
Prevention from Sharp Injuries in the Hospital Sector: An Italian National Observatory on the Implementation of the Council Directive 2010/32/EU before and during the COVID-19 Pandemic
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey: Structure and Method of Administration of Interviews
2.2. Sample of Hospitals
2.3. Target of the Interviews
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Surveys Results
- Knowledge of the requirements of the Legislative Decree 19/02/2014 (implementing the Directive 2010/32/EU)
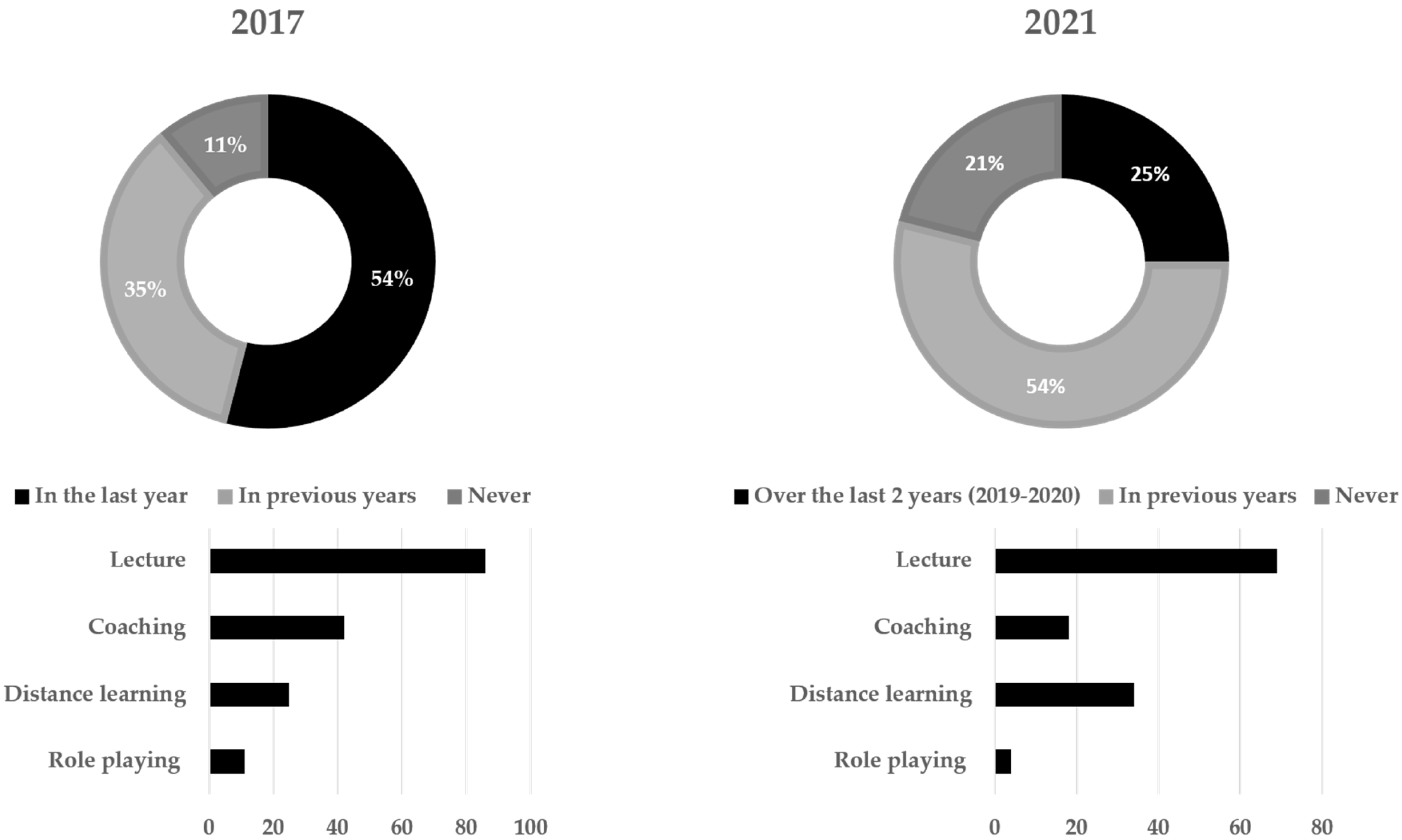
- Information, Education and Training
- Behaviors regarding the use and elimination of sharps
- Adoption of devices integrating a safety mechanism (safety-engineered devices, SED)
- Vaccinations
- Injuries, reporting and post-exposure protocol
- Obstacles to achieving sharps safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Council Directive 2010/32/EU of 10 May 2010 Implementing the Framework Agreement on Prevention from Sharp Injuries in the Hospital and Healthcare Sector Concluded by HOSPEEM and EPSU (Text with EEA Relevance). Off. J. Eur. Union 2010, L134/66, 66–72. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A32010L0032 (accessed on 14 June 2022).
- Centers for Disease Control (CDC). Recommendations for Prevention of HIV Transmission in Health-Care Settings. MMWR Suppl. 1987, 36, 1S–18S. [Google Scholar]
- Henderson, D.K.; Fahey, B.J.; Willy, M.; Schmitt, J.M.; Carey, K.; Koziol, D.E.; Lane, H.C.; Fedio, J.; Saah, A.J. Risk for occupational transmission of human immunodeficiency virus type 1 (HIV-1) associated with clinical exposures. A prospective evaluation. Ann. Intern. Med. 1990, 113, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, G.; Puro, V.; De Carli, G. The risk of occupational human immunodeficiency virus infection in health care workers. Italian Multicenter Study. The Italian Study Group on Occupational Risk of HIV infection. Arch. Intern. Med. 1993, 153, 1451–1458. [Google Scholar] [CrossRef] [PubMed]
- Cardo, D.M.; Culver, D.H.; Ciesielski, C.A.; Srivastava, P.U.; Marcus, R.; Abiteboul, D.; Heptonstall, J.; Ippolito, G.; Lot, F.; McKibben, P.S.; et al. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N. Engl. J. Med. 1997, 337, 1485–1490. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, G. Canada adopts nationwide needlestick surveillance system-EPINet. Infect. Control Hosp. Epidemiol. 1993, 14, 605. [Google Scholar] [CrossRef] [PubMed]
- Jagger, J.; Hunt, E.H.; Brand-Elnaggar, J.; Pearson, R.D. Rates of needle-stick injury caused by various devices in a university hospital. N. Engl. J. Med. 1988, 319, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Linnemann, C.C., Jr.; Cannon, C.; DeRonde, M.; Lanphear, B. Effect of educational programs, rigid sharps containers, and universal precautions on reported needlestick injuries in healthcare workers. Infect. Control Hosp. Epidemiol. 1991, 12, 214–219. [Google Scholar] [CrossRef]
- Haiduven, D.J.; DeMaio, T.M.; Stevens, D.A. A five-year study of needlestick injuries: Significant reduction associated with communication, education, and convenient placement of sharps containers. Infect. Control Hosp. Epidemiol. 1992, 13, 265–271. [Google Scholar] [CrossRef]
- Beekmann, S.E.; Vlahov, D.; Koziol, D.E.; McShalley, E.D.; Schmitt, J.M.; Henderson, D.K. Temporal association between implementation of universal precautions and a sustained, progressive decrease in percutaneous exposures to blood. Clin. Infect. Dis. 1994, 18, 562–569. [Google Scholar] [CrossRef]
- Haiduven, D.J.; Phillips, E.S.; Clemons, K.V.; Stevens, D.A. Percutaneous injury analysis: Consistent categorization, effective reduction methods, and future strategies. Infect. Control Hosp. Epidemiol. 1995, 16, 582–589. [Google Scholar] [CrossRef]
- Elder, A.; Paterson, C. Sharps injuries in UK health care: A review of injury rates, viral transmission and potential efficacy of safety devices. Occup. Med. 2006, 56, 566–574. [Google Scholar] [CrossRef] [Green Version]
- Tosini, W.; Ciotti, C.; Goyer, F.; Lolom, I.; L’Hériteau, F.; Abiteboul, D.; Pellissier, G.; Bouvet, E. Needlestick injury rates according to different types of safety-engineered devices: Results of a French multicenter study. Infect. Control Hosp. Epidemiol. 2010, 31, 402–407. [Google Scholar] [CrossRef]
- Tarigan, L.H.; Cifuentes, M.; Quinn, M.; Kriebel, D. Prevention of needle-stick injuries in healthcare facilities: A meta-analysis. Infect. Control Hosp. Epidemiol. 2015, 36, 823–829. [Google Scholar] [CrossRef]
- Ippolito, G.; De Carli, G.; Puro, V.; Petrosillo, N.; Arici, C.; Bertucci, R.; Bianciardi, L.; Bonazzi, L.; Cestrone, A.; Daglio, M.; et al. Device-specific risk of needlestick injury in Italian health care workers. JAMA 1994, 272, 607–610. [Google Scholar] [CrossRef]
- Puro, V.; De Carli, G.; Petrosillo, N.; Ippolito, G. Risk of exposure to bloodborne infection for Italian healthcare workers, by job category and work area. Studio Italiano Rischio Occupazionale da HIV Group. Infect. Control Hosp. Epidemiol. 2001, 22, 206–210. [Google Scholar] [CrossRef]
- Abu-Gad, H.A.; Al-Turki, K.A. Some epidemiological aspects of needle stick injuries among the hospital health care workers: Eastern Province, Saudi Arabia. Eur. J. Epidemiol. 2001, 17, 401–407. [Google Scholar] [CrossRef]
- Martins, A.; Coelho, A.C.; Vieira, M.; Matos, M.; Pinto, M.L. Age and years in practice as factors associated with needlestick and sharps injuries among health care workers in a Portuguese hospital. Accid. Anal. Prev. 2012, 47, 11–15. [Google Scholar] [CrossRef]
- Nsubuga, F.M.; Jaakkola, M.S. Needle stick injuries among nurses in sub-Saharan Africa. Trop. Med. Int. Health. 2005, 10, 773–781. [Google Scholar] [CrossRef]
- Richard, V.S.; Kenneth, J.; Ramaprabha, P.; Kirupakaran, H.; Chandy, G.M. Impact of introduction of sharps containers and of education programmes on the pattern of needle stick injuries in a tertiary care centre in India. J. Hosp. Infect. 2001, 47, 163–165. [Google Scholar] [CrossRef]
- Clarke, S.P.; Rockett, J.L.; Sloane, D.M.; Aiken, L.H. Organizational climate, staffing, and safety equipment as predictors of needlestick injuries and near-misses in hospital nurses. Am. J. Infect. Control 2002, 30, 207–216. [Google Scholar] [CrossRef]
- Alonso, A. Cementing sharps safety in the European Union: The importance of complying with the 2010 EU Council Directive on Sharps Injury Prevention. J. Nurs. Care 2014, 3, 169. [Google Scholar] [CrossRef] [Green Version]
- Needlestick Safety and Prevention Act of 2000. Pub. L. No. 106-430, 114 Stat. 1901; 6 November. 2000. Available online: https://www.govinfo.gov/content/pkg/PLAW-106publ430/pdf/PLAW-106publ430.pdf (accessed on 20 August 2022).
- Phillips, E.K.; Conaway, M.R.; Jagger, J.C. Percutaneous injuries before and after the Needlestick Safety and Prevention Act. N. Engl. J. Med. 2012, 366, 670–671. [Google Scholar] [CrossRef]
- Social Dialogue. “From Needlestick to Sharps”. Available online: http://ec.europa.eu/avservices/video/player.cfm?sitelang=en&ref=I072260 (accessed on 20 August 2022).
- Ippolito, G.; Puro, V.; Petrosillo, N.; De Carli, G. Surveillance of occupational exposure to bloodborne pathogens in health care workers: The Italian national programme. Eurosurveillance 1999, 4, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Di Bari, V.; De Carli, G.; Puro, V. Gruppo Collaborativo dello Studio Italiano sul Rischio Occupazionale da HIV e Altri Patogeni a Trasmissione Ematica (SIROH). Prevenzione delle punture accidentali prima della Direttiva 2010/32/UE in un campione di ospedali italiani [Prevention of accidental needle sticks before the Directive 2010/32/EU in a sample of Italian hospitals]. Med. Lav. 2015, 106, 186–205. [Google Scholar]
- Decreto Legislativo 19 Febbraio 2014, n. 19. Attuazione della Direttiva 2010/32/UE che Attua l’Accordo Quadro, Concluso da HOSPEEM e FSESP, in Materia di Prevenzione delle Ferite da Taglio o da Punta nel Settore Ospedaliero e Sanitario. (14G00031). G.U. 2014; Volume 155, pp. 1–5. Available online: http://www.gazzettaufficiale.it/eli/gu/2014/03/10/57/sg/pdf (accessed on 21 June 2022).
- Adeyemo, O.O.; Tu, S.; Falako, S.; Keene, D. Stressors on frontline healthcare workers during the COVID-19 pandemic: A focus on moral injury and implications for the future. Int. Arch. Occup. Environ. Health 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Patients Safety Learning: The Hub. Available online: https://www.pslhub.org/learn/culture/staff-safety/sharps-injuries-and-covid-research-by-ipsos-mori-on-behalf-of-european-biosafety-network-r4905/ (accessed on 24 June 2022).
- European Biosafety Network. European Healthcare Workers Suffered an Increase of 276,000 Sharps Injuries due to COVID-19. Available online: https://www.europeanbiosafetynetwork.eu/european-healthcare-workers-suffered-an-increase-of-276000-sharps-injuries-due-to-covid-19/ (accessed on 2 May 2021).
- The World Medical Association Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 26 July 2022).
- Ministero della Salute. Open Data. Posti Letto per Struttura Ospedaliera dal 2010 al 2019. Available online: https://www.dati.salute.gov.it/dati/dettaglioDataset.jsp?menu=dati&idPag=18 (accessed on 16 June 2022).
- Gershon, R.R.; Karkashian, C.D.; Grosch, J.W.; Murphy, L.R.; Escamilla-Cejudo, A.; Flanagan, P.A.; Bernacki, E.; Kasting, C.; Martin, L. Hospital safety climate and its relationship with safe work practices and workplace exposure incidents. Am. J. Infect. Control 2000, 28, 211–221. [Google Scholar] [CrossRef]
- De Carli, G.; National Institute for Infectious Diseases L. Spallanzani—IRCCS, Rome, Italy. Personal communication, 2018.
- Tuma, S.; Sepkowitz, K.A. Efficacy of safety-engineered device implementation in the prevention of percutaneous injuries: A review of published studies. Clin. Infect. Dis. 2006, 42, 1159–1170. [Google Scholar] [CrossRef]
- Reddy, V.K.; Lavoie, M.C.; Verbeek, J.H.; Pahwa, M. Devices for preventing percutaneous exposure injuries caused by needles in healthcare personnel. Cochrane Database Syst. Rev. 2017, 11, CD009740. [Google Scholar] [CrossRef]
- Lamontagne, F.; Abiteboul, D.; Lolom, I.; Pellissier, G.; Tarantola, A.; Descamps, J.M.; Bouvet, E. Role of safety-engineered devices in preventing needlestick injuries in 32 French hospitals. Infect. Control Hosp. Epidemiol. 2007, 28, 18–23. [Google Scholar] [CrossRef]
- Cullen, B.L.; Genasi, F.; Symington, I.; Bagg, J.; McCreaddie, M.; Taylor, A.; Henry, M.; Hutchinson, S.J.; Goldberg, D.J. Potential for reported needlestick injury prevention among healthcare workers through safety device usage and improvement of guideline adherence: Expert panel assessment. J. Hosp. Infect. 2006, 63, 445–451. [Google Scholar] [CrossRef]
- Ottino, M.C.; Argentero, A.; Argentero, P.A.; Garzaro, G.; Zotti, C.M. Needlestick prevention devices: Data from hospital surveillance in Piedmont, Italy-comprehensive analysis on needlestick injuries between healthcare workers after the introduction of safety devices. BMJ Open 2019, 9, e030576. [Google Scholar] [CrossRef]
- Dulon, M.; Stranzinger, J.; Wendeler, D.; Nienhaus, A. Causes of Needlestick and Sharps Injuries When Using Devices with and without Safety Features. Int. J. Environ. Res. Public Health 2020, 17, 8721. [Google Scholar] [CrossRef]
- Nioi, M.; Napoli, P.E.; Lobina, J.; Fossarello, M.; d’Aloja, E. COVID-19 and Italian Healthcare Workers from the initial sacrifice to the mRNA vaccine: Pandemic chrono-history, epidemiological data, ethical dilemmas, and future challenges. Front. Public Health 2021, 8, 591900. [Google Scholar] [CrossRef]
- ASTRID. Available online: https://www.astrid-online.it/static/upload/impa/impatto-covid-su-ricoveri-ospedalieri-istat-agenas.pdf (accessed on 30 June 2022).
- Palese, A.; Brugnolli, A.; Achil, I.; Mattiussi, E.; Fabris, S.; Kajander-Unkuri, S.; Dimonte, V.; Grassetti, L.; Danielis, M. The first COVID-19 new graduate nurses generation: Findings from an Italian cross-sectional study. BMC Nurs. 2022, 21, 101. [Google Scholar] [CrossRef]
- Corbaz-Kurth, S.; Juvet, T.M.; Benzakour, L.; Cereghetti, S.; Fournier, C.A.; Moullec, G.; Nguyen, A.; Suard, J.C.; Vieux, L.; Wozniak, H.; et al. How things changed during the COVID-19 pandemic’s first year: A longitudinal, mixed-methods study of organisational resilience processes among healthcare workers. Saf. Sci. 2022, 155, 105879. [Google Scholar] [CrossRef]
- Diktas, H.; Oncul, A.; Tahtasakal, C.A.; Sevgi, D.Y.; Kaya, O.; Cimenci, N.; Uzun, N.; Dokmetas, I. What were the changes during the COVID-19 pandemic era concerning occupational risks among health care workers? J. Infect. Public Health 2021, 14, 1334–1339. [Google Scholar] [CrossRef]
- Vieira, C.; Góis, J.; Laranjeira, P.; Pinho, P.; Norton, P. Underreporting of work accidents associated with blood-borne risk factors. Med. Lav. 2022, 113, e2022028. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Geographical Area | 200 Beds | 201–500 Beds | >500 Beds | Total | ||||
|---|---|---|---|---|---|---|---|---|
| 2017 | 2021 | 2017 | 2021 | 2017 | 2021 | 2017 | 2021 | |
| North-West | 4 | 6 | 8 | 15 | 10 | 11 | 22 | 32 |
| North-East | 7 | 1 | 4 | 9 | 4 | 10 | 15 | 20 |
| Center | 8 | 5 | 11 | 11 | 5 | 10 | 24 | 26 |
| South-Islands | 9 | 4 | 16 | 15 | 11 | 20 | 36 | 39 |
| Total | 28 | 16 | 39 | 50 | 30 | 51 | 97 | 117 |
| Safety-Engineered Devices | Nurses | Safety Managers | Hospital Pharmacists | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2017 | 2021 | 2017 | 2021 | |||||||
| 180 | 150 | 135 | 85 | |||||||
| N | % | N | % | p-Value | N | % | N | % | p-Value | |
| Vacuum-tube phlebotomy sets | ||||||||||
| Routinely available and used | 128 | 71 | 134 | 89 | 0.0001 | 86 | 64 | 63 | 74 | 0.1441 |
| Not routinely available | 36 | 20 | 12 | 8 | 0.0035 | 36 | 27 | 15 | 18 | 0.1677 |
| Not available in the hospital | 16 | 9 | 4 | 3 | 0.0334 | 13 | 10 | 7 | 8 | 0.9128 |
| Peripheral IV catheters | ||||||||||
| Routinely available and used | 121 | 67 | 125 | 83 | 0.0013 | 86 | 64 | 60 | 71 | 0.3650 |
| Not routinely available | 43 | 24 | 18 | 12 | 0.0086 | 33 | 24 | 20 | 24 | 1.0000 |
| Not available in the hospital | 16 | 9 | 7 | 5 | 0.1996 | 16 | 12 | 5 | 6 | 0.2181 |
| Arterial Blood Sampling syringes | ||||||||||
| Routinely available and used | 101 | 56 | 77 | 51 | 0.4496 | 72 | 53 | 29 | 34 | 0.0081 * |
| Not routinely available | 34 | 19 | 47 | 31 | 0.0129 | 37 | 27 | 33 | 39 | 0.1049 |
| Not available in the hospital | 45 | 25 | 26 | 17 | 0.1204 | 26 | 19 | 23 | 27 | 0.2351 |
| Arterial catheters | ||||||||||
| Routinely available and used | 74 | 41 | 41 | 27 | 0.0124 * | 76 | 56 | 24 | 28 | 0.0001 * |
| Not routinely available | 30 | 17 | 55 | 37 | 0.0001 | 32 | 24 | 36 | 42 | 0.0057 |
| Not available in the hospital | 76 | 42 | 54 | 36 | 0.2989 | 27 | 20 | 25 | 29 | 0.1507 |
| Lancets | ||||||||||
| Routinely available and used | 99 | 55 | 114 | 76 | 0.0001 | 63 | 47 | 39 | 46 | 1.0000 |
| Not routinely available | 30 | 17 | 26 | 17 | 0.9893 | 29 | 21 | 29 | 34 | 0.0556 |
| Not available in the hospital | 51 | 28 | 10 | 7 | 0.0000 | 43 | 32 | 17 | 20 | 0.0773 |
| Syringes for subcutaneous injection | ||||||||||
| Routinely available and used | 86 | 48 | 92 | 61 | 0.0188 | 49 | 36 | 47 | 55 | 0.0086 |
| Not routinely available | 38 | 21 | 30 | 20 | 0.9110 | 36 | 27 | 18 | 21 | 0.4470 |
| Not available in the hospital | 56 | 31 | 28 | 19 | 0.0140 | 50 | 37 | 20 | 24 | 0.0517 |
| Hypodermic needles for IM injection | ||||||||||
| Routinely available and used | 76 | 42 | 77 | 51 | 0.1231 | 53 | 39 | 58 | 68 | 0.0001 |
| Not routinely available | 39 | 22 | 42 | 28 | 0.2291 | 32 | 24 | 15 | 18 | 0.3690 |
| Not available in the hospital | 65 | 36 | 31 | 21 | 0.0031 | 50 | 37 | 12 | 14 | 0.0004 |
| Insulin pen needles | ||||||||||
| Routinely available and used | 95 | 53 | 81 | 54 | 0.9118 | 68 | 50 | 39 | 46 | 0.6101 |
| Not routinely available | 35 | 19 | 41 | 27 | 0.1179 | 33 | 24 | 27 | 32 | 0.3022 |
| Not available in the hospital | 50 | 28 | 28 | 19 | 0.0703 | 34 | 25 | 19 | 22 | 0.7517 |
| Scalpels § | ||||||||||
| Routinely available and used | 74 | 41 | 51 | 34 | 0.2255 | 65 | 48 | 27 | 32 | 0.0239 * |
| Not routinely available | 25 | 14 | 54 | 36 | 0.0000 | 25 | 19 | 33 | 39 | 0.0015 |
| Not available in the hospital | 81 | 45 | 45 | 30 | 0.0074 | 45 | 33 | 25 | 29 | 0.6459 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Carli, G.; Agresta, A.; Lecce, M.G.; Marchegiano, P.; Micheloni, G.; Sossai, D.; Campo, G.; Tomao, P.; Vonesch, N.; Leone, S.; et al. Prevention from Sharp Injuries in the Hospital Sector: An Italian National Observatory on the Implementation of the Council Directive 2010/32/EU before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 11144. https://doi.org/10.3390/ijerph191711144
De Carli G, Agresta A, Lecce MG, Marchegiano P, Micheloni G, Sossai D, Campo G, Tomao P, Vonesch N, Leone S, et al. Prevention from Sharp Injuries in the Hospital Sector: An Italian National Observatory on the Implementation of the Council Directive 2010/32/EU before and during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(17):11144. https://doi.org/10.3390/ijerph191711144
Chicago/Turabian StyleDe Carli, Gabriella, Alessandro Agresta, Maria Giuseppina Lecce, Patrizia Marchegiano, Gianpaolo Micheloni, Dimitri Sossai, Giuseppe Campo, Paola Tomao, Nicoletta Vonesch, Sara Leone, and et al. 2022. "Prevention from Sharp Injuries in the Hospital Sector: An Italian National Observatory on the Implementation of the Council Directive 2010/32/EU before and during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 17: 11144. https://doi.org/10.3390/ijerph191711144