

Effects of Cardiovascular Disease Risk Factors, Musculoskeletal Health, and Physical Fitness on Occupational Performance in Firefighters—A Systematic Review and Meta-Analysis
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Summary of Methods
2.2. Search Strategy for Identification of Studies
2.3. Electronic Literature Search
2.4. Additional Searches for Grey Literature
2.5. Selection of Studies
2.6. Data Extraction and Data Management
2.6.1. Critical Appraisal of Included Studies
2.6.2. Classification of Age and Obesity and Physical Fitness for Meta-Analysis
2.7. Data Analysis
2.7.1. Assessment of Overall Effect Size
2.7.2. Assessment of Heterogeneity
2.7.3. Subgroup Analysis and Investigation of Heterogeneity
3. Results
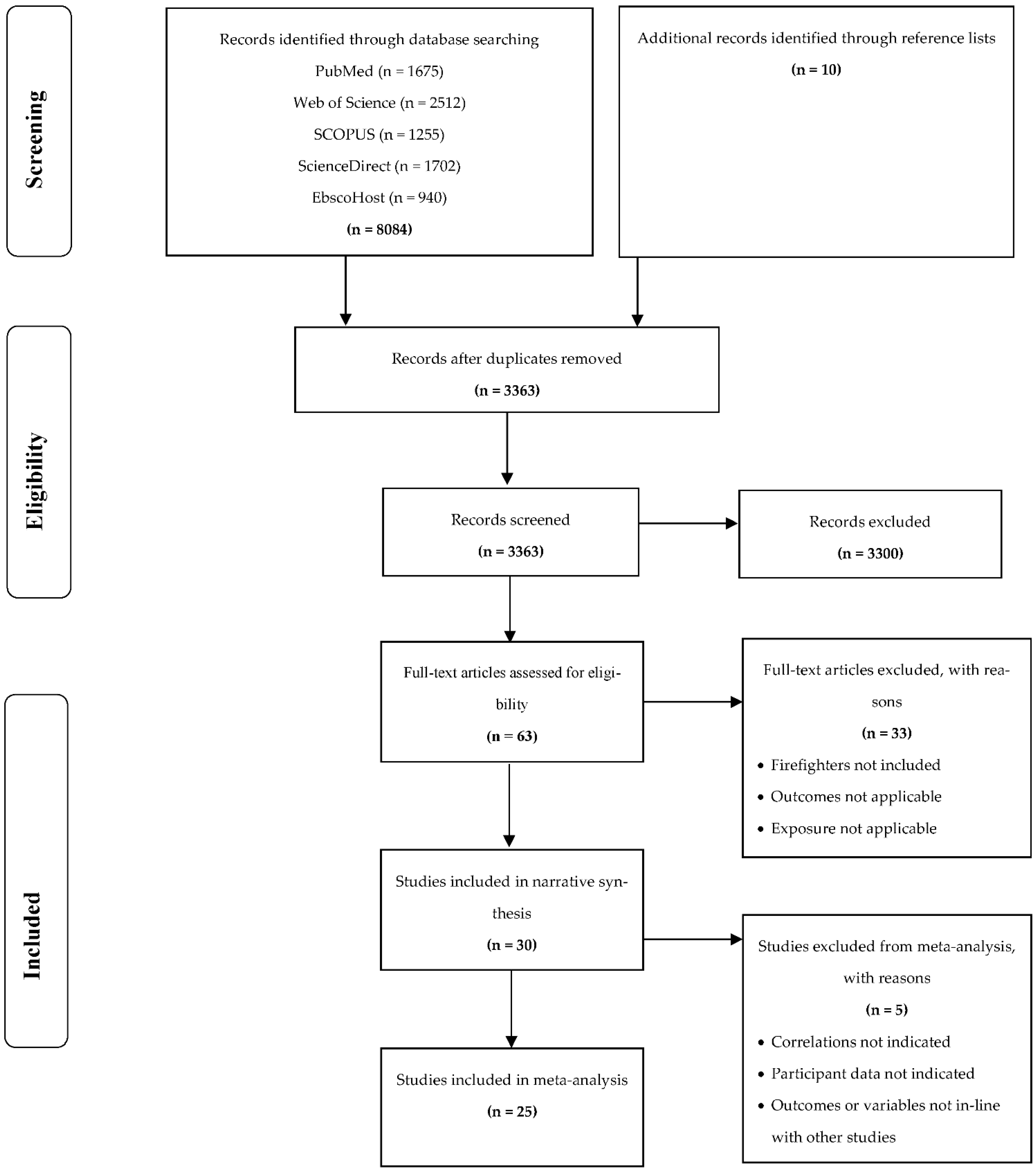
3.1. Study Selection
3.2. Assessment of the Strengths and Weaknesses of Studies
3.3. Study Characteristics
3.4. Cardiovascular Disease Risk Factors, Musculoskeletal Health and Occupational Performance
3.5. Physical Fitness and Occupational Performance in Firefighters

{kind=link}
{kind=link}
{kind=link}
| References | Study Design, Setting and Sample | Sample | Participant Information and Physical Fitness Measures | Occupational Performance Measures | Testing Procedure Details | Outcome |
|---|---|---|---|---|---|---|
| Chizewski et al. [66] | Cross-sectional study USA, Midwestern states | 89 male firefighter recruits | Age: 26.8 ± 4.2 years Body mass: 89.24 ± 16.33 kgs Height: 1.78 ± 0.07 m BMI: 28.11 ± 4.19 kg·m−2 1.5 Mile Run, push-ups, sit-ups bench press, flexibility, vertical jump. |
| Full PPE SCBA gear Sequential tasks 20.4 kgs | Significant relationships between cardiovascular endurance (r = −0.49, p < 0.01), bench press (r = −0.51, p < 0.01), push-ups (r = −0.38, p = 0.01), sit-ups (r = −0.41, p < 0.01), power (r = −0.32, p < 0.01) and total firefighting ability (total completion time). |
| Davis et al. [74] | Cross sectional study USA, Washington D.C | 100 full-time male firefighters | Age: 33.1 ± 7.63 Height: 176.7 ± 5.43 cm Weight: 83.4 ± 10.94 kgs LBM: 65.8 ± 5.98 kgs BF%: 21.1 ± 6.69% O2max: 39.60 ± 5.94 mL·kg·min. Treadmill test, handgrip strength, sit-ups, push-ups, sit-and-reach. |
| Full PPE SCBA gear Sequential tasks 24 kgs | Significant predictors of performance on simulated tasks included the firefighters’ lean body mass, maximal heart rate, cardiorespiratory fitness, age, and BF%. High muscular strength and endurance and near maximal aerobic capacity was necessary to complete simulated tasks. |
| Elsner and Kolkhorst [68] | Cross-sectional study USA, San Diego | 20 male firefighters | Age: 37.4 ± 8.5 years Height: 178 ± 6 cm Weight: 86.8 ± 8.9 kgs Body fat: 16.9 ± 4.7% Time: 11.65 ± 2.21 min Average O2: 29.1 ± 8.0 mL·kg·min Treadmill test |
| Full PPE and SCBA gear Sequential tasks | There was a moderately strong inverse relationship between O2max and performance time as well as a strong positive relationship between O2max and average O2 during the firefighting protocol. |
| Henderson et al. [80] | Cohort study USA, Milwaukee | 306 male and female firefighter recruits | Age: 26.1 ± 4.7 years Height: 180.5 ± 6.4 cm LBM: 74.4 ± 8.1 kgs BF%: 13.3 ± 4.5% Step test, bench press, lat pull-down, grip strength, sit-ups |
| Full PPE and SCBA gear Sequential tasks 29.3 kgs | BF% (r = −0.17) and age (r = −0.03) was negatively correlated with combat test performance. Absolute O2max (r = 0.43), bench press (r = 0.33), grip strength (r = 0.50), sit-ups (r = 0.31) were positively correlated with combat test performance. |
| Kleinberg et al. [67] | Cross-sectional study USA, North Carolina | 46 male firefighters | Age: 37.6 ± 7.2 years Stature: 180.2 ± 6.9 cm Body mass (kgs) 108.0 ± 19.8 kgs BMI: 33.1 ± 4.7 kg·m−2 Quadriceps cross-sectional area (QCSA) (cm2/kgs): 0.50 ± 0.07 Quadriceps echo intensity (QEI): 109.3 ± 13.9 | Stair-climb (s) | Fitted with weighted vest to simulate weight of PPE 22.7 kgs | Quadriceps cross-sectional area (QCSA) and quadriceps echo intensity (QEI) were significantly associated with stair-climb time (r = 20.492, p = 0.001; r = 0.363, p = 0.013, respectively). QCSA and QEI as significant predictors of stair-climb time (r = 0.560, p < 0.001) and a VIF of 1.046. |
| Lindberg et al. [62] | Cross sectional study Northern Sweden | 38 male and female full-time, volunteer firefighters and civilians. | Age: 34 ± 9.8 years Weight: 78 ± 11.1 kgs Height: 177.2 ± 7.9 cm BMI: 25 ± 2.7 kg·m−2 Grip strength, sit-ups, grip endurance, squat endurance, bench press endurance, chin ups, dips, upright barbell row, standing broad jump, barbell shoulder press |
| 19 kgs | Significant correlations were present between all field tests and all the firefighter specific tasks (r = 0.45 to 0.85). |
| Lindberg et al. [61] | Cross sectional study Northern Sweden | 38 male and female full-time, volunteer firefighters and civilians. | Age: 34 ± 9.8 years Weight: 78 ± 11.1 kgs Height: 177.2 ± 7.9 cm BMI: 25 ± 2.7 kg·m−2 Treadmill test, track running, step test, rowing. |
| 24 kgs | Absolute and relative O2max were significantly correlated to cutting (r = 0.55; r = 0.47), stairs (r = −0.75; r = −0.52), pulling (r = −0.74; r = −0.46), demolition (r = −0.79; r = −0.57), rescue (r = −0.79; r = −0.48) and terrain (r = −0.70; r = −0.74) performance. |
MacDermid et al. [29] | Cross-sectional study Canada, Hamilton | 293 male and female firefighters | Age: 42.6 ± 9.7 years Height: N/A Weight: N/A BMI: N/A | Work Limitations Questionnaire (WLQ-26)
| Not specified Discrete tasks Not specified | Firefighters who reported having moderate to severe muscle and joint problems took approximately 10s longer to complete the stair climb task than did firefighters not reporting those problems. |
| Michaelides et al. [73] | Cross-sectional study USA, Arkansas | 38 experienced volunteer firefighters | Age: 32.25 ± 6.07 years Weight: 96.1 ± 16.4 kgs Height: 178.21 ± 7.35 cm BF%: 21.78 ± 6.22% Abdominal strength, Relative power (vertical jump), Power (vertical jump), grip strength, bench press, squat, Sit and reach, Relative power (step test), Power (step test), Push-ups, Sit-ups |
| Full PPE and SCBA gear Sequential tasks 22.68 kgs | Upper body muscular endurance (push-ups to exhaustion) and upper body strength (1-RM bench press) were significantly inversely related with the total completion time the test (AT score; p < 0.01). In addition, there were significant positive associations (p < 0.01) between %BF and RHR variables and time to complete the AT. Flexibility, t(36) = 2.71, p < 0.05, %BF, t(36) = 3.11, p < 0.05, 1-RM bench press, t(36) = −2.24, p < 0.05, and 1-RM squat, t(36) = −2.06, p < 0.05, fitness parameters contributed significantly to the predictive power of firefighters’ AT performance. |
| Michaelides et al. [57] | Cross-sectional study USA, Arkansas | 90 full-time male firefighters | Age: 32.25 ± 6.07 years Height: 181.16 ± 6.62 cm Body weight: 97.04 ± 15.51 kgs Age: 33 ± 67years Body fat: 23.05 ± 5.58% BMI: 29.55 ± 3.67 kg·m−2 Waist circumference: 97.33 ± 10.96 cm Abdominal strength, Relative power (vertical jump), Power (vertical jump), grip strength, bench press, squat, Sit and reach, Relative power (step test), Power (step test), Push-ups, Sit-ups |
| Full PPE and SCBA gear Sequential tasks 22.68 kgs | Negative correlations indicated that higher performance on the fitness variables were associated with faster completion of the AT test, thus higher firefighting performance. Poor performance on the AT was significantly correlated (positive correlations) with high resting heart rate, body mass index (BMI), BF%, age, and waist size. Results showed that abdominal strength (t [53] = 22.94, p = 0.01); power, step test (t [53] = 22.37, p = 0.05); push-ups (t [53] = 1.97, p = 0.05); resting Hr (t [53] = 2.64, p = 0.05); and BF% (t [53] = 4.29, p = 0.01) contributed significantly to the predictive power of firefighters’ AT performance |
| Misner et al. [76] | Cross-sectional study USA, Chicago | 150 female firefighter applicants | Age: 27.1 ± 4.5 years Height: 164.9 ± 5.6 cm Body mass: 63.4 ± 7.9 kgs BF%: 19.0 ± 5.9% LBM: 50.8 ± 4.3 kgs Leg press, bicycle ergometer, vertical jump, Wingate anaerobic test. | Stair climb test | Harness containing air pack 13.1 kgs | Stair climb performance was significantly correlated with age, lean body mass, vertical jump and peak power |
| Myhre et al. [65] | Cross-sectional study USA | 222 male and female firefighters | Age: 30.4 ± 9.3 years Height: 178.6 ± 7.6 cm Weight: 83.5 ± 13.1 kgs BF%: 20.1 ± 6.9% Cycle ergometer test, bench press, upright forearm curl, upright row, barbell raise and lower. |
| Full PPE and SCBA gear Sequential tasks 22.2 kgs | Recue time was positively correlated to age (r = 0.38), and BF% (r = 0.36) and negatively correlated to O2max (r = −0.36), bench press (r = −0.18) and abdominal curl (r = −0.25). |
| Nazari et al. [31] | Cross-sectional study Canada, Ontario | 46 males and 3 females firefighters | Age: 33.66 ± 9.19 years Height: 1.81 ± 0.08 cm Weight: 90.35 ± 13.22 kgs BMI: 27.53 ± 3.56 kg·m−2 O2max: 40.30 ± 6.25 mL·kg·min Cardiorespiratory fitness NIOSH lower limb strength combined grip strength |
| Full PPE and SCBA gear Discrete tasks 22.7 kgs | A negative correlation was present and indicated that higher O2max and/or strength levels were associated with faster completion of tasks Grip strength (r = −0.30) and CRF (r = −0.25) was negatively correlated to hose drag task. CRF was negatively correlated to the stair climb (r = −0.31). In predicting hose drag completion times, firefighters’ age and right grip strength scores were shown to be the most statistically significant. |
| Perroni et al. [85] | Cross-sectional study Italy, Rome | 20 full-time male firefighters | Height: 177 ± 6 cm Weight: 77.2 ± 8.7 kgs BMI: 24.7 ± 2.1 kg·m−2 HRmax: 90 ± 5% (176 ± 9 bmp) O2peak: 43.1 ± 4.9 mL·kg·min. Treadmill test |
| Discrete testing 23 kgs | There was a significant correlation between O2peak and time to job completion of the simulated intervention (r = 0.09, p = 0.72). Correlation coefficients ranging from 0.09 to 0.53 existed between O2peak and time to complete the different tasks. |
| Phillips et al. [79] | longitudinal study, cohort and cross-sectional study design Canada, Alberta | 414 male firefighter applicants | Age: 27 ± 5 years Height: 180 ± 6 cm Mass: 89.0 ± 17.0 kgs BMI: 26.9 ± 4.2 kg·m−2 Treadmill: 15.9 ± 2.7 min Treadmill test |
| PPE only Sequential testing 23.3 kgs | There was a significant correlation between body mass and treadmill test duration and a stronger correlation (r = 0.76) between test duration and O2peak relative to total mass. The less than 70.0 and 70.0 to 79.9 kg mass categories were significantly slower compared with the others during the charged hose drag. For the weighted sled pull, forcible entry and victim rescue tasks, the less than 70 kg group was significantly slower. The more than 110.0 kg group was significantly slower than all the other groups on the ladder climb test. There were modest correlations (p < 0.05) between body mass and task completion time for the charged hose drag and weighted sled pull tests (r = 0.44, r = 0.36, respectively. There were weak correlations between task completion time and body mass for the forcible entry, victim rescue, and ladder climb tests. |
| Rhea et al. [42] | Cross-sectional study USA, Phoenix | 20 male firefighters | Age: 34.5 ± 6.1 years Professional service: 6.1 ± 5.2 years BF%: 16.6 ± 3.9% 12-min run, bench press 5 rm(kg) squat 5 rm (kg), hand grip strength (kg), row endurance, bench press endurance, shoulder press endurance (reps), bicep curl endurance, squat endurance, ab curls, hand grip endurance, 400-m run, body fat %: |
| Full SCBA gear Discrete testing 25 kg | Significant correlations (p < 0.05) between job performance and the following variables: total fitness (r = −0.62), bench press strength (r = −0.66), hand grip strength (r = −0.71), bent-over row endurance (r = −0.61), bench press endurance (r = −0.73), shoulder press endurance (r = −0.71), bicep endurance (r = −0.69), squat endurance (r = −0.47), and 400-m sprint time (r = 0.79). Significant correlations were also identified for each of the individual job performance tests. |
| Ryan et al. [69] | Cross-sectional study USA, North Carolina | 41 full-time male firefighters | Age: 32.3 ± 2.5 years Stature: 178.3 ± 2.4 cm Body mass: 92.3 ± 5.7 kgs BMI: 29.0 ± 1.6 kg·m−2 BF%: 24.1 ± 2.4% | Stair climb time | Fitted with weighted vest to simulate weight of PPE. 22.73 kgs | Faster firefighter Stair Climb times (lower scores) were significantly associated with greater Peak Torque (r = −0.421; p = 0.007), greater PP (r = −0.530; p = 0.001), less fatigability (r = −0.389; p = 0.014), younger age (r = 0.441; p = 0.004), lower %BF (r = 0.629; p < 0.001). |
| Saari et al. [74] | Cross-sectional study USA, Ohio | 74 full-time male firefighters | Younger vs. Older Age: 31.80 ± 3.42 vs. 44.65 ± 5.18 years Height: 179.85 ± 6.32 vs. 182.23 ± 5.57 cm Body mass: 92.61 ± 8.73 vs. 89.77 ± 23.06 kgs BF%: 15.94 ± 4.31 vs. 19.49 ± 4.58% Fat mass: 14.95 ± 4.84 vs. 17.71 ± 7.52 kgs Fat-free mass: 77.65 ± 6.32 vs. 72.06 ± 17.12 kgs Waist circumference: 88.67 ± 6.56 vs. 72.06 ± 17.12 cm Hip circumference: 102.47 ± 4.70 vs. 105.14 ± 6.57 cm |
| Full PPE and SCBA gear. Sequential testing Not specified | On average, it took older firefighters 8.8% longer to complete the course compared with younger firefighters (p = 0.029,). Age was positively correlated with course time (r = 0.297, p = 0.017) |
| Schonfeld et al. [60] | Cross-sectional study USA | 20 male volunteer firefighters | Age: 38.6 ± 2.5 years Height: 175.7 ± 1.1 cm Weight: 75.4 ± 1.9 kgs O2max: 48.5 ± 2.1 mL·kg·min BF%: 22.4 ± 0.9% Treadmill test |
| Full PPE and SCBA gear Sequential testing 24 kg | O2max (r = −0.628) and BF% (r = 0.467) were correlated with total performance time. BF% was only correlated individually to stair climb (r = 0.535), whereas O2max was correlated to all stair climb, chopping and victim drag (r = −0.627, −0.324 and −0.447) |
| Sheaff et al. [72] | Cross-sectional study USA, Baltimore–Washington | 33 Career and volunteer firefighters | Age: 28 ± 1 years Height: 179.2 ± 1.6 cm Weight: 87.6 ± 3.8 kgs BMI: 27.1 ± 0.9 kg·m−2 BF%: 22.2 ± 1.1% O2max: 41.5 ± 1.4 mL·kg·min Cycle ergometer, treadmill test, chest press, leg press, knee extension. |
| Full SCBA gear Sequential testing CPAT 22.7 kgs | O2max (r = 20.602; p = 0.001), 4-finger isometric grip strength (r = 20.504; p = 0.009), and upper body strength (r = 20.485; p = 0.001) were also significantly related to CPAT performance. Furthermore, maximal HR response to stair climbing was significantly related to performance time (r = 0.523; p = 0.01), and percent of maximal HR during the stair climb (r = 0.488; p = 0.012). |
| Siddall et al. [28] | Cross-sectional study United Kingdom, London | 68 (63 male; 5 female) full-time firefighters | Age: 41 ± 8 years Mass: 85.7 ± 12.9 kgs Height: 1.78 ± 0.06 m BF%: 19.7 ± 5.6% Fat mass: 17.3 ± 7.0 kgs absolute O2max: 4.0 ± 0.7 mL·kg·min relative O2max: 47.7 ± 9.0 mL·kg·min Treadmill test |
| Full PPE and SCBA gear Sequential testing 20.3 kgs | Relative O2 had a stronger inverse correlation with FFST performance time (R = −0.711; R2 = 0.506, SEE = ±56 s) than absolute O2 (R = −0.577; R2 = 0.332; SEE = ±65 s), explaining ~18% more of the variance in FFST performance. The combination of variables that produced the strongest prediction of FFST time was the absolute O2 and fat mass, which explained 26% and 8% of the variance. |
| Sothmann et al. [39] | Cross-sectional study USA, Chicago | 153 full-time male and female firefighters | Age: 36 ± 6 years Years as firefighter: 8 ± 5 years Height: 172 ± 7.6 cm Weight: 84 ± 13 kgs |
| Discrete testing Not disclosed | Women completed the simulation approximately 35% slower than men which when tested by ANOVA proved to be a statistically significant difference (F 1151 = 5.70, p = 0.01). There was a significant age effect (F 3149 = 5.76, p < 0.01) on the performance times of the simulation protocol. Firefighters aged 50 years and over performed the protocol significantly slower than each of the three younger age classifications. |
| Stevenson et al. [64] | Cross-sectional study United Kingdom, London | 69 full-time male and female firefighters | Age: 40 ± 8 years Mass: 85.8 ± 12.8 kgs Height: 178 ± 6 cm BMI: 27.0 ± 3.6 kg·m−2 BF%: 19.7 ± 5.5% O2max: 47.8 ± 9.0 mL·kg·min Treadmill test |
| Full PPE and SCBA gear Sequential testing 20.2 kgs | The time to complete the firefighting simulation test (FFST) was highly inversely correlated with cardiorespiratory fitness (r = −0.73, p = 0.01). |
| Skinner et al. [30] | Cross-sectional study Australia | 42 full-time male Aviation Rescue Firefighters | Age: 38.4 ± 7.6 years Height: 180.2 ± 6.6 cm Body mass: 81.9 kgs BMI: 26.2 ± 2.2 kg·m−2 Fat mass: 18.3 ± 5.6 kgs Lean mass: 62.7 ± 6.5 kgs BF%: 21.5 ± 4.6% O2max: 49.5 ± 6.9 mL·kg·min Treadmill test, 3rm bench press, 3rm leg press (kg), total grip strength (kg), anaerobic step test (max), sit and reach, abdominal curl, push ups. | Simulated aircraft rescue and firefighting (ARFF) tasks
| Full SCBA gear Sequential testing 16.5 kgs | Older age, and longer arm length had small-to-moderate correlations with slower time to complete the dummy drag and hose drag tasks respectively. A strong inverse correlation was observed between time to complete the simulated ARFF emergency protocol for speed at lactate threshold, anaerobic step test performance and O2max. 3RM bench press presented a moderate to strong inverse correlation to hose drag performance time. The muscular endurance measure of maximal push-ups was significantly inversely correlated (r = −0.3) with hose drag performance time. A strong inverse correlation was observed between time to complete the simulated ARFF emergency protocol for speed at lactate threshold, anaerobic step test performance and O2max |
| von Heimburg et al. [71] | Cross-sectional study Norway, Trondheim | 14 Part-time male firefighters | Age: 38 ± 9 years Height: 1.79 ± 0.07 m Weight: 83 ± 11 kgs BMI: 26 ± 2 kg·m−2 Waist circumference: 94 ± 7 cm Hip circumference: 102 ± 5 cm Waist-to-hip ratio: 0.92 ± 0.04 O2max: 4.4 ± 0.3 L·min O2max: 53 ± 5 mL·kg·min Treadmill test, leg press, bench press, press behind the neck. |
| Full PPE and SCBA gear Sequential testing | The peak oxygen uptake in absolute terms was 18% higher in the faster subjects than in the slower ones during the rescue. The accumulated oxygen uptake obtained by integrating the oxygen uptake over the whole operation was less in the faster subjects, both in absolute terms (17%) and relative to body mass (25%). The faster firefighters had an 8% higher O2max expressed in absolute terms, but there was no difference between the two groups when the O2max was expressed relative to body mass. The eight faster subjects were stronger (13%) than the six slower ones in terms of the pooled strength index. |
| von Heimburg et al. [58] | Cross-sectional study Norway, Trondheim | 22 full-time firefighters | 23 Males/1 female Age: 42 ± 9 vs. 26 years Height: 1.82 ± 0.05 vs. 1.69 cm Body mass: 85 ± 9 vs. 58 kgs BF%: 23 ± 6% vs. 16% Lean body mass: 66 ± 6 kgs vs. 49 kgs BMI: 26 ± 2 kg·m−2 vs. 20.3 kg·m−2 NLIA treadmill test | Part 1:
Part 2:
Part 3:
| Full PPE and SCBA gear Sequential testing 28 kgs | Firefighters with high O2max completed the test faster than firefighters with lower O2max. Performance on the Trondheim test correlated with the measured strength on all three strength tests and with the pooled strength index; the stronger participants were the fastest |
| von Heimburg et al. [70] | Cross-sectional study Norway, Trondheim | 43 experienced and inexperienced male and female firefighters | Age: 41.4 ± 4.2 years Body mass: 84 ± 9.9 kgs Height: 1.81 ± 0.06 cm BMI: 25.5 ± 2.6 kg·m−2 BF%: 21.6 ± 5.8% LBM: 65.8 ± 5.9 kgs NLIA Tests | Trondheim test Part 1:
| Full PPE and SCBA gear Sequential testing 23 kgs | The young men performed the skill and agility tasks faster than the senior firefighters and the female applicants. |
| Williford et al. [77] | Cross-sectional study USA, Alabama | 91 full-time male firefighters | Age: 31.69 ± 7.39 years Height: 177.29 ± 6.38 cm Weight: 83.97 ± 10.86 kgs BF%: 13.78 ± 4.31% O2 peak relative: 45.0 ± 6.0 mL·kg·min O2 peak absolute: 3.75 ± 0.43 L·min 1.5 mile run (s), Pull-ups, Push-ups Sit and reach(cm), Sit ups, Total grip strength (kg) |
| Full PPE and SCBA gear Sequential testing 23 kgs | Significant correlations (p < 0.01) were found between the total obstacle course time and the following: total grip strength (r = −0.54), FFW (r = −0.47), height (r = −0.40), pull-ups (r = −0.38), push-ups (r = −0.38), 1.5 mile run (r = −0.38), sit-ups (r = −0.32), weight (r = −0.30) and BF% (r = 0.30. FFW and 1.5 mile run times to predict total obstacle course time (r = 0.71, r2 = 0.50, SE = 99.18 s). |
| Windisch, et al. [75] | Cross-sectional study Germany, Munich | 41 full-time male firefighters | Age: 39 ± 9 years Height: 179.6 ± 2.3 cm Weight: 84.4 ± 9.2 kgs BMI: 26.1 ± 2.8 kg·m−2 O2max: 45.0 ± 6.0 mL·kg·min Treadmill test, leg press, hand grip, partial-curl ups, push-ups, shoulder press, rowing, standing long jump, sit and reach. |
| Full PPE with SCBA gear and without SCBA gear Sequential tasks | It can be noted that outstanding performers had significantly higher O2 peak (p = 0.001) and significantly lower mean heart rates during REPE (p = 0.001) while completing the exercise faster (p = 0.001) compared to average, below average and poor performers. Aerobic fitness was a significant predictor of the speed a firefighter can perform the tasks |
| Xu et al. [63] | Cross-sectional study China, South East | 20 full-time firefighters | Age: 25.65 ± 2.97 years; Height: 172.4 ± 4.8 cm; Body mass: 69.0 ± 8.9 kgs O2: 46.85 mL·kg·min BF%: 14.65% upper body muscular power: 675.35 watts lower body muscular power: 1705 watts Cycle ergometer, chest press, sitting leg power. |
| An increase in O2max decreased the time to complete firefighting tasks. Increased BF% increased the time to complete each task. Increased upper body strength the time to complete each task decreased. Increased lower body strength decreased the time to complete each task. |
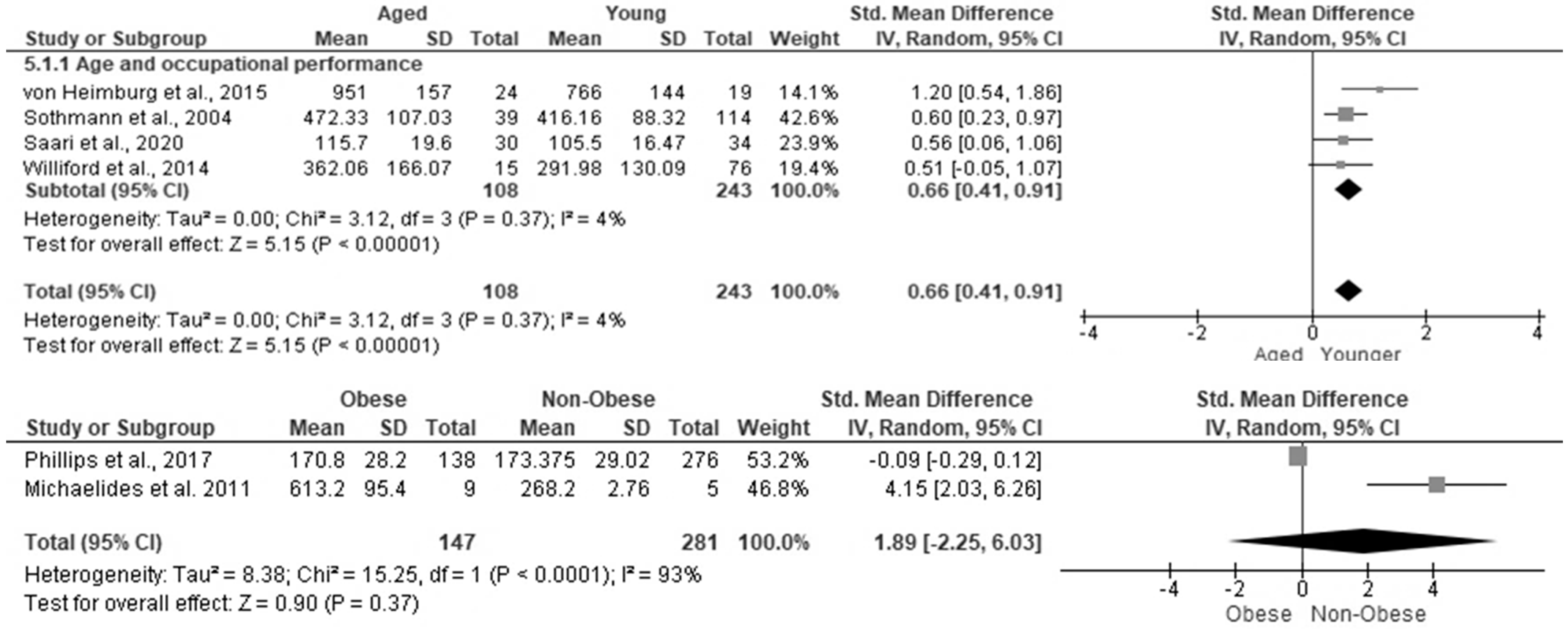
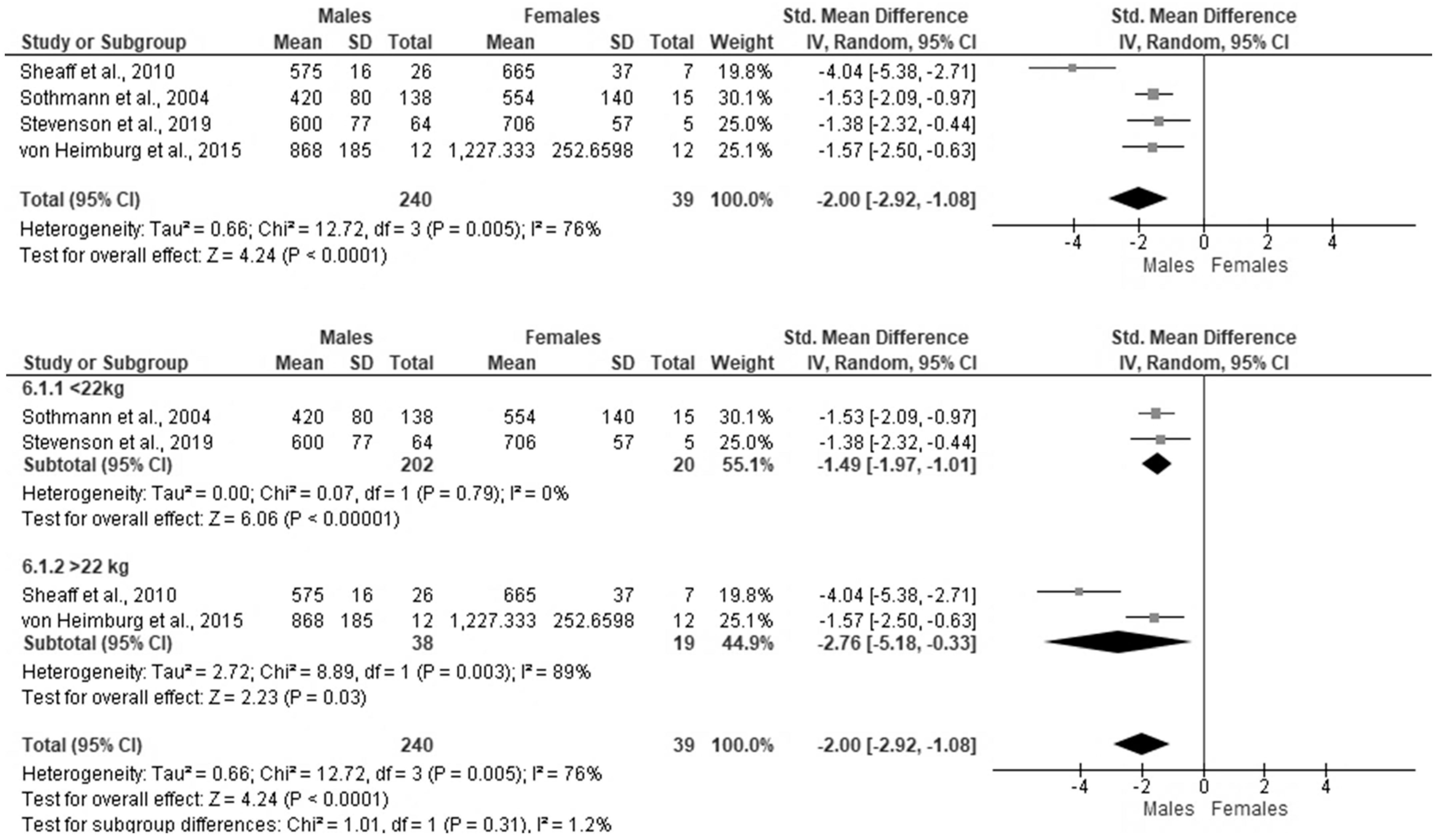
3.6. The Effect of Aging, Obesity, Heart Rate and Gender on Occupational Performance in Firefighters
3.7. Correlation between Obesity, Aging and Resting Heart Rate on Occupational Performance
3.8. Correlation between Fitness Parameters and Occupational Performance
3.9. Correlation between Obesity and Age on Individual Task Performance in Firefighters
3.10. Correlation between Physical Fitness and Individual Task Performance
4. Discussion
4.1. Summary of Evidence
4.2. The Effect of Age, Obesity, Blood Pressure, Heart Rate and Gender on Occupational Performance
4.3. The Effect of Physical Fitness on Occupational Performance
4.4. Limitations of the Study
4.5. Applicability of Evidence
4.6. Quality of Evidence
4.7. Gaps in the Literature
4.8. Implications for Future Research
5. Conclusions
6. Patents
Protocol Registration
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shin, J.-H.; Lee, J.-Y.; Yang, S.-H.; Lee, M.-Y.; Chung, I.-S. Factors related to heart rate variability among firefighters. Ann. Occup. Environ. Med. 2016, 28, 25. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L.; Barr, D.A.; Kales, S.N. Extreme sacrifice: Sudden cardiac death in the US Fire Service. Extreme Physiol. Med. 2013, 2, 6. [Google Scholar] [CrossRef] [PubMed]
- Soteriades, E.S.; Smith, D.L.; Tsismenakis, T.; Baur, D.M.; Kales, S.N. Cardiovascular disease in US firefighters: A systematic review. Cardiol. Rev. 2011, 19, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Lima, E.D.P.; Assunção, A.; Barreto, S.M. Smoking and occupational stressors in firefighters, 2011. Rev. Saude Publica 2013, 47, 897–904. [Google Scholar] [CrossRef]
- Navarro, K.M.; Kleinman, M.T.; Mackay, C.E.; Reinhardt, T.E.; Balmes, J.R.; Broyles, G.A.; Ottmar, R.D.; Naher, L.P.; Domitrovich, J.W. Wildland firefighter smoke exposure and risk of lung cancer and cardiovascular disease mortality. Environ. Res. 2019, 173, 462–468. [Google Scholar] [CrossRef]
- Smith, D.L.; Deblois, J.P.; Kales, S.N.; Horn, G.P. Cardiovascular Strain of Firefighting and the Risk of Sudden Cardiac Events. Exerc. Sport Sci. Rev. 2016, 44, 90–97. [Google Scholar] [CrossRef]
- Farioli, A.; Yang, J.; Teehan, D.; Baur, D.M.; Smith, D.L.; Kales, S.N. Duty-related risk of sudden cardiac death among young US firefighters. Occup. Med. 2014, 64, 428–435. [Google Scholar] [CrossRef]
- Smith, D.L.; Haller, J.M.; Korre, M.; Sampani, K.; Porto, L.G.G.; Fehling, P.C.; Christophi, C.A.; Kales, S.N. The Relation of Emergency Duties to Cardiac Death among US Firefighters. Am. J. Cardiol. 2019, 123, 736–741. [Google Scholar] [CrossRef]
- Marcel-Millet, P.; Ravier, G.; Grosprêtre, S.; Gimenez, P.; Freidig, S.; Groslambert, A. Physiological responses and parasympathetic reactivation in rescue interventions: The effect of the breathing apparatus. Scand. J. Med. Sci. Sports 2018, 28, 2710–2722. [Google Scholar] [CrossRef]
- Feairheller, D.L. Blood pressure and heart rate responses in volunteer firefighters while wearing personal protective equipment. Blood Press. Monit. 2015, 20, 194–198. [Google Scholar] [CrossRef]
- Rodrigues, S.; Dias, D.; Paiva, J.S.; Cunha, J.P. Psychophysiological Stress Assessment among On-Duty Firefighters. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 4335–4338. [Google Scholar] [CrossRef]
- Liao, L.-M.; Al-Zaiti, S.S.; Carey, M.G. Depression and heart rate variability in firefighters. SAGE Open Med. 2014, 2, 2050312114545530. [Google Scholar] [CrossRef]
- Hom, M.A.; Stanley, I.H.; Rogers, M.L.; Tzoneva, M.; Bernert, R.A.; Joiner, T.E. The Association between Sleep Disturbances and Depression among Firefighters: Emotion Dysregulation as an Explanatory Factor. J. Clin. Sleep Med. 2016, 12, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Gulliver, S.B.; Zimering, R.T.; Knight, J.; Morissette, S.B.; Kamholz, B.W.; Pennington, M.L.; Dobani, F.; Carpenter, T.P.; Kimbrel, N.A.; Keane, T.M.; et al. A prospective study of firefighters’ PTSD and depression symptoms: The first 3 years of service. Psychol. Trauma 2021, 13, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Ras, J.; Leach, L. Prevalence of Coronary Artery Disease Risk Factors in Firefighters in the City of Cape Town Fire and Rescue Service—A Descriptive Study. J. Public Health Res. 2021, 10, 2000. [Google Scholar] [CrossRef] [PubMed]
- Savall, A.; Charles, R.; Bertholon, A.; Gramont, B.; Trombert, B.; Barthélémy, J.-C.; Roche, F. Volunteer and career French firefighters: Cardiovascular risk factors and cardiovascular risk assessment. Eur. J. Prev. Cardiol. 2020, 27, 107–109. [Google Scholar] [CrossRef]
- Hunter, A.L.; Shah, A.; Langrish, J.P.; Raftis, J.B.; Lucking, A.J.; Brittan, M.; Venkatasubramanian, S.; Stables, C.; Stelzle, D.; Marshall, J.; et al. Fire Simulation and Cardiovascular Health in Firefighters. Circulation 2017, 135, 1284–1295. [Google Scholar] [CrossRef]
- Wolkow, A.; Netto, K.; Langridge, P.; Green, J.; Nichols, D.; Sergeant, M.; Aisbett, B. Cardiovascular risk screening of volunteer firefighters. In Proceedings of the Bushfire CRC & AFAC 2012 Conference Research Forum, Perth, Australia, 28 August 2012. [Google Scholar]
- Gendron, P.; Lajoie, C.; Laurencelle, L.; Trudeau, F. Cardiovascular disease risk in female firefighters. Occup. Med. 2018, 68, 412–414. [Google Scholar] [CrossRef]
- Azmi, N.L.A.M.; Masuri, M.G. Work-related musculoskeletal disorder (WMSDs) and functional status of firefighters in Klang Valley. Healthscope Off. Res. Book Fac. Health Sci. UiTM 2019, 2. Available online: http://healthscopefsk.com/index.php/research/article/view/74 (accessed on 7 August 2021).
- Kodom-Wiredu, J.K. The Relationship between Firefighters’ Work Demand and Work-related Musculoskeletal Disorders: The Moderating Role of Task Characteristics. Saf. Health Work 2019, 10, 61–66. [Google Scholar] [CrossRef]
- Ras, J.; Leach, L. Relationship between Physical Activity, Coronary Artery Disease Risk Factors and Musculoskeletal Injuries in the City of Cape Town Fire and Rescue Service. Inq. J. Health Care Organ. Financ. 2022, 59, 00469580221084485. [Google Scholar] [CrossRef]
- Saremi, M.; Madvari2, R.F.; Laal, F.; Noorizadeh, N.; Rahimi, E. Assessment of Mental Workload, Workability and Musculoskeletal Disorders of Firefighters. J. Community Health. Res. 2019, 8, 139–147. [Google Scholar] [CrossRef]
- Donovan, R.; Nelson, T.; Peel, J.; Lipsey, T.; Voyles, W.; Israel, R.G. Cardiorespiratory fitness and the metabolic syndrome in firefighters. Occup. Med. 2009, 59, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Lipsey, T.; Leach, H.J.; Nelson, T.L. Cardiac health and fitness of Colorado male/female firefighters. Occup. Med. 2017, 67, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.M.; Christophi, C.A.; Tsismenakis, T.; Cook, E.F.; Kales, S.N. Cardiorespiratory Fitness Predicts Cardiovascular Risk Profiles in Career Firefighters. J. Occup. Environ. Med. 2011, 53, 1155–1160. [Google Scholar] [CrossRef]
- Seyedmehdi, S.M.; Attarchi, M.; Cherati, A.S.; Hajsadeghi, S.; Tofighi, R.; Jamaati, H. Relationship of aerobic fitness with cardiovascular risk factors in firefighters. Work 2016, 55, 155–161. [Google Scholar] [CrossRef]
- Siddall, A.G.; Stevenson, R.D.M.; Turner, P.J.F.; Bilzon, J.L.J. Physical and Physiological Performance Determinants of a Firefighting Simulation Test. J. Occup. Environ. Med. 2018, 60, 637–643. Available online: https://journals.lww.com/joem/Fulltext/2018/07000/Physical_and_Physiological_Performance.10.aspx (accessed on 20 May 2022). [CrossRef]
- MacDermid, J.C.; Tang, K.; Sinden, K.E.; D’Amico, R. Work Functioning among Firefighters: A Comparison between Self-Reported Limitations and Functional Task Performance. J. Occup. Rehabil. 2019, 29, 194–204. [Google Scholar] [CrossRef]
- Skinner, T.L.; Kelly, V.G.; Boytar, A.N.; Peeters, G.; Rynne, S.B. Aviation Rescue Firefighters physical fitness and predictors of task performance. J. Sci. Med. Sport 2020, 23, 1228–1233. [Google Scholar] [CrossRef]
- Nazari, G.; MacDermid, J.C.; Sinden, K.E.; Overend, T.J. The Relationship between Physical Fitness and Simulated Firefighting Task Performance. Rehabil. Res. Pr. 2018, 2018, 3234176. [Google Scholar] [CrossRef]
- Li, J.; Wang, Y.; Jiang, R.; Li, J. Quantifying self-contained breathing apparatus on physiology and psychological responses during firefighting: A systematic review and meta-analysis. Int. J. Occup. Saf. Ergon. 2022, 1–13. [Google Scholar] [CrossRef]
- Nazari, G.; Lu, S.; MacDermid, J.C. Quantifying physiological responses during simulated tasks among Canadian firefighters: A systematic review and meta-analysis. J. Mil. Veter-Fam. Health. 2021, 7, 55–75. [Google Scholar] [CrossRef]
- Soares, E.M.K.V.K.; Smith, D.; Porto, L.G.G. Worldwide prevalence of obesity among firefighters: A systematic review protocol. BMJ Open 2020, 10, e031282. [Google Scholar] [CrossRef]
- Park, K.; Rosengren, K.S.; Horn, G.P.; Smith, D.L.; Hsiao-Wecksler, E.T. Assessing gait changes in firefighters due to fatigue and protective clothing. Saf. Sci. 2011, 49, 719–726. [Google Scholar] [CrossRef]
- Park, K.; Sy, J.F.; Horn, G.P.; Kesler, R.M.; Petrucci, M.N.; Rosengren, K.S.; Hsiao-Wecksler, E.T. Assessing gait changes in firefighters after firefighting activities and while carrying asymmetric loads. Appl. Ergon. 2018, 70, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Magyari, P.; Fonger, T.; May, J. Upper Body Muscular Endurance among Active Duty Male and Female Firefighters. J. Strength Cond. Res. 2010, 24, 1. Available online: https://journals.lww.com/nsca-jscr/Fulltext/2010/01001/Upper_Body_Muscular_Endurance_Among_Active_Duty.99.aspx (accessed on 20 May 2022). [CrossRef]
- Lindberg, A.-S.; Oksa, J.; Antti, H.; Malm, C. Multivariate Statistical Assessment of Predictors of Firefighters’ Muscular and Aerobic Work Capacity. PLoS ONE 2015, 10, e0118945. [Google Scholar] [CrossRef]
- Sothmann, M.S.; Gebhardt, D.L.; A Baker, T.; Kastello, G.M.; A Sheppard, V. Performance requirements of physically strenuous occupations: Validating minimum standards for muscular strength and endurance. Ergonomics 2004, 47, 864–875. [Google Scholar] [CrossRef]
- Schmit, M.; DeBeliso, M. The Relationship between Firefighters’ Physical Performance Aspects and Simulated Firefighting Demands. Turk. J. Kinesiol. 2019, 5, 63–75. [Google Scholar] [CrossRef]
- Smith, D.L.; Haller, J.M.; Benedict, R.; Moore-Merrell, L. Firefighter Incident Rehabilitation: Interpreting Heart Rate Responses. Prehospital Emerg. Care 2016, 20, 28–36. [Google Scholar] [CrossRef]
- Rhea, M.R.; Alvar, B.A.; Gray, R. Physical Fitness and Job Performance of Firefighters. J. Strength Cond. Res. 2004, 18, 348–352. [Google Scholar] [CrossRef]
- Hong, O.; Phelps, S.; Feld, J.; Vogel, S. Occupational Injuries, Duty Status, and Factors Associated with Injuries among Firefighters. Work. Health Saf. 2012, 60, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.; Molik, B.; Wójcik, A.; Rutkowska, I.; Nowacka-Dobosz, S.; Kowalczyk, M.; Marszalek, J. Physical Activity and Injuries Relating to Physical Fitness of Professional Firefighters. Adv. Rehabil. 2018, 32, 13–22. [Google Scholar] [CrossRef]
- Ras, J.; Leach, L. Use of Mobile Technology in Assessing Occupational Performance and Stress in Firefighters. In Handbook of Research on New Media, Training, and Skill Development for the Modern Workforce; Mentor, D., Ed.; IGI Global: Hershey, PA, USA, 2022; pp. 150–186. [Google Scholar] [CrossRef]
- Walls, R.S.; Eksteen, R.; Kahanji, C.; Cicione, A. Appraisal of fire safety interventions and strategies for informal settlements in South Africa. Disaster Prev. Manag. Int. J. 2019, 28, 343–358. [Google Scholar] [CrossRef]
- Walls, R.; Olivier, G.; Eksteen, R. Informal settlement fires in South Africa: Fire engineering overview and full-scale tests on “shacks”. Fire Saf. J. 2017, 91, 997–1006. [Google Scholar] [CrossRef]
- Ryan, A.M.; Greguras, G.J.; Ployhart, R.E. Perceived Job Relatedness of Physical Ability Testing for Firefighters: Exploring Variations in Reactions. Hum. Perform. 1996, 9, 219–240. [Google Scholar] [CrossRef]
- McDonough, S.L.; Phillips, J.S.; Twilbeck, T.J. Determining Best Practices to Reduce Occupational Health Risks in Firefighters. J. Strength Cond. Res. 2015, 29, 2041–2044. Available online: https://journals.lww.com/nsca-jscr/Fulltext/2015/07000/Determining_Best_Practices_to_Reduce_Occupational.34.aspx (accessed on 20 May 2022). [CrossRef]
- Nazari, G.; Osifeso, T.A.; MacDermid, J.C. Distribution of Number, Location of Pain and Comorbidities, and Determinants of Work Limitations among Firefighters. Rehabil. Res. Pr. 2020, 2020, 1942513. [Google Scholar] [CrossRef]
- Ras, J.; Kengne, A.P.; Smith, D.; Soteriades, E.S.; Leach, L. Effects of cardiovascular health, musculoskeletal health and physical fitness on occupational performance of firefighters: Protocol for a systematic review and meta-analysis. BMJ Open 2022, 12, e061435. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of Observational Studies in EpidemiologyA Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Brand, R.A. Editorial: Standards of Reporting: The CONSORT, QUORUM, and STROBE Guidelines. Clin. Orthop. Relat. Res. 2009, 467, 1393–1394. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [PubMed]
- Michaelides, M.A.; Parpa, K.M.; Henry, L.J.; Thompson, G.B.; Brown, B.S. Assessment of Physical Fitness Aspects and Their Relationship to Firefighters’ Job Abilities. J. Strength Cond. Res. 2011, 25, 956–965. [Google Scholar] [CrossRef] [PubMed]
- Von Heimburg, E.; Medbø, J.I. Energy Cost of the Trondheim Firefighter Test for Experienced Firefighters. Int. J. Occup. Saf. Ergon. 2013, 19, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Perroni, F.; Cignitti, L.; Cortis, C.; Capranica, L. Physical Fitness Profile of Professional Italian Firefighters: Differences among Age Groups. Appl. Ergon. 2014, 45, 456–461. [Google Scholar] [CrossRef]
- Schonfeld, B.R.; Doerr, D.F.; Convertino, V.A. An Occupational Performance Test Validation Program for Fire Fighters at the Kennedy Space Center. J. Occup. Environ. Med. 1990, 32, 638–643. Available online: https://journals.lww.com/joem/Fulltext/1990/07000/An_Occupational_Performance_Test_Validation.16.aspx (accessed on 20 May 2022). [CrossRef]
- Lindberg, A.-S.; Oksa, J.; Malm, C. Laboratory or Field Tests for Evaluating Firefighters’ Work Capacity? PLoS ONE 2014, 9, e91215. [Google Scholar] [CrossRef]
- Lindberg, A.-S.; Oksa, J.; Gavhed, D.; Malm, C. Field Tests for Evaluating the Aerobic Work Capacity of Firefighters. PLoS ONE 2013, 8, e68047. [Google Scholar] [CrossRef] [Green Version]
- Xu, D.; Song, Y.; Meng, Y.; István, B.; Gu, Y. Relationship between Firefighter Physical Fitness and Special Ability Performance: Predictive Research Based on Machine Learning Algorithms. Int. J. Environ. Res. Public Health. 2020, 17, 7689. [Google Scholar] [CrossRef]
- Stevenson, R.D.M.; Siddall, A.G.; Turner, P.J.F.; Bilzon, J.L.J. Validity and Reliability of Firefighting Simula-tion Test Performance. J. Occup. Environ. Med. 2019, 61, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Myhre, L.G.; Tucker, D.M.; Bauer, D.H.; Fisher, J.R., Jr.; Grimm, W.H. Relationship between Selected Measures of Physical Fitness and Performance of a Simulated Fire Fighting Emergency Task. ARMSTRONG LAB BROOKS AFB TX 1997. Available online: https://apps.dtic.mil/sti/citations/ADA319915 (accessed on 20 May 2022).
- Chizewski, A.; Box, A.; Kesler, R.; Petruzzello, S.J. Fitness Fights Fires: Exploring the Relationship between Physical Fitness and Firefighter Ability. Int. J. Environ. Res. Public Health. 2021, 18, 11733. [Google Scholar] [CrossRef] [PubMed]
- Kleinberg, C.R.; Ryan, E.D.; Tweedell, A.J.; Barnette, T.J.; Wagoner, C.W. Influence of Lower Extremity Muscle Size and Quality on Stair-Climb Performance in Career Firefighters. J. Strength Cond. Res. 2016, 30, 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- Elsner, K.L.; Kolkhorst, F.W. Metabolic demands of simulated firefighting tasks. Ergonomics 2008, 51, 1418–1425. [Google Scholar] [CrossRef] [PubMed]
- Ryan, E.D.; Laffan, M.R.; Trivisonno, A.J.; Gerstner, G.R.; Mota, J.A.; Giuliani, H.K.; Pietrosimone, B.G. Neuromuscular determinants of simulated occupational performance in career firefighters. Appl. Ergon. 2022, 98, 103555. [Google Scholar] [CrossRef]
- Von Heimburg, E.; Medbø, J.I.; Sandsund, M.; Reinertsen, R.E. Performance on a Work-Simulating Firefighter Test Versus Approved Laboratory Tests for Firefighters and Applicants. Int. J. Occup. Saf. Ergon. 2013, 19, 227–243. [Google Scholar] [CrossRef]
- Von Heimburg, E.D.; Rasmussen, A.K.R.; Medbø, J.I. Physiological responses of firefighters and performance predictors during a simulated rescue of hospital patients. Ergonomics 2006, 49, 111–126. [Google Scholar] [CrossRef]
- Sheaff, A.K.; Bennett, A.; Hanson, E.D.; Kim, Y.-S.; Hsu, J.; Shim, J.K.; Edwards, S.T.; Hurley, B.F. Physiological Determinants of the Candidate Physical Ability Test in Firefighters. J. Strength Cond. Res. 2010, 24, 3112–3122. [Google Scholar] [CrossRef]
- Michaelides, M.A.; Parpa, K.M.; Thompson, J.; Brown, B. Predicting Performance on a Firefghter’s Ability Test from Fitness Parameters. Res. Q. Exerc. Sport 2008, 79, 468–475. [Google Scholar] [CrossRef]
- Saari, A.I.; Renz, G.; Davis, P.; Abel, M.G. The Influence of Age on Firefighter Combat Challenge Performance and Exercise Training Habits. J. Strength Cond. Res. 2020, 34, 2500–2506. [Google Scholar] [CrossRef]
- Windisch, S.; Seiberl, W.; Schwirtz, A.; Hahn, D. Relationships between strength and endurance parameters and air depletion rates in professional firefighters. Sci. Rep. 2017, 7, 44590. [Google Scholar] [CrossRef]
- Misner, J.E.; Boileau, R.A.; Plowman, S.A.; Elmore, B.G.; Gates, M.A.; Gilbert, J.A.; Horswill, C. Leg Power Characteristics of Female Firefighter Applicants. J. Occup. Environ. Med. 1988, 30, 433–437. [Google Scholar] [CrossRef]
- Williford, H.N.; Duey, W.J.; Olson, M.S.; Howard, R.; Wang, N. Relationship between fire fighting suppression tasks and physical fitness. Ergonomics 1999, 42, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Davis, P.O.; Dotson, C.O.; Santa Maria, D.L. Relationship between Simulated Fire Fighting Tasks and Physical Performance Measures. Med. Sci. Sports Exerc. 1982, 14, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Phillips, D.B.; Scarlett, M.P.; Petersen, S.R. The Influence of Body Mass on Physical Fitness Test Performance in Male Firefighter Applicants. J. Occup. Environ. Med. 2017, 59, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Henderson, N.D.; Berry, M.W.; Matic, T. Field Measures of Strength and Fitness Predict Firefighter Performance on Physically Demanding Tasks. Pers. Psychol. 2007, 60, 431–473. [Google Scholar] [CrossRef]
- Haidich, A.B. Meta-analysis in medical research. Hippokratia 2010, 14, 29–37. Available online: https://pubmed.ncbi.nlm.nih.gov/21487488 (accessed on 20 May 2022). [PubMed]
- Akkaya-Hocagil, T. Meta-analysis: Methods for health and experimental studies: ShahjahanKhanSpringerNature Singapore Pte. Ltd. 2020. pp. 293. Biometrics 2022, 78, 414. [Google Scholar] [CrossRef]
- Lin, L. Comparison of four heterogeneity measures for meta-analysis. J. Eval. Clin. Pr. 2020, 26, 376–384. [Google Scholar] [CrossRef]
- Davis, S.C.; Jankovitz, K.Z.; Rein, S. Physical Fitness and Cardiac Risk Factors of Professional Firefighters across the Career Span. Res. Q. Exerc. Sport 2002, 73, 363–370. [Google Scholar] [CrossRef]
- Perroni, F.; Tessitore, A.; Cortis, C.; Lupo, C.; D’artibale, E.; Cignitti, L.; Capranica, L. Energy Cost and Energy Sources During a Simulated Firefighting Activity. J. Strength Cond. Res. 2010, 24, 3457–3463. Available online: https://journals.lww.com/nsca-jscr/Fulltext/2010/12000/Energy_Cost_and_Energy_Sources_During_a_Simulated.34.aspx (accessed on 20 May 2022). [CrossRef] [PubMed]
- Misner, J.E.; A Plowman, S.; A Boileau, R. Performance differences between males and females on simulated firefighting tasks. J. Occup. Med. Off. Publ. Ind. Med Assoc. 1987, 29, 801–805. [Google Scholar]
- Fyock-Martin, M.B.; Erickson, E.K.; Hautz, A.H.; Sell, K.M.; Turnbaugh, B.L.; Caswell, S.V.; Martin, J.R. What do Firefighting Ability Tests Tell Us about Firefighter Physical Fitness? A Systematic Review of the Current Evidence. J. Strength Cond. Res. 2020, 34, 2093–2103. [Google Scholar] [CrossRef]
- Hauschild, V.D.; DeGroot, D.W.; Hall, S.M.; Grier, T.L.; Deaver, K.D.; Hauret, K.G.; Jones, B.H. Fitness tests and occupational tasks of military interest: A systematic review of correlations. Occup. Environ. Med. 2017, 74, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Lentz, L.; Randall, J.R.; Gross, D.P.; Senthilselvan, A.; Voaklander, D. The Relationship between Physical Fit-ness and Occupational Injury in Emergency Responders: A Systematic Review. Am. J. Ind. Med. 2019, 62, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Lakatta, E.G. Age-associated Cardiovascular Changes in Health: Impact on Cardiovascular Disease in Older Persons. Heart Fail. Rev. 2002, 7, 29–49. [Google Scholar] [CrossRef]
- Costantino, S.; Paneni, F.; Cosentino, F. Ageing, metabolism and cardiovascular disease. J. Physiol. 2016, 594, 2061–20733. [Google Scholar] [CrossRef]
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/American heart association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Mazic, S.; Lazic, J.S.; Dekleva, M.; Antic, M.; Soldatovic, I.; Djelic, M.; Nesic, D.; Acimovic, T.; Lazic, M.; Lazovic, B.; et al. The impact of elevated blood pressure on exercise capacity in elite athletes. Int. J. Cardiol. 2015, 180, 171–177. [Google Scholar] [CrossRef]
- Hawkins, S.A.; Vie, L.L.; Wolf, P.S.A.; Lester, P.B.; Whittaker, K.S.; Hawkins, J.N.; Perez, A.L. Measuring Job Performance in the Army: Insights from Evidence on Civilian Stress and Health. In Occupational Stress and Well-Being in Military Contexts; Harms, P.D., Perrewé, P.L., Eds.; Emerald Publishing Limited: Bingley, UK, 2018; Volume 16, pp. 49–68. ISBN 978-1-78756-184-7. [Google Scholar]
- Durand, G.; Tsismenakis, A.J.; Jahnke, S.A.; Baur, D.M.; Christophi, C.A.; Kales, S.N. Firefighters’ physical activity: Relation to fitness and cardiovascular disease risk. Med. Sci. Sports Exerc. 2011, 43, 1752–1759. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.C.; Au, C.T.; Lee, F.Y.; So, R.C.; Wong, J.P.; Mak, G.Y.; Chien, E.P.; McManus, A.M. Association between Leisure Time Physical Activity, Cardiopulmonary Fitness, Cardiovascular Risk Factors, and Cardiovascular Workload at Work in Firefighters. Saf. Health. Work 2015, 6, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Alves, A.J.; Viana, J.; Cavalcante, S.L.; Oliveira, N.L.; Duarte, J.A.; Mota, J.; Oliveira, J.; Ribeiro, F. Physical activity in primary and secondary prevention of cardiovascular disease: Overview updated. World J. Cardiol. 2016, 8, 575. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.M.; Christophi, C.A.; Cook, E.F.; Kales, S.N. Age-Related Decline in Cardiorespiratory Fitness among Career Firefighters: Modification by Physical Activity and Adiposity. J. Obes. 2012, 2012, 710903. [Google Scholar] [CrossRef] [PubMed]
- Barry, A.M.; Lyman, K.J.; Dicks, N.D.; Landin, K.D.; McGeorge, C.R.; Hackney, K.J.; Walch, T.J. Firefighters’ Physical Activity and Waist Circumference as Predictors of VO2max. J. Occup. Environ. Med. 2019, 61, 849–853. [Google Scholar] [CrossRef] [PubMed]
- Kirlin, L.K.; Nichols, J.F.; Rusk, K.; A Parker, R.; Rauh, M.J. The effect of age on fitness among female firefighters. Occup. Med. 2017, 67, 528–533. [Google Scholar] [CrossRef]
- Mayer, J.M.; Nuzzo, J.L.; Chen, R.; Quillen, W.S.; Verna, J.L.; Miro, R.; Dagenais, S. The Impact of Obesity on Back and Core Muscular Endurance in Firefighters. J. Obes. 2012, 2012, 729283. [Google Scholar] [CrossRef]
- Poston, W.S.C.; Haddock, C.K.; Jahnke, S.A.; Jitnarin, N.; Tuley, B.C.; Kales, S.N. The Prevalence of Overweight, Obesity, and Substandard Fitness in a Population-Based Firefighter Cohort. J. Occup. Environ. Med. 2011, 53, 266–273. [Google Scholar] [CrossRef]
- Nikolakaros, G.; Vahlberg, T.; Auranen, K.; Sillanmäki, L.; Venetoklis, T.; Sourander, A. Obesity, Underweight, and Smoking Are Associated with Worse Cardiorespiratory Fitness in Finnish Healthy Young Men: A Population-Based Study. Front. Public Health 2017, 5, 206. Available online: https://www.frontiersin.org/article/10.3389/fpubh.2017.00206 (accessed on 20 May 2022). [CrossRef]
- Mehta, R.K. Impacts of obesity and stress on neuromuscular fatigue development and associated heart rate variability. Int. J. Obes. 2015, 39, 208–213. [Google Scholar] [CrossRef]
- Strauss, M.; Foshag, P.; Jehn, U.; Brzęk, A.; Littwitz, H.; Leischik, R. Higher cardiorespiratory fitness is strongly associated with lower cardiovascular risk factors in firefighters: A cross-sectional study in a German fire brigade. Sci. Rep. 2021, 11, 2445. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L.; Haller, J.M.; Benedict, R.; Moore-Merrell, L. Cardiac Strain Associated with High-rise Firefighting. J. Occup. Environ. Hyg. 2015, 12, 213–221. [Google Scholar] [CrossRef]
- Berryman, P.; Lukes, E.; Drew-Nord, D.C.; Hong, O.; Froelicher, E.S. Cardiovascular Risk Factors among Career Firefighters. AAOHN J. 2009, 57, 415–422. [Google Scholar] [CrossRef]
- Choi, B.; Ko, S.; Kojaku, S. Resting heart rate, heart rate reserve, and metabolic syndrome in professional firefighters: A cross-sectional study. Am. J. Ind. Med. 2017, 60, 900–910. [Google Scholar] [CrossRef] [PubMed]
- Williams-Bell, F.M.; Villar, R.; Sharratt, M.T.; Hughson, R.L. Physiological Demands of the Firefighter Candidate Physical Ability Test. Med. Sci. Sports Exerc. 2009, 41, 653–662. [Google Scholar] [CrossRef]
- Lyons, J.; Allsopp, A.; Bilzon, J. Influences of body composition upon the relative metabolic and cardiovascular demands of load-carriage. Occup. Med. 2005, 55, 380–384. [Google Scholar] [CrossRef]
- Lali, H.; Bukmir, L.; Ferhatovi, M. Simulation of Working Conditions by Maximum Work Load on Firefighters. Coll. Antropol. 2007, 31, 153–158. [Google Scholar]
- García-Pinillos, F.; Ruiz-Ariza, A.; Del Castillo, R.M.; Latorre-Román, P.Á. Impact of limited hamstring flexibility on vertical jump, kicking speed, sprint, and agility in young football players. J. Sports Sci. 2015, 33, 1293–1297. [Google Scholar] [CrossRef]
- Butler, R.J.; Contreras, M.; Burton, L.C.; Plisky, P.J.; Goode, A.; Kiesel, K. Modifiable risk factors predict injuries in firefighters during training academies. Work 2013, 46, 11–17. [Google Scholar] [CrossRef]



| Question | Michaelides et al. [57] | Skinner et al. [30] | von Heimburg et al. [58] | Perroni et al. [59] | Schonfeld et al. [60] | Lindberg et al. [61] | Lindberg et al. [62] | Siddal et al. [28] | Xu et al. [63] | Stevenson et al. [64] | Myhre et al. [65] | Chizewski et al. [66] | Kleinberg et al. [67] | Elsner and Kolkhorst [68] | Ryan et al. [69] | von Heimburg et al. [70] | von Heimburg et al., [71] | Rhea et al. [42] | Sheaff et al. [72] | Michaelides et al. [73] | Saari et al. [74] | Windisch, et al. [75] | Misner et al. [76] | Williford et al. [77] | Davis et al. [78] | Nazari et al. [31] | Sothmann et al. [39] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Introduction | |||||||||||||||||||||||||||
| Clear aims/objectives | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Methods | |||||||||||||||||||||||||||
| Study design appropriate for the stated aim(s)? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Sample size justified? | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | ⨯ | 🗸 | 🗸 | 🗸 | 🗸 | ⨯ | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Target/reference population clearly defined? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | ⨯ | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Sample frame taken from an appropriate population base to closely represent the target population? | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | 🗸 | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | 🗸 | 🗸 | 🗸 | 🗸 |
| Selection process likely to select subjects that were representative of the target population? | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | 🗸 | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | 🗸 | ⨯ | ⨯ | 🗸 | 🗸 | 🗸 | 🗸 |
| Measures undertaken to address and categorize non-responders? | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | ⨯ | 🗸 | 🗸 | 🗸 | ⨯ | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Were the risk factor and outcome variables measured appropriate to the aims of the study? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Were the risk factor and outcome variables measured correctly using instruments/measurements that had been trialed, piloted or published previously? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Clear which tests were used to determine statistical significance and/or precision estimates? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Were the methods sufficiently described to enable them to be repeated? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Results | |||||||||||||||||||||||||||
| Were the basic data adequately described? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Does the response rate raise concerns about non-response bias? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| If appropriate, was information about non-responders described? | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Were the results internally consistent? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Were the results presented for all the analyses described in the methods? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Discussion | |||||||||||||||||||||||||||
| Were the authors’ discussions and conclusions justified by the results? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Were the limitations of the study discussed? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | ⨯ | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Other | |||||||||||||||||||||||||||
| Were there any funding sources or conflicts of interest that may affect the authors’ interpretation of the results? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Was ethical approval or consent of participants attained? | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| TOTAL SCORE | 15 | 15 | 15 | 15 | 15 | 15 | 15 | 16 | 16 | 16 | 16 | 17 | 17 | 17 | 17 | 17 | 17 | 17 | 17 | 17 | 17 | 17 | 18 | 19 | 19 | 19 | 19 |
| Quality Assessment Criteria | Phillips et al. [79] | MacDermid et al. [29] | Hendersen et al. [80] |
|---|---|---|---|
| 1. Did the study address a clearly focused issue? | 🗸 | 🗸 | 🗸 |
| 2. Was the cohort recruited in an acceptable way? | 🗸 | 🗸 | 🗸 |
| 3. Was the exposure accurately measured to minimize bias? | 🗸 | 🗸 | 🗸 |
| 4. Was the outcome accurately measured to minimize bias? | 🗸 | 🗸 | 🗸 |
| 5. (a) Have the authors identified all important confounding factors? | 🗸 | 🗸 | 🗸 |
| 5. (b) Have they taken account of the confounding factors in the design and/or analysis? | 🗸 | 🗸 | 🗸 |
| 6. (a) Was the follow up of subjects complete enough? | 🗸 | 🗸 | 🗸 |
| 6. (b) Was the follow up of subjects long enough? | 🗸 | 🗸 | 🗸 |
| 7. What are the results of this study? | NA | NA | NA |
| 8. How precise are the results? | NA | NA | NA |
| 9. Do you believe the results? | 🗸 | 🗸 | 🗸 |
| 10. Can the results be applied to the local population? | 🗸 | 🗸 | 🗸 |
| 11. Do the results of this study fit with other available evidence? | 🗸 | 🗸 | 🗸 |
| 12. What are the implications of this study for practice? | 🗸 | 🗸 | 🗸 |
| TOTAL SCORE | 12 | 12 | 12 |
| Outcome | No. of Studies | No. of Participants | R (95% CI) | Z Score | p (Overall Effect) | Heterogeneity I2; Cohen’s Q; p | Egger’s Test Intercept (95%CI); p | Begg’s Test (τ; p) |
|---|---|---|---|---|---|---|---|---|
| Age | 8 | 944 | 0.224 (0.162 to 0.284) | 3.834 | <0.001 ** | 74.1%; 27.0136; <0.001 | 2.33 (−2.36–7.02); 0.269 | 0.18; 0.529 |
| Five or more tasks | 5 | 639 | 0.199 (0.0425 to 0.346) | 2.484 | 0.004 ** | 71.1%; 13.85; 0.008 | 4.18 (−2.14–10.48); 0.126 | 0.53; 0.197 |
| Males only | 6 | 416 | 0.282 (0.167 to 0.390) | 4.675 | <0.001 ** | 32.5%; 7.41; 0.191 | 2.82 (−5.30–10.95); 0.389 | 0.41; 0.243 |
| Weight | 5 | 749 | 0.286 (0.0968 to 0.455) | 2.927 | 0.003 ** | 83.9%; 24.90; <0.001 | 3.69 (−6.39–13.77); 0.329 | 0.20; 0.624 |
| Full-time only | 5 | 327 | 0.323 (0.220 to 0.418) | 5.912 | <0.001 ** | 0.0%; 3.68; 0.452 | 1.47 (−0.70–9.95); 0.621 | 0.40; 0.327 |
| Obesity | 9 | 876 | 0.316 (0.254 to 0.375) | 6.432 | <0.001 ** | 54.5%; 17.59; 0.025 | 1.79 (−0.49–4.07); 0.106 | 0.14; 0.597 |
| Five or more tasks | 5 | 572 | 0.350 (0.184 to 0.496) | 4.007 | <0.001 ** | 71.8%; 14.18; 0.007 | 3.48 (−1.66–8.62); 0.120 | 0.60; 0.142 |
| Males only | 6 | 348 | 0.413 (0.319 to 0.498) | 7.933 | <0.001 ** | 0.0%; 5.65; 0.463 | 0.19 (−3.53–3.91); 0.901 | 0.09; 0.758 |
| Sequential testing | 6 | 614 | 0.368 (0.218 to 0.501) | 4.601 | <0.001 ** | 69.1%; 16.19; 0.006 | 3.43 (−0.01–6.88); 0.051 | 0.47; 0.189 |
| Weight of PPE | 7 | 770 | 0.354 (0.228 to 0.468) | 5.253 | <0.001 ** | 62.4%; 15.94; 0.014 | 1.72 (−1.44–4.89); 0.220 | 0.19; 0.538 |
| Full-time only | 6 | 512 | 0.388 (0.310 to 0.460) | 9.095 | <0.001 ** | 16.4%; 5.98; 0.308 | 0.54 (−3.21–4.28); 0.712 | 0.33; 0.348 |
| Heart rate | 2 | 110 | 0.398 (0.226 to 0.547) | 4.301 | <0.001 ** | 0.0%; 0.41; 0.521 | 2.74 (--); <0.001 | 1.00; 0.317 |
| Outcome | No. of Studies | No. of Participants | R (95% CI) | Z Score | p (Overall Effect) | Heterogeneity I2; Cohen’s Q; p | Egger’s Test Intercept (95%CI); p | Begg’s Test (τ; p) |
|---|---|---|---|---|---|---|---|---|
| Cardiorespiratory fitness | 11 | 946 | −0.584 (−0.671 to −0.482) | −9.132 | <0.001 ** | 72.9%; 36.96; <0.001 | −2.52 (−4.80 to 0.23); 0.034 | −0.18; 0.432 |
| Gas analysis | 5 | 207 | −0.672 (−0.743 to −0.587) | −11.295 | <0.001 | 0.0%; 3.98; 0.407 | 1.17 (−3.72 to 6.07); 0.501 | 0.40; 0.327 |
| Sequential tasks | 8 | 635 | −0.589 (−0.682 to −0.476) | −8.390 | <0.001 ** | 64.1%; 19.49; 0.007 | −2.05 (−4.65 to 0.53); 0.099 | −0.29; 0.322 |
| Five or more tasks | 6 | 525 | −0.571 (−0.680 to −0.438) | −7.074 | <0.001 ** | 61.9%; 13.11; 0.022 | −1.99 (−4.88 to 0.91); 0.129 | −0.33; 0.348 |
| Males | 7 | 281 | −0.596 (−0.675 to −0.505) | −10.260 | <0.001 ** | 9.9%; 6.66; 0.353 | −0.72 (−4.04 to 2.59); 0.599 | −0.19; 0.538 |
| Males and females | 4 | 665 | −0.566 (−0.709 to −0.378) | −5.161 | <0.001 ** | 88.2%; 25.46; <0.001 | −7.31 (−15.92 to 1.29); 0.067 | −0.33; 0.497 |
| Weight of PPE | 7 | 678 | −0.551 (−0.660 to −0.419) | −7.005 | <0.001 ** | 68.3%; 18.94; 0.004 | −2.15 (−4.61 to 0.31); 0.075 | −0.09; 0.758 |
| Full-time only | 7 | 449 | −0.605 (−0.729 to −0.443) | −6.094 | <0.001 ** | 75.0%; 24.0390; <0.001 | −2.39 (−0.60 to 1.25); 0.152 | 0.00; 1.000 |
| Upper body endurance | 6 | 387 | −0.344 (−0.430 to −0.251) | −6.886 | <0.001 ** | 0.0%; 3.49; 0.624 | 1.13 (−4.07 to 6.33); 0.579 | 0.33; 0.348 |
| Weight of PPE | 4 | 256 | −0.363 (−0.467 to −0.250) | −5.949 | <0.002 ** | 0.0%; 1.3; 0.770 | −7.6 (−8.63 to 7.11); 0.717 | −0.33; 0.497 |
| Full−time only | 4 | 268 | −0.324 (−0.430 to −0.209) | −5.318 | <0.001 ** | 1.9%; 3.06; 0.383 | 4.30 (−9.22 to 17.82); 0.305 | 0.33; 0.497 |
| Abdominal endurance | 8 | 871 | −0.308 (−0.367 to −0.246) | −9.256 | <0.001 ** | 0.0%; 3.62; 0.822 | −0.05 (−1.65 to 1.54); 0.939 | 0.14; 0.621 |
| Five or more tasks | 5 | 587 | −0.333 (−0.403 to −0.258) | −8.267 | <0.001 ** | 0.0%; 2.22; 0.696 | −0.9 (−3.33 to 3.13); 0.929 | 0.00; 1.000 |
| Sequential tasks | 5 | 254 | −0.320 (−0.428 to −0.202) | −5.121 | <0.001 ** | 0.0%; 1.60; 0.808 | 1.38 (−1.35 to 4.11); 0.206 | 0.60; 0.142 |
| Males only | 5 | 323 | −0.349 (−0.443 to −0.247) | −6.391 | <0.001 ** | 0.0%; 2.01; 0.733 | 2.24 (−1.36 to 5.8); 0.142 | 0.60; 0.142 |
| Weight of PPE | 5 | 740 | −0.296 (−0.361 to −0.229) | −8.212 | <0.001 ** | 0.0%; 2.38; 0.795 | 0.09 (−1.89 to 2.09); 0.089 | 0.07; 0.851 |
| Full-time only | 5 | 446 | −0.294 (−0.377 to −0.205) | −6.284 | <0.001 ** | 0.0%; 1.82; 0.768 | −0.52 (−3.22 to 2.18); 0.584 | 0.00; 1.000 |
| Grip strength | 6 | 258 | −0.421 (−0.602 to −0.198) | −5.086 | <0.001 ** | 68.6%; 15.92; 0.007 | 0.59 (−4.30 to 5.48); 0.754 | −0.07; 0.851 |
| Five or more tasks | 4 | 502 | −0.439 (−0.578 to −0.274) | −4.882 | <0.001 ** | 68.9%; 9.67; 0.022 | 1.39 (−9.64 to 12.42); 0.642 | 0.67; 0.174 |
| Males only | 5 | 258 | −0.421 (−0.602 to −0.198) | −3.542 | <0.001 ** | 71.1%; 13.84; 0.008 | 0.59 (−430 to 5.48); 0.754 | −0.07; 0.851 |
| Weight of PPE | 5 | 522 | −0.473 (−0.604 to −0.317) | −5.420 | <0.001 ** | 66.9%; 12.07; 0.017 | −0.11 (−6.30 to 6.09); 0.959 | −0.20; 0.624 |
| Full-time only | 4 | 225 | −0.406 (−0.625 to −0.127) | −2.790 | 0.005 ** | 77.5; 13.31; 0.004 | −1.38 (−21.05 to 18.29); 0.791 | 0.00; 1.000 |
| Upper body strength | 8 | 814 | −0.318 (−0.380 to −0.254) | −5.756 | <0.001 ** | 57.7%; 16.53; 0.207 | −1.51 (−4.29 to 1.27); 0.232 | −0.29; 0.320 |
| Five or more tasks | 5 | 530 | −0.374 (−0.446 to −0.298) | −8.931 | <0.001 ** | 5.1; 4.21; 0.378 | −1.26 (−4.36 to 1.85); 0.288 | −0.20; 0.624 |
| Sequential tasks | 6 | 572 | −0.357 (−0.428 to −0.283) | −8.802 | <0.001 ** | 28.7; 7.01; 0.219 | −0.42 (−3.82 to 2.98); 0.750 | −0.06; 0.851 |
| Males only | 6 | 286 | −0.421 (−0.540 to −0.266) | −5.183 | <0.001 ** | 42.4%; 8.68; 0.122 | −0.83 (−6.93 to 5.28); 0.726 | −0.20; 0.573 |
| Weight of PPE | 6 | 683 | −0.339 (−0.449 to −0.219) | −5.321 | <0.001 ** | 50.2; 10.04; 0.074 | −1.89 (−4.52 to 0.74); 0.116 | −0.60; 0.091 |
| Full-time only | 5 | 389 | −0.313 (−0.470 to −0.137) | −3.409 | 0.001 ** | 57.5%; 9.40; 0.052 | −2.40 (−6.17 to 1.37); 0.136 | −0.80; 0.050 |
| Lower body strength | 3 | 122 | −0.216 (−0.383 to −0.0349) | −2.331 | 0.020 * | 0.0%; 0.27; 0.876 | −0.22 (−12.99 to 12.55); 0.863 | −0.33; 0.602 |
| Five or more tasks | 2 | 102 | −0.201 (−0.383 to −0.003) | −1.992 | 0.046 * | 0.0%; 0.10; 0.749 | 1.01 (--); <0.001 | 1.00; 0.317 |
| Full-time only | 2 | 92 | −0.236 (−0.424 to −0.029) | −2.232 | 0.026 * | 0.0%; 0.10; 0.751 | −0.70 (--); <0.001 | −1.00; 0.317 |
| Flexibility | 4 | 233 | −0.099 (−0.227 to 0.032) | −1.479 | 0.139 | 0.0%; 2.05; 0.560 | −2.58 (−8.81 to 3.64); 0.216 | −0.67; 0.174 |
| Outcome | No. of Studies | No. of Participants | R (95% CI) | Z Score | p (Overall Effect) | Heterogeneity I2; Cohen’s Q; p | Egger’s test Intercept (95%CI); p | Begg’s Test (τ; p) |
|---|---|---|---|---|---|---|---|---|
| Obesity | ||||||||
| Stair climb | 6 | 304 | 0.489 (0.361 to 0.599) | 6.696 | <0.001 ** | 39.2%; 8.23; 0.144 | −1.98 (−6.92 to 2.97); 0.33 | −0.28; 0.44 |
| Five or more tasks | 2 | 160 | 0.537 (0.416 to 0.640) | 7.453 | <0.001 ** | 0.0%; 0.12; 0.729 | 3.43 (--); <0.001 | 1.00; 0.317 |
| Sequential tasks | 4 | 222 | 0.485 (0.375 to 0.581) | 7.670 | <0.001 ** | 36.8%; 4.75; 0.191 | −1.26 (−12.73 to 10.21); 0.682 | −0.33; 0.497 |
| Males only | 5 | 242 | 0.468 (0.308 to 0.577) | 7.654 | <0.001 ** | 33.6%; 6.02; 0.197 | −1.78 (−7.33 to 3.78); 0.383 | −0.32; 0.439 |
| Weight of PPE | 4 | 200 | 0.514 (0.401 to 0.611) | 7.789 | <0.001 ** | 0.0%; 2.07; 0.557 | −1.29 (−6.31 to 3.73); 0.385 | −0.18; 0.709 |
| Full-time only | 4 | 222 | 0.435 (0.259 to 0.583) | 4.543 | <0.001 ** | 48.9%; 5.8771; 0.118 | −3.45 (−11.86 to 4.96); 0.219 | −0.33; 0.497 |
| Hose drag | 5 | 242 | 0.241 (0.095 to 0.378) | 3.580 | <0.001 ** | 19.5%; 4.97; 0.290 | 1.54 (−3.59 to 6.66); 0.411 | 0.53; 0.197 |
| Five or more tasks | 2 | 160 | 0.231 (−0.004 to 0.442) | 1.926 | 0.054 | 55.8%; 2.26; 0.133 | 14.85 (--); <0.001 | 1.00; 0.317 |
| Sequential tasks | 4 | 222 | 0.249 (0.0702 to 0.412) | 2.710 | 0.007 ** | 39.6%; 4.97; 0.174 | 2.46 (−7.39 to 12.31); 0.395 | 0.67; 0.174 |
| Weight of PPE | 4 | 200 | 0.255 (0.117 to 0.383) | 3.577 | <0.001 ** | 31.5%; 4.38; 0.223 | 1.81 (−5.65 to 9.26); 0.407 | 0.55; 0.264 |
| Full-time only | 4 | 222 | 0.206 (0.073 to 0.3310 | 3.022 | 0.003 ** | 0.0%; 2.59; 0.458 | 0.27 (−8.63 to 9.18); 0.908 | 0.33; 0.497 |
| Victim drag | 5 | 242 | 0.254 (0.129 to 0.371) | 3.915 | <0.001 ** | 0.0%; 1.51; 0.825 | −0.35 (−3.51 to 2.81); 0.746 | −0.11; 0.796 |
| Five or more tasks | 2 | 160 | 0.280 (0.129 to 0.419) | 3.575 | <0.001 ** | 0.0%; 0.22; 0.639 | 4.52 (--); <0.001 | 1.00; 0.317 |
| Sequential tasks | 4 | 222 | 0.244 (0.113 to 0.366) | 3.601 | <0.001 ** | 0.0%; 1.15; 0.765 | −1.45 (−5.45 to 2.56); 0.261 | −0.33; 0.497 |
| Males only | 5 | 242 | 0.254 (0.129 to 0.371) | 3.915 | <0.001 ** | 0.0%; 1.51; 0.825 | −0.35 (−3.51 to 2.81); 0.746 | −0.11; 0.796 |
| Weight of PPE | 4 | 200 | 0.275 (0.138 to 0.401) | 3.864 | <0.001 ** | 0.0%; 0.99; 0.805 | −0.16 (−4.53 to 4.2); 0.886 | 0.18; 0.709 |
| Full-time only | 4 | 222 | 0.266 (0.136 to 0.386) | 3.946 | <0.001 ** | 0.0%; 1.08; 0.782 | 0.38 (−5.27 to 6.03); 0.801 | 0.00; 1.000 |
| Forcible entry | 2 | 160 | 0.285 (0.135 to 0.423) | 3.639 | <0.001 ** | 24.1%; 0.1.32; 0.251 | 11.51 (--); <0.001 | 1.00; 0.317 |
| Equipment hoist | 2 | 111 | 0.197 (0.008 to 0.372) | 2.044 | 0.041 * | 0.0%; 0.65; 0.419 | −1.58 (--); <0.001 | −1.00; 0.317 |
| Age | ||||||||
| Stair climb | 4 | 324 | 0.345 (0.166 to 0.502) | 3.669 | <0.001 ** | 62.3%; 7.74; 0.052 | 2.72 (−9.94 to 15.38); 0.453 | 0.33; 0.497 |
| Sequential tasks | 2 | 133 | 0.431 (0.280 to 0.562 | 5.201 | <0.001 ** | 7.7; 1.08; 0.298 | −3.74 (--); <0.001 | −1.00; 0.317 |
| Full-time male firefighters | 3 | 174 | 0.434 (0.302 to 0.549) | 5.963 | <0.001 ** | 0.0%; 1.09; 0.581 | −2.26 (−27.04 to 22.53); 0.454 | −0.33; 0.602 |
| Hose drag | 3 | 222 | 0.0403 (0.094 to 0.173) | 0.589 | 0.556 | 0.0%; 0.26; 0.889 | 0.46 (−19.37 to 20.29); 0.817 | −0.33; 0.602 |
| Victim rescue | 3 | 222 | 0.147 (−0.079 to 0.359) | 1.280 | 0.200 | 62.8%; 5.37; 0.068 | 6.62 (−44.75 to 57.99); 0.349 | 0.33; 0.602 |
| Forcible entry | 2 | 180 | 0.0318 (−0.116 to 0.178) | 0.419 | 0.675 | 0.0%; 0.08; 0.771 | 35.74 (--); <0.001 | 1.00; 0.317 |
| Outcome | No. of Studies | No. of Participants | R (95% CI) | Z Score | p (Overall Effect) | Heterogeneity I2; Cohen’s Q; p-Value | Egger’s test Intercept (95%CI); p | Begg’s Test (τ; p) |
|---|---|---|---|---|---|---|---|---|
| Cardiorespiratory fitness | ||||||||
| Stair climb | 4 | 351 | −0.421 (−0.639 to −0.140 | −2.856 | 0.004 ** | 82.9%; 17.55;<0.001 | 4.39 (−4.24 to 13.03); 0.159 | 0.33; 0.497 |
| Sequential testing | 3 | 302 | −0.451 (−0.702 to −0.100) | −2.472 | 0.013 * | 85.4%; 13.69; 0.001 | −8.39 (−254.21 to 237.44); 0.739 | −0.33; 0.602 |
| Weight of PPE | 3 | 309 | −0.513 (−0.680 to −0.296) | −4.244 | <0.001 ** | 70.7%; 6.81; 0.033 | 3.13 (−23.58 to 29.83); 0.377 | 0.33; 0.602 |
| Full-time only | 2 | 91 | −0.214 (−0.406 to −0.005) | −2.007 | 0.045 * | 5.8%; 1.06; 0.303 | 17.68 (--); <0.001 | 1.00; 0.317 |
| Hose drag | 3 | 180 | −0.197 (−0.376 to −0.004) | −1.997 | 0.046 * | 38.1%; 3.23; 0.198 | 3.64 (−55.99 to 63.26); 0.580 | 1.00; 0.117 |
| Five or more and Sequential | 2 | 131 | −0.138 (−0.415 to 0.163) | −0.897 | 0.370 | 61.9%; 2.62; 0.105 | 5.98 (--); <0.001 | 1.00; 0.317 |
| Weight of PPE | 2 | 138 | −0.278 (−0.427 to −0.114) | −3.279 | 0.001 ** | 0.0%; 0.04; 0.839 | 0.93 (--); <0.001 | −1.00; 0.317 |
| Victim drag | 4 | 391 | −0.356 (−0.500 to −0.194) | −4.146 | <0.001 ** | 57.1; 6.99; 0.072 | 2.09 (−6.87 to 11.05); 0.421 | 0.33; 0.497 |
| Five or more tasks | 2 | 127 | −0.384 (−0.525 to −0.223) | −4.450 | <0.001 | 0.0%; 0.69; 0.406 | −2.72 (--); <0.001 | −1.00; 0.317 |
| Sequential tasks | 3 | 169 | −0.300 (−0.504 to −0.066) | −2.488 | 0.013 * | 55.6%; 4.50; 0.105 | 0.88 (−73.51 to 75.27); 0.905 | −0.33; 0.602 |
| Males only | 2 | 131 | −0.220 (−0.482 to 0.079) | −1.449 | 0.147 | 61.6%; 2.60; 0.107 | 5.95 (--); <0.001 | 1.00; 0.317 |
| Weight of PPE | 2 | 260 | −0.452 (−0.544 to −0.349) | −7.757 | <0.001 ** | 0.0%; 0.05; 0.817 | −4.41 (--); <0.001 | −1.00; 0.317 |
| Full-time only | 3 | 353 | −0.320 (−0.501 to −0.113) | −2.977 | 0.003 ** | 69.3%; 6.61; 0.039 | 4.37 (−6.36 to 15.14); 0.122 | 1.00; 0.117 |
| Saw hold | 2 | 80 | 0.301 (−0.601 to 0.074) | −1.580 | 0.114 | 64.8%; 2.84; 0.092 | −44.09 (--); <0.001 | −1.00; 0.317 |
| Upper body endurance | ||||||||
| Stair climb | 3 | 205 | −0.408 (−0.518 to −0.285) | −6.061 | <0.001 ** | 0.0%; 1.28; 0.527 | 3.93 (−9.22 to 17.07); 0.164 | 1.00; 0.1172 |
| Weight of PPE | 2 | 163 | −0.436 (−0.553 to −0.301) | −5.850 | <0.001 ** | 0.0%; 0.37; 0.541 | 7.13 (--); <0.001 | 1.00; 0.3173 |
| Hose drag | 4 | 294 | −0.290 (−0.393 to −0.180) | −5.010 | <0.001 ** | 0.0%; 0.56; 0.905 | −2.15 (−6.03 to 1.72); 0.139 | −0.33; 0.497 |
| Weight of PPE | 2 | 205 | −0.290 (−0.413 to −0.157) | −4.183 | <0.001 ** | 0.0%; 0.56; 0.754 | 0.78 (--); <0.001 | 1.00; 0.317 |
| Full-time only | 3 | 163 | −0.266 (−0.404 to −0.115) | −3.410 | 0.001 ** | 0.0%; 0.00; 0.947 | −2.48 (−15.86 to 10.89); 0.256 | −0.33; 0.602 |
| Victim rescue | 4 | 294 | −0.200 (−0.363 to −0.025) | −2.23 | 0.026 * | 55.2%; 6.69; 0.083 | 4.01 (−19.23 to 27.24); 0.536 | 0.67; 0.174 |
| Weight of PPE | 2 | 163 | −0.197 (−0.537 to 0.197) | −0.980 | 0.327 | 84.5%; 6.44; 0.011 | 29.60 (--); <0.001 | 1.00; 0.317 |
| Full-time only | 3 | 205 | −0.183 (−0.420 to 0.077) | −1.383 | 0.167 | 69.9; 6.63; 0.036 | 4.30 (−99.57 to 108.17); 0.692 | 0.33; 0.602 |
| Forcible entry | 3 | 252 | −0.247 (−0.407 to −0.072) | −2.743 | 0.006 ** | 51.1%; 4.09; 0.129 | 21.43 (−25.53 to 68.39); 0.109 | 1.00; 0.117 |
| Weight of PPE and full-time | 2 | 163 | −0.220 (−0.488 to 0.086) | −1.411 | 0.158 | 74.3%; 3.88; 0.049 | 22.98 (--); <0.001 | 1.00; 0.317 |
| Abdominal endurance | ||||||||
| Stair climb | 5 | 262 | −0.415 (−0.512 to −0.306) | −6.933 | <0.001 ** | 25.7%; 5.38; 0.250 | 1.51 (−5.21 to 8.22); 0.526 | 0.00; 1.00 |
| Five or more tasks and sequential | 3 | 200 | −0.472 (−0.574 to −0.354) | −7.079 | <0.001 ** | 0.0%; 1.12; 0.572 | −3.07 (−21.12 to 14.99); 0.276 | −1.00; 0.117 |
| Full-time Males firefighters | 3 | 224 | −0.388 (−0.496 to −0.268) | −5.962 | <0.001 ** | 22.8%; 3.88; 0.274 | 2.53 (−5.17 to 10.23); 0.293 | 0.33; 0.497 |
| Weight of PPE | 4 | 220 | −0.452 (−0.554 to −0.338) | −7.035 | <0.001 ** | 0.0%; 2.52; 0.473 | 4.73 (−49.98 to 59.44); 0.470 | 0.33; 0.602 |
| Hose drag | 5 | 313 | −0.230 (−0.334 to −0.120) | −4.034 | <0.001 ** | 17.3%; 4.83; 0.305 | 2.61 (−2.40 to 7.62); 0.196 | 0.40; 0.327 |
| Five or more tasks | 3 | 251 | −0.253 (−0.367 to −0.132) | −4.029 | <0.001 ** | 0.0%; 1.05; 1.000 | −5.72 (−116.29 to 104.85); 0.629 | −0.33; 0.602 |
| Sequential tasks | 4 | 293 | −0.256 (−0.361 to −0.143) | −4.381 | <0.001 ** | 0.0%; 1.06; 0.786 | −0.92 (−10.99 to 9.14); 0.732 | 0.00; 1.00 |
| Weight of PPE | 2 | 182 | −0.157 (−0.367 to 0.068) | −1.374 | 0.169 | 48.8%; 3.91; 0.142 | 3.11 (25.36 to 31.59); 0.397 | 0.33; 0.602 |
| Full-time firefighters | 4 | 224 | −0.201 (−0.326 to −0.069) | −2.961 | 0.003 ** | 27.9%; 4.16; 0.245 | 2.41 (−6.16 to 10.97); 0.350 | 0.33; 0.497 |
| Victim drag | 6 | 351 | −0.151 (−0.290 to −0.006) | −2.044 | 0.041 * | 41.4%; 8.52; 0.129 | 1.01 (−5.24 to 7.27); 0.677 | 0.33; 0348 |
| Five or more Tasks | 4 | 289 | −0.189 (−0.342 to −0.027) | −2.276 | 0.023 | 46.6%; 5.62; 0.132 | −3.96 (−21.81 to 13.89); 0.441 | 0.00; 1.00 |
| Sequential tasks | 5 | 331 | −0.176 (−0.281 to −0.068) | −3.165 | 0.002 ** | 29.1%; 5.64; 0.228 | −2.37 (−11.97 to 7.22); 0.489 | 0.00; 1.00 |
| Males only | 4 | 271 | −0.113 (−0.231 to 0.008) | −1.834 | 0.067 | 34.3%; 4.57; 0.206 | 3.33 (-.345 to 10.12); 0.169 | 1.00; 0.042 |
| Weight of PPE | 4 | 220 | −0.137 (−0.366 to 0.108) | −1.098 | 0.272 | 64.7%; 8.50; 0.037 | 1.16 (−14.11 to 16.44) | 0.33; 0.497 |
| Full-time | 4 | 224 | −0.0845 (−0.248 to 0.084) | −0.984 | 0.325 | 30.4%; 4.31; 0.230 | 2.58 (−5.77 to 10.93); 0.315 | 0.67; 0.174 |
| Forcible entry | 3 | 251 | −0.195 (−0.313 to −0.072) | −3.081 | 0.002 ** | 0.0%; 1.39; 0.499 | 11.35 (−35.85 to 58.56); 0.201 | 0.33; 0.602 |
| Weight of PPE | 2 | 162 | −0.160 (−0.308 to −0.004) | −2.012 | 0.044 * | 0.0%; 0.79; 0.374 | 9.78 (--); <0.001 | 1.00; 0.317 |
| Equipment hoist | 2 | 111 | −0.168 (−0.400 to 0.167) | −0.844 | 0.399 | 37.1%; 1.59; 0.207 | 2.48 (--); <0.001 | 1.00; 0.317 |
| Saw hold | 2 | 80 | 0.252 (−0.300 to −0.677) | −0.891 | 0.373 | 83.8%; 6.17; 0.013 | 64.96 (--); <0.001 | 1.00; 0.317 |
| Grip strength | ||||||||
| Stair climb | 6 | 312 | −0.200 (−0.502 to 0.071) | −1.510 | 0.131 | 85.5%; 34.49;<0.0001 | −2.29 (−15.69 to 11.10); 0.348 | −0.33; 0.348 |
| Hose drag | 5 | 274 | −0.378 (−0.589 to −0.119) | −2.806 | 0.005 ** | 78.9%; 19.00;<0.001 | −3.97 (−16.26 to 8.33); 0.379 | 0.00; 1.00 |
| Five or more tasks | 2 | 163 | −0.325 (−0.496 to −0.129) | −3.188 | 0.001 ** | 42.5%; 1.74; 0.188 | 15.38 (--); <0.001 | 1.00; 0.317 |
| Males only | 4 | 225 | −0.429 (−0.668 to −0.108) | −2.566 | 0.010 * | 83.3%; 17.92; <0.001 | −3.69 (−24.39 to 17.01); 0.524 | 0.00; 1.00 |
| Weight of PPE | 4 | 232 | −0.442 (−0.666 to −0.145) | −2.834 | 0.005 ** | 81.8%; 16.45;<0.001 | −5.37 (−21.79 to 11.06); 0.295 | −0.33; 0.497 |
| Victim rescue | 5 | 263 | −0.578 (−0.713 to −0.402) | −5.545 | <0.001 ** | 68.2%; 12.56; 0.014 | −2.11 (−12.47 to 8.25); 0.563 | −0.40; 0.327 |
| Five or more tasks | 3 | 201 | −0.610 (−0.773 to −0.372) | −4.366 | <0.001 ** | 78.8%; 9.43; 0.009 | −6.89 (−95.23 to 81.44); 0.503 | −0.33; 0.602 |
| Sequential tasks | 4 | 243 | −0.561 (−0.716 to −0.353) | −4.697 | <0.001 ** | 74.7%; 11.84; 0.008 | −2.44 (−29.09 to 24.22); 0.732 | −0.33; 0.497 |
| Full-time male firefighters | 4 | 225 | −0.507 (−0.600 to −0.401) | −8.152 | <0.001 ** | 35.5; 4.65; 0.199 | −0.51 (−12.29 to 11.27); 0.869 | 0.00; 1.00 |
| Weight of PPE | 4 | 221 | −0.621 (−0.758 to −0.432) | −5.388 | <0.001 ** | 69.6%; 9.86; 0.019 | −3.07 (−17.08 to 10.93); 0.445 | −0.33; 0.497 |
| Forcible entry | 2 | 163 | −0.426 (−0.623 to −0.179) | −3.248 | 0.001 ** | 67.2; 3.05; 0.081 | 20.36 (--); <0.001 | 1.00; 0.317 |
| Equipment hoist | 2 | 111 | −0.420 (−0.703 to −0.023) | −2.066 | 0.039 * | 64.8%; 2.84; 0.092 | 3.29 (--); <0.001 | 1.00; 0.317 |
| Saw hold | 2 | 80 | 0.468 (−0.0836 to 0.800) | 1.682 | 0.093 | 85.1%; 6.70; 0.009 | 67.71 (--); <0.001 | 1.00; 0.317 |
| Upper body strength | ||||||||
| Stair climb | 3 | 134 | −0.140 (−0.306 to 0.035) | −1.571 | 0.116 | 0.0%; 1.45; 0.484 | −2.33 (−17.66 to 12.99); 0.304 | −1.00; 0.117 |
| Hose drag | 3 | 134 | −0.544 (−0.748 to −0.247) | −3.337 | 0.001 ** | 71.9%; 7.11; 0.029 | −5.71 (19.89 to 8.48); 0.123 | −1.00; 0.117 |
| Five or more tasks | 2 | 114 | −0.402 (−0.547 to −0.233) | −4.421 | <0.001 ** | 0.0%; 0.45; 0.502 | −3.38 (--); <0.001 | −1.00; 0.317 |
| Weight of PPE | 2 | 92 | −0.609 (−0.888 to −0.002) | −1.966 | 0.049 * | 85.9%; 7.10; 0.008 | −5.91 (--); <0.001 | −1.00; 0.317 |
| Victim rescue | 3 | 134 | −0.350 (−0.573 to −0.080) | −2.512 | 0.012 * | 56.1%; 4.55; 0.103 | −3.10 (−47,24 to 41.04); 0.536 | −0.33; 0.602 |
| Five or more tasks | 2 | 114 | −0.255 (−0.422 to −0.073) | −2.715 | 0.007 ** | 0.0%; 0.67; 0.412 | 4.13 (--); <0.001 | 1.00; 0.317 |
| Weight of PPE | 2 | 92 | −0.461 (−0.733 to −0.064) | −2.248 | 0.025 * | 64.6%; 2.82; 0.093 | −3.72 (--); <0.001 | −1.00; 0.317 |
| Lower body strength | ||||||||
| Stair climb | 5 | 329 | −0.0460 (−0.155 to 0.064) | −0.817 | 0.414 | 0.0%; 1.54; 0.819 | −0.64 (−3.45 to 2.17); 0.522 | −0.20; 0.624 |
| Hose drag | 4 | 179 | −0.244 (−0.381 to −0.097) | −3.223 | 0.001 ** | 0.0%; 1.72; 0.632 | −1.92 (−8.87 to 5.03); 0.357 | 0.00; 1.00 |
| five or more tasks | 2 | 110 | −0.222 (−0.395 to −0.033) | −2.298 | 0022 * | 0.0%; 0.29; 0.591 | 2.71 (--); <0.001 | 1.00; 0.317 |
| Weight of PPE | 3 | 137 | −0.271 (−0.422 to −0.104) | −3.139 | 0.002 ** | 0.0%; 1.29; 0.525 | −2.19 (−20.28 to 15.90); 0.367 | −0.33; 0.602 |
| Victim rescue | 3 | 130 | −0.254 (−0.411 to −0.081) | −2.851 | 0.004 ** | 0.0%; 0.29; 0.862 | −0.93 (−11.45 to 9.60); 0.462 | −0.33; 0.602 |
| five or more tasks | 2 | 110 | −0.246 (−0.416 to −0.059) | −2.559 | 0.010 * | 0.0%; 0.25; 0.619 | −2.79 (--); <0.001 | −1.00; 0.317 |
| Weight of PPE | 2 | 88 | −0.229 (−0.422 to −0.017) | −2.111 | 0.035 * | 0.0%; 0.13; 0.724 | −0.81 (--); <0.001 | −1.00; 0.317 |
| Flexibility | ||||||||
| Stair climb | 2 | 133 | −0.190 (−0.351 to −0.019) | −1.959 | 0.030 * | 11.4%; 1.13; 0.288 | 3.82 (--); <0.001 | 1.00; 0.317 |
| Hose drag | 3 | 222 | −0.130 (−0.259 to 0.004) | −1.908 | 0.056 | 0.0%; 0.94; 0.626 | −2.55 (−28.08 to 22.98); 0.425 | −1.00; 0.012 |
| Victim rescue | 3 | 222 | −0.0792 (−0.210 to 0.055) | −1.159 | 0.247 | 0.0%; 1.67; 0.434 | −4.09 (−22.07 to 13.89); 0.212 | −1.00; 0.117 |
| Forcible entry | 2 | 180 | −0.0700 (−0.215 to 0.078) | −0.924 | 0.355 | 0.0%; 0.66; 0.418 | 99.59 (--); <0.001 | 1.00; 0.317 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ras, J.; Kengne, A.P.; Smith, D.L.; Soteriades, E.S.; November, R.V.; Leach, L. Effects of Cardiovascular Disease Risk Factors, Musculoskeletal Health, and Physical Fitness on Occupational Performance in Firefighters—A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 11946. https://doi.org/10.3390/ijerph191911946
Ras J, Kengne AP, Smith DL, Soteriades ES, November RV, Leach L. Effects of Cardiovascular Disease Risk Factors, Musculoskeletal Health, and Physical Fitness on Occupational Performance in Firefighters—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(19):11946. https://doi.org/10.3390/ijerph191911946
Chicago/Turabian StyleRas, Jaron, Andre P. Kengne, Denise L. Smith, Elpidoforos S. Soteriades, Rucia V. November, and Lloyd Leach. 2022. "Effects of Cardiovascular Disease Risk Factors, Musculoskeletal Health, and Physical Fitness on Occupational Performance in Firefighters—A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 19: 11946. https://doi.org/10.3390/ijerph191911946