
Alcohol Consumption and Adiposity: A Longitudinal Analysis of 45,399 UK Biobank Participants

Abstract
:1. Introduction
2. Materials and Methods
2.1. Outcomes
2.2. Alcohol Consumption
2.3. Baseline Covariates
2.4. Statistical Analysis
- (a)
- Repeated all main models in the sub-sample of participants who had data across all adiposity outcomes (n = 17,443).
- (b)
- Repeated all main models after excluding underweight (BMI < 18.5 kg/m2) participants at baseline as underweight status might reflect undiagnosed chronic illness.
- (c)
- Repeated all main models by adjusting for energy intake instead of vegetable and fruit consumption as a proxy for dietary quality.
- (d)
- Repeated all main models after excluding non-current drinkers and using 1st quartile of alcohol consumption as a reference.
- (e)
- Repeated all main models with an alternative alcohol categorization we have used before [25] that is based on lifetime drinking status and the UK alcohol consumption guideline (never drinkers, previous drinkers, occasional drinkers, current drinkers within guideline (<14 UK unit/week), within doubled guideline (14 ≤ 28 UK unit/week), and above doubled guideline (≥28 UK unit/week).
- (f)
- Multiple logistic regression models to examine the associations between total alcohol consumption and type-specific alcohol consumption with incidence of overweight (BMI ≥ 25.0 kg/m2) and obesity (BMI ≥ 30.0 kg/m2). For this analysis, we excluded participants with baseline overweight or obesity. We adjusted the model for baseline age, socioeconomic status, smoking status, major illness, sleep, PA, sitting time, and fruit and vegetable consumption. In type-specific analyses, models were further adjusted for total alcohol consumption.
3. Results
3.1. Overall Alcohol Consumption Volume
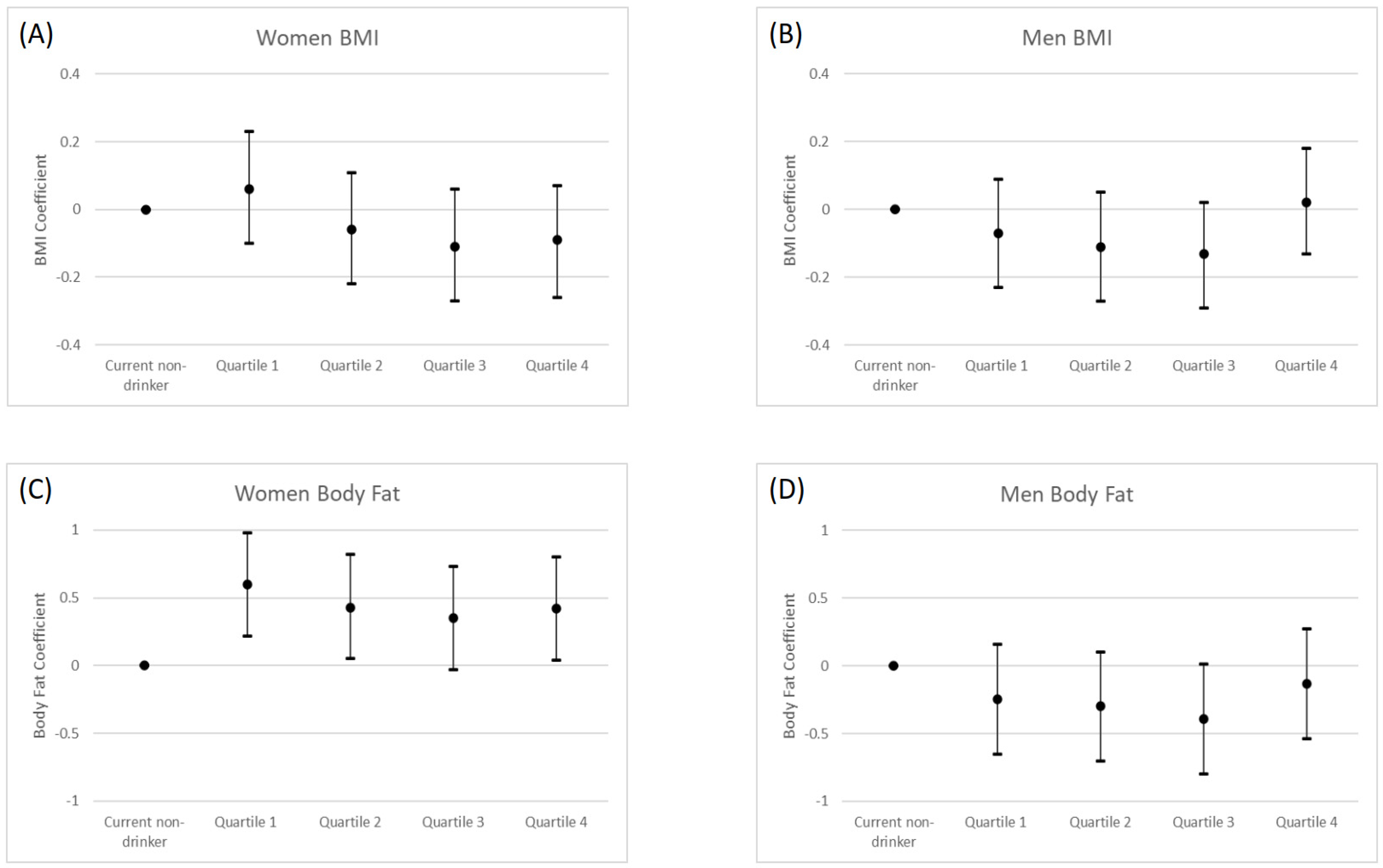
3.1.1. General Adiposity
3.1.2. Central Adiposity
3.2. Individual Types of Drinks
3.2.1. General Adiposity
3.2.2. Central Adiposity
3.3. Incidence of Obesity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ronksley, P.E.; Brien, S.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Association of alcohol consumption with selected cardiovascular disease outcomes: A systematic review and meta-analysis. BMJ 2011, 342, d671. [Google Scholar] [CrossRef] [PubMed]
- Baliunas, D.O.; Taylor, B.J.; Irving, H.; Roerecke, M.; Patra, J.; Mohapatra, S.; Rehm, J. Alcohol as a risk factor for type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2009, 32, 2123–2132. [Google Scholar] [CrossRef] [PubMed]
- Boffetta, P.; Hashibe, M. Alcohol and cancer. Lancet Oncol. 2006, 7, 149–156. [Google Scholar] [CrossRef]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Suter, P.M.; Tremblay, A. Is alcohol consumption a risk factor for weight gain and obesity? Crit. Rev. Clin. Lab. Sci. 2005, 42, 197–227. [Google Scholar] [CrossRef] [PubMed]
- Yeomans, M.R. Effects of alcohol on food and energy intake in human subjects: Evidence for passive and active over-consumption of energy. Br. J. Nutr. 2004, 92, S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Lukasiewicz, E.; Mennen, L.I.; Bertrais, S.; Arnault, N.; Preziosi, P.; Galan, P.; Hercberg, S. Alcohol intake in relation to body mass index and waist-to-hip ratio: The importance of type of alcoholic beverage. Public Health Nutr. 2005, 8, 315–320. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Sharper, A.G.; Whincup, P.H. Alcohol and adiposity: Effects of quantity and type of drink and time relation with meals. Int. J. Obes. 2005, 29, 1436–1444. [Google Scholar] [CrossRef]
- Butler, L.; Popkin, B.M.; Poti, J.M. Associations of Alcoholic Beverage Consumption with Dietary Intake, Waist Circumference, and Body Mass Index in US Adults: National Health and Nutrition Examination Survey 2003–2012. J. Acad. Nutr. Diet. 2018, 118, 409–420. [Google Scholar] [CrossRef]
- Downer, M.K.; Bertoia, M.L.; Mukamal, K.J.; Rimm, E.B.; Stampfer, M.J. Change in alcohol intake in relation to weight change in a cohort of US men with 24 years of follow-up. Obesity 2017, 25, 1988–1996. [Google Scholar] [CrossRef] [Green Version]
- Poudel, P.; Ismailova, K.; Andersen, L.B.; Larsen, S.C.; Heitmann, B.L. Adolescent wine consumption is inversely associated with long-term weight gain: Results from follow-up of 20 or 22 years. Nutr. J. 2019, 18, 1–7. [Google Scholar] [CrossRef]
- Tolstrup, J.S.; Halkjær, J.; Heitmann, B.L.; Tjønneland, A.M.; Overvad, K.; Sørensen, T.I.; Grønbæk, M.N. Alcohol drinking frequency in relation to subsequent changes in waist circumference. Am. J. Clin. Nutr. 2008, 87, 957–963. [Google Scholar] [CrossRef]
- French, M.T.; Norton, E.C.; Fang, H.; Maclean, J.C. Alcohol consumption and body weight. Health Econ. 2010, 19, 814–832. [Google Scholar] [CrossRef]
- Romaguera, D.; Ängquist, L.; Du, H.; Jakobsen, M.U.; Forouhi, N.G.; Halkjær, J.; Feskens, E.J.M.; van der A, D.L.; Masala, G.; Steffen, A.; et al. Dietary determinants of changes in waist circumference adjusted for body mass index–a proxy measure of visceral adiposity. PLoS ONE 2010, 5, e11588. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Shaper, A.G. Alcohol, body weight, and weight gain in middle-aged men. Am. J. Clin. Nutr. 2003, 77, 1312–1317. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Field, A.E.; Colditz, G.A.; Rimm, E.B. Alcohol intake and 8-year weight gain in women: A prospective study. Obes. Res. 2004, 12, 1386–1396. [Google Scholar] [CrossRef]
- MacInnis, R.J.; Hodge, A.M.; Dixon, H.G.; Peeters, A.; Johnson, L.E.; English, D.R.; Giles, G.G. Predictors of increased body weight and waist circumference for middle-aged adults. Public Health Nutr. 2014, 17, 1087–1097. [Google Scholar] [CrossRef]
- Traversy, G.; Chaput, J.P. Alcohol consumption and obesity: An update. Curr. Obes. Rep. 2015, 4, 122–130. [Google Scholar] [CrossRef]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [Green Version]
- Vasold, K.L.; Parks, A.C.; Phelan, D.M.; Pontifex, M.B.; Pivarnik, J.M. Reliability and Validity of Commercially Available Low-Cost Bioelectrical Impedance Analysis. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 406–410. [Google Scholar] [CrossRef]
- Caulfield, M.; Munroe, P.; Pembroke, J.; Samani, N.; Dominiczak, A.; Brown, M.; Webster, C.; Ratcliffe, P.; O’Shea, S.; Papp, J.; et al. Genome-wide mapping of human loci for essential hypertension. Lancet 2003, 361, 2118–2123. [Google Scholar] [CrossRef]
- Powell, L.; Feng, Y.; Duncan, M.J.; Hamer, M.; Stamatakis, E. Does a physically active lifestyle attenuate the association between alcohol consumption and mortality risk? Findings from the UK biobank. Prev. Med. 2020, 130, 105901. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Townsend, P.; Phillimore, P.; Beattie, A. Health and Deprivation: Inequality and the North; Croom Helm: London, UK, 1988. [Google Scholar]
- Perreault, K.; Bauman, A.; Johnson, N.; Britton, A.; Rangul, V.; Stamatakis, E. Does physical activity moderate the association between alcohol drinking and all-cause, cancer and cardiovascular diseases mortality? A pooled analysis of eight British population cohorts. Br. J. Sports Med. 2017, 51, 651–657. [Google Scholar] [CrossRef]
- Sammel, M.D.; Grisso, J.A.; Freeman, E.W.; Hollander, L.; Liu, L.; Liu, S.; Nelson, D.B.; Battistini, M. Weight gain among women in the late reproductive years. Fam. Pract. 2003, 20, 401–409. [Google Scholar] [CrossRef]
- Koh-Banerjee, P.; Chu, N.-F.; Spiegelman, D.; Rosner, B.; Colditz, G.; Willett, W.; Rimm, E. Prospective study of the association of changes in dietary intake, physical activity, alcohol consumption, and smoking with 9-y gain in waist circumference among 16 587 US men. Am. J. Clin. Nutr. 2003, 78, 719–727. [Google Scholar] [CrossRef]
- Stevens, J.; Katz, E.G.; Huxley, R.R. Associations between gender, age and waist circumference. Eur. J. Clin. Nutr. 2010, 64, 6–15. [Google Scholar] [CrossRef]
- Colditz, G.A.; Giovannucci, E.; Rimm, E.B.; Stampfer, M.J.; Rosner, B.; Speizer, F.E.; Gordis, E.; Willett, W.C. Alcohol in relation to diet and obesity in women and men. Am. J. Clin. Nutr. 1991, 54, 49–55. [Google Scholar] [CrossRef]
- Sayon-Orea, C.; Bes-Rastrollo, M.; Nunez-Cordoba, J.M.; Basterra-Gortari, F.J.; Buenza, J.J.; Martinez-Gonzalez, M.A. Type of alcoholic beverage and incidence of overweight/obesity in a Mediterranean cohort: The SUN project. Nutrition 2011, 27, 802–808. [Google Scholar] [CrossRef]
- Ruidavets, J.B.; Bataille, V.; Dallongeville, J.; Simon, C.; Bingham, A.; Amouyel, P.; Arveiler, D.; Ducimetière, P.; Ferrières, J. Alcohol intake and diet in France, the prominent role of lifestyle. Eur. Heart J. 2004, 25, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Vadstrup, E.S.; Petersen, L.; Sørensen, T.I.A.; Grønbaek, M. Waist circumference in relation to history of amount and type of alcohol: Results from the Copenhagen City Heart Study. Int. J. Obes. 2003, 27, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Halkjær, J.; Tjønneland, A.; Thomsen, B.L.; Overvad, K.; Sørensen, T.I. Intake of macronutrients as predictors of 5-y changes in waist circumference. Am. J. Clin. Nutr. 2006, 84, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Schütze, M.; Schulz, M.; Steffen, A.; Bergmann, M.; Kroke, A.; Lissner, L.; Boeing, H. Beer consumption and the ‘beer belly’: Scientific basis or common belief? Eur. J. Clin. Nutr. 2009, 63, 1143–1149. [Google Scholar] [CrossRef]
- Frezza, M.; di Padova, C.; Pozzato, G.; Terpin, M.; Baraona, E.; Lieber, C.S. High blood alcohol levels in women: The role of decreased gastric alcohol dehydrogenase activity and first-pass metabolism. N. Engl. J. Med. 1990, 322, 95–99. [Google Scholar] [CrossRef]
- Griswold, M.G.; Fullman, N.; Hawley, C.; Arian, N.; Zimsen, S.R.; Tymeson, H.D.; Venkateswaran, V.; Tapp, A.D.; Forouzanfar, M.H.; Salama, J.S.; et al. Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef]
- Wang, L.; Lee, I.M.; Manson, J.E.; Buring, J.E.; Sesso, H.D. Alcohol consumption, weight gain, and risk of becoming overweight in middle-aged and older women. Arch. Intern. Med. 2010, 170, 453–461. [Google Scholar] [CrossRef]
- Friesema, I.; Veenstra, M.Y.; Zwietering, P.J.; Knottnerus, J.A.; Garretsen, H.; Lemmens, P. Measurement of lifetime alcohol intake: Utility of a self-administered questionnaire. Am. J. Epidemiol. 2004, 159, 809–817. [Google Scholar] [CrossRef]
- Del Boca, F.K.; Darkes, J. The validity of self-reports of alcohol consumption: State of the science and challenges for research. Addiction 2003, 98, 1–12. [Google Scholar] [CrossRef]
- Batty, G.D.; Gale, C.R.; Kivimäki, M.; Deary, I.J.; Bell, S. Comparison of risk factor associations in UK Biobank against representative, general population based studies with conventional response rates: Prospective cohort study and individual participant meta-analysis. BMJ 2020, 368, m131. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Women | Men | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Drinking Status (UK Units) | Non-Current Drinkers | 1st Quartile (≤1.3) | 2nd Quartile (<6.9) | 3rd Quartile (<14.3) | 4th Quartile (≥14.3) | Non-Current Drinkers | 1st Quartile (≤6.5) | 2nd Quartile (<15.9) | 3rd Quartile (<29.2) | 4th Quartile (≥29.2) |
| n | 1360 | 5009 | 4841 | 5994 | 6088 | 899 | 4712 | 5571 | 5708 | 5217 |
| Age (years) | 56.0 (7.8) | 55.3 (7.6) | 55.9 (7.5) | 55.6 (7.3) | 55.2 (7.2) | 56.2 (8.1) | 56.4 (8.0) | 57.0 (7.7) | 57.1 (7.6) | 56.9 (7.3) |
| Body mass index (kg/m2) 1 | 26.9 (5.5) | 27.2 (5.4) | 26.1 (4.6) | 25.7 (4.3) | 26.0 (4.3) | 27.2 (4.7) | 27.3 (4.3) | 26.9 (3.8) | 27.1 (3.6) | 27.8 (3.8) |
| BF% 2 | 36.2 (7.2) | 36.6 (7.0) | 35.4 (6.7) | 34.9 (6.5) | 35.3 (6.5) | 24.5 (6.2) | 24.4 (5.9) | 24.0 (5.5) | 24.4 (5.4) | 25.3 (5.3) |
| WC (cm) 3 | 83.3 (13.1) | 84.0 (12.7) | 81.7 (11.4) | 80.9 (10.7) | 82.0 (10.8) | 94.7 (12.2) | 95.2 (11.5) | 94.1 (10.4) | 94.7 (10.0) | 96.5 (10.5) |
| WHR 3 | 0.8 (0.1) | 0.8 (0.1) | 0.8 (0.1) | 0.8 (0.1) | 0.8 (0.1) | 0.9 (0.1) | 0.9 (0.1) | 0.9 (0.1) | 0.9 (0.1) | 0.9 (0.1) |
| Townsend deprivation index 4 | −1.5 (3.0) | −1.7 (2.9) | −2.1 (2.6) | −2.2 (2.5) | −2.0 (2.6) | −1.2 (3.1) | −1.8 (2.8) | −2.3 (2.6) | −2.3 (2.5) | −2.0 (2.7) |
| Fruit and vegetable consumption (servings/day) | 4.9 (3.5) | 4.7 (3.0) | 4.7 (2.8) | 4.7 (2.7) | 4.7 (3.0) | 4.2 (3.9) | 3.9 (3.2) | 4.0 (2.7) | 4.0 (2.9) | 3.8 (2.8) |
| Sedentary behaviour (hours/day) | 4.0 (2.9) | 4.0 (2.9) | 4.0 (2.5) | 3.9 (2.5) | 4.0 (2.7) | 4.7 (3.5) | 4.9 (3.1) | 4.7 (2.9) | 4.8 (2.9) | 4.9 (3.1) |
| CVD/cancer history (%) 5 | 27.2 | 25.7 | 24.1 | 23.6 | 23.3 | 35.0 | 34.4 | 32.2 | 31.6 | 31.8 |
| Adequate sleep duration (7–9 h) (%) | 71.9 | 76.7 | 78.5 | 78.6 | 77.6 | 72.9 | 76.0 | 77.5 | 77.8 | 76.7 |
| Never smoker (%) | 75.6 | 71.3 | 71.8 | 65.6 | 50.1 | 64.3 | 66.2 | 63.7 | 52.2 | 38.9 |
| Meeting physical activity guidelines (%) 6 | 72.7 | 72.4 | 76.6 | 76.7 | 76.9 | 70.4 | 73.3 | 77.4 | 79.5 | 78.3 |
| General Adiposity | Central Adiposity | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BMI (n = 40,696) | BF% (n = 18,480) | WC (n = 40,790) | WHR (n = 18,488) | |||||||||||||
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |||||||||
| Coefficient | 95% CI | Coefficient | 95% CI | Coefficient | 95% CI | Coefficient | 95% CI | Coefficient | 95% CI | Coefficient | 95% CI | Coefficient | 95% CI | Coefficient | 95% CI | |
| Women | ||||||||||||||||
| Quartile 1 | 0.06 | −0.11, 0.22 | 0.06 | −0.1, 0.23 | 0.62 | 0.24, 1 | 0.6 | 0.22, 0.98 | 0.48 | −0.09, 1.06 | 0.51 | −0.07, 1.08 | 0.004 | −0.002, 0.011 | 0.004 | −0.002, 0.01 |
| Quartile 2 | −0.07 | −0.24, 0.09 | −0.06 | −0.22, 0.11 | 0.45 | 0.07, 0.84 | 0.43 | 0.05, 0.82 | −0.43 | −1, 0.15 | −0.36 | −0.94, 0.21 | −0.001 | −0.008, 0.005 | −0.001 | −0.008, 0.005 |
| Quartile 3 | −0.13 | −0.29, 0.04 | −0.11 | −0.27, 0.05 | 0.38 | 0, 0.75 | 0.35 | −0.03, 0.73 | −0.47 | −1.03, 0.09 | −0.41 | −0.97, 0.16 | 0.001 | −0.005, 0.007 | 0.001 | −0.005, 0.007 |
| Quartile 4 | −0.09 | −0.25, 0.07 | −0.1 | −0.26, 0.07 | 0.46 | 0.09, 0.84 | 0.42 | 0.04, 0.8 | −0.28 | −0.84, 0.29 | −0.28 | −0.84, 0.29 | 0.002 | −0.005, 0.008 | 0.001 | −0.006, 0.007 |
| Men | ||||||||||||||||
| Quartile 1 | −0.09 | −0.25, 0.07 | −0.07 | −0.23, 0.09 | −0.24 | −0.65, 0.16 | −0.24 | −0.65, 0.16 | −0.13 | −0.76, 0.5 | −0.04 | −0.67, 0.59 | 0.003 | −0.004, 0.01 | 0.004 | −0.004, 0.011 |
| Quartile 2 | −0.15 | −0.3, 0.01 | −0.11 | −0.26, 0.05 | −0.31 | −0.71, 0.09 | −0.3 | −0.7, 0.11 | −0.48 | −1.1, 0.14 | −0.34 | −0.97, 0.28 | 0.001 | −0.006, 0.008 | 0.002 | −0.005, 0.009 |
| Quartile 3 | −0.16 | −0.31, 0 | −0.12 | −0.28, 0.03 | −0.38 | −0.79, 0.02 | −0.39 | −0.79, 0.02 | −0.38 | −1, 0.24 | −0.28 | −0.91, 0.34 | 0.001 | −0.006, 0.008 | 0.001 | −0.006, 0.008 |
| Quartile 4 | 0.04 | −0.12, 0.19 | 0.03 | −0.12, 0.19 | −0.08 | −0.48, 0.33 | −0.12 | −0.53, 0.28 | 0.37 | −0.26, 1 | 0.36 | −0.27, 0.99 | 0.006 | −0.002, 0.013 | 0.005 | −0.002, 0.012 |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| Coefficient | 95% CI | Coefficient | 95% CI | Coefficient | 95% CI | |
| BMI (n = 40,696) | ||||||
| Women | ||||||
| Red wine | −0.11 | −0.16, −0.05 | −0.09 | −0.15, −0.04 | −0.09 | −0.15, −0.04 |
| Champagne | −0.09 | −0.15, −0.04 | −0.08 | −0.13, −0.02 | −0.08 | −0.13, −0.02 |
| Beer | −0.04 | −0.11, 0.03 | −0.04 | −0.11, 0.03 | −0.04 | −0.11, 0.03 |
| Spirits | 0.06 | 0, 0.13 | 0.06 | −0.01, 0.12 | 0.06 | −0.01, 0.12 |
| Fortified wine | 0.01 | −0.09, 0.1 | 0.02 | −0.08, 0.12 | 0.02 | −0.08, 0.12 |
| Men | ||||||
| Red wine | −0.09 | −0.14, −0.04 | −0.06 | −0.11, −0.01 | −0.06 | −0.11, −0.02 |
| Champagne | −0.07 | −0.12, −0.03 | −0.05 | −0.09, 0 | −0.05 | −0.09, 0 |
| Beer | −0.02 | −0.07, 0.03 | −0.02 | −0.07, 0.03 | −0.02 | −0.08, 0.03 |
| Spirits | 0.04 | −0.01, 0.09 | 0.03 | −0.02, 0.08 | 0.03 | −0.02, 0.08 |
| Fortified wine | −0.02 | −0.11, 0.06 | −0.01 | −0.09, 0.08 | −0.01 | −0.09, 0.08 |
| BF% (n = 18,480) | ||||||
| Women | ||||||
| Red wine | −0.06 | −0.19, 0.07 | −0.06 | −0.2, 0.07 | −0.06 | −0.19, 0.08 |
| Champagne | −0.03 | −0.17, 0.1 | −0.04 | −0.17, 0.1 | −0.03 | −0.17, 0.1 |
| Beer | −0.09 | −0.26, 0.08 | −0.1 | −0.27, 0.08 | −0.09 | −0.26, 0.09 |
| Spirits | 0.16 | 0, 0.31 | 0.14 | −0.01, 0.3 | 0.14 | −0.01, 0.3 |
| Fortified wine | −0.01 | −0.23, 0.21 | −0.02 | −0.24, 0.2 | −0.02 | −0.24, 0.2 |
| Men | ||||||
| Red wine | −0.18 | −0.31, −0.06 | −0.17 | −0.3, −0.05 | −0.16 | −0.29, −0.03 |
| Champagne | −0.13 | −0.25, −0.01 | −0.11 | −0.23, 0.01 | −0.1 | −0.22, 0.02 |
| Beer | 0.03 | −0.1, 0.16 | 0.02 | −0.11, 0.15 | 0.02 | −0.11, 0.15 |
| Spirits | −0.04 | −0.16, 0.09 | −0.05 | −0.18, 0.07 | −0.05 | −0.18, 0.07 |
| Fortified wine | −0.05 | −0.27, 0.17 | −0.03 | −0.25, 0.19 | −0.02 | −0.24, 0.2 |
| WC (n = 40,790) | ||||||
| Women | ||||||
| Red wine | −0.65 | −0.84, −0.45 | −0.6 | −0.8, −0.41 | −0.58 | −0.77, −0.38 |
| Champagne | −0.55 | −0.74, −0.36 | −0.5 | −0.69, −0.3 | −0.49 | −0.68, −0.29 |
| Beer | −0.35 | −0.59, −0.11 | −0.37 | −0.61, −0.12 | −0.35 | −0.59, −0.1 |
| Spirits | 0.3 | 0.07, 0.52 | 0.28 | 0.06, 0.5 | 0.26 | 0.04, 0.49 |
| Fortified wine | −0.26 | −0.6, 0.07 | −0.21 | −0.54, 0.13 | −0.19 | −0.53, 0.15 |
| Men | ||||||
| Red wine | −0.4 | −0.6, -0.21 | −0.32 | −0.51, −0.12 | −0.28 | −0.47, −0.08 |
| Champagne | −0.34 | −0.53, −0.15 | −0.25 | −0.44, −0.06 | −0.23 | −0.42, −0.04 |
| Beer | −0.28 | −0.48, −0.08 | −0.29 | −0.48, −0.09 | −0.29 | −0.48, −0.09 |
| Spirits | 0.24 | 0.04, 0.43 | 0.22 | 0.02, 0.41 | 0.21 | 0.02, 0.41 |
| Fortified wine | 0.01 | −0.33, 0.35 | 0.08 | −0.26, 0.42 | 0.1 | −0.24, 0.44 |
| WHR (n = 18,488) | ||||||
| Women | ||||||
| Red wine | −0.003 | −0.005, 0 | −0.003 | −0.005, 0 | −0.002 | −0.005, 0 |
| Champagne | −0.002 | −0.004, 0.001 | −0.003 | −0.005, 0 | −0.003 | −0.005, 0 |
| Beer | 0 | −0.003, 0.003 | −0.001 | −0.003, 0.002 | 0 | −0.003, 0.003 |
| Spirits | 0.002 | −0.001, 0.005 | 0.002 | −0.001, 0.004 | 0.002 | −0.001, 0.004 |
| Fortified wine | −0.001 | −0.005, 0.003 | 0 | −0.004, 0.003 | 0 | −0.004, 0.003 |
| Men | ||||||
| Red wine | −0.002 | −0.004, 0.001 | −0.001 | −0.003, 0.001 | −0.001 | −0.003, 0.001 |
| Champagne | −0.003 | −0.005, 0 | −0.001 | −0.003, 0.001 | −0.001 | −0.003, 0.001 |
| Beer | −0.001 | −0.003, 0.002 | −0.001 | −0.003, 0.001 | 0 | −0.003, 0.002 |
| Spirits | 0.003 | 0, 0.005 | 0.003 | 0, 0.005 | 0.003 | 0, 0.005 |
| Fortified wine | 0.001 | −0.003, 0.004 | 0.001 | −0.003, 0.005 | 0.001 | −0.002, 0.005 |
| Incident Overweight (BMI ≥ 25 kg/m2) | Incident Obesity (≥30 kg/m2) | |||||||
|---|---|---|---|---|---|---|---|---|
| Women (Case/Total = 1389/9725) | Men (936/5787) | Women (904/17,077) | Men (864/15,790) | |||||
| Odds Ratio | 95% CI | Odds Ratio | 95% CI | Odds Ratio | 95% CI | Odds Ratio | 95% CI | |
| Total alcohol consumptiona | ||||||||
| Quartile 1 | 1.21 | 0.93, 1.59 | 0.91 | 0.64, 1.29 | 0.93 | 0.71, 1.22 | 0.93 | 0.65, 1.34 |
| Quartile 2 | 0.89 | 0.68, 1.17 | 0.94 | 0.66, 1.33 | 0.6 | 0.45, 0.8 | 0.8 | 0.56, 1.15 |
| Quartile 3 | 0.83 | 0.64, 1.09 | 0.89 | 0.62, 1.26 | 0.53 | 0.4, 0.7 | 0.82 | 0.58, 1.18 |
| Quartile 4 | 0.94 | 0.72, 1.23 | 1.13 | 0.79, 1.62 | 0.61 | 0.46, 0.8 | 1.09 | 0.77, 1.56 |
| Alcohol typeb | ||||||||
| Red wine | 0.83 | 0.73, 0.94 | 0.9 | 0.77, 1.06 | 0.75 | 0.65, 0.88 | 0.8 | 0.69, 0.94 |
| Champagne | 0.82 | 0.73, 0.93 | 0.88 | 0.76, 1.03 | 0.81 | 0.7, 0.94 | 0.82 | 0.71, 0.95 |
| Beer | 0.94 | 0.82, 1.09 | 0.94 | 0.8, 1.11 | 0.9 | 0.76, 1.08 | 0.84 | 0.71, 0.99 |
| Spirits | 1.08 | 0.94, 1.24 | 1.05 | 0.9, 1.23 | 1.23 | 1.05, 1.44 | 1.06 | 0.92, 1.23 |
| Fortified wine | 0.78 | 0.63, 0.98 | 0.83 | 0.63, 1.1 | 1.02 | 0.79, 1.31 | 1.04 | 0.8, 1.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inan-Eroglu, E.; Huang, B.-H.; Hamer, M.; Britton, A.; Stamatakis, E. Alcohol Consumption and Adiposity: A Longitudinal Analysis of 45,399 UK Biobank Participants. Int. J. Environ. Res. Public Health 2022, 19, 11945. https://doi.org/10.3390/ijerph191911945
Inan-Eroglu E, Huang B-H, Hamer M, Britton A, Stamatakis E. Alcohol Consumption and Adiposity: A Longitudinal Analysis of 45,399 UK Biobank Participants. International Journal of Environmental Research and Public Health. 2022; 19(19):11945. https://doi.org/10.3390/ijerph191911945
Chicago/Turabian StyleInan-Eroglu, Elif, Bo-Huei Huang, Mark Hamer, Annie Britton, and Emmanuel Stamatakis. 2022. "Alcohol Consumption and Adiposity: A Longitudinal Analysis of 45,399 UK Biobank Participants" International Journal of Environmental Research and Public Health 19, no. 19: 11945. https://doi.org/10.3390/ijerph191911945