

The Use of the ICF Classification Sheet to Assess Cognitive-Behavioral Disorders and Verbal Communication in Patients after Ischemic and Hemorrhagic Stroke during Rehabilitation
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group/Inclusion and Exclusion Criteria
- Restoring executive functions (e.g., day planning training, the chronology of proceedings, supervision over the implementation of daily duties).
- Training of memory processes (e.g., short-term memory in the verbal and visual modality and long-term memory in information encoding and decoding).
- Attention processes training (focusing attention on one indicated stimulus and shifting and dividing attention between several stimuli).
2.2. Cognitive-Behavioral Disorders
2.3. Verbal Communication Disorders
2.4. ICF Profile
2.4.1. ICF Categories of Cognitive Behavioral Disorders
2.4.2. ICF Categories of Verbal Communication Disorders
2.5. Statistical Analysis
3. Results
3.1. Study Groups
3.2. Cognitive Behavioral Disorders
3.3. Verbal Communication Disorders
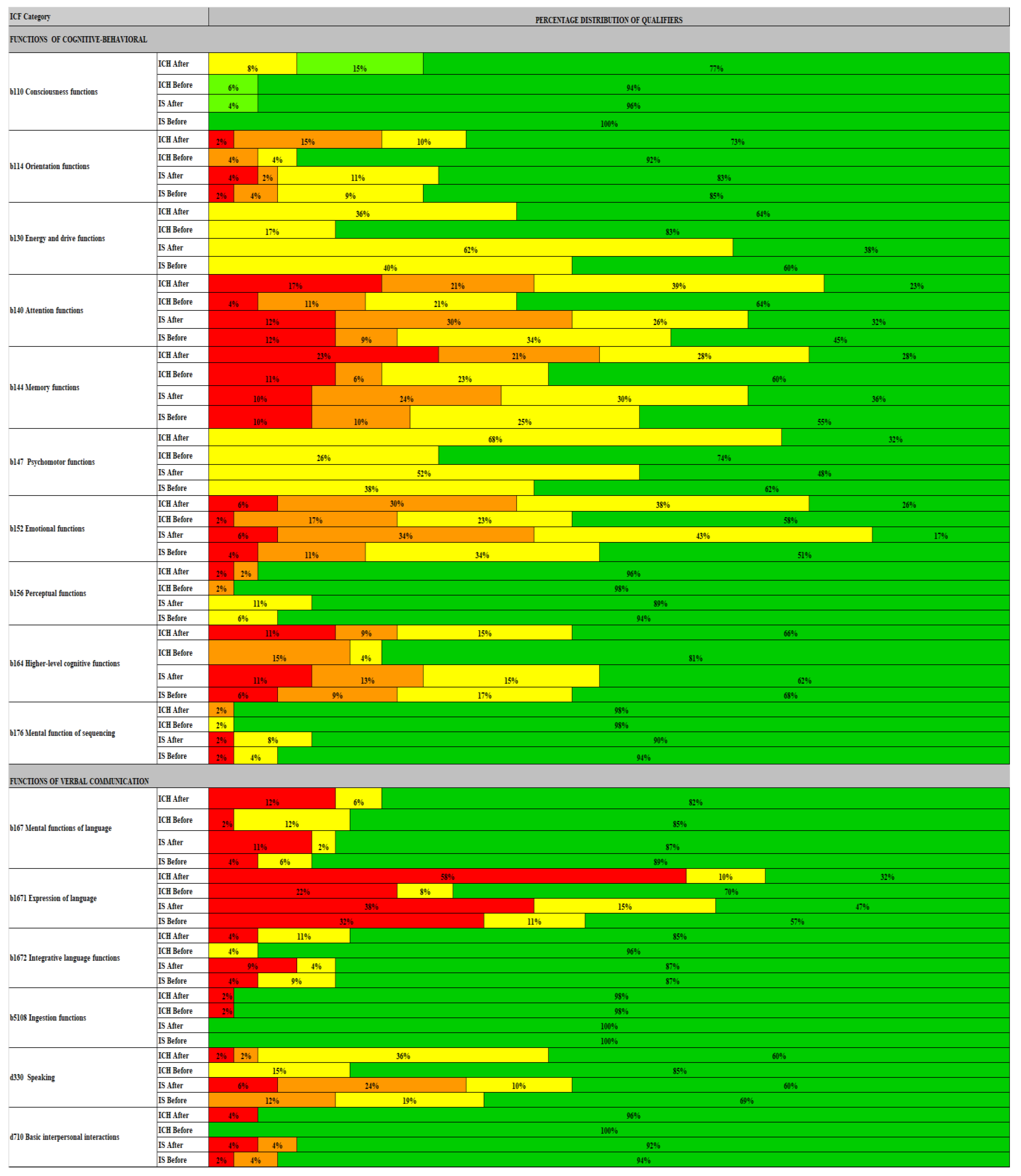
3.4. Profile of Cognitive and Speech Therapy Disorders According to the ICF Classification Categories
3.4.1. ICH
3.4.2. IS
3.4.3. ICH vs. IS
4. Discussion
5. Conclusions
- (1).
- The type of stroke suffered determines the frequency and type of cognitive-behavioral and verbal communication disorders.
- (2).
- The ICF classification can be used to assess the occurrence of psychological and speech therapy disorders depending on the clinical type of stroke.
- (3).
- Using one tool during rehabilitation containing a description of cognitive-behavioral disorders as well as verbal communication in the form of an ICF sheet may improve communication between a speech therapist and a psychologist, which in turn may lead to an increase in the effectiveness of the therapy.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eurostat. Causes of Death in 2013, Pressrelease, 91/2016–4 May 2016. Available online: https://ec.europa.eu/eurostat/documents/2995521/7247552/3-04052016-BP-EN.pdf/fd9d9755-e9d0-4389-a0e8-8fa879efa375 (accessed on 31 July 2016).
- Swarowska, M.; Burkot, J.; Janowska, A.; Klimkowicz-Mrowiec, A.; Pera, J.; Slowik, A.; Dziedzic, T. Improvement of survival in Polish stroke patients is related to reduced stroke severity and better control of risk Factors: The Krakow Stroke Database. Arch. Med. Sci. 2016, 12, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Godefroy, O.; Fickl, A.; Roussel, M.; Auribault, C.; Bugnicourt, J.M.; Lamy, C.; Canaple, S.; Petitnicolas, G. Is the Montreal Cognitive Assessment superior to the Mini-Mental State Examination to detect poststrokecognitive impairment? A study with neuropsychological evaluation. Stroke 2011, 42, 1712–1716. [Google Scholar] [PubMed]
- Cicerone, K.D.; Langenbahn, M.; Braden, C.; Malec, J.F.; Kalmar, K.; Fraas, M.; Felicetti, T.; Laatsch, L.; Harley, J.P.; Bergquist, T.; et al. Evidence-based cognitive rehabilitation: Updated review of the literature from 2003 through 2008. Arch. Phys. Med. Rehabil. 2011, 92, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Pater, M.; Coshall, C.; Rudd, A.G.; Wolfe, C.D.A. Natural history of cognitive impairment after stroke and factors associated with its recovery. Clin. Rehabil. 2003, 17, 158–166. [Google Scholar]
- Rost, N.S.; Brodtmann, A.; Pase, M.P.; van Veluw, S.J.; Biffi, A.; Duering, M.; Hinman, J.D.; Dichgans, M. Post-Stroke Cognitive Impairment and Dementia. Circ. Res. 2022, 130, 1252–1271. [Google Scholar] [CrossRef] [PubMed]
- Dromerick, A.; Reding, M. Medical and neurological complications during inpatient stroke rehabilitation. Stroke 1994, 25, 358–361. [Google Scholar] [CrossRef]
- Bhogal, S.K.; Teasell, R.; Speechley, M. Intensity of aphasia therapy, impact on recovery. Stroke 2003, 34, 987–993. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Diseases (ICD-10). Available online: http://www.who.int/classifications/icd/en/ (accessed on 1 January 2020).
- De Haan, R.; Horn, J.; Limburg, M.; Van Der Meulen, J.; Bossuyt, P. A comparison of five stroke scales with measures of disability, handicap, and quality of life. Stroke 1993, 24, 178–181. [Google Scholar] [CrossRef]
- Brola, W.; Czernicki, J. Porównanie skal uszkodzenia stosowanych w ocenie pacjentów po udarze mózgu. Postępy Rehabil. 1999, 13, 37–43. [Google Scholar]
- Prodinger, B.; Stucki, G.; Coenen, M.; Tennant, A. The measurement of functioning using the International Classification of Functioning, Disability and Health: Comparing qualifier ratings with existing health status instruments. Disabil. Rehabil. 2017, 1–8. [Google Scholar] [CrossRef]
- Silva, S.M.; Corrêa, F.I.; Faria, C.D.; Buchalla, C.M.; Silva, P.F.; Corrêa, J.C. Evaluation of post-stroke functionality based on the International Classification of Functioning, Disability, and Health: A proposal for use of assessment tools. J. Phys. Ther. Sci. 2015, 27, 1665–1670. [Google Scholar] [CrossRef] [PubMed]
- Algurén, B.; Lundgren-Nilsson, A.; Sunnerhagen, K.S. Functioning of stroke survivors—A validation of the ICF core set for stroke in Sweden. Disabil. Rehabil. 2010, 32, 551–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonsdottir, J.; Bowman, T.; Casiraghi, A.; Ramella, M.; Montesano, A.; IRCCS FDG-ICF Group. Functional profiles derived from the ICF Generic set and the responsiveness and validity of the Generic-6 set’s Functioning score among persons after stroke. Eur. J. Phys. Rehabil. Med. 2022, 58, 16–25. [Google Scholar] [CrossRef]
- Yamada, Y.; Metoki, N.; Yoshida, H.; Satoh, K.; Ichihara, S.; Kato, K.; Kameyama, T.; Yokoi, K.; Matsuo, H.; Segawa, T.; et al. Genetic Risk for Ischemic and Hemorrhagic Stroke. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 1920–1925. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chapman, A.M.; Plested, M.; Jackson, D.; Purroy, F. The Incidence, Prevalence, and Mortality of Stroke in France, Germany, Italy, Spain, the UK and the US: A Literature Review. Stroke Res. Treat. 2012, 2012, 436125. [Google Scholar] [CrossRef] [PubMed]
- Perin, C.; Bolis, M.; Limonta, M.; Meroni, R.; Ostasiewicz, K.; Cornaggia, C.M.; Alouche, S.R.; da Silva Matuti, G.; Cerri, C.G.; Piscitelli, D. Differences in Rehabilitation Needs after Stroke: A Similarity Analysis on the ICF Core Set for Stroke. Int. J. Environ. Res. Public Health 2020, 17, 4291. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Lee, K.B.; Roh, H.; Ahn, M.Y.; Hwang, H.W. Gender differences in the functional recovery after acute stroke. J. Clin. Neurol. 2010, 6, 183–188. [Google Scholar] [CrossRef]
- Lai, S.M.; Duncan, P.W.; Dew, P.; Keighley, J. Sex differences in stroke recovery. Prev. Chronic Dis. 2005, 2, A13. [Google Scholar]
- MacDonald, S.L.; Hall, R.E.; Bell, C.M.; Cronin, S.; Jaglal, S.B. Sex differences in the outcomes of adults admitted to inpatient rehabilitation after stroke. PM&R 2021, 14, 779–785. [Google Scholar]
- Kwakkel, G. Impact of intensity of practice after stroke: Issues for consideration. Disabil. Rehabil. 2006, 28, 823–830. [Google Scholar] [CrossRef]
- Chae, J.; Zorowitz, R.D.; Johnston, M.V. Functional outcome of hemorrhagic and nonhemorrhagic stroke patients after in-patient rehabilitation. Am. J. Phys. Med. Rehabil. 1996, 75, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, S. Functional outcome of ischemic and hemorrhagic stroke patients after inpatient rehabilitation: A matched comparison. Stroke 2003, 34, 2861–2865. [Google Scholar] [CrossRef] [PubMed]
- O’Donoghue, M.; Leahy, S.; Boland, P.; Galvin, R.; McManus, J.; Hayes, S. Rehabilitation of Cognitive Deficits Poststroke: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Stroke 2022, 53, 1700–1710. [Google Scholar] [CrossRef] [PubMed]
- Hurford, R.; Charidimou, A.; Fox, Z.; Cipolotti, L.; Werring, D.J. Domain-specific trends in cognitive impairment after acute ischaemic stroke. J. Neurol. 2013, 260, 237–241. [Google Scholar] [CrossRef]
- Cumming, T.B.; Marshall, R.S.; Lazar, R.M. Stroke, cognitive deficits, and rehabilitation: Still an incomplete picture. Int. J. Stroke 2013, 8, 38–45. [Google Scholar] [CrossRef]
- Rasquin, S.M.; Verhey, F.; Lousberg, R.; Lodder, J. Cognitive performance after first ever stroke related to progression of vascular brain damage; a 2 year follow up CT scan study. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1075–1079. [Google Scholar] [CrossRef]
- Narasimahalu, K.; Ang, S.; De Silva, D.A.; Wong, M.C.; Chang, H.M.; Chia, K.S.; Auchus, A.P.; Chen, C.P. The prognostic effects of post stroke cognitive impairment no dementia and domain-specific cognitive impairments in nondisabled ischemic stroke patients. Stroke 2011, 42, 833–838. [Google Scholar]
- Ruchinskas, R.; Curyto, K. Cognitive screening in geriatric rehabilitation. Rehabil. Psychol. 2003, 48, 14–22. [Google Scholar] [CrossRef]
- Brodaty, H.; Withall, A.; Altendorf, A.; Sachdev, P.S. Rates of depression at 3 and 15 months post stroke and their relationship with cognitive decline: The Sydney Stroke Study. Am. J. Geriatr. Psychiatry 2007, 15, 477–486. [Google Scholar] [CrossRef]
- Srikanth, V.K.; Thrift, A.G.; Saling, M.M.; Anderson, J.F.; Dewey, H.M.; Macdonell, R.A.; Donnan, G.A. Increased risk of cognitive impairment 3 months after mild to moderate first-ever stroke: A community-based prospective study of nonaphasic English-speaking survivors. Stroke 2003, 34, 1136–1143. [Google Scholar] [CrossRef]
- Kinoshita, S.; Abo, M.; Okamoto, T.; Kakuda, W.; Miyamura, K.; Kimura, I. Responsiveness of the functioning and disability parts of the International Classification of Functioning, Disability, and Health core sets in postacute stroke patients. Int. J. Rehabil. Res. 2017, 40, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Bickenbach, J.; Cieza, S.; Rauch, S.; Stucki, G. ICF Core Sets Manual for Clinical Practice; Hogrefe: Göttingen, Germany, 2012. [Google Scholar]
- Ewert, T.; Allen, D.D.; Wilson, M.; Ustün, B.; Stucki, G. Validation of the International Classification of Functioning Disability and Health framework using multidimensional item response modeling. Disabil. Rehabil. 2010, 32, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Ewert, T.; Usturn, T.B.; Chatterji, S.; Konstanjsek, N.; Strucki, G. Development of ICF Core Sets for patients with chronic Condition. J. Rehabil. Med. 2004, 44, 9–11. [Google Scholar]
- McIntyre, A.; Tempest, S. Two steps forward, one step back? A commentary on the disease-specific core sets of the International Classification of Functioning, Disability and Health (ICF). Disabil. Rehabil. 2007, 29, 1475–1479. [Google Scholar] [CrossRef]
- Wong, A.; Lau, S.C.; Fong, M.W.; Cella, D.; Lai, J.S.; Heinemann, A.W. Conceptual Underpinnings of the Quality of Life in Neurological Disorders (Neuro QoL): Comparisons of Core Sets for Stroke, Multiple Sclerosis, Spinal Cord Injury, and Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2018, 99, 1763–1775. [Google Scholar] [CrossRef]
- Kohler, F.; Selb, M.; Escorpizo, R.; Kostanjsek, N.; Stucki, G.; Riberto, M. International Society of Physical and Rehabilitation Medicine, Sub-Committee Implementation of the ICF Practipications of the Sao Paulo. J. Rehabil. Med. 2012, 10, 805–810. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| ICH | IS | p | ||
|---|---|---|---|---|
| Sex n (%) | Females | 20 (42.6%) | 30 (63.8%) | 0.039 a |
| Males | 27 (57.4%) | 17 (36.2%) | ||
| Age (years) | Mean ± SD | 67.3 ± 10.6 | 71.7 ± 9.81 | 0.038 b |
| Median | 66 | 70 | ||
| Min–Max | 49–92 | 51–92 | ||
| Time from stroke to rehabilitation (days) | Mean ± SD | 33.5 ± 17.7 | 18.0 ± 8.6 | <0.001 b |
| Median | 29 | 16 | ||
| Duration of rehabilitation (days) | Mean ± SD | 69.1 ± 32.2 | 59.0 ± 34.9 | 0.118 b |
| Median | 63 | 51 | ||
| NIHSS before rehabilitation | Mean ± SD | 13 ± 5 | 12 ± 4 | 0.847 b |
| Median | 12 | 12 | ||
| Min–Max | 5–24 | 6–24 | ||
| NIHSS after rehabilitation | Mean ± SD | 5 ± 5 | 9 ± 4 | <0.001 b |
| Median | 5 | 8 | ||
| Min–Max | 0–17 | 4–22 | ||
| ICF Category | Qualifier Criteria | ICH | IS | ICH vs. IS | |||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | p | Before | After | p | Before | After | ||
| b110 Consciousness functions | 0—full consciousness | 36 (76.6%) | 44 (93.6%) | 0.005 | 45 (95.7%) | 47 (100.0%) | 1.0 | 0.007 | 0.784 |
| 1—sleepy | 7 (14.9%) | 3 (6.4%) | 2 (4.3%) | 0 (0%) | |||||
| 2—not fully conscious | 4 (8.5%) | 0 (0%) | 0 (0%) | 0 (0%) | |||||
| 3—unconscious | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | |||||
| b114 Orientation functions | 0—full orientation as to time and place preserved | 34 (72.3%) | 43 (91.5%) | 0.002 | 39 (83.0%) | 40 (85.1%) | 0.180 | 0.201 | 0.343 |
| 1—orientation to place and time preserved | 5 (10.6%) | 2(4.3%) | 5 (10.6%) | 4 (8.5%) | |||||
| 2—lack of full orientation as to the place or time | 7 (14.9%) | 2 (4.3%) | 1 (2.1%) | 2 (4.3%) | |||||
| 3—complete disorientation as to place and time | 1 (2.1%) | - | 2 (4.3%) | 1 (2.1%) | |||||
| b130 Energy and drive functions | 0—no mood disorders | 17 (36.2%) | 39 (83.0%) | <0.001 | 18 (38.3%) | 28 (59.6%) | 0.009 | 0.831 | 0.007 |
| 1—depressed mood | 30 (63.8%) | 8 (17.0%) | 29 (61.7%) | 19 (40.4%) | |||||
| b140 Attention functions | 0—no disturbances in attention systems | 11 (23.4%) | 30 (63.8%) | <0.001 | 15(31.9%) | 21 (44.7%) | 0.002 | 0.71 | 0.071 |
| 1—slight attention disorders | 18 (38.3%) | 10 (21.3%) | 12 (25.5%) | 16 (34.0%) | |||||
| 2—moderate attention disorders | 10 (21.3%) | 5 (10.6%) | 14 (29.8%) | 4 (8.5%) | |||||
| 3-severe attention disorders | 8 (17.0%) | 2 (4.3%) | 6 (12.8%) | 6 (12.8%) | |||||
| b144 Memory functions | 0—no memory impairment | 13 (27.7%) | 28 (59.6%) | <0.001 | 17 (36.2%) | 26 (55.3%) | 0.005 | 0.177 | 0.656 |
| 1—mild memory impairment | 13 (27.7%) | 11 (23.4%) | 14 (29.8%) | 11 (23.4%) | |||||
| 2—moderate memory impairment | 10 (21.3%) | 3 (6.4%) | 11 (23.4%) | 5 (10.6%) | |||||
| 3—severe memory impairment | 11 (23.4%) | 5 (10.6%) | 5 (10.6%) | 5 (10.6%) | |||||
| b147 Psychomotor functions | 0—no psychomotor slowing down | 15 (31.9%) | 35 (74.5%) | <0.001 | 23 (48.9%) | 29 (61.7%) | 0.074 | 0.06 | 0.184 |
| 1—psychomotor slowing down | 32 (68.1) | 12 (25.5%) | 24(51.06%) | 18 (38.30%) | |||||
| b152 Emotional functions | 0—no emotional disturbances | 12 (25.5%) | 27 (57.4%) | 0.003 | 8 (17%) | 24 (51.1%) | <0.001 | 0.464 | 0.725 |
| 1—slight emotional disturbances | 18 (38.3%) | 11 (23.4%) | 20 (42.6%) | 16 (34.0%) | |||||
| 2—moderate emotional disturbances | 14 (29.8%) | 8 (17%) | 16 (34.0%) | 5 (10.6%) | |||||
| 3—severe emotional disturbances | 3 (6.4%) | 1 (2.1%) | 3 (6.4%) | 2 (4.3%) | |||||
| b156 Perceptual functions | 0—no agnosia | 45 (95.7%) | 46 (97.9%) | 0.18 | 42 (89.4%) | 44 (93.6%) | 0.18 | 0.281 | 0.331 |
| 1—light agnosia | 0 (0%) | 0 (0%) | 5 (10.6%) | 3 (6.4%) | |||||
| 2—moderate agnosia | 1 (2.1%) | 1 (2.1%) | 0 (0%) | 0 (0%) | |||||
| 3—severe agnosia | 1 (2.1%) | 0 (0%) | 0 (0%) | 0 (0%) | |||||
| b164 Higher-level cognitive functions | 0—no disorders of the executive systems | 31 (66.0%) | 38 (80.9%) | 0.013 | 29 (61.7%) | 32 (68.1%) | 0.066 | 0.669 | 0.198 |
| 1—slight disorders of the executive systems | 7 (14.9%) | 2 (4.3%) | 7 (14.9%) | 8 (17.0%) | |||||
| 2—moderate disorders of the executive systems | 4 (8.5%) | 7 (14.9%) | 6 (12.8%) | 4 (8.5%) | |||||
| 3—moderate disorders of the executive systems | 5 (10.6%) | 0 (0%) | 5 (10.6%) | 3 (6.4%) | |||||
| b176 Mental function of sequencing complex movements | 0—no apraxia | 46 (97.9%) | 46 (97.9%) | 1 | 42 (89.4%) | 44 (93.6%) | 0.583 | 0.101 | 0.309 |
| 1—slight apraxia | 0 (0%) | 1 (2.1%) | 4 (8.5%) | 2 (4.3%) | |||||
| 2—moderate apraxia | 1 (2.1%) | 0 (0%) | 0 (0%) | 0 (0%) | |||||
| 3—severe apraxia | 0 (0%) | 0 (0%) | 1 (2.1%) | 1 (2.1%) | |||||
| ICF Category | Qualifier Criteria | ICH | IS | ICH vs. IS | |||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | p | Before | After | p | Before | After | ||
| b167 Mental functions of language | 0—linguistic functions preserved | 38 (80.9%) | 40 (85.1%) | 0.018 | 41 (87.2%) | 42 (89.4%) | 0.068 | 0.432 | 0.579 |
| 1—partially impaired language functions | 3 (6.4%) | 6 (12.8%) | 1 (2.1%) | 3 (6.4%) | |||||
| 2—completely impaired linguistic functions | 6 (12.8%) | 1 (2.1%) | 5 (10.6%) | 2 (4.3%) | |||||
| b1671 Expression of language | 0—no speech disorders | 15 (31.9%) | 33 (70.2%) | <0.001 | 22 (46.8%) | 27 (57.4%) | 0.028 | 0.075 | 0.193 |
| 1—blurred speech | 5 (10.6%) | 4 (8.5%) | 7 (14.9%) | 5 (10.6%) | |||||
| 2—dysarthric speech | 27 (57.4%) | 10 (21.3%) | 18 (38.3%) | 15 (31.9%) | |||||
| b1672 Integrative language functions | 0—no aphasia | 40 (85.1%) | 45 (95.7%) | 0.003 | 41 (87.2%) | 41 (87.2%) | 0.012 | 0.845 | 0.133 |
| 1—sensory or motor aphasia | 5 (10.6%) | 2 (4.3%) | 2 (4.3%) | 4 (8.5%) | |||||
| 2—sensory and motor aphasia | 2 (4.3%) | 0 (0%) | 4 (8.5%) | 2 (4.3%) | |||||
| b5108 Ingestion functions. other specified | 0—no dysphagia | 46 (97.9%) | 46 (97.9%) | 1 | 47(100.0%) | 47(100.0%) | 1 | 0.859 | 0.860 |
| 1—dysphagia | 1 (2.1%) | 1 (2.1%) | 0 (0%) | 0 (0%) | |||||
| d330 Speaking | 0—no word choice disorders | 28 (59.6%) | 40 (85.1%) | 0.001 | 28 (59.6%) | 32 (68.1%) | 0.001 | 0.347 | 0.033 |
| 1—inadequate. limited word choice | 17 (36.2%) | 7 (14.9%) | 5 (10.6%) | 9 (19.1%) | |||||
| 2—no sentence formulation | 1 (2.1%) | 0 (0%) | 11 (23.4%) | 6 (12.8%) | |||||
| 3—no speech. making sounds | 1 (2.1%) | 0 (0)%) | 3 (6.4%) | 0 (0%) | |||||
| d710 Basic interpersonal interactions | 0—preserved | 45 (95.7%) | 47 (100%) | 0.180 | 43 (91.5%) | 44 (93.6%) | 0.5 | 0.427 | 0.082 |
| 1—moderately disturbed | 0 (0%) | 0 (0%) | 2 (4.3%) | 2 (4.3%) | |||||
| 2—completely disturbed | 2 (4.3%) | 0 (0%) | 2 (4.3%) | 1 (2.1%) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucka, E.; Lucki, M.; Cybulski, M.; Daroszewski, P.; Lisiński, P. The Use of the ICF Classification Sheet to Assess Cognitive-Behavioral Disorders and Verbal Communication in Patients after Ischemic and Hemorrhagic Stroke during Rehabilitation. Int. J. Environ. Res. Public Health 2022, 19, 12127. https://doi.org/10.3390/ijerph191912127
Lucka E, Lucki M, Cybulski M, Daroszewski P, Lisiński P. The Use of the ICF Classification Sheet to Assess Cognitive-Behavioral Disorders and Verbal Communication in Patients after Ischemic and Hemorrhagic Stroke during Rehabilitation. International Journal of Environmental Research and Public Health. 2022; 19(19):12127. https://doi.org/10.3390/ijerph191912127
Chicago/Turabian StyleLucka, Ewa, Mateusz Lucki, Marcin Cybulski, Przemysław Daroszewski, and Przemysław Lisiński. 2022. "The Use of the ICF Classification Sheet to Assess Cognitive-Behavioral Disorders and Verbal Communication in Patients after Ischemic and Hemorrhagic Stroke during Rehabilitation" International Journal of Environmental Research and Public Health 19, no. 19: 12127. https://doi.org/10.3390/ijerph191912127