
Diet and Systemic Lupus Erythematosus (SLE): From Supplementation to Intervention
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
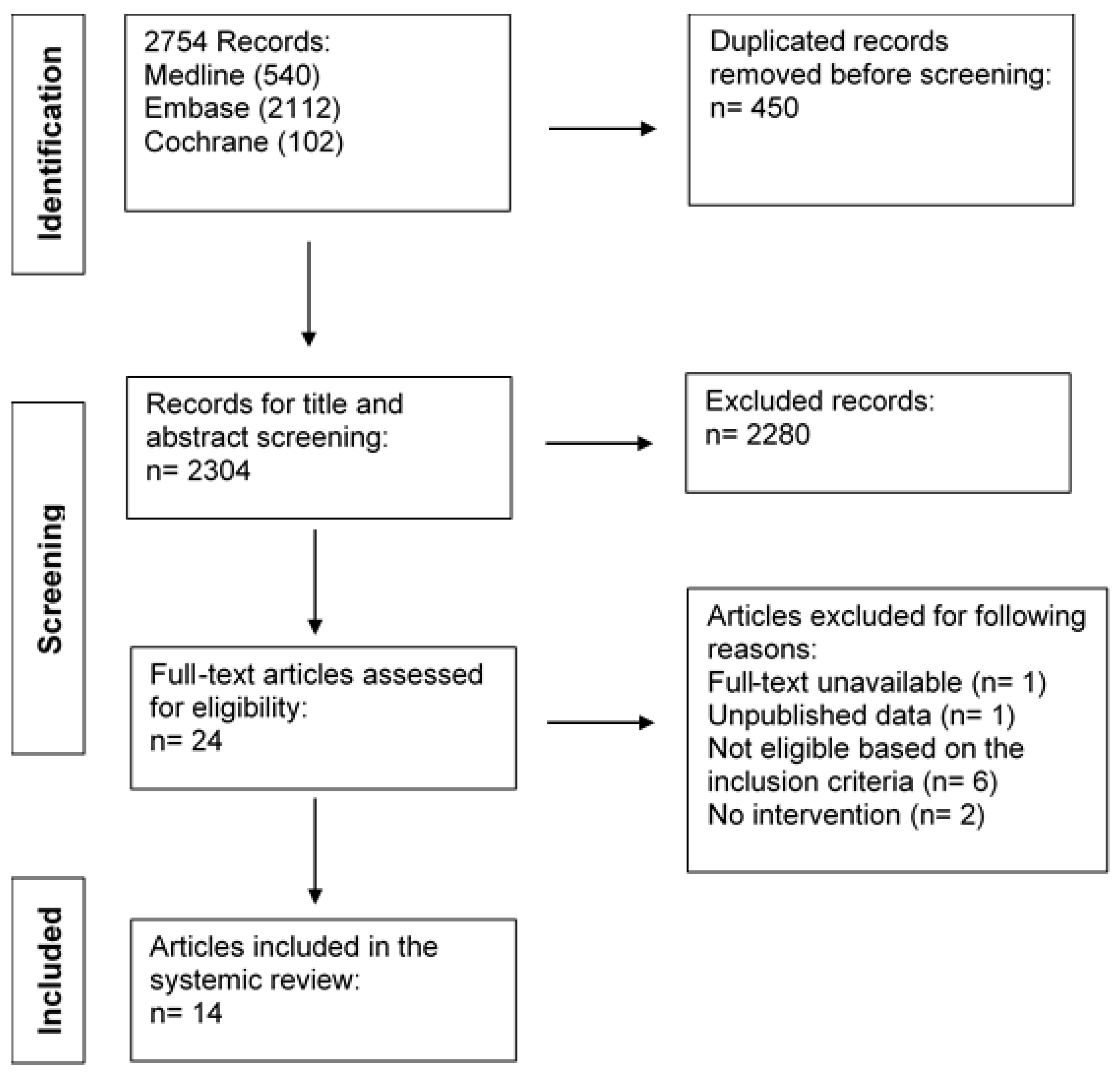
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Results
3.1. Characteristics of Eligible Studies
3.2. Effects of Vitamin D Supplementation Interventions in Patients with SLE
3.2.1. Serum Concentration of Vitamin D
3.2.2. Immune Function
3.2.3. Disease Activity
3.2.4. Safety
3.2.5. Bone Mass Density (BMD)
3.3. Effects of Omega-3 Fish Oil Supplementation Interventions in Patients with SLE
3.3.1. Lipid Profiles and Adipokines
3.3.2. Immune Response
3.3.3. Disease Activity
3.3.4. Vascular Health
3.3.5. Other Comorbidities
3.3.6. Safety
3.4. Effects of Vitamin E Supplementation Interventions in Patients with SLE
3.5. Effects of Curcumin Supplementation Interventions on Patients with SLE
3.6. Effects of Dietary Restriction Interventions on Patients with SLE
4. Discussion
4.1. Vitamin D and SLE
4.2. Omega-3 and SLE
4.3. Vitamin E and SLE
4.4. Curcumin and SLE
4.5. Diet Restrictions and SLE
4.6. Implications for Future Research
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Soto, M.A.; Sánchez-Hidalgo, M.; Alarcón-De-La-Lastra, C. An update on diet and nutritional factors in systemic lupus erythematosus management. Nutr. Res. Rev. 2017, 30, 118–137. [Google Scholar] [CrossRef] [PubMed]
- Pons-Estel, G.J.; Ugarte-Gil, M.F.; Alarcón, G.S. Epidemiology of systemic lupus erythematosus. Expert Rev. Clin. Immunol. 2017, 13, 799–814. [Google Scholar] [CrossRef]
- Noble, P.W.; Bernatsky, S.; Clarke, A.E.; Isenberg, D.A.; Ramsey-Goldman, R.; Hansen, J.E. DNA-damaging autoantibodies and cancer: The lupus butterfly theory. Nat. Rev. Rheumatol. 2016, 12, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, S.R.; Kasturi, S.; Costenbader, K.H. The epidemiology of atherosclerotic cardiovascular disease among patients with SLE: A systematic review. Semin. Arthritis Rheum. 2013, 43, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Kaul, A.; Gordon, C.; Crow, M.K.; Touma, Z.; Urowitz, M.B.; van Vollenhoven, R.; Ruiz-Irastorza, G.; Hughes, G. Systemic lupus erythematosus. Nat. Rev. Dis. Primers 2016, 2, 16039. [Google Scholar] [CrossRef] [PubMed]
- Gergianaki, I.; Garantziotis, P.; Adamichou, C.; Saridakis, I.; Spyrou, G.; Sidiropoulos, P.; Bertsias, G. High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete. J. Clin. Med. 2021, 10, 998. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.; Bland, A.R.; Maker, C.; Dunnage, J.; Bruce, I.N. Individuals living with lupus: Findings from the LUPUS UK Members Survey 2014. Lupus 2018, 27, 681–687. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Tziolos, N.; Bertsias, G.; Boumpas, D.T. Update on the diagnosis and management of systemic lupus erythematosus. Ann. Rheum. Dis. 2021, 80, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Irastorza, G.; Danza, A.; Khamashta, M. Glucocorticoid use and abuse in SLE. Rheumatology 2012, 51, 1145–1153. [Google Scholar] [CrossRef]
- Al Sawah, S.; Zhang, X.; Zhu, B.; Magder, L.S.; Foster, S.A.; Iikuni, N.; Petri, M. Effect of corticosteroid use by dose on the risk of developing organ damage over time in systemic lupus erythematosus-the Hopkins Lupus Cohort. Lupus Sci. Med. 2015, 2, e000066. [Google Scholar] [CrossRef] [Green Version]
- Khamashta, M.; Bruce, I.; Gordon, C.; Isenberg, D.; Ateka-Barrutia, O.; Gayed, M.; Donatti, C.; Guillermin, A.-L.; Foo, J.; Perna, A. The cost of care of systemic lupus erythematosus (SLE) in the UK: Annual direct costs for adult SLE patients with active autoantibody-positive disease. Lupus 2013, 23, 273–283. [Google Scholar] [CrossRef] [PubMed]
- de Medeiros, M.C.S.; Medeiros, J.C.A.; de Medeiros, H.J.; Leitão, J.C.G.D.C.; Knackfuss, M.I. Dietary intervention and health in patients with systemic lupus erythematosus: A systematic review of the evidence. Crit. Rev. Food Sci. Nutr. 2019, 59, 2666–2673. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Khandker, S.S.; Kotyla, P.J.; Hassan, R. Immunomodulatory Effects of Diet and Nutrients in Systemic Lupus Erythematosus (SLE): A Systematic Review. Front. Immunol. 2020, 11, 1477. [Google Scholar] [CrossRef]
- Academy of Nutrition and Dietetics. Evidence Analysis Manuel: Steps in the Academy Evidence Analysis Process. Available online: https://www.andeal.org/evidence-analysis-manual (accessed on 1 July 2021).
- Azzeh, F.S.; Al-Kushi, A.G.; Header, E.A.; ElSawy, N.A.; Hijazi, H.H.; Jazar, A.; Ghaith, M.M.; Alarjah, M.A. Effect of Vitamin D and calcium supplementation in patients with systemic lupus erythematosus. Saudi J. Med. Med. Sci. 2018, 6, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Andreoli, L.; Dall’Ara, F.; Piantoni, S.; Zanola, A.; Piva, N.; Cutolo, M.; Tincani, A. A 24-month prospective study on the efficacy and safety of two different monthly regimens of vitamin D supplementation in pre-menopausal women with systemic lupus erythematosus. Lupus 2015, 24, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Aranow, C.; Kamen, D.L.; Dall’Era, M.; Massarotti, E.M.; Mackay, M.C.; Koumpouras, F.; Coca, A.; Chatham, W.W.; Clowse, M.E.B.; Criscione-Schreiber, L.G.; et al. Randomized, double-blind, placebo-controlled trial of the effect of vitamin D3 on the interferon signature in patients with systemic lupus erythematosus. Arthritis Rheumatol. 2015, 67, 1848–1857. [Google Scholar] [CrossRef]
- Arriens, C.; Hynan, L.S.; Lerman, R.H.; Karp, D.R.; Mohan, C. Placebo-controlled randomized clinical trial of fish oil’s impact on fatigue, quality of life, and disease activity in Systemic Lupus Erythematosus. Nutr. J. 2015, 14, 82. [Google Scholar] [CrossRef]
- Bello, K.J.; Fang, H.; Fazeli, P.; Bolad, W.; Corretti, M.; Magder, L.S.; Petri, M. Omega-3 in SLE: A double-blind, placebo-controlled randomized clinical trial of endothelial dysfunction and disease activity in systemic lupus erythematosus. Rheumatol. Int. 2013, 33, 2789–2796. [Google Scholar] [CrossRef] [PubMed]
- Borges, M.C.; Santos, F.D.M.M.D.; Telles, R.W.; Andrade, M.V.; Correia, M.I.T.D.; Lanna, C.C.D. Omega-3 fatty acids, inflammatory status and biochemical markers of patients with systemic lupus erythematosus: A pilot study. Rev. Bras. Reum. Engl. Ed. 2017, 57, 526–534. [Google Scholar] [CrossRef]
- Shirzadi, M.; Karimzadeh, H.; Karimifar, M. The effect of Vitamin D supplementation in disease activity of systemic lupus erythematosus patients with Vitamin D deficiency: A randomized clinical trial. J. Res. Med. Sci. 2017, 22, 4. [Google Scholar] [CrossRef]
- Lozovoy, M.A.B.; Simão, A.N.C.; Morimoto, H.K.; Scavuzzi, B.M.; Iriyoda, T.V.M.; Reiche, E.M.V.; Cecchini, R.; Dichi, I. Fish Oil N-3 Fatty Acids Increase Adiponectin and Decrease Leptin Levels in Patients with Systemic Lupus Erythematosus. Mar. Drugs 2015, 13, 1071–1083. [Google Scholar] [CrossRef] [PubMed]
- Maeshima, E.; Liang, X.-M.; Goda, M.; Otani, H.; Mune, M. The efficacy of vitamin E against oxidative damage and autoantibody production in systemic lupus erythematosus: A preliminary study. Clin. Rheumatol. 2006, 26, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Marinho, A.; Carvalho, C.; Boleixa, D.; Bettencourt, A.; Leal, B.; Guimarães, J.; Neves, E.; Oliveira, J.C.; Almeida, I.; Farinha, F.; et al. Vitamin D supplementation effects on FoxP3 expression in T cells and FoxP3+/IL-17A ratio and clinical course in systemic lupus erythematosus patients: A study in a Portuguese cohort. Immunol. Res. 2017, 65, 197–206. [Google Scholar] [CrossRef]
- Piantoni, S.; Andreoli, L.; Scarsi, M.; Zanola, A.; Dall’Ara, F.; Pizzorni, C.; Cutolo, M.; Airò, P.; Tincani, A. Phenotype modifications of T-cells and their shift toward a Th2 response in patients with systemic lupus erythematosus supplemented with different monthly regimens of vitamin D. Lupus 2015, 24, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Singgih Wahono, C.; Diah Setyorini, C.; Kalim, H.; Nurdiana, N.; Handono, K. Effect of Curcuma xanthorrhiza Supplementation on Systemic Lupus Erythematosus Patients with Hypo vitamin D Which Were Given Vitamin D3 towards Disease Activity (SLEDAI), IL-6, and TGF-beta1 Serum. Int. J. Rheumatol. 2017, 2017, 7687053. [Google Scholar] [CrossRef] [PubMed]
- Wright, S.A.; O’Prey, F.M.; McHenry, M.T.; Leahey, W.J.; Devine, A.B.; Duffy, E.M.; Johnston, D.G.; Finch, M.B.; Bell, A.L.; McVeigh, G.E. A randomised interventional trial of omega-3-polyunsaturated fatty acids on endothelial function and disease activity in systemic lupus erythematosus. Ann. Rheum. Dis. 2008, 67, 841–848. [Google Scholar] [CrossRef]
- Davies, R.J.; Lomer, M.; Yeo, S.I.; Avloniti, K.; Sangle, S.R.; D’Cruz, D.P. Weight loss and improvements in fatigue in systemic lupus erythematosus: A controlled trial of a low glycaemic index diet versus a calorie restricted diet in patients treated with corticosteroids. Lupus 2012, 21, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Hewison, M. Vitamin D and the Immune System: New Perspectives on an Old Theme. Endocrinol. Metab. Clin. N. Am. 2010, 39, 365–379. [Google Scholar] [CrossRef] [PubMed]
- Lavi Arab, F.; Rastin, M.; Faraji, F.; Zamani Taghizadeh Rabe, S.; Tabasi, N.; Khazaee, M.; Haghmorad, D.; Mahmoudi, M. Assessment of 1,25-dihydroxyvitamin D3 effects on Treg cells in a mouse model of systemic lupus erythematosus. Immunopharm. Immunot. 2015, 37, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Tabasi, N.; Rastin, M.; Mahmoudi, M.; Ghoryani, M.; Mirfeizi, Z.; Rabe, S.Z.T.; Reihani, H. Influence of vitamin D on cell cycle, apoptosis, and some apoptosis related molecules in systemic lupus erythematosus. Iran. J. Basic. Med. Sci. 2015, 18, 1107–1111. [Google Scholar]
- Schneider, L.; Dos Santos, A.S.P.; Santos, M.; da Silva Chakr, R.M.; Monticielo, O.A. Vitamin D and systemic lupus erythematosus: State of the art. Clin. Rheumatol. 2014, 33, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Baeke, F.; Van Etten, E.; Overbergh, L.; Mathieu, C. Vitamin D3 and the immune system: Maintaining the balance in health and disease. Nutr. Res. Rev. 2007, 20, 106–118. [Google Scholar] [CrossRef]
- Mok, C.C. Vitamin D and systemic lupus erythematosus: An update. Expert Rev. Clin. Immunol. 2013, 9, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Gatenby, P.; Lucas, R.; Swaminathan, A. Vitamin D deficiency and risk for rheumatic diseases: An update. Curr. Opin. Rheumatol. 2013, 25, 184–191. [Google Scholar] [CrossRef]
- Terrier, B.; Derian, N.; Schoindre, Y.; Chaara, W.; Geri, G.; Zahr, N.; Mariampillai, K.; Rosenzwajg, M.; Carpentier, W.; Musset, L.; et al. Restoration of regulatory and effector T cell balance and B cell homeostasis in systemic lupus erythematosus patients through vitamin D supplementation. Arthritis Res. Ther. 2012, 14, R221. [Google Scholar] [CrossRef] [PubMed]
- Psarras, A.; Emery, P.; Vital, E.M. Type I Interferon-Mediated Autoimmune Diseases: Pathogenesis, diagnosis, and targeted therapy. Rheumatology 2017, 56, 1662–1675. [Google Scholar] [CrossRef]
- Caetano, M.; Terreri, M.T.; Ortíz, T.; Pinheiro, M.; Souza, F.; Sarni, R. Bone mineral density reduction in adolescents with systemic erythematosus lupus: Association with lack of vitamin D supplementation. Clin. Rheumatol. 2015, 34, 2065–2070. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Xie, C.; Han, J.; Ye, Y.; Weiel, J.; Li, Q.; Blanco, I.; Ahn, C.; Olsen, N.; Putterman, C.; et al. Metabolic Disturbances Associated with Systemic Lupus Erythematosus. PLoS ONE 2012, 7, e37210. [Google Scholar] [CrossRef]
- Duarte-García, A.; Myasoedova, E.; Karmacharya, P.; Hocaoğlu, M.; Murad, M.H.; Warrington, K.J.; Crowson, C.S. Effect of omega-3 fatty acids on systemic lupus erythematosus disease activity: A systematic review and meta-analysis. Autoimmun. Rev. 2020, 19, 102688. [Google Scholar] [CrossRef]
- Akbar, U.; Yang, M.; Kurian, D.; Mohan, C. Omega-3 Fatty Acids in Rheumatic Diseases: A Critical Review. J. Clin. Rheumatol. 2017, 23, 330–339. [Google Scholar] [CrossRef]
- Gaitonde, S.; Samols, D.; Kushner, I. C-reactive protein and systemic lupus erythematosus. Arthritis Care Res. 2008, 59, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- Firooz, N.; Albert, D.; Wallace, D.; Ishimori, M.; Berel, D.; Weisman, M. High-sensitivity C-reactive protein and erythrocyte sedimentation rate in systemic lupus erythematosus. Lupus 2011, 20, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Chessa, E.; Piga, M.; Floris, A.; Devilliers, H.; Cauli, A.; Arnaud, L. Use of Physician Global Assessment in systemic lupus erythematosus: A systematic review of its psychometric properties. Rheumatology 2020, 59, 3622–3632. [Google Scholar] [CrossRef] [PubMed]
- Haque, S.; Skeoch, S.; Rakieh, C.; Edlin, H.; Ahmad, Y.; Ho, P.; Gorodkin, R.; Alexander, M.Y.; Bruce, I.N. Progression of subclinical and clinical cardiovascular disease in a UK SLE cohort: The role of classic and SLE-related factors. Lupus Sci. Med. 2018, 5, e000267. [Google Scholar] [CrossRef] [PubMed]
- Schulz, E.; Gori, T.; Münzel, T. Oxidative stress and endothelial dysfunction in hypertension. Hypertens. Res. 2011, 34, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Pajak, A.; Marventano, S.; Castellano, S.; Galvano, F.; Bucolo, C.; Drago, F.; Caraci, F. Role of Omega-3 Fatty Acids in the Treatment of Depressive Disorders: A Comprehensive Meta-Analysis of Randomized Clinical Trials. PLoS ONE 2014, 9, e96905. [Google Scholar] [CrossRef] [PubMed]
- Fenton, J.I.; Hord, N.G.; Ghosh, S.; Gurzell, E.A. Immunomodulation by dietary long chain omega-3 fatty acids and the potential for adverse health outcomes. Prostaglandins Leukot. Essent. Fat. Acids 2013, 89, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Rezaieyazdi, Z.; Sahebari, M.; Saadati, N.; Khodashahi, M. Vitamin E and Autoimmune Diseases: A Narrative Review. Rev. Clin. Med. 2018, 5, 42–48. [Google Scholar]
- Hsieh, C.-C.; Lin, B.-F. The effects of vitamin E supplementation on autoimmune-prone New Zealand black × New Zealand white F1 mice fed an oxidised oil diet. Br. J. Nutr. 2005, 93, 655–662. [Google Scholar] [CrossRef]
- Hsieh, C.-C.; Lin, B.-F. Opposite effects of low and high dose supplementation of vitamin E on survival of MRL/lpr mice. Nutrition 2005, 21, 940–948. [Google Scholar] [CrossRef]
- Miller, E.R., III; Pastor-Barriuso, R.; Dalal, D.; Riemersma, R.A.; Appel, L.J.; Guallar, E. Meta-Analysis: High-Dosage Vitamin E Supplementation May Increase All-Cause Mortality. Ann. Intern. Med. 2005, 142, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Anand, P.; Kunnumakkara, A.B.; Newman, R.A.; Aggarwal, B.B. Bioavailability of curcumin: Problems and promises. Mol. Pharm. 2007, 4, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Mohan, C.; Putterman, C. Genetics and pathogenesis of systemic lupus erythematosus and lupus nephritis. Nat. Rev. Nephrol. 2015, 11, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Kim, H.; Lee, G.; Chung, H.-S.; Bae, H. Curcumin attenuates lupus nephritis upon interaction with regulatory T cells in New Zealand Black/White mice. Br. J. Nutr. 2012, 110, 69–76. [Google Scholar] [CrossRef]
- Wang, M.; Zhou, G.; Lv, J.; Zeng, P.; Guo, C.; Wang, Q. Curcumin modulation of the activation of PYK2 in peripheral blood mononuclear cells from patients with lupus nephritis. Rheumatology 2017, 55, 269–275. [Google Scholar] [CrossRef]
- Handono, K.; Pratama, M.Z.; Endharti, A.T.; Kalim, H. Treatment of low doses curcumin could modulate Th17/Treg balance specifically on CD4+ T cell cultures of systemic lupus erythematosus patients. Cent. Eur. J. Immunol. 2015, 40, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Khajehdehi, P.; Zanjaninejad, B.; Aflaki, E.; Nazarinia, M.; Azad, F.; Malekmakan, L.; Dehghanzadeh, G.-R. Oral Supplementation of Turmeric Decreases Proteinuria, Hematuria, and Systolic Blood Pressure in Patients Suffering From Relapsing or Refractory Lupus Nephritis: A Randomized and Placebo-controlled Study. J. Ren. Nutr. 2012, 22, 50–57. [Google Scholar] [CrossRef]
- Scrivo, R.; Massaro, L.; Barbati, C.; Vomero, M.; Ceccarelli, F.; Spinelli, F.R.; Riccieri, V.; Spagnoli, A.; Alessandri, C.; Desideri, G.; et al. The role of dietary sodium intake on the modulation of T helper 17 cells and regulatory T cells in patients with rheumatoid arthritis and systemic lupus erythematosus. PLoS ONE 2017, 12, e0184449. [Google Scholar] [CrossRef]
- Tsigalou, C.; Konstantinidis, T.; Paraschaki, A.; Stavropoulou, E.; Voidarou, C.; Bezirtzoglou, E. Mediterranean Diet as a Tool to Combat Inflammation and Chronic Diseases. An Overview. Biomedicines 2020, 8, 201. [Google Scholar] [CrossRef] [PubMed]
- Robinson, G.A.; Mcdonnell, T.; Wincup, C.; Martin-Gutierrez, L.; Wilton, J.; Kalea, A.Z.; Ciurtin, C.; Pineda-Torra, I.; Jury, E.C. Diet and lupus: What do the patients think? Lupus 2019, 28, 755–763. [Google Scholar] [CrossRef]
- Knippenberg, A.; Robinson, G.A.; Wincup, C.; Ciurtin, C.; Jury, E.C.; Kalea, A.Z. Plant-based dietary changes may improve symptoms in patients with systemic lupus erythematosus. Lupus 2022, 31, 65–76. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study (Country) | Study Design | Sample Size (n) | Intervention (Control Group) | Duration (Year (yr); Month (m); Week (wk)) | Main Findings | Quality Assessment Rating |
|---|---|---|---|---|---|---|
| Andreoli et al., 2015 [16] (Italy) | Randomised prospective study with cross-over design | 34 female patients with SLE | Vitamin D3 supplements; switch to the alternative dose after one year Intervention: Intensive Dose: 7500 μg vit D3 initial intake, then 1250 μg/m as maintenance Control Group: Standard Dose: 625 μg/m | 2 yr | Intensive vit D supplement dose was safe and restored vit D (higher ratio of patients in the sufficiency range when compared with the same ratio in control group (75% vs. 28%, p.0.001). Control group: negative effect on 25− OH vit D levels, with a decline in the rate of sufficient patients from 64% to 38%. No significant changes in disease outcomes. Possible selection bias. | Ø |
| Piantoni et al., 2015 [20] (Italy) | Randomised prospective study with cross-over design | 34 female patients with SLE | Vitamin D3 supplements for vit D deficient patients; switch to the alternative dose after one year Intervention: Intensive Dose: 7500 μg vit D3 initial intake, then 1250 μg/m as maintenance Control Group: Standard Dose: 625 μg/m | 2 yr | Enhanced regulation T cells, seemed to have immunomodulatory effect. Intervention group: reduction in the IFN-γ/IL-4 ratio (from 12.1 to 3.2; p = 0.01) among CD8+T cells. The reduction in this ratio in the control group was not statistically significant (from 7.5 to 5.6) suggesting a role of vit D in modulating cytokines balance: supressed Th1 pathway and promoted Th2 pathway. | + |
| Aranow et al., 2015 [17] (USA) | Double-blind placebo-controlled trial | 3 male, 51 female patients with SLE | Interventions: Low-dose group: oral vitamin D3 50 μg/d High-dose group: 100 μg/d Control Group: Placebo | 12 wks | Vit D supplementation restored vit D levels. High-dose supplementation was safe. No changes in expression of IFN signature and IFNα-inducible genes. Disease activity observed in both groups remained stable and was independent of supplements. | + |
| Shirzadi, Karimzadeh and Karimifar, 2017 [18] (Iran) | Double-blind placebo-controlled RCT | 9 male, 81 female patients with SLE | Intervention group: Oral vitamin D3 1250 μg/wk for first 3 m, then 1250 μg/m for 6 m Control Group: Placebo | 9 m | Vit D supplements significantly improved vit D levels in intervention group (17.36 ± 4.26 ng/mL vs. baseline 37.69 ± 5.92 ng/mL, p < 0.001). The mean of vitamin D had no significant difference before and after intervention in placebo group (16.78 ± 4.39 ng/mL vs. 16.62 ± 4.61 ng/mL, p = 0.53). No significant improvement in disease activity (mean of disease activity (SLEDAI) was not different significantly before and after vit D administration (3.09 ± 2.36 vs.1.62 ± 1.25, p = 0.39). | + |
| Marinho et al. 2017 [19] (Portugal) | Prospective cross-sectional study with dose escalating protocol | 1 male, 23 female patients with SLE | Intervention dose was determined based on patients’ vit D levels Baseline: <50 nmol/L: 1250 μg/wk cholecalciferol/ for 8 wks, then 50 μg/d >50 nmol/L and <75 nmol/L: 100 μg/d for 8 weeks, then 50 μg/d >75 nmol/L: 50 μg/d 3-month follow-up: <50 nmol/L: 1250 μg/wk cholecalciferol/for 8 wks, then 50 μg/d >50 nmol/L and <75 nmol/L: 100 μg/d for 8 weeks, then 100 μg/d >75 nmol/L and <125 nmol/L: 50 μg/d >125 nmol/L: 25 μg/d | 6 m | Vit D supplementation -safe therapy; significantly increased vit D levels; decreased disease activity; beneficial immunological effects: increased FoxP3+ expression in CD4+ T cells, decreased CD4+IL-17A, improved Treg/Th17 ratio, an effect described for the first time in SLE patients, of real benefit, as shown by the effective decrease in the SLEDAI scores. Highlighted the importance of individualised supplements dose for patients. | Ø |
| Al-Kushi et al., 2018 [15] (Saudi Arabia) | Prospective interventional study | 15 male, 66 female patients with SLE | Intervention: Corticosteroid Treatment w/Supplementation Group: Mean prednisone dose: 7.3 ± 3.1 mg/d, with (35 μg cholecalciferol + 1250 mg calcium carbonate tablet/d) Control groups:
| 6 m | Vitamin D and calcium intake benefited the side effect of corticosteroids. Significantly increased serum vitamin level. Significantly increased bone mass density and decreased the frequency of osteopenia and osteoporosis. Intervention group: BMD improvements in T-scores (p = 0.002); the frequency of osteopenia decreased from 40% (n = 12) at baseline to 16.7% (n = 5); frequency of osteoporosis decreased from 26.7% (n = 8) to 13.3% (n = 4). In the other two control groups after 6 months osteopenia prevalence increased while there was no change in the number of osteoporotic patients. No significant improvement in immune markers and disease activity. | + |
| Study (Country) | Study Design | Sample Size (n) | Intervention (Control Group) | Duration | Main Findings | Quality Assessment Rating |
|---|---|---|---|---|---|---|
| Arriens et al., 2015 [21] (USA) | Single-blind (patients) placebo-controlled RCT | 7 male, 25 female patients with SLE | Intervention group: 6 capsules fish oil/day (2.25 g EPA and 2.25 g DHA) Control group: 6 capsules placebo/day (purified olive oil) | 6 m | Fish oil intake resulted in a trend of improvement in fatigue and emotional well-being under the RAND SF-36 scale in treatment (median change of 10) vs. placebo (−2.50), p = 0.092, but no significant difference in FSS score. Improved disease activity under PGA score in treatment (median change of −0.550) vs. placebo (0.50), p = 0.015, but no significant change in SLEDAI scores. Significantly decreased ESR in treatment (median change of −5.0 mm/h) vs. placebo (4.5 mm/h), p = 0.008 and IL-12 levels (−16.13 vs. 8.54, p = 0.058), but increased IL-13 levels (−3.89 vs. −16.86, p = 0.033), suggesting reduced inflammation. | Ø |
| Bello et al., 2013 [22] (USA) | Double-blind placebo-controlled RCT | 5 male, 80 female patients with SLE | Intervention group: Omega-3 3 g (1.8 g EPA and 1.2 g DHA) Control group: Placebo (corn starch) | 12 wks | Omega-3 intake might increase total cholesterol and LDL-cholesterol (average increase in treatment group of 3.11 ± 21.99 mg/dL vs. placebo of 1.87 ± 18.29 mg/dL, p = 0.0266). No significant differences in flow-mediated dilation, inflammatory markers, and disease activity in the two groups. | + |
| Borges et al., 2017 [23] (Brazil) | RCT | 49 female patients with SLE | Intervention group: Oral omega-3 fatty acids (1.08 g EPA and 0.2 g DHA/d) Control group: Maintain habitual diet | 12 wks | Omega-3 supplements decreased serum CRP level in the treatment group (median from 5.0 (4.9–8.1) to 4.9 (4.9–7.2) ), compared with an increase in the control group, p = 0.008). No significant differences in IL-6 and IL-10 cytokines, adiponectin, and leptin levels. Omega-3 intakes increased serum cholesterol (median from 168.0 (151.0–194.0) to 188.0 (162.0–214.5), p = 0.12) and LDL-cholesterol (median from 95.0 (80.0–116.0) to 115.5 (90.0–129.2), p = 0.003), although they remained within normal limits. | + |
| Wright et al., 2008 [25] (UK-Northern Ireland) | Randomised intervention trial | 4 male, 56 female patients with SLE (4 dropped out) | Intervention group: Omacor 4 capsules/d (1.8 g EPA and 1.2 g DHA) Control group: Placebo 4 capsules/day (olive oil) | 24 wks | Low-dose omega-3 PUFAs supplement improved disease activity; SLAM-R (from 9.4 (SD 3.0) to 6.3 (2.5), p < 0.001) and BILAG (from 13.6 (6.0) to 6.7 (3.8), p < 0.001). It also improved endothelial function; reduced FMD (from 3.0% (−0.5 to 8.2) to 8.9% (1.3 to 16.9), p < 0.001). It also reduced oxidative stress; platelet 8-isoprostanes (from 177 pg/mg protein (23–387) to 90 pg/mg protein (32–182), p = 0.007). | + |
| Lozovoy et al., 2015 [24] (Brazil) | Double-blind placebo-controlled trial | 5 male, 57 female patients with SLE | Intervention group: Fish oil n-3 fatty acids 3 g/d (10 capsules, equal to 1.8 g EPA and 1.2 g DHA originated from sardines) Control group: Maintain habitual diet | 4 m | Fish oil supplement significantly decreased triacylglycerol (from 112.0 (69.0–143.0) to 95.5 (79.3–129.8), p = 0.039) but increased total cholesterol (from 193.0 (162.0–216.0) to 205.0 (181.8–232.3), p = 0.026). Observed increased plasma adiponectin (p ˂ 0.026) and reduced leptin (p ˂ 0.024) level, suggesting potential benefit of reducing cardiovascular risk. Also observed a significant reduction in disease activity (from 2 (0–10) to 0 (0–6), p = 0.0232) in the treatment group. | + |
| Study (Country) | Study Design | Sample Size (n) | Intervention | Duration | Main Findings | Quality Assessment Rating |
|---|---|---|---|---|---|---|
| Maeshima et al., 2007 [26] (Japan) | Non-randomised intervention trial (Preliminary study) | 3 male, 33 female patients with SLE | Intervention group: Oral vit E 150–300 mg/d with PSL Control group: PSL only | 3 to 48 months (22.8 ± 16.8 months) | Lower anti-ds DNA antibody titre in the intervention group vs. treatment group (during intense sunlight: 17.9 ± 20.3 IU/L vs. 66.3 ± 76.8 IU/L, respectively; during the remainder of the year 16.3 ± 19.4 IU/L vs. 55.8 ± 59 IU/L, respectively) No significant difference of urinary 8-OHdG observed. Vitamin E might regulate antibody and autoantibody production independent of antioxidant activity. | Ø |
| Study (Country) | Study Design | Sample Size (n) | Intervention | Duration | Main Findings | Quality Assessment Rating |
|---|---|---|---|---|---|---|
| Singgih Wahono et al., 2017 [27] (Indonesia) | Double-blind RCT | 39 patients with SLE | Intervention group: Cholecalciferol 30 μg/d + Curcuma xanthorrhiza 60 mg/d Control group: Cholecalciferol 30 μg/d + placebo tablet/d | 3 m | Increased serum vitamin D, TGF-𝛽1 level, decreased IL-6 level and improved disease activity in both groups. No different effect by curcumin supplements. SLEDAI score had a moderate positive correlation with serum IL-6 level (r = 0.569, p = 0.000) but not with TGF-β1 (r = 0.055, p = 0.74). | + |
| Study | Study Design | Sample Size (n) | Intervention | Duration | Main Findings | Quality Assessment Rating |
|---|---|---|---|---|---|---|
| Davies et al., 2012 [28] (UK) | Clinical trial | 23 female patients with SLE | Low-GI diet: Carbohydrate 45 g/d with low-GI food, no restriction of protein and fat Macronutrient composition (% total energy intake, Kcal/day): 10–15% carbohydrate, 25% protein, 60% fat (saturated and unsaturated); calories ad libitum Low-calorie diet: 2000 Kcal/day Macronutrient composition (% total energy intake): 50% Carbohydrate, 15% Protein, 30% Fat Study Duration: 6 weeks | 6 wks | Both low-GI and low-calorie diets were safe and well-tolerated. Significant weight loss in both groups of participants who use low-dose corticosteroid: low-GI diet group 3.9 ± 0.9 kg; low-calorie diet group 2.4 ± 2.2 kg; p < 0.01 for both groups from baseline values. No significant difference in the effect of two diets. No significant changes within or between groups in disease activity, cardiovascular biomarkers, insulin sensitivity. Weight loss and diet intervention might contribute to improvement in fatigue. | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiao, H.; Acar, G.; Robinson, G.A.; Ciurtin, C.; Jury, E.C.; Kalea, A.Z. Diet and Systemic Lupus Erythematosus (SLE): From Supplementation to Intervention. Int. J. Environ. Res. Public Health 2022, 19, 11895. https://doi.org/10.3390/ijerph191911895
Jiao H, Acar G, Robinson GA, Ciurtin C, Jury EC, Kalea AZ. Diet and Systemic Lupus Erythematosus (SLE): From Supplementation to Intervention. International Journal of Environmental Research and Public Health. 2022; 19(19):11895. https://doi.org/10.3390/ijerph191911895
Chicago/Turabian StyleJiao, Hanxiao, Gizem Acar, George A. Robinson, Coziana Ciurtin, Elizabeth C. Jury, and Anastasia Z. Kalea. 2022. "Diet and Systemic Lupus Erythematosus (SLE): From Supplementation to Intervention" International Journal of Environmental Research and Public Health 19, no. 19: 11895. https://doi.org/10.3390/ijerph191911895