2017, 248, 182–187. [Google Scholar] [CrossRef]
- Olesen, K.K.W.; Madsen, M.; Lip, G.Y.H.; Egholm, G.; Thim, T.; Jensen, L.O.; Raungaard, B.; Nielsen, J.C.; Bøtker, H.E.; Sørensen, H.T.; et al. Coronary artery disease and risk of adverse cardiac events and stroke. Eur. J. Clin. Investig. 2017, 47, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Sarwar, N.; Gao, P.; Seshasai, S.R.K.; Gobin, R.; Kaptoge, S.; Angelantonio, E.D.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; Stampfer, M.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar]
- Alloubani, A.; Nimer, R.; Samara, R. Relationship between hyperlipidemia, cardiovascular disease and stroke: A systematic review. Curr. Cardiol. Rev. 2021, 17, e051121189015. [Google Scholar] [CrossRef]
- Liu, Y.; Li, J.; Dou, Y.; Ma, H. Impacts of type 2 diabetes mellitus and hypertension on the incidence of cardiovascular diseases and stroke in China real-world setting: A retrospective cohort study. BMJ Open 2021, 11, e053698. [Google Scholar] [CrossRef]
- Vallejo-Garcia, J.L.; Asencio-Duran, M.; Pastora-Salvador, N.; Vinciguerra, P.; Romano, M.R. Role of inflammation in endophthalmitis. Mediat. Inflamm. 2012, 2012, 196094. [Google Scholar] [CrossRef]
- Jin, R.; Liu, L.; Zhang, S.; Nanda, A.; Li, G. Role of inflammation and its mediators in acute ischemic stroke. J. Cardiovasc. Transl. Res. 2013, 6, 834–851. [Google Scholar] [CrossRef] [Green Version]
- Iadecola, C.; Buckwalter, M.S.; Anrather, J. Immune Responses to Stroke: Mechanisms, Modulation, and Therapeutic Potential. J. Clin. Investig. 2020, 130, 2777–2788. [Google Scholar] [CrossRef]
- Wu, T.Y.; Majeed, A.; Kuo, K.N. An overview of the healthcare system in Taiwan. Lond. J. Prim. Care 2010, 3, 115–119. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Endophthalmitis | Total | With | Without | P | |||
|---|---|---|---|---|---|---|---|
| Variables | n | % | n | % | n | % | |
| Total | 2745 | 549 | 20.00 | 2196 | 80.00 | ||
| Gender | 0.999 | ||||||
| Male | 1535 | 55.92 | 307 | 55.92 | 1228 | 55.92 | |
| Female | 1210 | 44.08 | 242 | 44.08 | 968 | 44.08 | |
| Age (years) | 37.07 ± 19.23 | 37.00 ± 18.65 | 37.08 ± 19.80 | 0.892 | |||
| Age group (yrs) | 0.999 | ||||||
| 20–39 | 1600 | 58.29 | 320 | 58.29 | 1280 | 58.29 | |
| 40–59 | 765 | 27.87 | 153 | 27.87 | 612 | 27.87 | |
| ≥60 | 380 | 13.84 | 76 | 13.84 | 304 | 13.84 | |
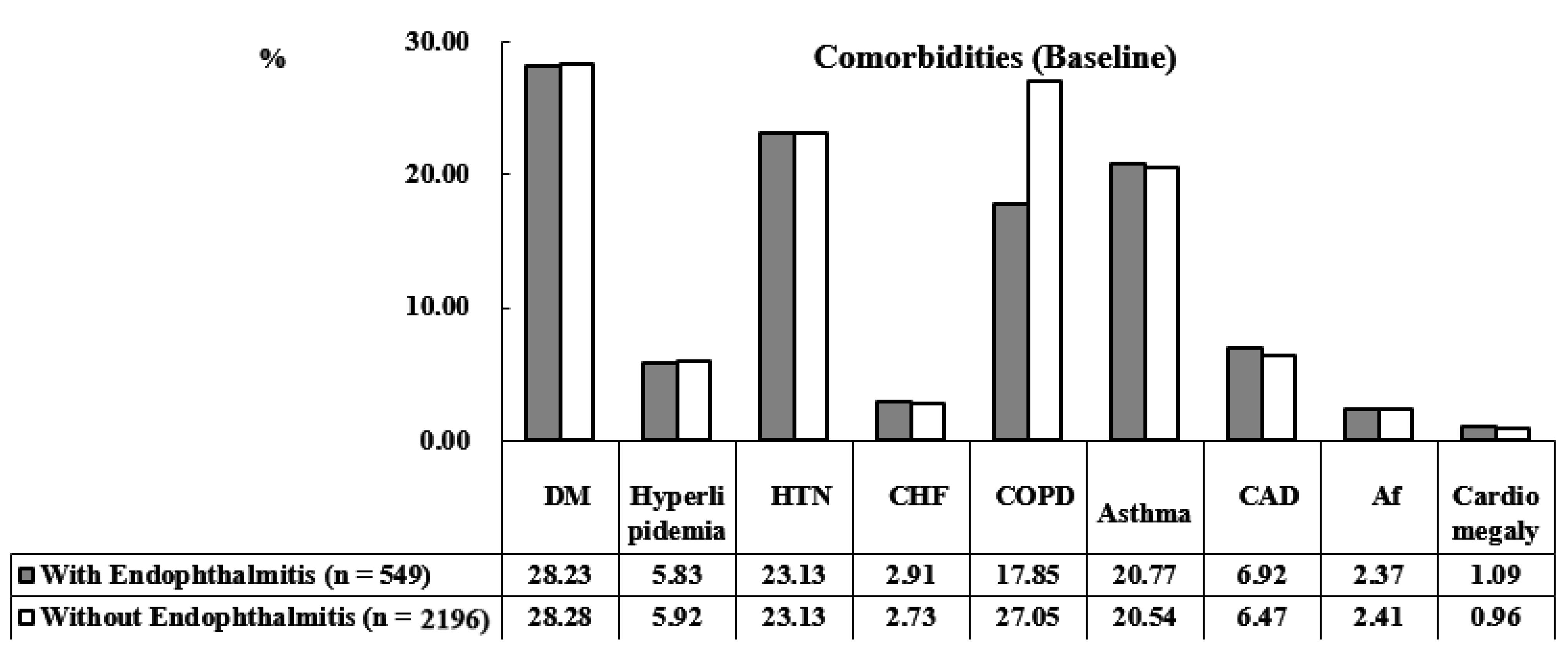
| DM | 0.922 | ||||||
| Without | 1969 | 71.73 | 394 | 71.77 | 1575 | 71.72 | |
| With | 776 | 28.27 | 155 | 28.23 | 621 | 28.28 | |
| Hyperlipidemia | 0.857 | ||||||
| Without | 2583 | 94.10 | 517 | 94.17 | 2066 | 94.08 | |
| With | 162 | 5.90 | 32 | 5.83 | 130 | 5.92 | |
| HTN | 0.935 | ||||||
| Without | 2110 | 76.87 | 422 | 76.87 | 1688 | 76.87 | |
| With | 635 | 23.13 | 127 | 23.13 | 508 | 23.13 | |
| CHF | 0.850 | ||||||
| Without | 2669 | 97.23 | 533 | 97.09 | 2136 | 97.27 | |
| With | 76 | 2.77 | 16 | 2.91 | 60 | 2.73 | |
| COPD | 0.883 | ||||||
| Without | 2053 | 74.79 | 451 | 82.15 | 1602 | 72.95 | |
| With | 692 | 25.21 | 98 | 17.85 | 594 | 27.05 | |
| Asthma | 0.752 | ||||||
| Without | 2180 | 79.42 | 435 | 79.23 | 1745 | 79.46 | |
| With | 565 | 20.58 | 114 | 20.77 | 451 | 20.54 | |
| CAD | 0.582 | ||||||
| Without | 2565 | 93.44 | 511 | 93.08 | 2054 | 93.53 | |
| With | 180 | 6.56 | 38 | 6.92 | 142 | 6.47 | |
| Af | 0.968 | ||||||
| Without | 2679 | 97.60 | 536 | 97.63 | 2143 | 97.59 | |
| With | 66 | 2.40 | 13 | 2.37 | 53 | 2.41 | |
| Cardiomegaly | 0.569 | ||||||
| Without | 2718 | 99.02 | 543 | 98.91 | 2175 | 99.04 | |
| With | 27 | 0.98 | 6 | 1.09 | 21 | 0.96 | |
| CCI_R | 0.91 ± 1.13 | 0.93 ± 1.19 | 0.90 ± 1.11 | 0.218 | |||
| Endophthalmitis | Total | With | Without | P | |||
|---|---|---|---|---|---|---|---|
| Variables | n | % | n | % | n | % | |
| Total | 2745 | 549 | 20.00 | 2196 | 80.00 | ||
| Stroke | <0.001 | ||||||
| Without | 2427 | 88.42 | 460 | 83.79 | 1967 | 89.57 | |
| With | 318 | 11.58 | 89 | 16.21 | 229 | 10.43 | |
| Gender | 0.999 | ||||||
| Male | 1535 | 55.92 | 307 | 55.92 | 1228 | 55.92 | |
| Female | 1210 | 44.08 | 242 | 44.08 | 968 | 44.08 | |
| Age (yrs) | 41.47 ± 19.97 | 41.24 ± 19.78 | 41.53 ± 20.02 | 0.613 | |||
| Age group (yrs) | 0.658 | ||||||
| 20–39 | 1556 | 56.70 | 310 | 56.45 | 1246 | 56.76 | |
| 40–59 | 756 | 27.53 | 148 | 27.04 | 607 | 27.65 | |
| ≥60 | 433 | 15.78 | 91 | 16.51 | 342 | 15.59 | |
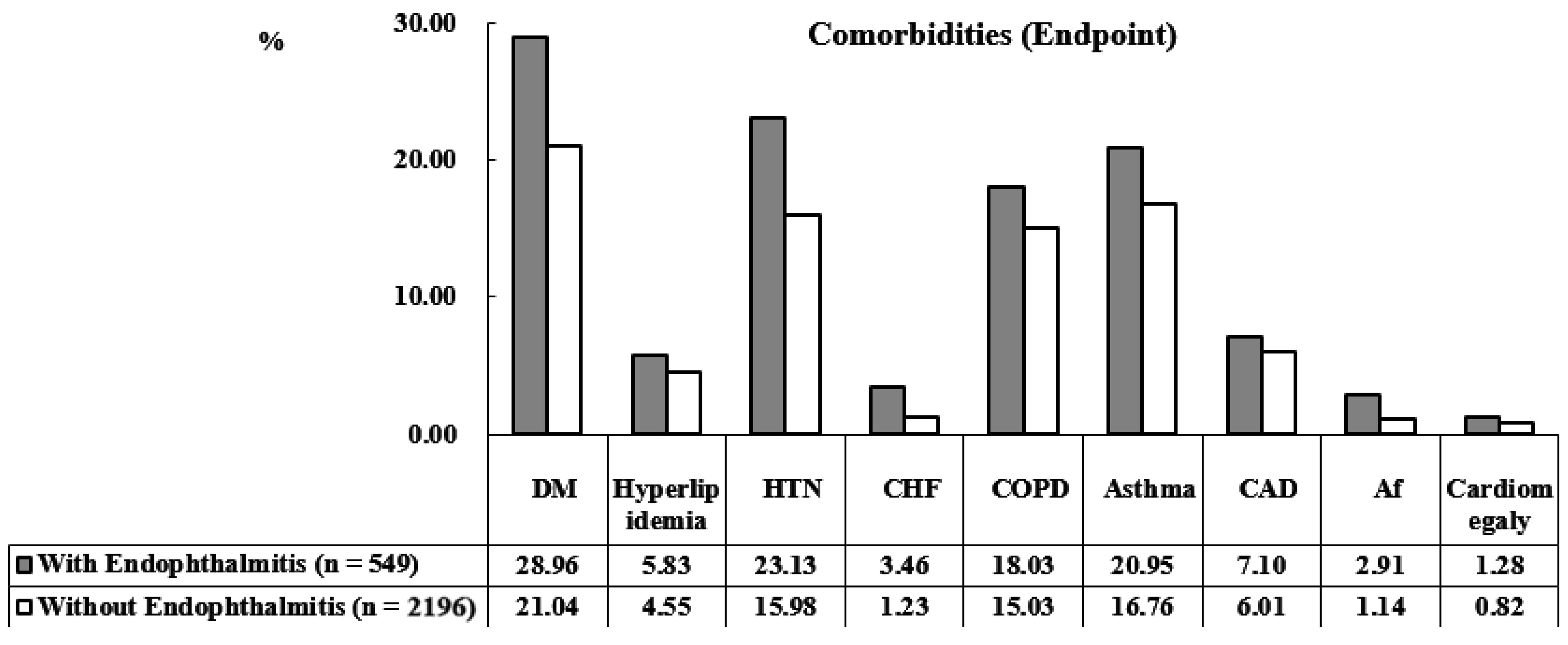
| DM | <0.001 | ||||||
| Without | 2124 | 77.38 | 390 | 71.04 | 1734 | 78.96 | |
| With | 621 | 22.62 | 159 | 28.96 | 462 | 21.04 | |
| Hyperlipidemia | 0.067 | ||||||
| Without | 2613 | 95.19 | 517 | 94.17 | 2096 | 95.45 | |
| With | 132 | 4.81 | 32 | 5.83 | 100 | 4.55 | |
| HTN | <0.001 | ||||||
| Without | 2267 | 82.59 | 422 | 76.87 | 1845 | 84.02 | |
| With | 478 | 17.41 | 127 | 23.13 | 351 | 15.98 | |
| CHF | <0.001 | ||||||
| Without | 2699 | 98.32 | 530 | 96.54 | 2169 | 98.77 | |
| With | 46 | 1.68 | 19 | 3.46 | 27 | 1.23 | |
| COPD | <0.001 | ||||||
| Without | 2316 | 84.37 | 450 | 81.97 | 1866 | 84.97 | |
| With | 429 | 15.63 | 99 | 18.03 | 330 | 15.03 | |
| Asthma | <0.001 | ||||||
| Without | 2262 | 82.40 | 434 | 79.05 | 1828 | 83.24 | |
| With | 483 | 17.60 | 115 | 20.95 | 368 | 16.76 | |
| CAD | 0.284 | ||||||
| Without | 2574 | 93.77 | 510 | 92.90 | 2064 | 93.99 | |
| With | 171 | 6.23 | 39 | 7.10 | 132 | 6.01 | |
| Af | <0.001 | ||||||
| Without | 2704 | 98.51 | 533 | 97.09 | 2171 | 98.86 | |
| With | 41 | 1.49 | 16 | 2.91 | 25 | 1.14 | |
| Cardiomegaly | 0.240 | ||||||
| Without | 2720 | 99.09 | 542 | 98.72 | 2178 | 99.18 | |
| With | 25 | 0.91 | 7 | 1.28 | 18 | 0.82 | |
| CCI_R | 0.95 ± 1.13 | 0.98 ± 1.16 | 0.89 ± 1.11 | 0.026 | |||
| All-caused mortality | 0.002 | ||||||
| Without | 2461 | 89.65 | 475 | 86.52 | 1986 | 90.44 | |
| With | 284 | 10.35 | 74 | 13.48 | 210 | 9.56 | |
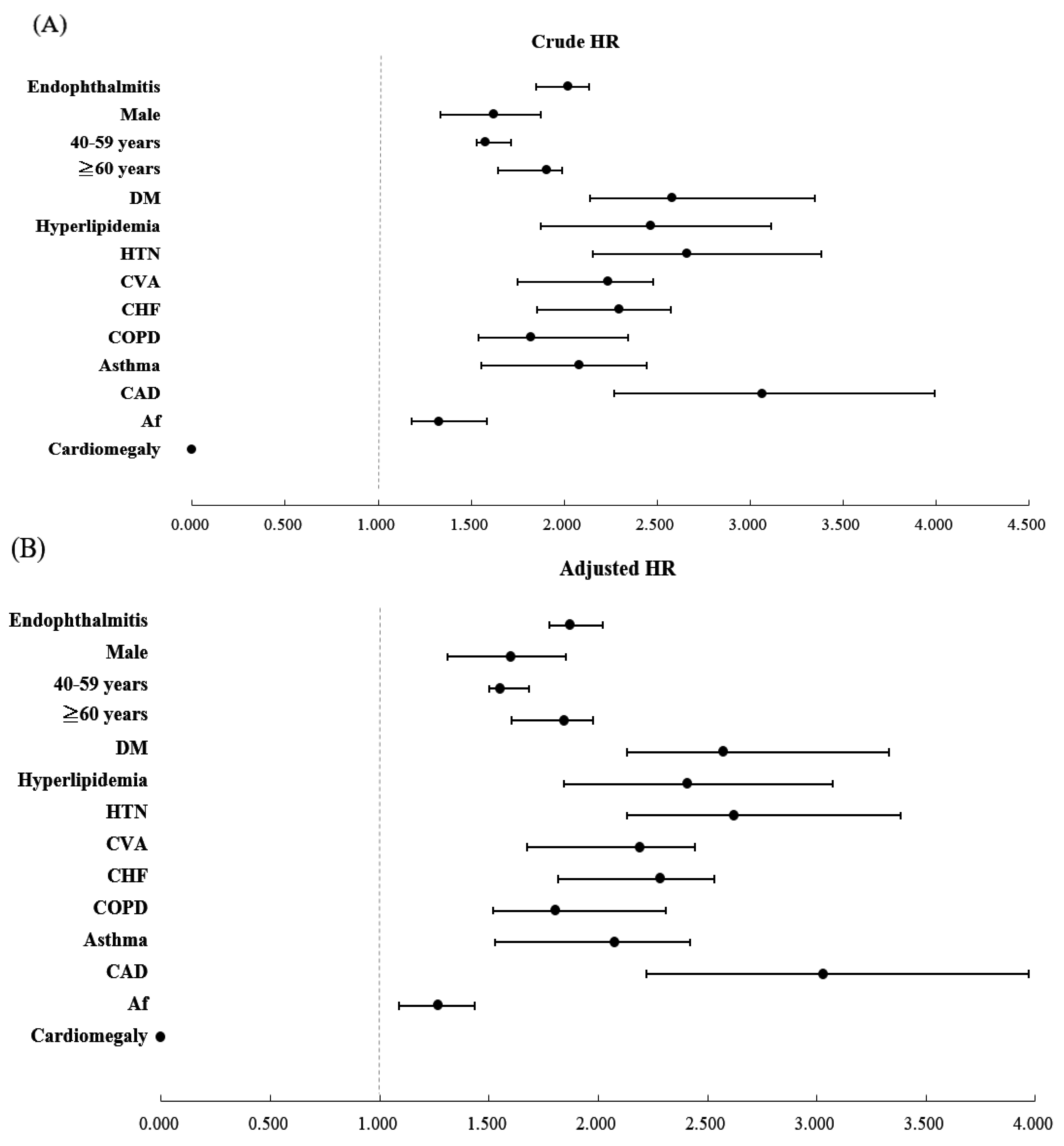
| Variables | Crude HR | 95% CI | 95% CI | P | Adjusted HR | 95% CI | 95% CI | P |
|---|---|---|---|---|---|---|---|---|
| Endophthalmitis | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.021 | 1.850 | 2.135 | <0.001 | 1.873 | 1.776 | 2.022 | <0.001 |
| Gender | ||||||||
| Male | 1.621 | 1.333 | 1.874 | <0.001 | 1.602 | 1.311 | 1.852 | <0.001 |
| Female | Reference | Reference | ||||||
| Age (yrs) | ||||||||
| 20–39 | Reference | Reference | ||||||
| 40–59 | 1.576 | 1.530 | 1.713 | <0.001 | 1.553 | 1.502 | 1.685 | <0.001 |
| ≥60 | 1.906 | 1.644 | 1.991 | <0.001 | 1.843 | 1.602 | 1.975 | <0.001 |
| DM | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.580 | 2.141 | 3.348 | <0.001 | 2.572 | 2.132 | 3.330 | <0.001 |
| Hyperlipidemia | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.469 | 1.872 | 3.112 | <0.001 | 2.410 | 1.841 | 3.072 | <0.001 |
| HTN | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.662 | 2.156 | 3.385 | <0.001 | 2.623 | 2.130 | 3.381 | <0.001 |
| CVA | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.236 | 1.752 | 2.478 | <0.001 | 2.191 | 1.672 | 2.440 | <0.001 |
| CHF | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.297 | 1.855 | 2.573 | <0.001 | 2.286 | 1.817 | 2.532 | <0.001 |
| COPD | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.824 | 1.539 | 2.345 | <0.001 | 1.803 | 1.519 | 2.311 | <0.001 |
| Asthma | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.082 | 1.554 | 2.443 | <0.001 | 2.076 | 1.529 | 2.419 | <0.001 |
| CAD | ||||||||
| Without | Reference | Reference | ||||||
| With | 3.068 | 2.267 | 3.991 | <0.001 | 3.031 | 2.218 | 3.971 | <0.001 |
| Af | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.326 | 1.178 | 1.586 | <0.001 | 1.267 | 1.090 | 1.433 | <0.001 |
| Cardiomegaly | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.000 | - | - | 0.999 | 0.000 | - | - | 0.999 |
| CCI_R | 1.649 | 1.602 | 1.660 | <0.001 | 1.625 | 1.595 | 1.649 | <0.001 |
| Endophthalmitis | With | Without (Reference) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Stratified | Events | PYs | Rate (per 105 PYs) | Events | PYs | Rate (per 105 PYs) | Adjusted HR | 95% CI | 95% CI | P |
| Total | 89 | 5170.50 | 1724.44 | 229 | 21,103.84 | 1085.11 | 1.873 | 1.776 | 2.022 | <0.001 |
| Gender | ||||||||||
| Male | 59 | 2895.28 | 2043.40 | 118 | 11,814.92 | 998.74 | 2.455 | 2.328 | 2.651 | <0.001 |
| Female | 30 | 2275.22 | 1318.55 | 111 | 9288.92 | 1194.97 | 1.270 | 1.205 | 1.371 | <0.001 |
| Age (yrs) | ||||||||||
| 20–39 | 57 | 2918.36 | 1953.15 | 153 | 11,987.22 | 1276.36 | 1.787 | 1.695 | 1.929 | <0.001 |
| 40–59 | 26 | 1390.02 | 1870.48 | 65 | 5838.24 | 1113.35 | 1.900 | 1.802 | 2.051 | <0.001 |
| ≥60 | 6 | 862.12 | 714.76 | 11 | 3278.38 | 335.53 | 3.284 | 3.114 | 3.546 | <0.001 |
| DM | ||||||||||
| Without | 55 | 3705.28 | 1488.74 | 184 | 16,640.57 | 1105.73 | 1.571 | 1.490 | 1.695 | <0.001 |
| With | 34 | 1465.22 | 2320.47 | 45 | 4463.27 | 1008.23 | 2.791 | 2.647 | 3.014 | <0.001 |
| Hyperlipidemia | ||||||||||
| Without | 62 | 4867.61 | 1277.06 | 190 | 20,155.82 | 942.66 | 1.571 | 1.490 | 1.695 | <0.001 |
| With | 27 | 302.89 | 8914.13 | 39 | 948.02 | 4113.84 | 2.734 | 2.592 | 2.952 | <0.001 |
| HTN | ||||||||||
| Without | 53 | 3973.26 | 1338.00 | 183 | 17,668.73 | 1035.73 | 1.522 | 1.444 | 1.644 | <0.001 |
| With | 36 | 1197.24 | 3006.92 | 46 | 3435.11 | 1339.11 | 2.632 | 2.496 | 2.841 | <0.001 |
| CVA | ||||||||||
| Without | 60 | 4872.48 | 1234.73 | 193 | 20,013.39 | 964.35 | 1.502 | 1.424 | 1.621 | <0.001 |
| With | 29 | 298.02 | 9730.89 | 36 | 1090.45 | 3301.39 | 3.591 | 3.404 | 3.877 | <0.001 |
| CHF | ||||||||||
| Without | 77 | 5031.25 | 1533.66 | 214 | 20,831.98 | 1027.27 | 1.761 | 1.669 | 1.900 | <0.001 |
| With | 12 | 139.25 | 8617.59 | 15 | 271.86 | 5517.55 | 1.897 | 1.799 | 2.048 | <0.001 |
| COPD | ||||||||||
| Without | 78 | 4242.07 | 1842.55 | 211 | 17,901.39 | 1178.68 | 1.831 | 1.736 | 1.977 | <0.001 |
| With | 11 | 928.43 | 1184.80 | 18 | 3202.45 | 562.07 | 2.774 | 2.631 | 2.994 | <0.001 |
| Asthma | ||||||||||
| Without | 72 | 4104.26 | 1758.22 | 208 | 17,635.59 | 1179.43 | 1.761 | 1.670 | 1.901 | <0.001 |
| With | 17 | 1066.24 | 1594.39 | 21 | 3468.25 | 605.49 | 3.050 | 2.893 | 3.293 | <0.001 |
| CAD | ||||||||||
| Without | 79 | 4820.06 | 1642.35 | 219 | 19,814.43 | 1105.26 | 1.761 | 1.670 | 1.901 | <0.001 |
| With | 10 | 350.44 | 2853.56 | 10 | 1289.41 | 775.55 | 3.952 | 3.747 | 4.266 | <0.001 |
| Af | ||||||||||
| Without | 86 | 5028.24 | 1713.56 | 227 | 20,975.81 | 1082.20 | 1.865 | 1.767 | 2.012 | <0.001 |
| With | 3 | 142.26 | 2108.81 | 2 | 128.03 | 1562.13 | 2.367 | 2.245 | 2.556 | <0.001 |
| Cardiomegaly | ||||||||||
| Without | 89 | 5100.24 | 1748.19 | 229 | 21,009.16 | 1090.00 | 1.873 | 1.776 | 2.022 | <0.001 |
| With | 0 | 70.26 | 0.00 | 0 | 94.68 | 0.00 | - | - | - | - |
| Endophthalmitis | With | Without (Reference) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Stroke Subgroup | Events | PYs | Rate (per 105 PYs) | Events | PYs | Rate (per 105 PYs) | Adjusted HR | 95% CI | 95% CI | P |
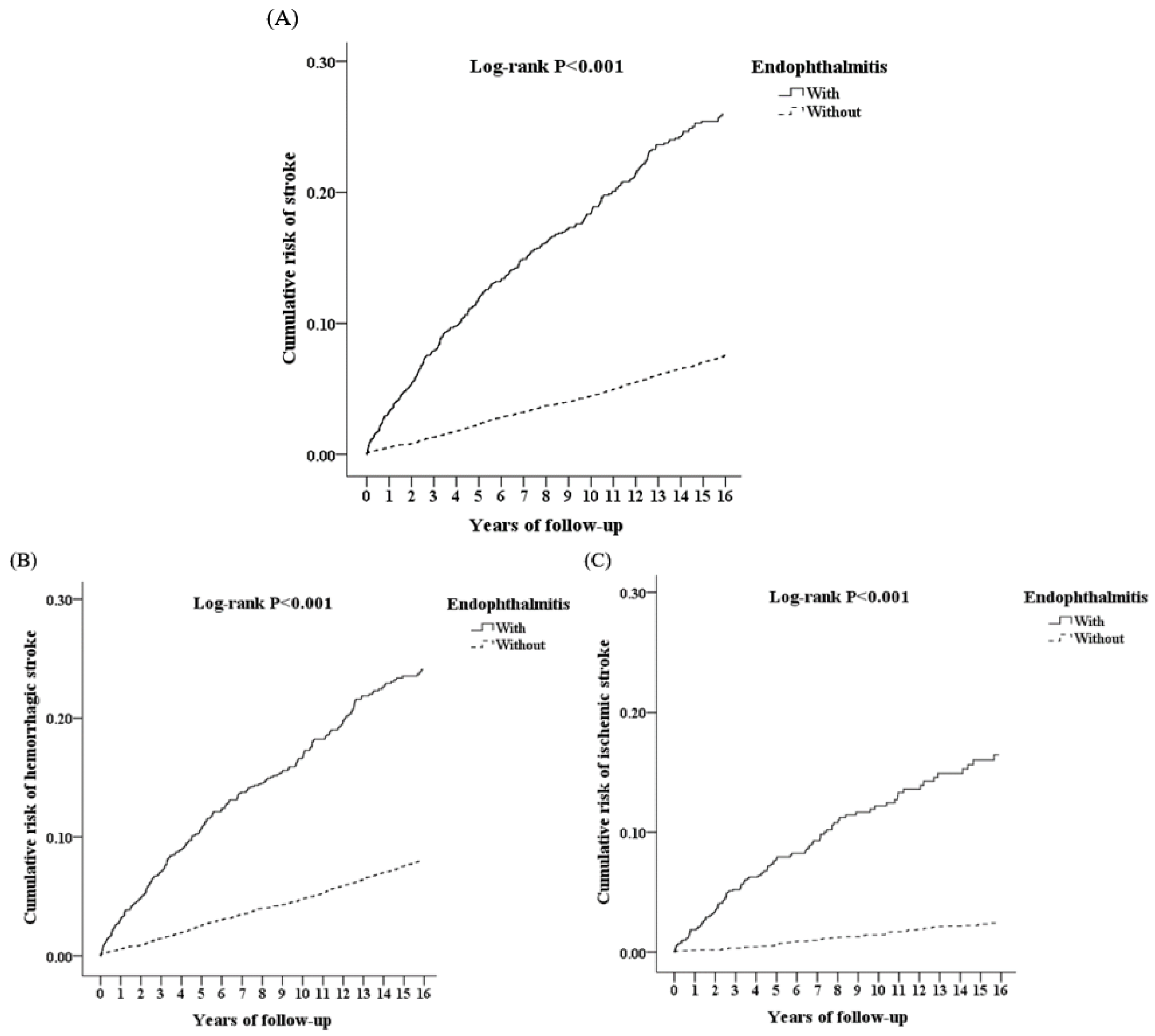
| Overall | 89 | 5170.5 | 1724.44 | 229 | 21,103.84 | 1085.11 | 1.873 | 1.776 | 2.022 | <0.001 |
| Hemorrhagic stroke | 47 | 5170.5 | 909.00 | 119 | 21,103.84 | 563.88 | 1.998 | 1.895 | 2.153 | <0.001 |
| Ischemic stroke | 42 | 5170.5 | 812.30 | 110 | 21,103.84 | 521.23 | 1.794 | 1.692 | 1.924 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, Y.-E.; Chien, W.-C.; Chen, Y.-H.; Chung, C.-H.; Chen, J.-T.; Chen, C.-L. Correlation between Endophthalmitis and Stroke Development in Ankylosing Spondylitis Patients: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 13108. https://doi.org/10.3390/ijerph192013108
Tsai Y-E, Chien W-C, Chen Y-H, Chung C-H, Chen J-T, Chen C-L. Correlation between Endophthalmitis and Stroke Development in Ankylosing Spondylitis Patients: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(20):13108. https://doi.org/10.3390/ijerph192013108
Chicago/Turabian StyleTsai, Yung-En, Wu-Chien Chien, Yi-Hao Chen, Chi-Hsiang Chung, Jiann-Torng Chen, and Ching-Long Chen. 2022. "Correlation between Endophthalmitis and Stroke Development in Ankylosing Spondylitis Patients: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 19, no. 20: 13108. https://doi.org/10.3390/ijerph192013108