
Assessment of Viscoelastic Parameters of Muscles in Children Aged 4–9 Months with Minor Qualitative Impairment of the Motor Pattern after Vojta Therapy Implementation


Abstract
:1. Introduction
2. Materials and Methods
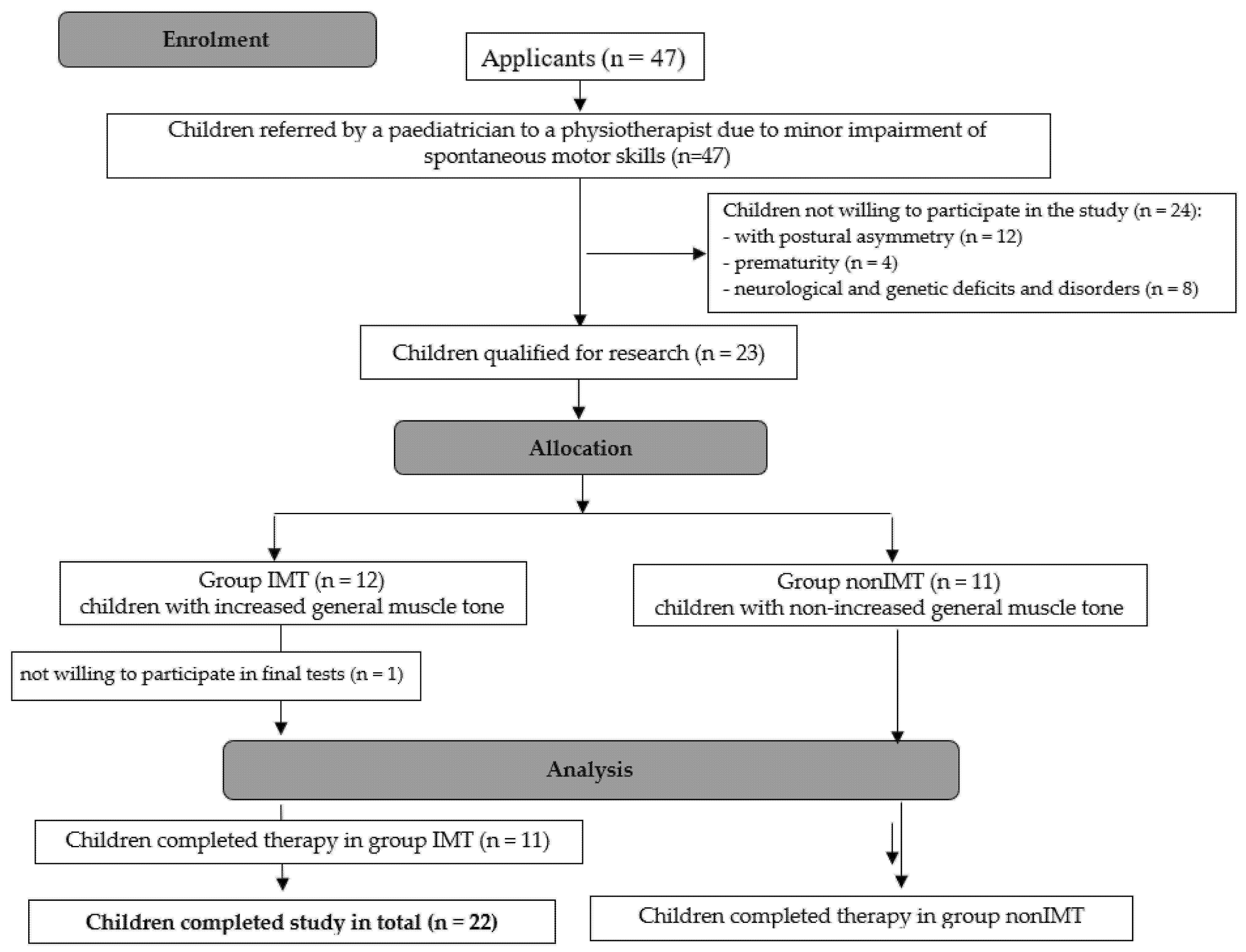
2.1. Study Group
2.2. Research Methods
2.3. Statistical Analysis
3. Results
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- van Haastert, I.C.; de Vries, L.S.; Helders, P.J.M.; Jongmans, M.J. Early gross motor development of preterm infants according to the Alberta Infant Motor Scale. J. Pediatr. 2006, 149, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Sheldrick, R.C.; Schlichting, L.E.; Berger, B.; Clyne, A.; Ni, P.; Perrin, E.C.; Vivier, P.M. Establishing New Norms for Developmental Milestones. Pediatrics 2019, 144, e20190374. [Google Scholar] [CrossRef] [PubMed]
- Todd, A.J.; Carroll, M.T.; Robinson, A.; Mitchell, E.K.L. Adverse Events Due to Chiropractic and Other Manual Therapies for Infants and Children: A Review of the Literature. J. Manip. Physiol. Ther. 2015, 38, 699–712. [Google Scholar] [CrossRef] [PubMed]
- Colson, S.D.; Meek, J.H.; Hawdon, J.M. Optimal positions for the release of primitive neonatal reflexes stimulating breastfeeding. Early Hum. Dev. 2008, 84, 441–449. [Google Scholar] [CrossRef]
- ICD-10|Brak Oczekiwanego Prawidłowego Rozwoju Fizjologicznego. Available online: https://bml.pl/narzedzia/icd10/brak-oczekiwanego-prawidlowego-rozwoju-fizjologicznego (accessed on 23 November 2021).
- Sakalidis, V.S.; McClellan, H.L.; Hepworth, A.R.; Kent, J.C.; Lai, C.T.; Hartmann, P.E.; Geddes, D.T. Oxygen Saturation and Suck-Swallow-Breathe Coordination of Term Infants during Breastfeeding and Feeding from a Teat Releasing Milk Only with Vacuum. Int. J. Pediatr. 2012, 2012, 130769. [Google Scholar] [CrossRef] [Green Version]
- Viswanathan, S.; Jadcherla, S. Feeding and Swallowing Difficulties in Neonates: Developmental Physiology and Pathophysiology. Clin. Perinatol. 2020, 47, 223–241. [Google Scholar] [CrossRef]
- Akuthota, V.; Nadler, S.F. Core strengthening11No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the author(s) or upon any organization with which the authors is/are associated. Arch. Phys. Med. Rehabil. 2004, 85, 86–92. [Google Scholar] [CrossRef]
- Shinkle, J.; Nesser, T.W.; Demchak, T.J.; McMannus, D.M. Effect of Core Strength on the Measure of Power in the Extremities. J. Strength Cond. Res. 2012, 26, 373–380. [Google Scholar] [CrossRef]
- Hodges, P.W. Is there a role for transversus abdominis in lumbo-pelvic stability? Man Ther. 1999, 4, 74–86. [Google Scholar] [CrossRef] [Green Version]
- Zazulak, B.; Cholewicki, J.; Reeves, P.N. Neuromuscular control of trunk stability: Clinical implications for sports injury prevention. JAAOS-J. Am. Acad. Orthop. Surg. 2008, 16, 497–505. [Google Scholar] [CrossRef]
- Walker, M.; Rothstein, J.; Finucane, S.; Lamb, R. Relationships Between Lumbar Lordosis, Pelvic Tilt, and Abdominal Muscle Performance. Phys. Ther. 1987, 67, 512–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeVeau, B.F.; Bernhardt, D.B. Developmental Biomechanics: Effect of Forces on the Growth, Development, and Maintenance of the Human Body. Phys. Ther. 1984, 64, 1874–1882. [Google Scholar] [CrossRef]
- Tecklin, J.S. Pediatric Physical Therapy; Lippincott Williams & Wilkins: Hagerstown, MD, USA, 2008. [Google Scholar]
- Sung, Y.-H.; Ha, S.-Y. The Vojta approach changes thicknesses of abdominal muscles and gait in children with spastic cerebral palsy: A randomized controlled trial, pilot study. Technol. Health Care 2020, 28, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Sahrmann, S.A. Does Postural Assessment Contribute to Patient Care? J. Orthop. Sports Phys. 2002, 32, 376–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, S.-Y.; Sung, Y.-H. Effects of Vojta method on trunk stability in healthy individuals. J. Exerc. Rehabil. 2016, 12, 542. [Google Scholar] [CrossRef]
- Asunta, P.; Viholainen, H.; Ahonen, T.; Rintala, P. Psychometric properties of observational tools for identifying motor difficulties—A systematic review. BMC Pediatr. 2019, 19, 322. [Google Scholar] [CrossRef] [Green Version]
- Blank, R. European Academy of Childhood Disability (EACD): Recommendations on the definition, diagnosis and intervention of developmental coordination disorder (pocket version). German-Swiss interdisciplinary clinical practice guideline S3-standard according to the Association of the Scientific Medical Societies in Germany. Pocket version. Definition, diagnosis, assessment, and intervention of developmental coordination disorder (DCD). Dev. Med. Child Neurol. 2012, 54, e1–e7. [Google Scholar]
- Weinke, I. Early Diagnosis of Cerebral Palsy: Vojta Approach. Mov. Disord. Child. 1992, 36, 86–90. [Google Scholar]
- Da Silva, A.J.; Neves, L.A.T.; da Frônio, J.S.; Ribeiro, L.C. Factors Related To Motor Developmental Delay Of Newborns. J. Hum. Growth Dev. 2014, 24, 320–327. [Google Scholar] [CrossRef] [Green Version]
- Vojta: The Basic Elements of Treatment According to Vojta—Google Scholar. Available online: https://scholar.google.com/scholar_lookup?title=The%20basic%20elements%20of%20treatment%20according%20to%20Vojta&pages=75-85&publication_year=1984&author=Vojta%2CV (accessed on 22 November 2021).
- Abbott, A.; Bartlett, D. The Relationship Between the Home Environment and Early Motor Development. Phys. Occup. Ther. Pediatr. 1999, 19, 43–57. [Google Scholar] [CrossRef]
- Cintas, H.M. Cross-Cultural Variation in Infant Motor Development. Phys. Occup. Ther. Pediatr. 1989, 8, 143635931. [Google Scholar] [CrossRef]
- Sakalidis, V.S.; Geddes, D.T. Suck-Swallow-Breathe Dynamics in Breastfed Infants. J. Hum. Lact 2016, 32, 201–211; quiz 393–395. [Google Scholar] [CrossRef] [PubMed]
- Codoni, S.; Sprigi-Gantert, I.; Indri, I.; von Jackowski, J.A. Spezielle manuelle Verfahren in der Behandlung von kraniomandibulären Dysfunktionen. MKG-Chir. 2016, 9, 167–175. [Google Scholar] [CrossRef]
- Pyda-Dulewicz, A. Wpływ pierwszej fazy odruchowego obrotu według Vojty na zakres ruchomości odcinka szyjnego u niemowląt. Ann. Acad. Med. Silesiensis 2015, 69, 111–117. [Google Scholar] [CrossRef]
- Ditroilo, M.; Hunter, A.M.; Haslam, S.; De Vito, G. The effectiveness of two novel techniques in establishing the mechanical and contractile responses of biceps femoris. Physiol. Meas. 2011, 32, 1315. [Google Scholar] [CrossRef] [Green Version]
- Mullix, J.; Warner, M.; Stokes, M. Testing muscle tone and mechanical properties of rectus femoris and biceps femoris using a novel hand held MyotonPRO device: Relative ratios and reliability. Work. Pap. Health Sci. 2012, 1, 1–8. [Google Scholar]
- Pożarowszczyk, B.; Pawlaczyk, W.; Smoter, M.; Zarzycki, A.; Mroczek, D.; Kumorek, M.; Witkowski, K.; Adam, K. Effects of karate fights on Achilles tendon stiffness measured by myotonometry. J. Hum. Kinet. 2017, 56, 93–97. [Google Scholar] [CrossRef]
- Chuang, L.; Wu, C.; Lin, K. Reliability, validity, and responsiveness of myotonometric measurement of muscle tone, elasticity, and stiffness in patients with stroke. Arch. Phys. Med. Rehabil. 2012, 93, 532–540. [Google Scholar] [CrossRef]
- Epple, C.; Maurer-Burkhard, B.; Lichti, M.-C.; Steiner, T. Vojta therapy improves postural control in very early stroke rehabilitation: A randomised controlled pilot trial. Neurol. Res. Pract. 2020, 2, 23. [Google Scholar] [CrossRef]
- Jung, M.W.; Landenberger, M.; Jung, T.; Lindenthal, T.; Philippi, H. Vojta therapy and neurodevelopmental treatment in children with infantile postural asymmetry: A randomised controlled trial. J. Phys. Ther. Sci. 2017, 29, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Barassi, G.; Giannuzzo, G.; De Santis, R.; Dragonetti, A. Adaptive Neuromodulation in the Treatment of Spasticity. J. Adv. Health Care 2020, 2. Available online: https://jahc.eu/volume-2/jahc2010-003/ (accessed on 9 October 2020).
- Novak, I.; Mcintyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.-A.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.K. Functional movement assessment with the Test of Infant Motor Performance. J Perinatol 2021, 41, 2385–2394. [Google Scholar] [CrossRef]
- Goo, M.; Tucker, K.; Johnston, L.M. Muscle tone assessments for children aged 0 to 12 years: A systematic review. Dev. Med. Child Neurol. 2018, 60, 660–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisilewicz, A.; Janusiak, M.; Szafraniec, R.; Smoter, M.; Ciszek, B.; Madeleine, P.; Fernández-De-Las-Peñas, C.; Kawczyński, A. Changes in Muscle Stiffness of the Trapezius Muscle After Application of Ischemic Compression into Myofascial Trigger Points in Professional Basketball Players. J. Hum. Kinet. 2018, 64, 35–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordez, A.; Guével, A.; Casari, P.; Catheline, S.; Cornu, C. Assessment of muscle hardness changes induced by a submaximal fatiguing isometric contraction. J. Electromyogr. Kinesiol. 2009, 19, 484–491. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| IMT Group (n = 11) | nonIMT Group (n = 11) | |||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| sex (F/M) | 3/8 | 5/6 | ||
| age [months] | 6.95 | 3.14 | 7.05 | 3.43 |
| Apgar score [points] | 9.27 | 1.10 | 9.73 | 0.65 |
| IMT Group | nonIMT Group | |||||
|---|---|---|---|---|---|---|
| Mean | Median | SD | Mean | Median | SD | |
| Frequency 1 [Hz] | 21.04 | 21.90 | 4.27 | 22.70 | 22.80 | 2.55 |
| Frequency 2 [Hz] | 19.98 | 20.20 | 2.59 | 22.55 | 22.90 | 2.06 |
| Frequency 3 [Hz] | 21.96 | 22.40 | 1.94 | 21.79 | 22.50 | 2.42 |
| Elasticity 1 | 0.99 | 0.94 | 0.23 | 1.09 | 1.00 | 0.24 |
| Elasticity 2 | 1.03 | 1.02 | 0.18 | 0.97 | 1.04 | 0.18 |
| Elasticity 3 | 0.99 | 0.92 | 0.12 | 0.98 | 1.02 | 0.24 |
| Stiffness 1 [N/m] | 582.70 | 556.00 | 135.61 | 578.36 | 555.00 | 87.07 |
| Stiffness 2 [N/m] | 460.82 | 500.00 | 114.96 | 582.09 | 608.00 | 90.50 |
| Stiffness 3 [N/m] | 586.89 | 592.00 | 88.86 | 605.27 | 546.00 | 167.07 |
| Relaxation 1 [ms] | 8.84 | 9.05 | 1.86 | 9.14 | 9.10 | 1.56 |
| Relaxation 2 [ms] | 10.95 | 10.30 | 1.96 | 8.98 | 8.90 | 1.52 |
| Relaxation 3 [ms] | 8.90 | 9.00 | 1.46 | 9.14 | 9.80 | 2.16 |
| Creep 1 | 0.60 | 0.60 | 0.15 | 0.59 | 0.58 | 0.09 |
| Creep 2 | 0.69 | 0.66 | 0.11 | 0.57 | 0.56 | 0.09 |
| Creep 3 | 0.58 | 0.58 | 0.09 | 0.61 | 0.65 | 0.14 |
| IMT Group vs. nonIMT Group | Measurement | ||
|---|---|---|---|
| 1 | 2 | 3 | |
| Frequency | 0.2810 | 0.0206 * | 0.8707 |
| Stiffness | 0.9307 | 0.0124 * | 0.7702 |
| Elasticity | 0.3377 | 0.4538 | 0.9106 |
| Relaxation | 0.6956 | 0.0182 * | 0.7829 |
| Creep | 0.7461 | 0.0123 * | 0.5709 |
| IMT Group | nonIMT Group | |||||||
|---|---|---|---|---|---|---|---|---|
| Measurement: | Measurement: | |||||||
| p ANOVA | 1 vs. 2 | 1 vs. 3 | 2 vs. 3 | p ANOVA | 1 vs. 2 | 1 vs. 3 | 2 vs. 3 | |
| Frequency | 0.0122 * | 0.0197 * | 0.8922 | 0.0472 * | 0.2087 | N | N | N |
| Stiffness | 0.0216 * | 0.0356 * | 0.9429 | 0.0657 | 0.9787 | N | N | N |
| Elasticity | 0.4665 | N | N | N | 0.5441 | N | N | N |
| Relaxation | 0.0088 * | 0.0172 * | 0.9596 | 0.0292 * | 0.4704 | N | N | N |
| Creep | 0.1166 | N | N | N | 0.1118 | N | N | N |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ptak, A.; Dębiec-Bąk, A.; Stefańska, M. Assessment of Viscoelastic Parameters of Muscles in Children Aged 4–9 Months with Minor Qualitative Impairment of the Motor Pattern after Vojta Therapy Implementation. Int. J. Environ. Res. Public Health 2022, 19, 10448. https://doi.org/10.3390/ijerph191610448
Ptak A, Dębiec-Bąk A, Stefańska M. Assessment of Viscoelastic Parameters of Muscles in Children Aged 4–9 Months with Minor Qualitative Impairment of the Motor Pattern after Vojta Therapy Implementation. International Journal of Environmental Research and Public Health. 2022; 19(16):10448. https://doi.org/10.3390/ijerph191610448
Chicago/Turabian StylePtak, Agnieszka, Agnieszka Dębiec-Bąk, and Małgorzata Stefańska. 2022. "Assessment of Viscoelastic Parameters of Muscles in Children Aged 4–9 Months with Minor Qualitative Impairment of the Motor Pattern after Vojta Therapy Implementation" International Journal of Environmental Research and Public Health 19, no. 16: 10448. https://doi.org/10.3390/ijerph191610448