
Impact of Antiretroviral Therapy on Oral Health among Children Living with HIV: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. PECO(S) Statements
2.2. Participants (P)
2.3. Exposure (E) and Control (C)
2.4. Outcome Measures (O)
- (a)
- Dental caries;
- (b)
- Oral hygiene and periodontal health status;
- (c)
- HIV-related orofacial diseases based on the WHO clinical staging and immunological classification, including stage 2 (angular cheilitis, herpes zoster, linear gingival erythema, recurrent oral ulceration, parotid enlargement), stage 3 (oral candidiasis, oral hairy leukoplakia acute necrotising ulcerative gingivitis/periodontitis), and stage 4 (herpes simplex infection, Kaposi’s sarcoma);
- (d)
- Saliva immunoglobulin quantity;
- (e)
- Oral microbiome count;
- (f)
- Dental development and maturation.
2.5. Studies (S)
2.6. Search Strategies
2.7. Selection of Studies
2.8. Data Extraction and Management
2.9. Measures of Effect
2.10. Subgroup Analyses
2.11. Assessment of Risk of Bias
2.12. Data Synthesis
2.13. Assessment of Heterogeneity
2.14. Assessment of Publication Bias
2.15. Assessment of Quality of Evidence
3. Results
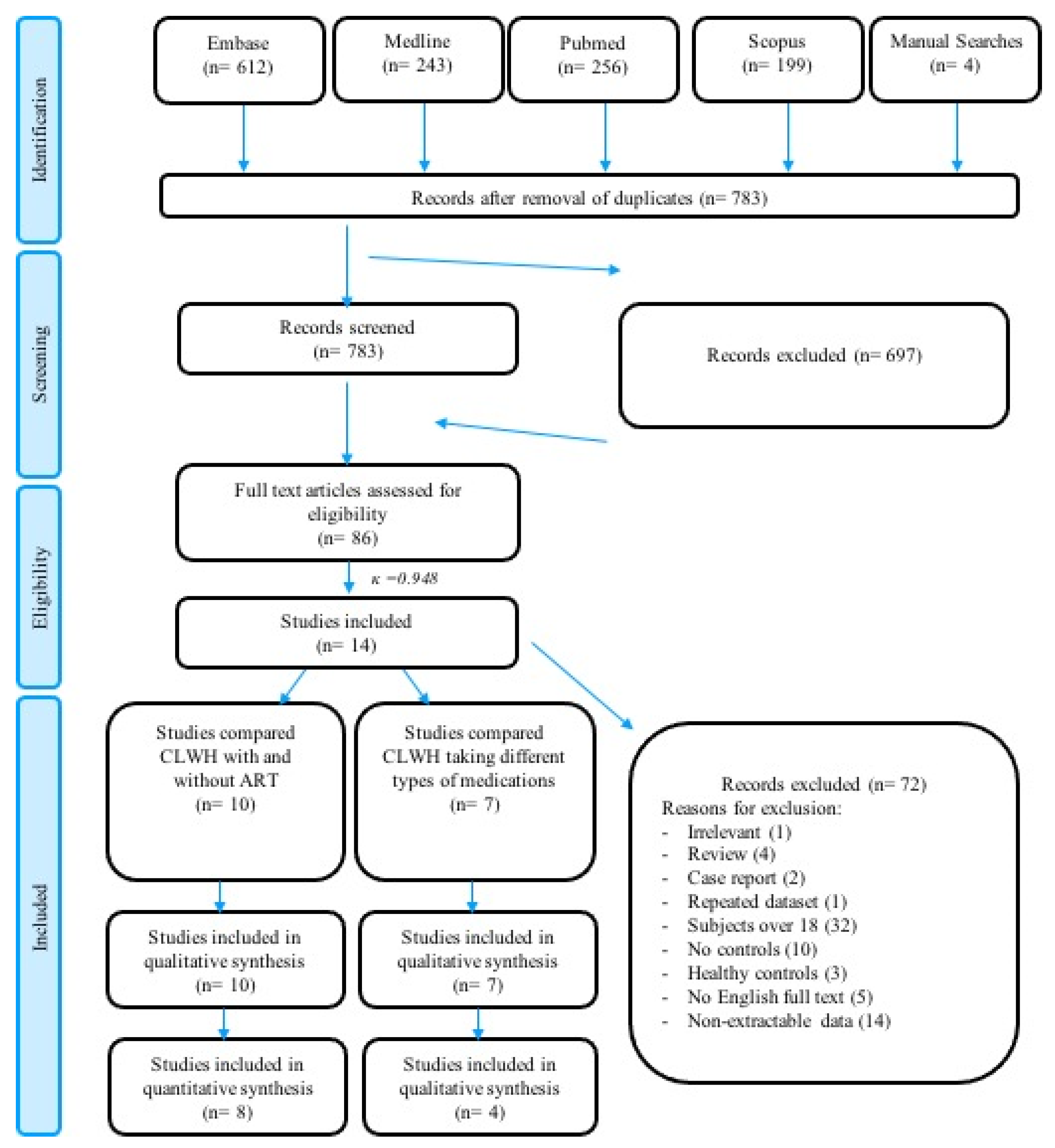
3.1. Study Selection
3.2. Study Characteristics
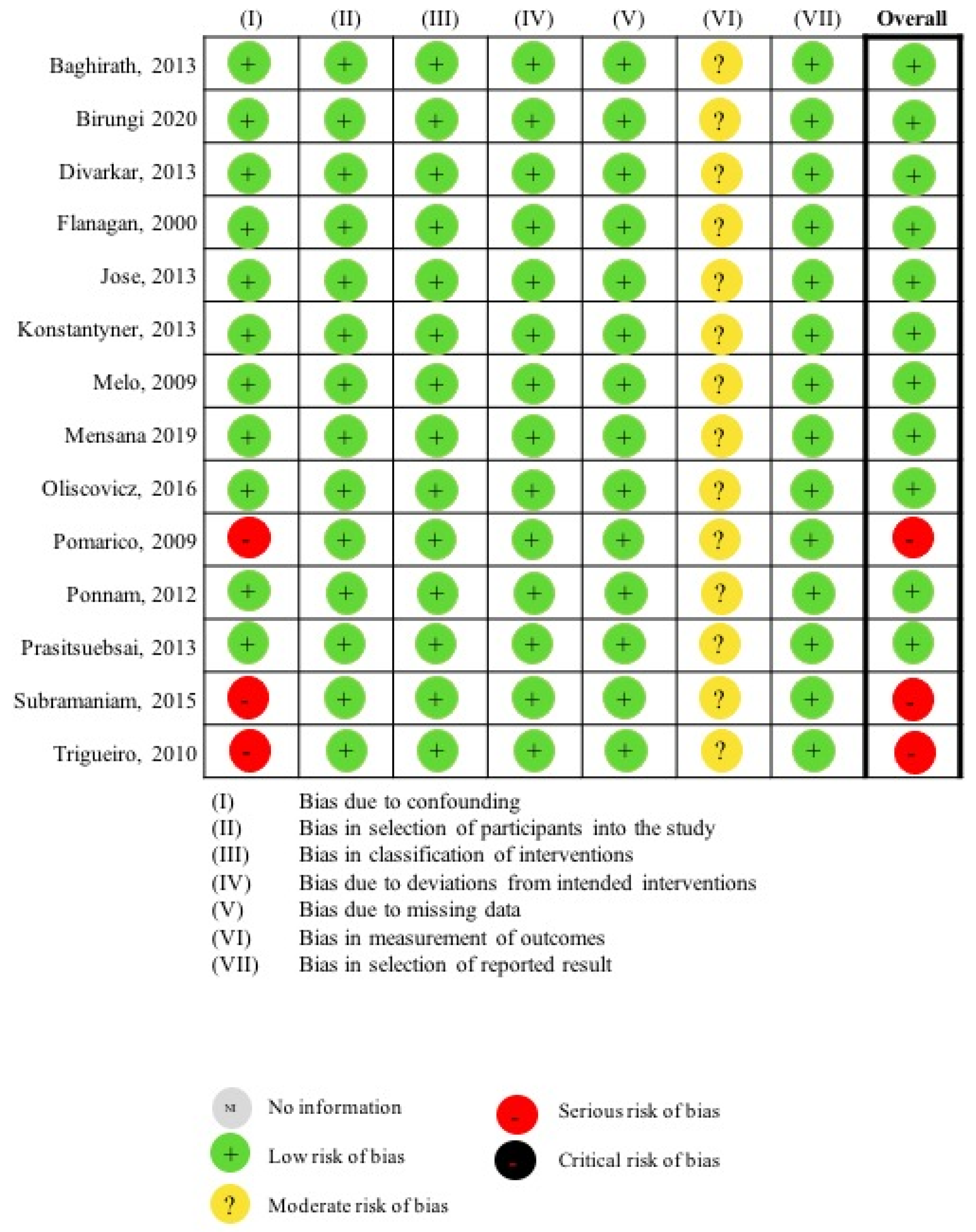
3.3. Risk of Bias of Included Studies
3.4. CLWH under ART versus Those without Dental Caries Experience
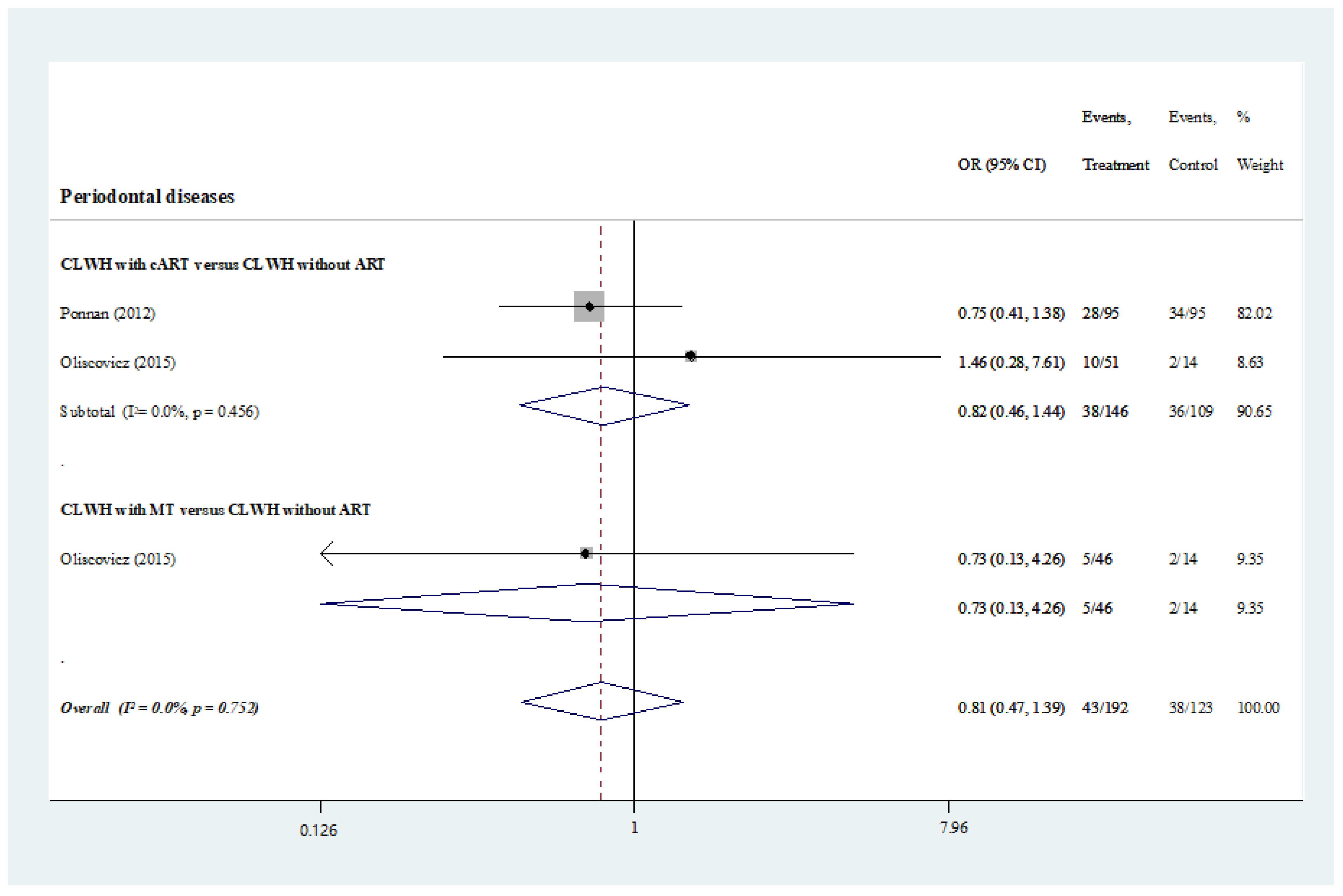
Oral Hygiene and Periodontal Status
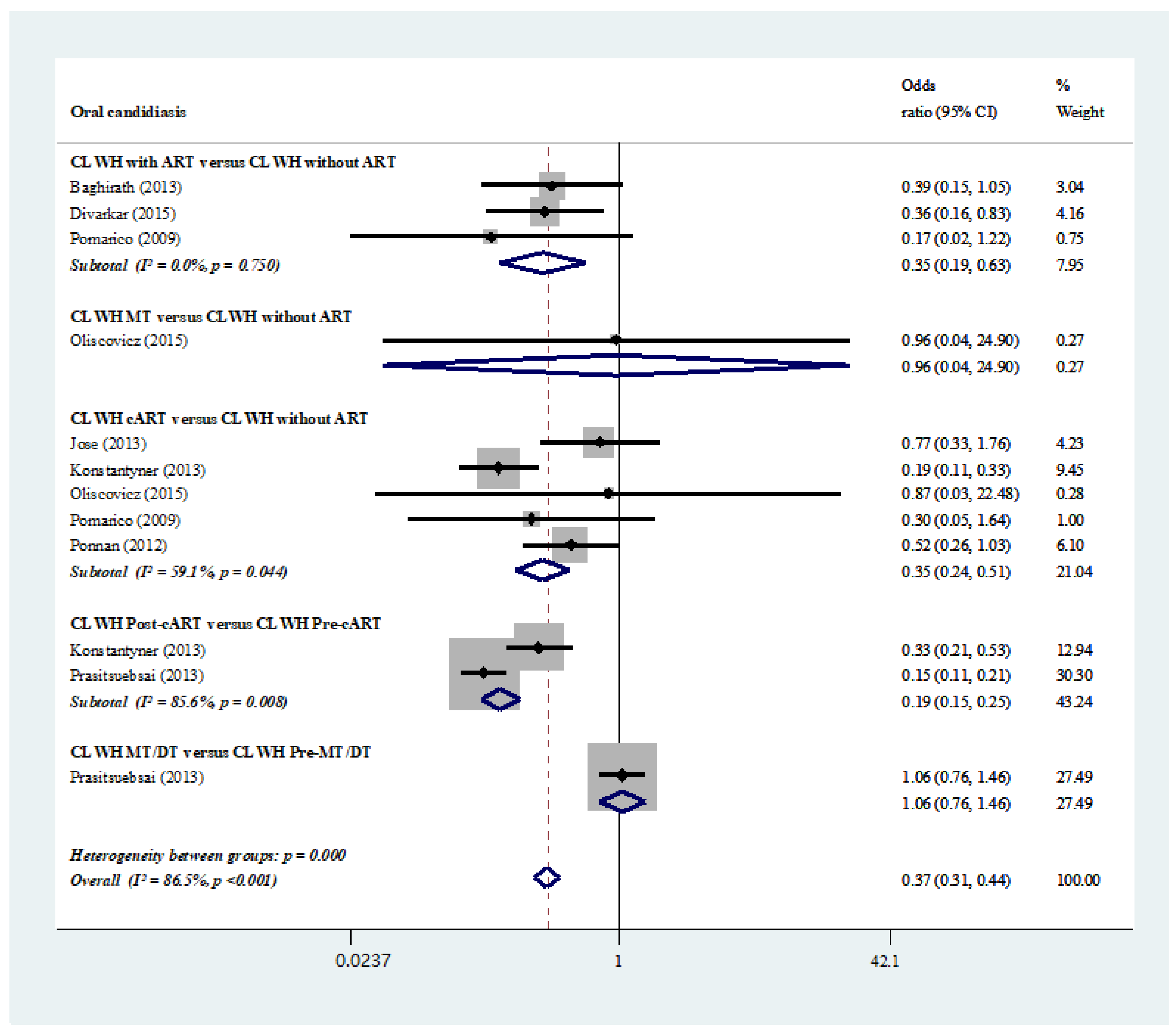
3.5. Oral Candidiasis and Oral Microbiome Count
3.6. Other HIV-Related Orofacial Diseases
3.7. Saliva Immunoglobulins Quantity
3.8. Dental Development and Maturation
3.9. CLWH under Different ART Medications
3.10. Other Associated Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Glick, M.; Williams, D.M.; Kleinman, D.V.; Vujicic, M.; Watt, R.G.; Weyant, R.J. A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. J. Public Health Dent. 2017, 77, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.M.; McGrath, C.P.; King, N.M.; Lo, E.C. Oral health-related quality of life in Hong Kong preschool children. Caries Res. 2011, 45, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Acs, G.; Lodolini, G.; Kaminsky, S.; Cisneros, G.J. Effect of nursing caries on body weight in a pediatric population. Pediatr. Dent. J. 1992, 14, 302–305. [Google Scholar]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar]
- Hanna, J.J.; Nijhawan, A.E.; Lehmann, C.U.; Medford, R.J. Simulating Facebook Advertisements to Establish Cost per New HIV Diagnosis Using Routine and Targeted Models in a Local Population. Healthcare 2022, 10, 1195. [Google Scholar] [CrossRef]
- Marcu, E.A.; Dinescu, S.N.; Pădureanu, V.; Dumitrescu, F.; Diaconu, R. Perinatal Exposure to HIV Infection: The Experience of Craiova Regional Centre, Romania. Healthcare 2022, 10, 308. [Google Scholar] [CrossRef]
- Unicef. Global and Regional Trend. Available online: https://data.unicef.org/topic/hivaids/global-regional-trends/#:~:text=An%20estimated%20110%2C000%20%5B74%2C000%2D180%2C000,children%20under%2010%20years%20old (accessed on 2 August 2022).
- Poorolajal, J.; Hooshmand, E.; Mahjub, H.; Esmailnasab, N.; Jenabi, E. Survival rate of AIDS disease and mortality in HIV-infected patients: A meta-analysis. Public Health 2016, 139, 3–12. [Google Scholar] [CrossRef]
- Lilian, R.R.; Mutasa, B.; Railton, J.; Mongwe, W.; Mc, I.J.; Struthers, H.E.; Peters, R.P. A 10-year cohort analysis of routine paediatric ART data in a rural South African setting. Epidemiol. Infect. 2017, 145, 170–180. [Google Scholar] [CrossRef]
- World Health Organization. Paediatric HIV Data and Statistics. Available online: https://www.who.int/hiv/topics/paediatric/data/en/index1.html (accessed on 2 August 2022).
- Sharma, G.; Oberoi, S.S.; Vohra, P.; Nagpal, A. Oral manifestations of HIV/AIDS in Asia: Systematic review and future research guidelines. J. Clin. Exp. Dent. 2015, 7, e419–e427. [Google Scholar] [CrossRef]
- Scully, C.; Diz Dios, P. Orofacial effects of antiretroviral therapies. Oral Dis. 2001, 7, 205–210. [Google Scholar] [CrossRef]
- Donaldson, M.; Goodchild, J.H.; Epstein, J.B. Sugar content, cariogenicity, and dental concerns with commonly used medications. J. Am. Dent. Assoc. 2015, 146, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Unicef. The United Nations Convention on the Rights of the Child. Available online: https://www.unicef.org.uk/what-we-do/un-convention-child-rights/ (accessed on 5 August 2022).
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Bradburn, M.J.; Egger, M. Meta–Analysis in Stata™. In Systematic Reviews in Health Care: Meta-Analysis in Context; Wiley: London, UK, 2001. [Google Scholar]
- Löe, H.; Silness, J. Periodontal disease in pregnancy I. Prevalence and severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef]
- Silness, J.; Löe, H. Periodontal disease in pregnancy II. Correlation between oral hygiene and periodontal condition. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. Br. Med. J. 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; Group, C.S.M. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; pp. 241–284. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Br. Med. J. 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.; Hill, S. How to GRADE the Quality of the Evidence. Cochrane Consumers and Communication Group. Version 3.0. December 2016. Available online: http://cccrg.cochrane.org/author-resources (accessed on 18 September 2022).
- Baghirath, P.; Krishna, A.; Gannepalli, A.; Ali, M. Oral manifestations of HIV in children receiving anti-retroviral therapy in Hyderabad, India. Eur. Arch. Paediatr. Dent. 2013, 14, 389–395. [Google Scholar] [CrossRef]
- Birungi, N.; Fadnes, L.T.; Engebretsen, I.M.S.; Tumwine, J.K.; Astrom, A.N. Antiretroviral treatment and its impact on oral health outcomes in 5 to 7 year old Ugandan children: A 6 year follow-up visit from the ANRS 12174 randomized trial. Medicine 2020, 99, e22352. [Google Scholar] [CrossRef]
- Divakar, D.D.; Al Kheraif, A.A.; Ramakrishnaiah, R.; Khan, A.A.; Sandeepa, N.; Alshahrani, O.A.; Alahmari, A. Oral manifestations in human immunodeficiency virus infected pediatric patients receiving and not receiving antiretroviral therapy: A cross sectional study. Paediatr. Croat. 2015, 59, 152–158. [Google Scholar] [CrossRef]
- Flanagan, M.A.; Barasch, A.; Koenigsberg, S.R.; Fine, D.; Houpt, M. Prevalence of oral soft tissue lesions in HIV-infected minority children treated with highly active antiretroviral therapies. Pediatr. Dent. J. 2000, 22, 287–291. [Google Scholar]
- Jose, R.; Chandra, S.; Puttabuddi, J.H.; Vellappally, S.; Al Khuraif, A.A.; Halawany, H.S.; Abraham, N.B.; Jacob, V.; Hashim, M. Prevalence of oral and systemic manifestations in pediatric HIV cohorts with and without drug therapy. Curr. HIV Res. 2013, 11, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Konstantyner, T.C.; Silva, A.M.; Tanaka, L.F.; Marques, H.H.; Latorre Mdo, R. Factors associated with time free of oral candidiasis in children living with HIV/AIDS, São Paulo, Brazil. Cad. Saude Publica 2013, 29, 2197–2207. [Google Scholar] [CrossRef] [PubMed]
- Melo, N.R.; Taguchi, H.; Culhari, V.P.; Kamei, K.; Mikami, Y.; Smith, S.N.; Vilela, M.S. Oral candidiasis of HIV-infected children undergoing sequential HIV therapies. Med. Mycol. 2009, 47, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Mensana, M.P.; Nugraha, A.P.; Ernawati, D.S.; Soebadi, B.; Triyono, E.A.; Husada, D.; Prasetyo, R.A. Sensitivity and specificity of linear gingival erythema as immune suppression marker in pediatric HIV-infected at UPIPI Soetomo general hospital Surabaya, Indonesia. Indian J. Public Health Res. Dev. 2019, 10, 572–577. [Google Scholar] [CrossRef]
- Oliscovicz, N.F.; Pomarico, L.; Castro, G.F.; Souza, I.P. Effect of highly active antiretroviral therapy use on oral manifestations in pediatric patients infected with HIV. Indian J. Dent. Res. 2015, 26, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Pomarico, L.; Cerqueira, D.F.; de Araujo Soares, R.M.; de Souza, I.P.; de Araujo Castro, G.F.; Socransky, S.; Haffajee, A.; Teles, R.P. Associations among the use of highly active antiretroviral therapy, oral candidiasis, oral Candida species and salivary immunoglobulin A in HIV-infected children. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2009, 108, 203–210. [Google Scholar] [CrossRef]
- Ponnam, S.R.; Srivastava, G.; Theruru, K. Oral manifestations of human immunodeficiency virus in children: An institutional study at highly active antiretroviral therapy centre in India. J. Oral Maxillofac. Pathol. 2012, 16, 195–202. [Google Scholar] [CrossRef]
- Prasitsuebsai, W.; Sethaputra, C.; Lumbiganon, P.; Hansudewechakul, R.; Chokephaibulkit, K.; Truong, K.H.; Nguyen, L.V.; Mohd Razali, K.A.; Nik Yusoff, N.K.; Fong, M.S.; et al. Adherence to antiretroviral therapy, stigma and behavioral risk factors in HIV-infected adolescents in Asia. AIDS Care 2018, 30, 727–733. [Google Scholar] [CrossRef]
- Subramaniam, P.; Kumar, K.; Girish Babu, K. Levels of salivary immunoglobulin a (SIgA) in HIV infected children. J. Clin. Pediatr. Dent. 2015, 39, 377–381. [Google Scholar] [CrossRef]
- Trigueiro, M.; Tedeschi-Oliveira, S.V.; Melani, R.F.; Ortega, K.L. An assessment of adverse effects of antiretroviral therapy on the development of HIV positive children by observation of dental mineralization chronology. J. Oral Pathol. Med. 2010, 39, 35–40. [Google Scholar] [CrossRef]
- Oliveira, C.A.; Tannure, P.N.; de Souza, I.P.; Maia, L.C.; Portela, M.B.; Castro, G.F. Is dental caries experience increased in HIV-infected children and adolescents? A meta-analysis. Acta Odontol. Scand. 2015, 73, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Masanjala, W. The poverty-HIV/AIDS nexus in Africa: A livelihood approach. Soc. Sci. Med. 2007, 64, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Dörfer, C.E.; Schlattmann, P.; Foster Page, L.; Thomson, W.M.; Paris, S. Socioeconomic inequality and caries: A systematic review and meta-analysis. J. Dent. Res. 2015, 94, 10–18. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antiretroviral Therapy of HIV Infection in Infants and Children: Towards Universal Access: Recommendations for a Public Health Approach [2010 Revision]. Available online: https://www.who.int/hiv/pub/paediatric/infants2010/en/ (accessed on 5 August 2022).
- Marcotte, H.; Lavoie, M.C. Oral microbial ecology and the role of salivary immunoglobulin A. Microbiol. Mol. Biol. Rev. 1998, 62, 71–109. [Google Scholar] [CrossRef]
- Javed, F.; Akram, Z.; Binshabaib, M.S.; Alharthi, S.S.; Kellesarian, S.V.; Vohra, F. Is salivary IgA level a potential biomarker for immunosuppression in HIV-positive children? A systematic review and meta-analysis. Rev. Med Virol. 2017, 27, e1933. [Google Scholar] [CrossRef]
- Haeri-Araghi, H.; Zarabadipour, M.; Safarzadeh-Khosroshahi, S.; Mirzadeh, M. Evaluating the relationship between dental caries number and salivary level of IgA in adults. J. Clin. Exp. Dent. 2018, 10, e66–e69. [Google Scholar] [CrossRef]
- Rangbulla, V.; Nirola, A.; Gupta, M.; Batra, P.; Gupta, M. Salivary IgA, Interleukin-1β and MMP-8 as Salivary Biomarkers in Chronic Periodontitis Patients. Chin. J. Dent. Res. 2017, 20, 43–51. [Google Scholar] [CrossRef]
- Barcellini, W.; Colombo, G.; La Maestra, L.; Clerici, G.; Garofalo, L.; Brini, A.T.; Lipton, J.M.; Catania, A. Alpha-melanocyte-stimulating hormone peptides inhibit HIV-1 expression in chronically infected promonocytic U1 cells and in acutely infected monocytes. J. Leukoc. Biol. 2000, 68, 693–699. [Google Scholar]
- Langford, A.; Pohle, H.D.; Gelderblom, H.; Zhang, X.; Reichart, P.A. Oral hyperpigmentation in HIV-infected patients. Oral Surg. Oral Med. Oral Pathol. 1989, 67, 301–307. [Google Scholar] [CrossRef]
- Weitzmann, M.N. Bone and the Immune System. Toxicol. Pathol. 2017, 45, 911–924. [Google Scholar] [CrossRef]
- Hauk, M.J.; Moss, M.E.; Weinberg, G.A.; Berkowitz, R.J. Delayed tooth eruption: Association with severity of HIV infection. Pediatr. Dent. J. 2001, 23, 260–262. [Google Scholar]
- Borderi, M.; Farneti, B.; Tampellini, L.; Giuliani, R.; Verucchi, G.; Vescini, F.; Caudarella, R.; Chiodo, F. HIV-1, HAART and bone metabolism. New Microbiol. 2002, 25, 375–384. [Google Scholar] [PubMed]
- Pinzone, M.R.; Di Rosa, M.; Malaguarnera, M.; Madeddu, G.; Focà, E.; Ceccarelli, G.; d’Ettorre, G.; Vullo, V.; Fisichella, R.; Cacopardo, B.; et al. Vitamin D deficiency in HIV infection: An underestimated and undertreated epidemic. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 1218–1232. [Google Scholar] [PubMed]
- Foster, C.; Lyall, H. HIV and mitochondrial toxicity in children. J. Antimicrob. Chemother. 2008, 61, 8–12. [Google Scholar] [CrossRef]
- Sehrawat, J.S.; Singh, M.; Sharma, V. Forensic dental age estimation of sub-adult individuals using Nolla’s Radiographic method: A systematic review and meta-analysis. Braz. J. Forensic Sci. Med. Law Bioeth. 2016, 6, 32–46. [Google Scholar] [CrossRef] [Green Version]
- Madeddu, G.; Spanu, A.; Solinas, P.; Calia, G.M.; Lovigu, C.; Chessa, F.; Mannazzu, M.; Falchi, A.; Mura, M.S.; Madeddu, G. Bone mass loss and vitamin D metabolism impairment in HIV patients receiving highly active antiretroviral therapy. Q. J. Nucl. Med. 2004, 48, 39–48. [Google Scholar]
- Anaya-Saavedra, G.; Flores-Moreno, B.; Garcia-Carranca, A.; Irigoyen-Camacho, E.; Guido-Jimenez, M.; Ramirez-Amador, V. HPV oral lesions in HIV-infected patients: The impact of long-term HAART. J. Oral Pathol. Med. 2013, 42, 443–449. [Google Scholar] [CrossRef]
- Greenspan, D.; Canchola, A.J.; MacPhail, L.A.; Cheikh, B.; Greenspan, J.S. Effect of highly active antiretroviral therapy on frequency of oral warts. Lancet 2001, 357, 1411–1412. [Google Scholar] [CrossRef]
- Hodgson, T.A.; Greenspan, D.; Greenspan, J.S. Oral lesions of HIV disease and HAART in industrialized countries. Adv. Dent. Res. 2006, 19, 57–62. [Google Scholar] [CrossRef]
- Wells, G. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology.oxford.htm (accessed on 5 August 2022).
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Losilla, J.-M.; Oliveras, I.; Marin-Garcia, J.A.; Vives, J. Three risk of bias tools lead to opposite conclusions in observational research synthesis. J. Clin. Epidemiol. 2018, 101, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Cuello, C.; Akl, E.A.; Mustafa, R.A.; Meerpohl, J.J.; Thayer, K.; Morgan, R.L.; Gartlehner, G.; Kunz, R.; Katikireddi, S.V. GRADE guidelines: 18. How ROBINS-I and other tools to assess risk of bias in nonrandomized studies should be used to rate the certainty of a body of evidence. J. Clin. Epidemiol. 2019, 111, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.L.; Thayer, K.A.; Santesso, N.; Holloway, A.C.; Blain, R.; Eftim, S.E.; Goldstone, A.E.; Ross, P.; Guyatt, G.; Schünemann, H.J. Evaluation of the risk of bias in non-randomized studies of interventions (ROBINS-I) and the ‘target experiment’concept in studies of exposures: Rationale and preliminary instrument development. Environ. Int. 2018, 120, 382–387. [Google Scholar] [CrossRef]
- Jüni, P.; Holenstein, F.; Sterne, J.; Bartlett, C.; Egger, M. Direction and impact of language bias in meta-analyses of controlled trials: Empirical study. Int. J. Epidemiol. 2002, 31, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Klassen, T.P.; Schulz, K.F.; Berlin, J.A.; Jadad, A.R.; Liberati, A. What contributions do languages other than English make on the results of meta-analyses? J. Clin. Epidemiol. 2000, 53, 964–972. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year, Country a) P/R | Number of Subjects (% Males) | Age Range (Year) | Recruitment | Inclusion (I)/Exclusion (E) Criteria b | Confounders Evaluated | Outcome Measures | ||
|---|---|---|---|---|---|---|---|---|
| 1. | Baghirath (2013; IND) P | CLWH ART | 50 (46) | 5–12 | Nireekshana ART Centre, Hyderabad (NGO) | (I) Seropositive for antibody to HIV when tested by a particle agglutination test for antibodies to HIV and enzyme-linked immunosorbent assay (ELISA) (E) HIV-infected subjects with a history of local radiation therapy to the head and neck region. | ✓ Duration of therapy | ✓ Linear gingival erythema ✓ Hairy leukoplakia ✓ Angular cheilitis ✓ Oral ulcers ✓ Candidiasis ✓ Hyperpigmentation |
| CLWH NMD | 50 (50) | 5–12 | ||||||
| 2 | Birungi (2020; UGA) P | CLWH PI (Lopinavir/ Ritonanavir) | 80 (48) | 5–7 | Ouagadougou University Teaching Hospital (urban site in Burkina Faso), East London Hospital Complex (urban site in South Africa); Mbale Regional Referral Hospital (semi-rural site in Uganda); and Lusaka University Teaching Hospital (urban site in Zambia). | (I) Singleton (I) Breastfed on day 7 by their mothers (I) Negative HIV-1 DNA PCR on day 7 (I) Received any prevention of mother-to-child treatment (E) Newborns who had clinical signs or biological abnormalities of grade 2 or higher on the US National Institutes of Health Division of AIDS adverse events grading tables (E) Serious congenital malformations or birthweight was 2.0 kg or lower. | ✓ Marital status ✓ Socio-economic status ✓ Education level ✓ HIV clinical staging ✓ Detectable viral load ✓ Gender | ✓ Caries ✓ Gingival bleeding |
| CLWH NRTI (Lamivudine) | 84 (53) | 5–7 | ||||||
| 3 | Divakar (2015; SAU) P | CLWH ART | 62 (59.6) | 5–15 | District Hospital ART Centre | (I) Positive on particle agglutination test for antibodies to HIV and enzyme-inked immunosorbent assay (ELISA) (E) History of adverse habits such as tobacco and betel nut | ✓ Duration of therapy | ✓ Linear gingival erythema ✓ Hairy leukoplakia ✓ Angular cheilitis ✓ Oral ulcers ✓ Candidiasis ✓ Hyperpigmentation |
| CLWH NMD | 55 (53.7) | 5–15 | ||||||
| 4 | Flanagan (2000, BRA) P | CLWH cART | 23 (NR) | 6–18 | University-Affiliated Paediatric Infectious Disease Clinic | (I) Active treatment at the paediatric HIV clinic (I) Ambulatory capability (I) Life expectancy of over three months | None | ✓ Candidiasis |
| CLWH RTI | 14 (NR) | 6–18 | ||||||
| 5 | Jose (2013, IND) P | CLWH cART | 47 (34.0) | 2–12 | Hospital and out-patient centres | (I) Definitive diagnosis for HIV infection confirmed either by enzyme-linked immunosorbent assay (ELISA)/Western blot/HIV tri-dot tests (I) A combination therapy or cART with nucleoside reverse transcriptase inhibitors such as combivir (zidovudine + lamivudine combination) and/or lamivudine + stavudine and non-nucleoside reverse transcriptase inhibitors such as nevirapine/efavirenz were the prescribed drug regimens. (E) Children requiring urgent medical attention | ✓ CD4+ counts ✓ Duration of therapy | ✓ Angular cheilitis ✓ Linear gingival erythema ✓ Recurrent oral ulcerations ✓ Oral candidiasis ✓ Oral hairy leukoplakia ✓ Chronic herpes simplex infection ✓ Hyperpigmentation |
| CLWH NMD | 53 (45.2) | 2–12 | ||||||
| 6 | Konstantyner (2013; BRA) R | CLWH Pre-cART | 284 (NR) | 0.3–17.8 | Reference centre for the treatment of AIDS | (I) Laboratory confirmation of HIV infection contracted through vertical transmission (I) Less than 13 years of age at the time of admission to the health centre (E) Patients in follow-up for less than 90 days (E) Anti-inflammatory drugs and periodontal therapy in the past 6 months prior to the initial evaluation | ✓ Antiretroviral regimen | ✓ Oral candidiasis |
| CLWH Post-cART | 137(NR) | 0.3–17.8 | ||||||
| 7 | Melo (2009; BRA) P | CLWH MT | 61 (80.3) | 3–15 | University Paediatric Immunodeficiency Outpatient Service | ✓ CDC immunological category | ✓ Oral candidiasis | |
| CLWH cART and PI | 61 (80.3) | 3–15 | ||||||
| 8 | Mensana (2019; IDN) P | CLWH ART | 24 (NR) | 0–18 | Outpatient clinic UPIPI, Soetomo General Hospital | (E) Parental refusal in providing consent (E) Children being not cooperative during examination (E) No CD4 values found within 6 months interval from the date of an oral examination on patients’ medical record | ✓ Immune suppression ✓ Age | ✓ Linear gingival erythema |
| CLWH NMD | 4 (NR) | 0–18 | ||||||
| 9 | Oliscovicz (2016; BRA) R | CLWH cART | 51 (NR) | 2–16 | Paediatric AIDS Outpatient Clinic | (I) Definitively diagnosed with HIV infection according to criteria established by the Centers for Disease Control and Prevention | ✓ None | ✓ Gingivitis ✓ Parotid hypertrophy ✓ Linear gingival erythema |
| CLWH ART | 46 (NR) | 2–16 | ||||||
| CLWH NMD | 14 (NR) | 2–16 | ||||||
| 10 | Pomarico (2009; BRA) P | CLWH cART | 24 (50) | 2–13 | Paediatric AIDS Outpatients Clinic at the Federal University | (I) Definitive diagnosis for HIV infection confirmed by 2 positive ELISA tests and 1 positive Western blot (E) Presence of fixed or removable orthodontic appliances and systemic or local antifungal treatment within the last three months | ✓ AIDS status | ✓ Candida species ✓ Specific SIgA |
| CLWH NMD | 25 (42) | 2–13 | ||||||
| CLWH cART | 16 (31) | 2–13 | ||||||
| 11 | Ponnam (2012, IND) P | CLWH cART | 95(45.3) | 5–15 | Anti-Retroviral Therapy (ART) Center in Government General Hospital | (I) Came to the ART Center for the first time without previous history of anti-retroviral therapy | ✓ Age ✓ Socio-economic status | ✓ Candidiasis ✓ Caries ✓ Gingivitis/periodontitis ✓ Dental ✓ Ulcerative stomatitis ✓ Hyperpigmentation ✓ Mucocele |
| CLWH NMD | 95 (NR) | 5–15 | ||||||
| 12 | Prasitsuebsai (2013, IDN, IND, KHM, MYS, THA,) P | CLWH Pre-cART | 2129 (NR) | 0–18 | 14 participating clinics in Cambodia (n = 3), India (n = 1), Indonesia (n = 1), Malaysia (n = 4) and Thailand (n = 5). | (I) Conclusively diagnosed with HIV, using age-appropriate testing or through a presumptive clinical diagnosis of HIV infection defined as meeting WHO criteria for initiating antiretroviral therapy (ART). (I) Retrospective data provided were available. | ✓ CD4+ counts | ✓ Oral candidiasis ✓ Acute necrotising ulcerative ✓ Gingivitis/periodontitis ✓ Kaposi’s sarcoma |
| CLWH ART | 1480 (50.5) | 0–18 | ||||||
| CLWH MT, DT | 272 (51.8) | 0–18 | ||||||
| 13 | Subramaniam (2015; IND) P | CLWH Pre-ART | 25 (80) | 6–8 | HIV centres | (I) HIV-infected children aged 6–8 years (I) Children prior to the onset of anti-retroviral therapy and Group 2 consisting of children undergoing anti-retroviral therapy for more than 3 years | None | ✓ Specific SIgA |
| CLWH Post-ART | 25 (58.5) | 6–8 | HIV centres | |||||
| 14 | Trigueiro (2010; BRA) R | CLWH NRTI | 6 (NR) | 3–14 | University Centre for Special Care Patients | (I) HIV-positive patients | None | ✓ Dental mineralisation chronology |
| CLWH NRTI+PI | 23 (NR) | 3–14 | ||||||
| CLWH NRTI+NNRTI | 11 (NR) | 3–14 | ||||||
| CLWH NRTI+NNRTI+PI | 6 (NR) | 3–14 | ||||||
| CLWH NMD | 7 (NR) | 3–14 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lam, P.P.Y.; Zhou, N.; Yiu, C.K.Y.; Wong, H.M. Impact of Antiretroviral Therapy on Oral Health among Children Living with HIV: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 11943. https://doi.org/10.3390/ijerph191911943
Lam PPY, Zhou N, Yiu CKY, Wong HM. Impact of Antiretroviral Therapy on Oral Health among Children Living with HIV: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(19):11943. https://doi.org/10.3390/ijerph191911943
Chicago/Turabian StyleLam, Phoebe Pui Ying, Ni Zhou, Cynthia Kar Yung Yiu, and Hai Ming Wong. 2022. "Impact of Antiretroviral Therapy on Oral Health among Children Living with HIV: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 19: 11943. https://doi.org/10.3390/ijerph191911943