

Two-Stage Gene Therapy (VEGF, HGF and ANG1 Plasmids) as Adjunctive Therapy in the Treatment of Critical Lower Limb Ischemia in Diabetic Foot Syndrome
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
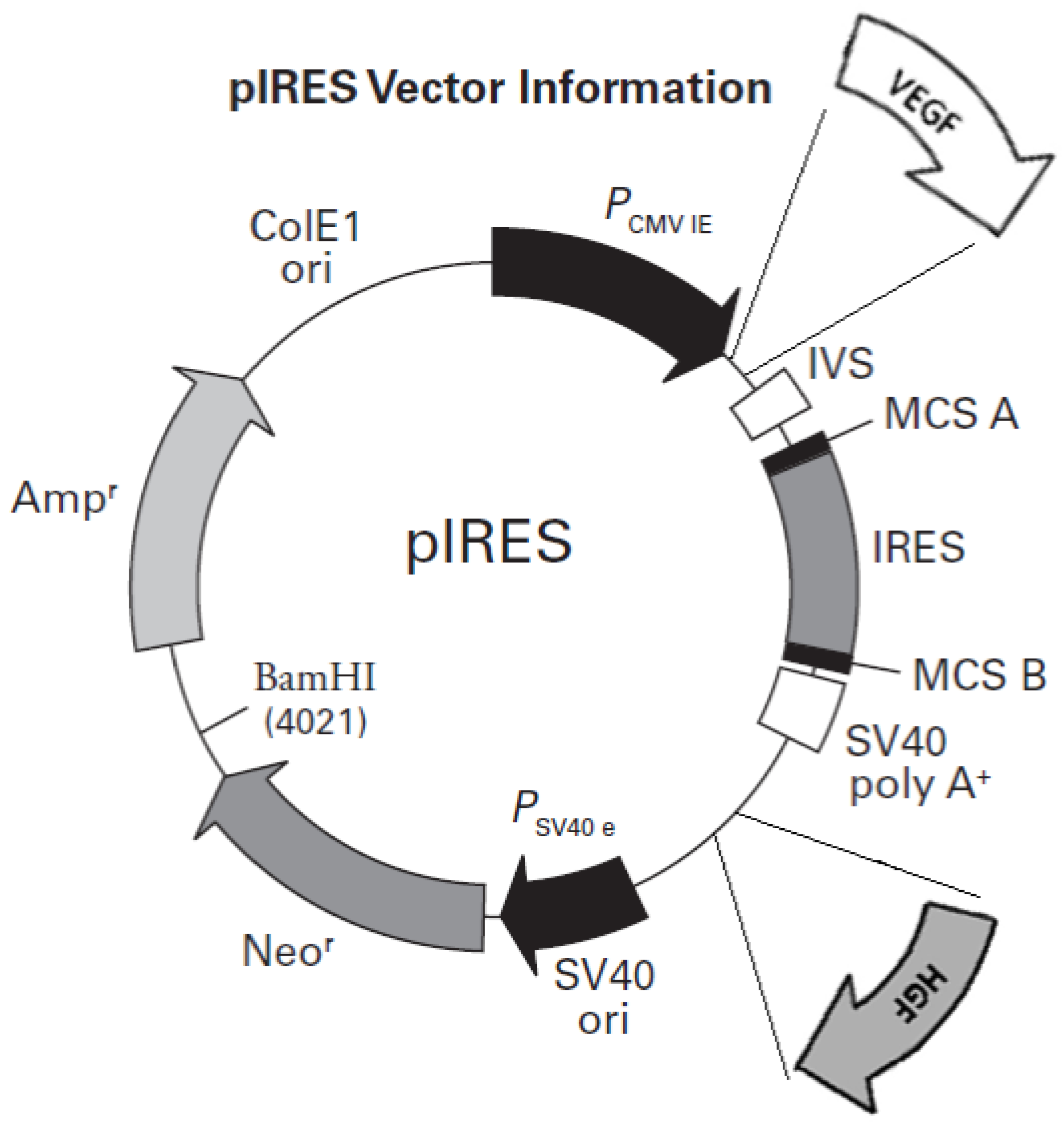
2.1. Preparation of Plasmid DNA
2.2. Patient Cohort
2.3. Administration of Plasmids
2.4. Clinical Evaluation
2.5. Ankle–Brachial Index (ABI)
2.6. Resting Pain
2.7. Transcutaneous Oxygen Pressure (TcPO2) Measurements
2.8. Statistical Analysis
3. Results
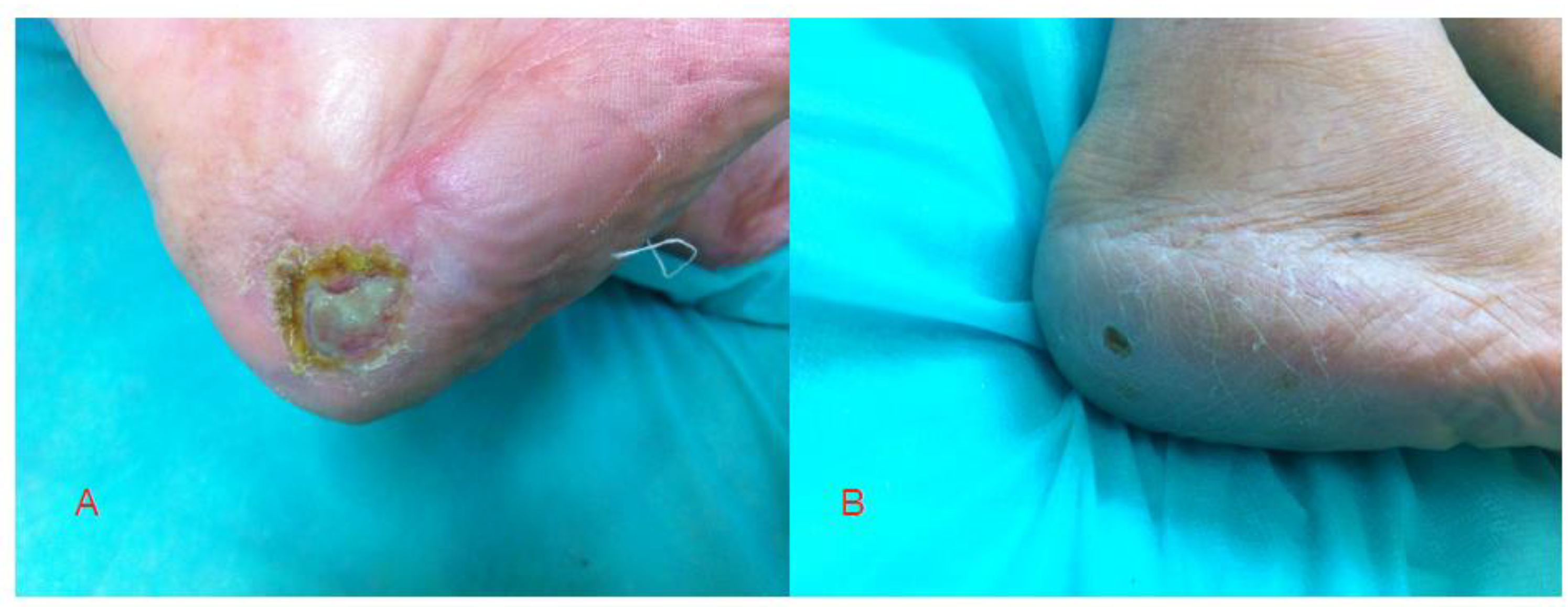
3.1. Clinical Follow-Up
3.2. ABI Results
3.3. PtcO2 Results
3.4. Resting Pain (VAS)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2021, 183, 109119. [Google Scholar] [CrossRef]
- Janeczko, D. Epidemiologia cukrzycy typu 2. In Cukrzyca T.1; Sieradzki, J., Ed.; Via Medica: Gdańsk, Poland, 2015; pp. 124–142. [Google Scholar]
- Singh, N.; Armstrong, D.G.; Lipsky, B.A. Preventing Foot Ulcers in Patients With Diabetes. JAMA 2005, 293, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, R.E.; Ahroni, J.H.; Boyko, E.J.; Stensel, V.L. Chronology and determinants of tissue repair in diabetic lower-extremity ulcers. Diabetes 1991, 40, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Lavery, L.; Ashry, H.R.; Van Houtum, W.; Pugh, J.A.; Harkless, L.B.; Basu, S. Variation in the Incidence and Proportion of Diabetes-Related Amputations in Minorities. Diabetes Care 1996, 19, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Siitonen, O.I.; Niskanen, L.K.; Laakso, M.; Siitonen, J.T. Lower-extremity amputations in diabetic and nondiabetic patients. A population-based study in eastern Finland. Diabetes Care 1993, 16, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Farber, A.; Eberhardt, R.T. The Current State of Critical Limb Ischemia: A Systematic Review. JAMA Surg. 2016, 151, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Freisinger, E.; Malyar, N.M.; Reinecke, H.; Lawall, H. Impact of diabetes on outcome in critical limb ischemia with tissue loss: A large-scaled routine data analysis. Cardiovasc. Diabetol. 2017, 16, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabiani, I.; Calogero, E.; Pugliese, N.R.; Di Stefano, R.; Nicastro, I.; Buttitta, F.; Nuti, M.; Violo, C.; Giannini, D.; Morgantini, A.; et al. Critical Limb Ischemia: A Practical Up-To-Date Review. Angiology 2017, 69, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Skóra, J.; Barć, P.; Pupka, A.; Dawiskiba, T.; Korta, K.; Albert, M.; Szyber, P. Transplantation of autologous bone marrow mononuclear cells with VEGF gene improves diabetic critical limb ischaemia. Endokrynol. Polska 2013, 64, 129–138. [Google Scholar]
- Sengupta, S.; Gherardi, E.; Sellers, L.A.; Wood, J.M.; Sasisekharan, R.; Fan, T.-P.D. Hepatocyte growth factor/scatter factor can induce angiogenesis independently of vascular endothelial growth factor. Arter. Thromb. Vasc. Biol. 2003, 23, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadakierska-Chudy, A.; Skóra, J.; Barć, P.; Baczyńska, D.; Kasprzykowska, U.; Pupka, A.; Ussowicz, M.; Szyber, P.; Dobosz, T. Angiogenic therapy for critical lower limb ischemia. Adv. Clin. Exp. Med. 2010, 19, 347–359. [Google Scholar]
- Barć, P.; Antkiewicz, M.; Śliwa, B.; Baczyńska, D.; Witkiewicz, W.; Skóra, J. Treatment of critical limb ischemia by pIRES/VEGF165/HGF administration. Ann.Vasc.Surg. 2019, 60, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Sadakierska-Chudy, A.; Baczyńska, D.; Skóra, J.P. Transfection Efficiency and Cytotoxicity of Transfection Reagents in Human Umbilical Vein Endothelial Cells. Adv. Clin. Exp. Med. 2008, 17, 625–634. [Google Scholar]
- Barc, P.; Płonek, T.; Baczyńska, D.; Pupka, A.; Witkiewicz, W.; Mastalerz-Migas, A.; Milnerowicz, A.; Antkiewicz, M.; Hałoń, A.; Skóra, J.P. Role of vascular endothelial growth factor in inducing production of angiopoetin-1—in vivo study in Fisher rats. Pol. J. Pathol. 2017, 68, 326–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skóra, J.P.; Płonek, T.; Barc, P.; Baczynska, D.; Radwanska, A.; Pupka, A.; Korta, K.; Ussowicz, M.; Strożecki, L.; Kupczyńska-Markiewicz, D.; et al. The Formation of Blood Vessel after the Administration of the Plasmid Encoding Ang-1 Gene in Fischer Rats. Adv. Clin. Exp. Med. 2016, 25, 611–615. [Google Scholar] [CrossRef] [Green Version]
- Rosengart, T.K.; Bishawi, M.M.; Halbreiner, M.S.; Fakhoury, M.; Finnin, E.; Hollmann, C.; Shroyer, A.L.; Crystal, R.G. Long-Term Follow-Up Assessment of a Phase 1 Trial of Angiogenic Gene Therapy Using Direct Intramyocardial Administration of an Adenoviral Vector Expressing the VEGF121 cDNA for the Treatment of Diffuse Coronary Artery Disease. Hum. Gene Ther. 2013, 24, 203–208. [Google Scholar] [CrossRef] [Green Version]
- Amann, B.; Luedemann, C.; Ratei, R.; Schmidt-Lucke, J.A. Autologous Bone Marrow Cell Transplantation Increases Leg Perfusion and Reduces Amputations in Patients with Advanced Critical Limb Ischemia Due to Peripheral Artery Disease. Cell Transplant. 2009, 18, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.G. Critical Limb Ischemia: Cell and Molecular Therapies for Limb Salvage. Methodist DeBakey Cardiovasc. J. 2012, 8, 20–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of Health, Poland. Available online: https://pacjent.gov.pl/artykul/cukrzyca-w-liczbach (accessed on 30 August 2022).
- Hedman, M.; Muona, K.; Hedman, A. Eight-year safety follow-up of coronary artery disease patients after local intracoronary VEGF gene transfer. Gene Ther. 2009, 16, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kastrup, J.; Jørgensen, E.; Rück, A.; Tägil, K.; Glogar, D.; Ruzyllo, W.; Bøtker, H.E.; Dudek, D.; Drvota, V.; Hesse, B.; et al. Direct intramyocardial plasmid vascular endothelial growth factor-A165gene therapy in patients with stable severe angina pectoris: A randomized double-blind placebo-controlled study: The Euroinject One trial. J. Am. Coll. Cardiol. 2005, 45, 982–988. [Google Scholar] [CrossRef] [Green Version]
- Carmeliet, P. Angiogenesis in health and disease. Nat. Med. 2003, 9, 653–660. [Google Scholar] [CrossRef]
- Inampudi, C.; Akintoye, E.; Ando, T.; Briasoulis, A. Angiogenesis in peripheral arterial disease. Curr. Opin. Pharmacol. 2018, 39, 60–67. [Google Scholar] [CrossRef]
- Muona, K.; Mäkinen, K.; Hedman, M.; Manninen, H.; Ylä-Herttuala, S. 10-year safety follow-up in patients with local VEGF gene transfer to ischemic lower limb. Gene Ther. 2011, 19, 392–395. [Google Scholar] [CrossRef]
- Ylä-Herttuala, S. Gene Therapy of Critical Limb Ischemia Enters Clinical Use. Mol. Ther. J. Am. Soc. Gene Ther. 2019, 27, 2053. [Google Scholar] [CrossRef]
- Suri, C.; McClain, J.; Thurston, G.; McDonald, D.M.; Zhou, H.; Oldmixon, E.H.; Sato, T.N.; Yancopoulos, G.D. Increased Vascularization in Mice Overexpressing Angiopoietin-1. Science 1998, 282, 468–471. [Google Scholar] [CrossRef]
- Thurston, G.; Suri, C.; Smith, K.; McClain, J.; Sato, T.N.; Yancopoulos, G.D.; McDonald, D.M. Leakage-Resistant Blood Vessels in Mice Transgenically Overexpressing Angiopoietin-1. Science 1999, 286, 2511–2514. [Google Scholar] [CrossRef]
- Thurston, G.; Rudge, J.S.; Ioffe, E.; Zhou, H.; Ross, L.; Croll, S.; Glazer, N.; Holash, J.; McDonald, D.M.; Yancopoulos, G.D. Angiopoietin-1 protects the adult vasculature against plasma leakage. Nat. Med. 2000, 6, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, N. Role of vascular endothelial growth factor in the regulation of angiogenesis. Kidney Int. 1999, 56, 794–814. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, N.; Davis-Smyth, T. The biology of vascular endothelial growth factor. Endocr. Rev. 1997, 18, 4–25. [Google Scholar] [CrossRef]
- FTanaka, F.; Ishikawa, S.; Yanagihara, K.; Miyahara, R.; Kawano, Y.; Li, M.; Otake, Y.; Wada, H. Expression of angiopoietins and its clinical significance in non-small cell lung cancer. Cancer Res. 2002, 62, 7124–7129. [Google Scholar]
- Fagiani, E.; Christofori, G. Angiopoietins in angiogenesis. Cancer Lett. 2013, 328, 18–26. [Google Scholar] [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Before Treatment (±SD) | After 3 Months (±SD) | p-Value | ||
|---|---|---|---|---|
| Wound classification (cm) | Group 1 | 1.80 ± 0.42 | 1.40 ± 0.52 | 0.037 * |
| Group 2 (control) | 1.78 ± 0.44 | 1.67 ± 0.50 | 0.347 | |
| ABI | Group 1 | 0.44 ± 0.14 | 0.47 ± 0.12 | 0.028 * |
| Group 2 (control) | 0.46 ± 0.18 | 0.49 ± 0.17 | 0.175 | |
| PtcO2 (mmHg) | Group 1 | 26.90 ± 8.99 | 33.9 ± 6.33 | 0.001 * |
| Group 2 (control) | 28.71 ± 10.89 | 32.0 ± 8.81 | 0.058 | |
| VAS | Group 1 | 6.80 ± 1.48 | 2.10 ± 1.10 | <0.001 * |
| Group 2 (control) | 7.44 ± 1.42 | 3.78 ± 1.64 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barć, P.; Antkiewicz, M.; Frączkowska-Sioma, K.; Kupczyńska, D.; Lubieniecki, P.; Witkiewicz, W.; Małodobra-Mazur, M.; Baczyńska, D.; Janczak, D.; Skóra, J.P. Two-Stage Gene Therapy (VEGF, HGF and ANG1 Plasmids) as Adjunctive Therapy in the Treatment of Critical Lower Limb Ischemia in Diabetic Foot Syndrome. Int. J. Environ. Res. Public Health 2022, 19, 12818. https://doi.org/10.3390/ijerph191912818
Barć P, Antkiewicz M, Frączkowska-Sioma K, Kupczyńska D, Lubieniecki P, Witkiewicz W, Małodobra-Mazur M, Baczyńska D, Janczak D, Skóra JP. Two-Stage Gene Therapy (VEGF, HGF and ANG1 Plasmids) as Adjunctive Therapy in the Treatment of Critical Lower Limb Ischemia in Diabetic Foot Syndrome. International Journal of Environmental Research and Public Health. 2022; 19(19):12818. https://doi.org/10.3390/ijerph191912818
Chicago/Turabian StyleBarć, Piotr, Maciej Antkiewicz, Katarzyna Frączkowska-Sioma, Diana Kupczyńska, Paweł Lubieniecki, Wojciech Witkiewicz, Małgorzata Małodobra-Mazur, Dagmara Baczyńska, Dariusz Janczak, and Jan Paweł Skóra. 2022. "Two-Stage Gene Therapy (VEGF, HGF and ANG1 Plasmids) as Adjunctive Therapy in the Treatment of Critical Lower Limb Ischemia in Diabetic Foot Syndrome" International Journal of Environmental Research and Public Health 19, no. 19: 12818. https://doi.org/10.3390/ijerph191912818