
Cognitive Function and the Ability to Operate Long-Term Oxygen Therapy Equipment: An Exploratory Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measurement
2.3.1. LTOT Equipment Operation Ability Survey
2.3.2. Lung Information Needs Questionnaire (LINQ)
2.3.3. Montreal Cognitive Assessment (MoCA)
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Patients and Their Family Members
3.2. Validity and Reliability of the Survey on the Ability to Operate LTOT Equipment
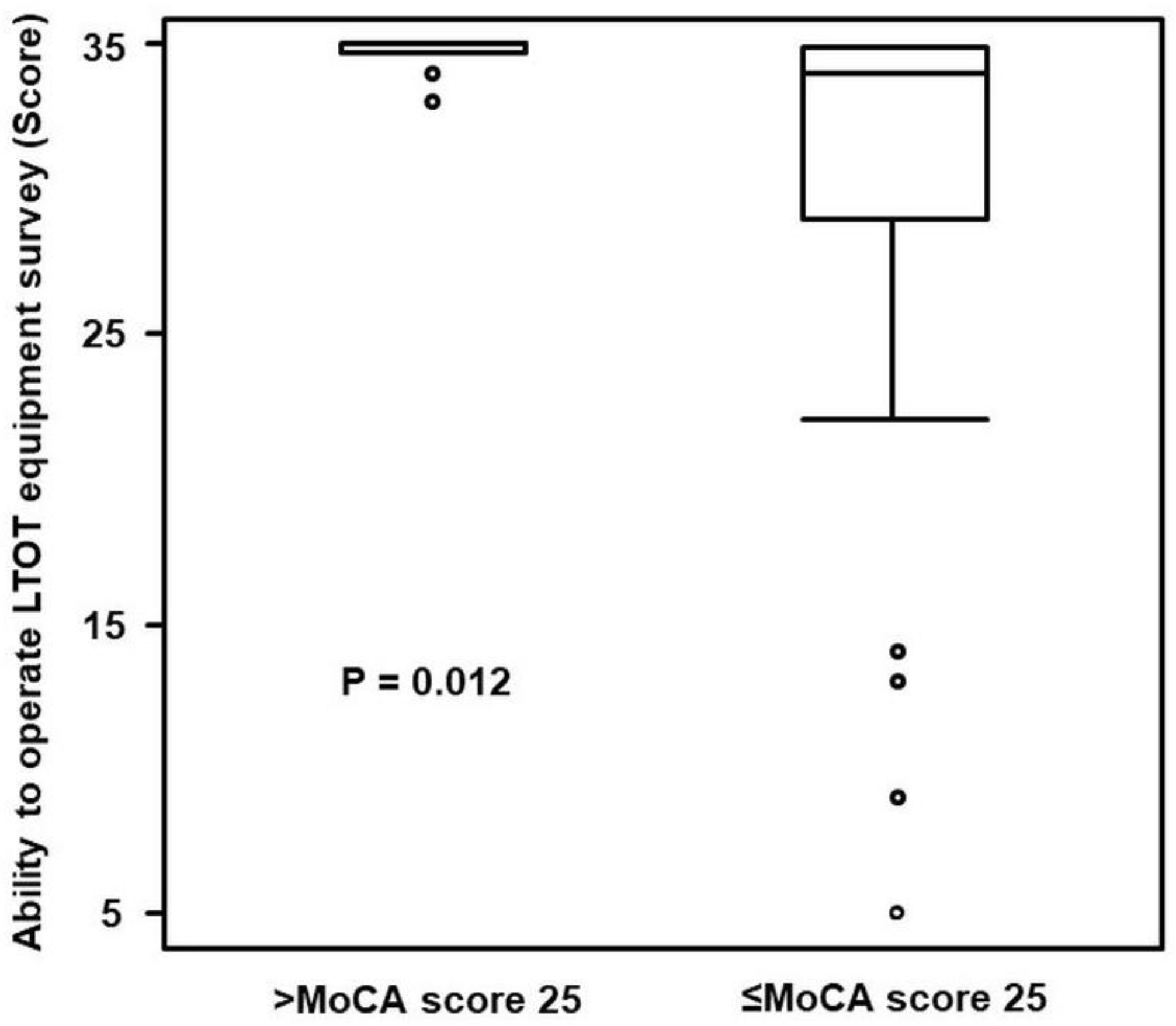
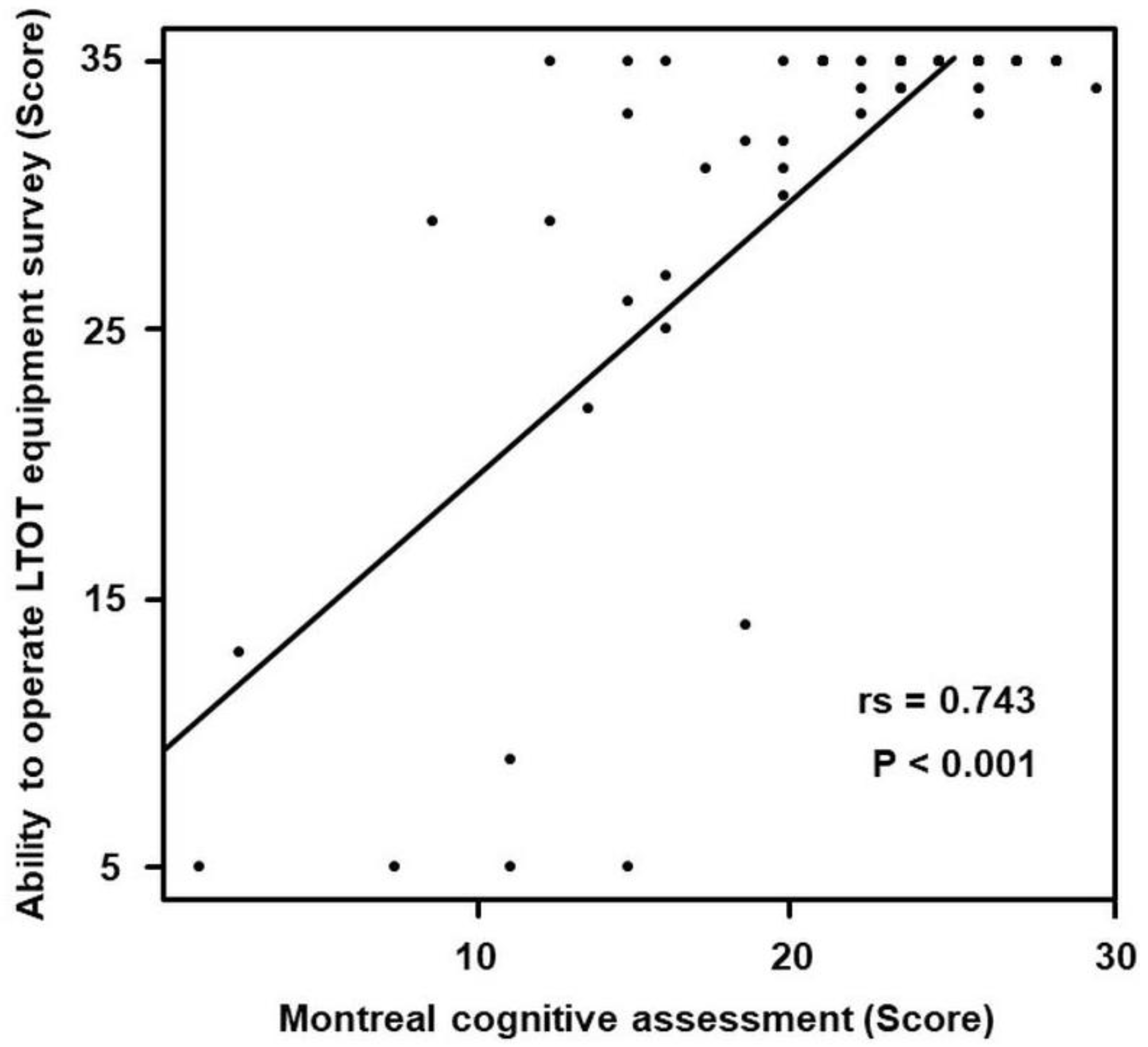
3.3. Relationship between LTOT Equipment Operation Ability Survey and MoCA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jacobs, S.S.; Krishnan, J.A.; Lederer, D.J.; Ghazipura, M.; Hossain, T.; Tan, A.M.; Carlin, B.; Drummond, M.B.; Ekström, M.; Garvey, C.; et al. Home oxygen therapy for adults with chronic lung disease. An official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 202, e121–e141. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, H.; Miyamoto, K. Oxygen Therapy, 2nd ed.; The Japanese Respiratory Society, The Japan Society for Respiratory Care and Rehabilitation: Tokyo, Japan, 2017. [Google Scholar]
- Hardinge, M.; Suntharalingam, J.; Wilkinson, T. Guideline update: The British Thoracic Society Guidelines on home oxygen use in adults. Thorax 2015, 70, 589–591. [Google Scholar] [CrossRef]
- Maekura, R.; Hiraga, T.; Miki, K.; Kitada, S.; Miki, M.; Yoshimura, K.; Yamamoto, H.; Kawabe, T.; Mori, M. Personalized pulmonary rehabilitation and occupational therapy based on cardiopulmonary exercise testing for patients with advanced chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 1787–1800. [Google Scholar] [CrossRef] [PubMed]
- Peckham, D.G.; McGibbon, K.; Tonkinson, J.; Plimbley, G.; Pantin, C. Improvement in patient compliance with long-term oxygen therapy following formal assessment with training. Respir. Med. 1998, 92, 1203–1206. [Google Scholar] [CrossRef]
- Albert, R.K.; Au, D.H.; Blackford, A.L.; Casaburi, R.; Cooper, J.A., Jr.; Criner, G.J.; Diaz, P.; Fuhlbrigge, A.L.; Gay, S.E.; Kanner, R.E.; et al. A randomized trial of long-term oxygen for COPD with moderate desaturation. N. Engl. J. Med. 2016, 375, 1617–1627. [Google Scholar] [CrossRef] [PubMed]
- Tanash, H.A.; Ringbaek, T.; Huss, F.; Ekström, M. Burn injury during long-term oxygen therapy in Denmark and Sweden: The potential role of smoking. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Semasinghe Bandaralage, S.P.; Denniss, A.R.; Syed, M.; Sriram, K.B. Long-term oxygen therapy-related adverse outcomes resulting in hospitalisation: 3-year experience of an Australian metropolitan health service. Intern. Med. J. 2019, 49, 1435–1437. [Google Scholar] [CrossRef]
- Caneiras, C.; Jácome, C.; Moreira, E.; Oliveira, D.; Dias, C.C.; Mendonça, L.; Mayoralas-Alises, S.; Fonseca, J.A.; Diaz-Lobato, S.; Escarrabill, J.; et al. A qualitative study of patient and carer experiences with home respiratory therapies: Long-term oxygen therapy and home mechanical ventilation. Pulmonology 2022, 28, 268–275. [Google Scholar] [CrossRef]
- Russ, T.C.; Kivimäki, M.; Batty, G.D. Respiratory disease and lower pulmonary function as risk factors for dementia: A systematic review with meta-analysis. Chest 2020, 157, 1538–1558. [Google Scholar] [CrossRef]
- Karamanli, H.; Ilik, F.; Kayhan, F.; Pazarli, A.C. Assessment of cognitive impairment in long-term oxygen therapy-dependent COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 2087–2094. [Google Scholar] [CrossRef]
- Annaka, H.; Nomura, T.; Moriyama, H. Sedentary time and cognitive impairment in patients using long-term oxygen therapy: A cross-sectional study. Int. J. Environ. Res. Public Health 2022, 19, 1726. [Google Scholar] [CrossRef] [PubMed]
- Grant, I.; Heaton, R.K.; McSweeny, A.J.; Adams, K.M.; Timms, R.M. Neuropsychologic findings in hypoxemic chronic obstructive pulmonary disease. Arch. Intern. Med. 1982, 142, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Nygård, L.; Starkhammar, S. The use of everyday technology by people with dementia living alone: Mapping out the difficulties. Aging Ment. Health 2007, 11, 144–155. [Google Scholar] [CrossRef]
- Rosenberg, L.; Kottorp, A.; Winblad, B.; Nygård, L. Perceived difficulty in everyday technology use among older adults with or without cognitive deficits. Scand. J. Occup. Ther. 2009, 16, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Nygård, L.; Pantzar, M.; Uppgard, B.; Kottorp, A. Detection of activity limitations in older adults with MCI or Alzheimer’s disease through evaluation of perceived difficulty in use of everyday technology: A replication study. Aging Ment. Health 2012, 16, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Baird, C.; Lovell, J.; Johnson, M.; Shiell, K.; Ibrahim, J.E. The impact of cognitive impairment on self-management in chronic obstructive pulmonary disease: A systematic review. Respir. Med. 2017, 129, 130–139. [Google Scholar] [CrossRef]
- Allen, S.C.; Jain, M.; Ragab, S.; Malik, N. Acquisition and short-term retention of inhaler techniques require intact executive function in elderly subjects. Age Ageing 2003, 32, 299–302. [Google Scholar] [CrossRef]
- O’Conor, R.; Wolf, M.S.; Smith, S.G.; Martynenko, M.; Vicencio, D.P.; Sano, M.; Wisnivesky, J.P.; Federman, A.D. Health literacy, cognitive function, proper use, and adherence to inhaled asthma controller medications among older adults with asthma. Chest 2015, 147, 1307–1315. [Google Scholar] [CrossRef]
- O’Conor, R.; Muellers, K.; Arvanitis, M.; Vicencio, D.P.; Wolf, M.S.; Wisnivesky, J.P.; Federman, A.D. Effects of health literacy and cognitive abilities on COPD self-management behaviors: A prospective cohort study. Respir. Med. 2019, 160, 105630. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Hyland, M.E.; Jones, R.C.; Hanney, K.E. The Lung Information Needs Questionnaire: Development, preliminary validation and findings. Respir. Med. 2006, 100, 1807–1816. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Villeneuve, S.; Pepin, V.; Rahayel, S.; Bertrand, J.A.; de Lorimier, M.; Rizk, A.; Desjardins, C.; Parenteau, S.; Beaucage, F.; Joncas, S.; et al. Mild cognitive impairment in moderate to severe COPD: A preliminary study. Chest 2012, 142, 1516–1523. [Google Scholar] [CrossRef] [PubMed]
- Beavers, A.S.; Lounsbury, J.W.; Richards, J.K.; Huck, S.W.; Skolits, G.; Esquivel, S.L. Practical considerations for using exploratory factor analysis in educational research. Pract. Assess. Res. Eval. 2013, 18, 1–13. [Google Scholar]
- Bland, J.M.; Altman, D.G. Cronbach’s alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef]
- Hung, W.W.; Wisnivesky, J.P.; Siu, A.L.; Ross, J.S. Cognitive decline among patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2009, 180, 134–137. [Google Scholar] [CrossRef]
- Bors, M.; Tomic, R.; Perlman, D.M.; Kim, H.J.; Whelan, T.P. Cognitive function in idiopathic pulmonary fibrosis. Chronic Respir. Dis. 2015, 12, 365–372. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Hazardous Behaviors | Adverse Events | Equipment Operation | Question |
|---|---|---|---|
| Smoking/contact with open flames | Explosion and fire | Avoidance of fire | Can you avoid causing fires while using the home oxygen equipment? |
| Poorly adjusted flow rate | Worsening respiratory failure | Adjustment of flow rates | Can you adjust the flow rate while in the toilet, in the bath, or going out? |
| Lack of understanding about portable oxygen | Running out of oxygen | Operation of portable oxygen | Can you use portable oxygen? |
| Stumbling on the equipment and portable oxygen | Falls | Avoidance of contact with the cannula and portable oxygen | Can you avoid contact with the cannula and portable oxygen? |
| Lack of understanding about the equipment | No oxygen supply | Dealing with alarms | Can you deal with alarms regarding forgetting to shut the cylinder or running out of oxygen? |
| Question 1: Can you avoid causing fires while using the home oxygen equipment? | ||||||||
| Full assistance | ① | ② | ③ | ④ | ⑤ | ⑥ | ⑦ | Completely independent |
| Question 2: Can you adjust the flow rate while in the toilet, in the bath, or going out? | ||||||||
| Full assistance | ① | ② | ③ | ④ | ⑤ | ⑥ | ⑦ | Completely independent |
| Question 3: Can you use portable oxygen? | ||||||||
| Full assistance | ① | ② | ③ | ④ | ⑤ | ⑥ | ⑦ | Completely independent |
| Question 4: Can you avoid contact with the cannula and portable oxygen? | ||||||||
| Full assistance | ① | ② | ③ | ④ | ⑤ | ⑥ | ⑦ | Completely independent |
| Question 5: Can you deal with alarms regarding forgetting to shut the cylinder or running out of oxygen? | ||||||||
| Full assistance | ① | ② | ③ | ④ | ⑤ | ⑥ | ⑦ | Completely independent |
| Characteristics | Participants (n = 60) | Families (n = 60) |
|---|---|---|
| Age (years) | 77 (6) * | 70 (11) * |
| Gender | ||
| Male | 48 (80%) † | 11 (18%) † |
| Female | 12 (20%) † | 49 (82%) † |
| Education (years) | 12.0 (9.0–12.0) ‡ | |
| Relationship with patients | ||
| Spouse | 36 (65%) † | |
| Son/daughter | 16 (27%) † | |
| Other | 8 (8%) † | |
| Disease | ||
| Chronic obstructive pulmonary disease | 24 (40%) † | |
| Interstitial pneumonia | 23 (38%) † | |
| Other | 13 (22%) † | |
| Spirometry | ||
| Forced expiratory volume 1.0% | 74.1 (50.0–89.5) ‡ | |
| Group of COPD 1 | 47.0 (39.0−53.5) ‡ | |
| Group of interstitial pneumonia | 89.6 (82.9−94.4) ‡ | |
| Group of other diseases | 71.9 (60.0−85.2) ‡ | |
| %Vital capacity | 66.4 (57.8–84.8) ‡ | |
| Group of COPD 1 | 72.4 (63.3−96.5) ‡ | |
| Group of interstitial pneumonia | 66.0 (59.0−82.4) ‡ | |
| Group of other diseases | 56.3 (40.9−69.5) ‡ | |
| mMRC 2 | 2.0 (1.0–3.0) ‡ | |
| LTOT 3 | ||
| History (months) | 13.0 (7.0–41.5) ‡ | |
| Oxygen flow (L) | 3.0 (2.0–4.0) ‡ | |
| Concentrator | 56 (92%) † | |
| Liquid oxygen | 4 (8%) † | |
| Portable oxygen | 60 (100%) † | |
| Lung Information Needs Questionnaire | 2.0 (1.0−4.75) ‡ | |
| LTOT Equipment Operation Ability Survey | 35.0 (31.0−35.0) ‡ | |
| Montreal cognitive assessment | 23.0 (18.0–25.7) ‡ | |
| score ≤ 25 | 45 (75%) † |
| Survey | Factor Loading | Cronbach’s Coefficient Alpha |
|---|---|---|
| Total score of LTOT 1 equipment operation ability survey (questions 1−5) | − | 0.932 |
| Question 1 Can you avoid causing fires during the use of the home oxygen equipment? | 0.911 | 0.908 |
| Question 2 Can you adjust the flow rate in the toilet, in the bath, or going out? | 0.824 | 0.921 |
| Question 3 Can you use portable oxygen? | 0.840 | 0.923 |
| Question 4 Can you avoid contact with the cannula and portable oxygen? | 0.894 | 0.910 |
| Question 5 Can you deal with alarms regarding forgetting to shut the cylinder or running out of oxygen? | 0.836 | 0.919 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Annaka, H.; Nomura, T.; Moriyama, H. Cognitive Function and the Ability to Operate Long-Term Oxygen Therapy Equipment: An Exploratory Study. Int. J. Environ. Res. Public Health 2022, 19, 10708. https://doi.org/10.3390/ijerph191710708
Annaka H, Nomura T, Moriyama H. Cognitive Function and the Ability to Operate Long-Term Oxygen Therapy Equipment: An Exploratory Study. International Journal of Environmental Research and Public Health. 2022; 19(17):10708. https://doi.org/10.3390/ijerph191710708
Chicago/Turabian StyleAnnaka, Hiroki, Tomonori Nomura, and Hiroshi Moriyama. 2022. "Cognitive Function and the Ability to Operate Long-Term Oxygen Therapy Equipment: An Exploratory Study" International Journal of Environmental Research and Public Health 19, no. 17: 10708. https://doi.org/10.3390/ijerph191710708