
Obesity, Burden of Ischemic Heart Diseases and Their Ecological Association: The Case of Uzbekistan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations, World Population Prospects 2019, Department of Economic and Social Affiars Population Dynamics. Available online: https://population.un.org/wpp/ (accessed on 21 February 2022).
- Ahmedov, M.; Azimov, R.; Mutalova, Z.; Huseynov, S.; Tsoyi, E.; Rechel, B. Uzbekistan: Health System Review. Health Syst. Transit. 2014, 16, 1–137. [Google Scholar] [PubMed]
- Ross, R. Atherosclerosis as an inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Álvarez-Álvarez, M.M.; Zanetti, D.; Carreras-Torres, R.; Moral, P.; Athanasiadis, G. A survey of sub-Saharan gene flow into the Mediterranean at risk loci for coronary artery disease. Eur. J. Hum. Genet. 2017, 25, 472–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lui, M.; Safiri, S.; Mereke, A.; Davletov, K.; Mebonia, N.; Myrkassymova, A.; Aripov, T.; Mirrakhimov, E.; Aghayan, S.A.; Gamkrelidze, A.; et al. Burden of Ischemic Heart Disease in Central Asian Countries, 1990–2017. IJC Hear. Vasc. 2021, 33, 100726. [Google Scholar] [CrossRef]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Associacion of All-Cause Mortality with overweight and Obesity Using Standard Body Mass Index Categories: A Systematic Reviewed and Meta-Analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.W.F.; D’Agostino, R.B.; Sullivan, L.; Parise, H.; Kannel, W.B. Overweight and Obesity as Determinants of Cardiovascular Risk. Arch. Intern. Med. 2002, 162, 1867–1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellulu, M.; Abed, Y.; Rahmat, A.; Ranneh, Y.; Ali, F. Epidemiology of obesity in developing countries: Challenges and prevention. Glob. Epidemic Obes. 2014, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- McGill Jr, H.C.; McMahan, C.A.; Herderick, E.E.; Zieske, A.W.; Malcom, G.T.; Tracy, R.E.; Strong, J.P. Obesity Accelerates the Progression of Coronary Atherosclerosis in Young Men. Circulation 2002, 105, 2712–2718. [Google Scholar] [CrossRef] [PubMed]
- NCD-risC. Risk Factor Collabration. Data Visualisiations. Explore Country Risk Factor Data using Dynamic Graphics. Available online: https://www.ncdrisc.org/data-visualisations.html (accessed on 14 September 2021).
- World Health Organisation. Obesity and Overweight—Key Facts. Available online: http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 26 November 2018).
- WHO MONICA Project Principal Investigators. The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): A major international collaboration. J. Clin. Epidemiol. 1988, 41, 105–114. [Google Scholar] [CrossRef]
- IHME. GHDx. Global Health Data Exchange. Discover the World’s Heath Data. GBD Result Tool. Available online: https://ghdx.healthdata.org/gbd-results-tool (accessed on 24 September 2021).
- Fox, J. Applied Regression Analysis and Generalized Linear Models, 3rd ed.; Sage Publications Inc.: New Delhi, India, 2015; pp. 356–359. [Google Scholar]
- Schisterman, E.F.; Cole, S.R.; Platt, R.W. Overadjustment Bias and Unneccessary Adjustment in Epidemilogic Studies. Epidemilogy 2009, 20, 488–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, Y.; Hajifathalian, K.; Ezzati, M.; Woodward, M.; Rimm, E.B.; Danaei, G.; D’Este, C. Metabolic mediators of the effects of body-mass index, overweight, and obesity on coronary heart disease and stroke: A pooled analysis of 97 prospective cohorts with 1·8 million participants. Lancet 2014, 383, 970–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Copeland, W.K.; Vedanthan, R.; Grant, E.; Lee, J.E.; Gu, D.; Gupta, P.C.; Ramadas, K.; Inoue, M.; Tsugane, S.; et al. Association between body mass index and cardiovascular disease mortality in east Asians and south Asians: Pooled analysis of prospective data from the Asia Cohort Consortium. BMJ 2013, 347, f5446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, J.W.; Konz, E.C. Obesity and Disease Management: Effects of Weight Loss on Comorbid Conditions. Obes. Res. 2001, 9 (Suppl. 4), 326S–334S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engstrom, G.; Berglund, G.; Goransson, M.; Hansen, O.; Hedblad, B.; Merlo, J.; Tyden, P.; Janzon, L. Distribution and determinants of ischaemic heart disease in an urban population. A study from the myocardial infarction register in Malmo, Sweden. J. Intern. Med. 2000, 247, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Akil, L.; Ahmad, H.A. Relationships between Obesity and Cardiovascular Diseases in Four Southern States and Colorado. J. Heal. Care Poor Underserved. 2011, 22, 61–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietiläinen, K.H.; Kaprio, J.; Borg, P.; Plasqui, G.; Yki-Järvinen, H.; Kujala, U.; Rose, R.J.; Westerterp, K.R.; Rissanen, A. Physical Inactivity and Obesity: A Vicious Circle. Obesity 2008, 16, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Overcoming Barries to Physical Activity. Available online: https://www.cdc.gov/physicalactivity/basics/adding-pa/barriers.html (accessed on 12 August 2022).
- UK Active. Turning the Tide of Activity. Available online: https://www.ukactive.com/wp-content/uploads/2018/09/ukactive_Turning_the_tide_of_inactivity.pdf (accessed on 12 August 2022).
- Our World in Data. Daily per Capita Fat Supply, 1961 to 2013. Available online: https://ourworldindata.org/search?q=Fat+supply+by+region%2C+daily-per-capita-fat+supply (accessed on 14 November 2021).
- Aronne, L.J.; Nelinson, D.S.; Lillo, J.L. Obesity As Disease State: A New Paradigm for Diagnosis and Treatment. Clin. Cornerstone 2009, 9, 9–29. [Google Scholar] [CrossRef]
- IPHR International Partnership for Human Rights. Reforming Healthcare in Uzbekistan: What Role for the International Community? Available online: https://www.iphronline.org/uzbekistan_healthcare.html?msclkid=7ffa16d4b08d11ecb44218b3c325fff8 (accessed on 25 January 2022).
- Resolution of the Cabinet of Ministers of the Republic of Uzbekistan. On the State Program “Year of Health” No. 3–4, Article 25. Available online: http://dd.gov.uz/ru/pages/2005 (accessed on 25 January 2022).
- Resolution of the Cabinet of Ministers of the Republic of Uzbekistan. On Effective use of Borrowed Funds and Measures to Effectively Use the International Bank for the Development of the Health-1 Project and Development of the Health-2 Project. No. 256. 6 June 2003. Tashkent. Available online: http://old.lex.uz/docs/482154 (accessed on 26 January 2022).
- Morgenstern, H. Uses of ecologic analysis in epidemiologic research. Am. J. Public Health 1982, 72, 1336–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engin, A. The Definition and Prevalence of Obesity and Metabolic Syndrome. Obes. Lipotoxicity 2017, 960, 1–17. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
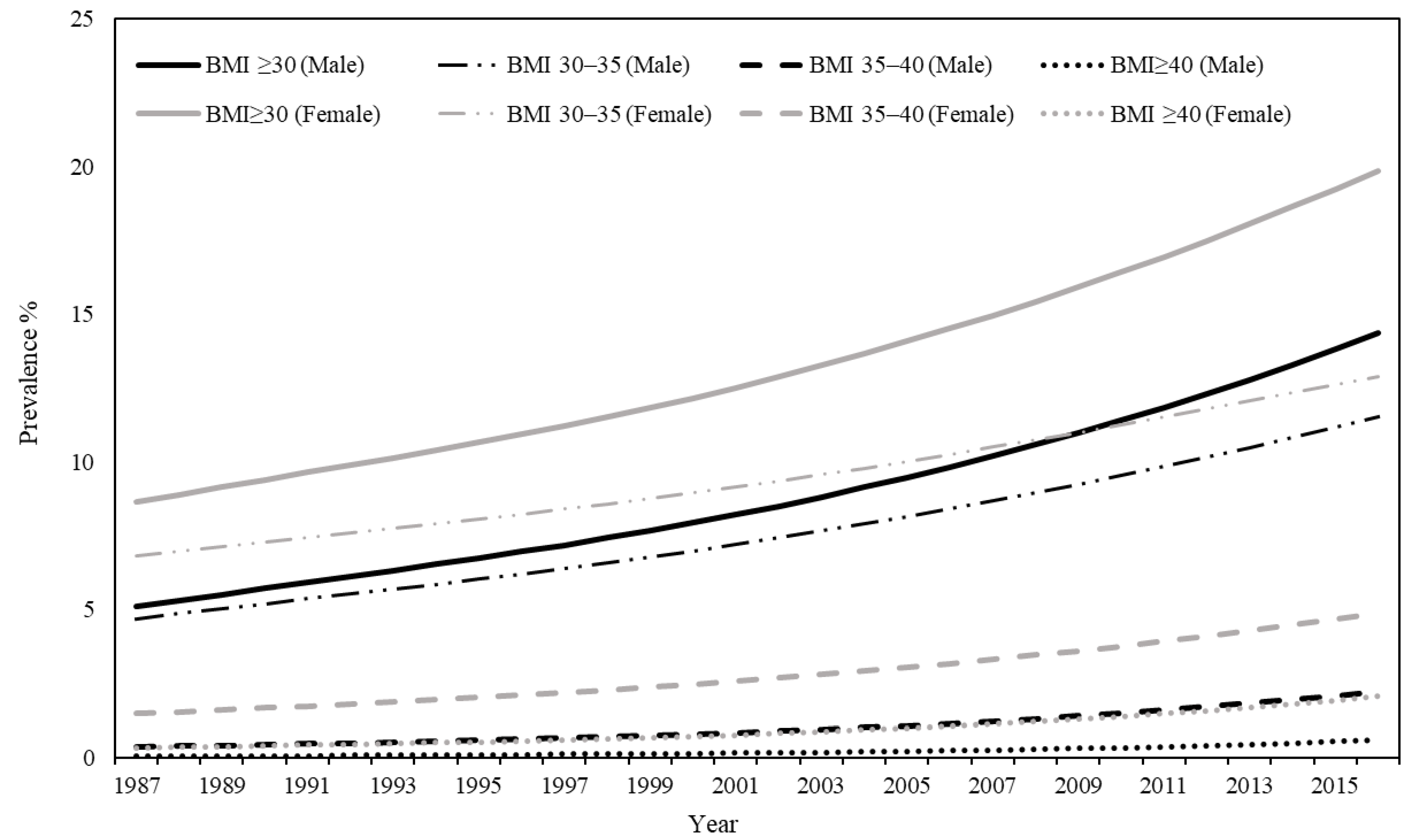
| Class of Obesity | Prevalence 1 | Average Annual Percentage Change (%) 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| 1987 | 1997 | 2007 | 2016 | 1987–1997 | 1997–2007 | 2007–2016 | 1987–2016 | |
| Men | ||||||||
| Obesity (BMI ≥ 30) | 5.13 | 7.20 | 10.21 | 14.37 | 3.39 | 3.46 | 3.89 | 3.57 |
| Class I (BMI 30.0–34.9) | 4.71 | 6.40 | 8.69 | 11.52 | 3.07 | 3.05 | 3.22 | 3.11 |
| Class II (BMI 35.0–35.9) | 0.37 | 0.68 | 1.24 | 2.24 | 6.07 | 6.09 | 6.88 | 6.30 |
| Class III (BMI ≥ 40) | 0.05 | 0.12 | 0.27 | 0.60 | 8.61 | 8.30 | 9.26 | 8.60 |
| Women | ||||||||
| Obesity (BMI ≥ 30) | 8.67 | 11.23 | 14.97 | 19.86 | 2.56 | 2.91 | 3.23 | 2.89 |
| Class I (BMI 30.0–34.9) | 6.85 | 8.41 | 10.51 | 12.91 | 2.03 | 2.25 | 2.35 | 2.21 |
| Class II (BMI 35.0–35.9) | 1.48 | 2.20 | 3.32 | 4.88 | 3.97 | 4.18 | 4.40 | 4.17 |
| Class III (BMI ≥ 40) | 0.34 | 0.61 | 1.14 | 2.08 | 5.99 | 6.41 | 6.96 | 6.42 |
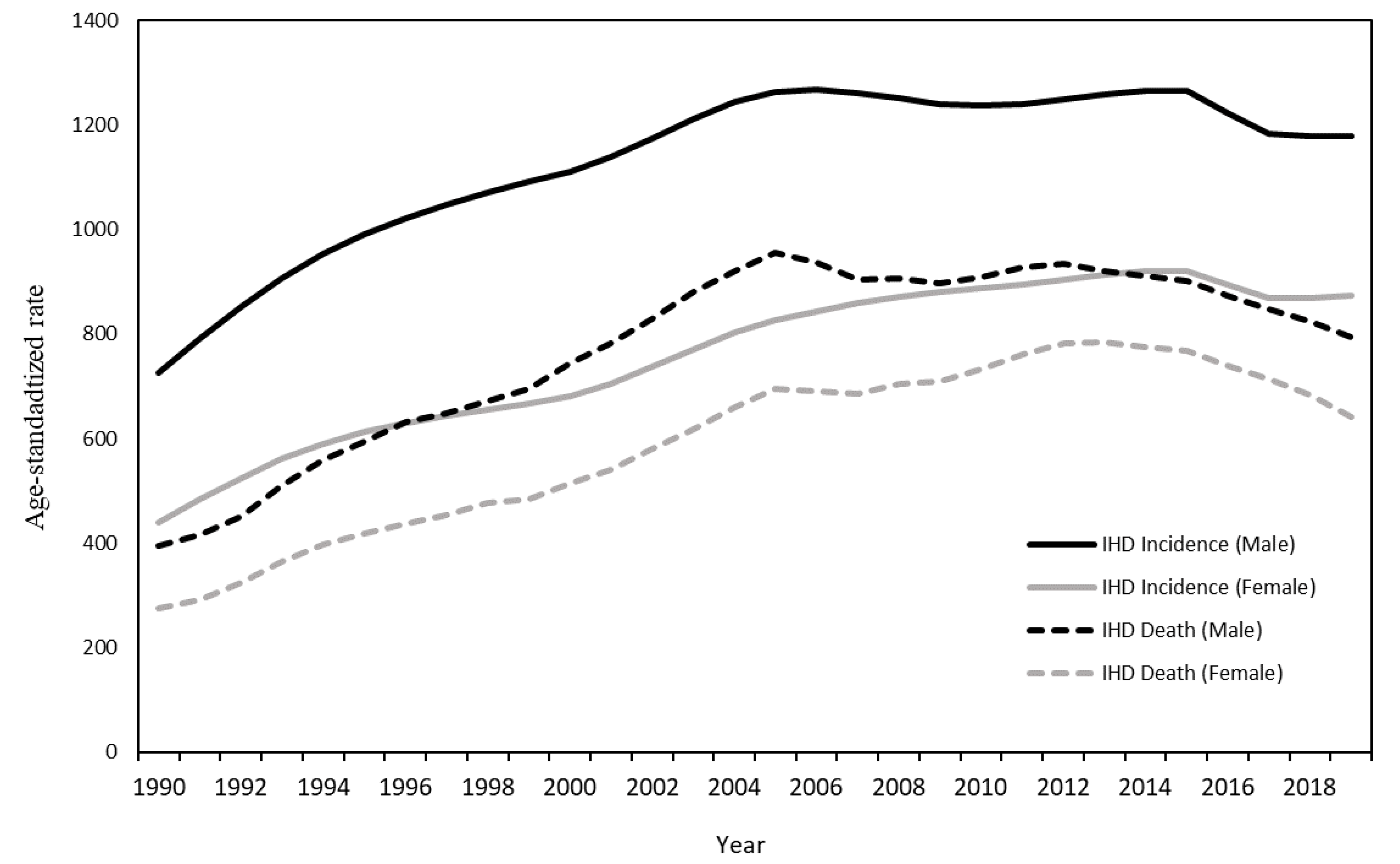
| Number | % of All Cause 1 | ASR | Average AnnualPercentage Change (%) 2 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1990 | 2000 | 2010 | 2019 | 1990 | 2000 | 2010 | 2019 | 1990 | 2000 | 2010 | 2019 | 1990–2000 | 2000–2010 | 2010–2019 | 1990–2019 | |
| Incidence | ||||||||||||||||
| Male | 32,152 | 49,648 | 66,649 | 84,349 | 0.08 | 0.10 | 0.12 | 0.13 | 724.6 | 1110.5 | 1236.0 | 1178.4 | 4.42 | 1.20 | −0.76 | 1.39 |
| Female | 27,655 | 42,449 | 49,423 | 59,386 | 0.06 | 0.08 | 0.08 | 0.08 | 440.4 | 681.9 | 887.7 | 873.9 | 4.28 | 2.58 | −0.48 * | 2.24 |
| Death | ||||||||||||||||
| Male | 15,488 | 27,603 | 37,405 | 40,615 | 22.2 | 28.6 | 36.0 | 36.1 | 394.7 | 744.3 | 909.5 | 792.7 | 7.00 | 1.93 | −1.83 | 2.41 |
| Female | 16,611 | 29,844 | 34,749 | 34,886 | 27.2 | 34.3 | 39.5 | 38.4 | 274.8 | 514.3 | 733.5 | 640.8 | 6.75 | 3.86 | −1.44 | 3.25 |
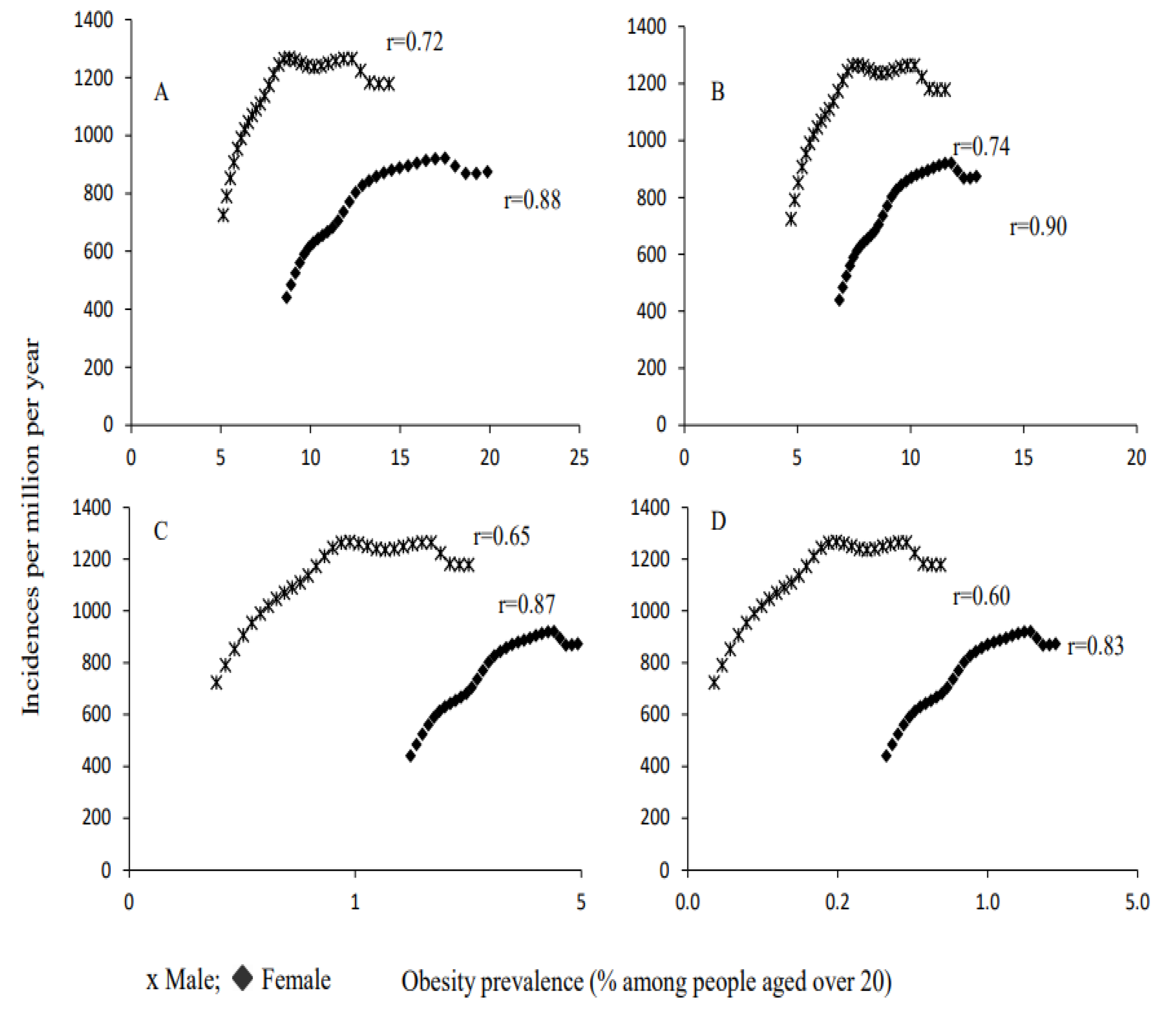
| A | ||||||||
|---|---|---|---|---|---|---|---|---|
| Class of Obesity | Regression Parameters | Adjusted R2 | p Value | |||||
| B0 | (95% CI) | p Value | B1 | (95% CI) | p Value | |||
| Male | ||||||||
| Obesity (BMI ≥ 30) | 772.9 | (632.1–913.6) | <0.0001 | 40.2 | (24.9–55.3) | <0.0001 | 0.51 | <0.0001 |
| Class I (BMI 30.0–34.9) | 704.3 | (549.6–859.0) | <0.0001 | 55.8 | (36.1–75.4) | <0.0001 | 0.55 | <0.0001 |
| Class II (BMI 35.0–35.9) | 942 | (845.9–1037.8) | <0.0001 | 182.3 | (99.7–264.9) | <0.0001 | 0.42 | 0.0001 |
| Class III (BMI ≥ 40) | 996.7 | (914.6–1079.1) | <0.0001 | 587.3 | (287.4–887.3) | <0.0001 | 0.36 | 0.0004 |
| Female | ||||||||
| Obesity (BMI ≥ 30) | 248.7 | (139.6–357.9) | <0.0001 | 38.3 | (30.3–46.3) | <0.0001 | 0.78 | <0.0001 |
| Class I (BMI 30.0–34.9) | 76.9 | (−53.0–206.9) | 0.236 | 71.6 | (58.2–85.1) | <0.0001 | 0.81 | <0.0001 |
| Class II (BMI 35.0–35.9) | 403 | (320.5–485.5) | <0.0001 | 125.0 | (97.6–152.5) | <0.0001 | 0.76 | <0.0001 |
| Class III (BMI ≥ 40) | 535.5 | (468.8–602.2) | <0.0001 | 235.3 | (172.9–297.6) | <0.0001 | 0.68 | <0.0001 |
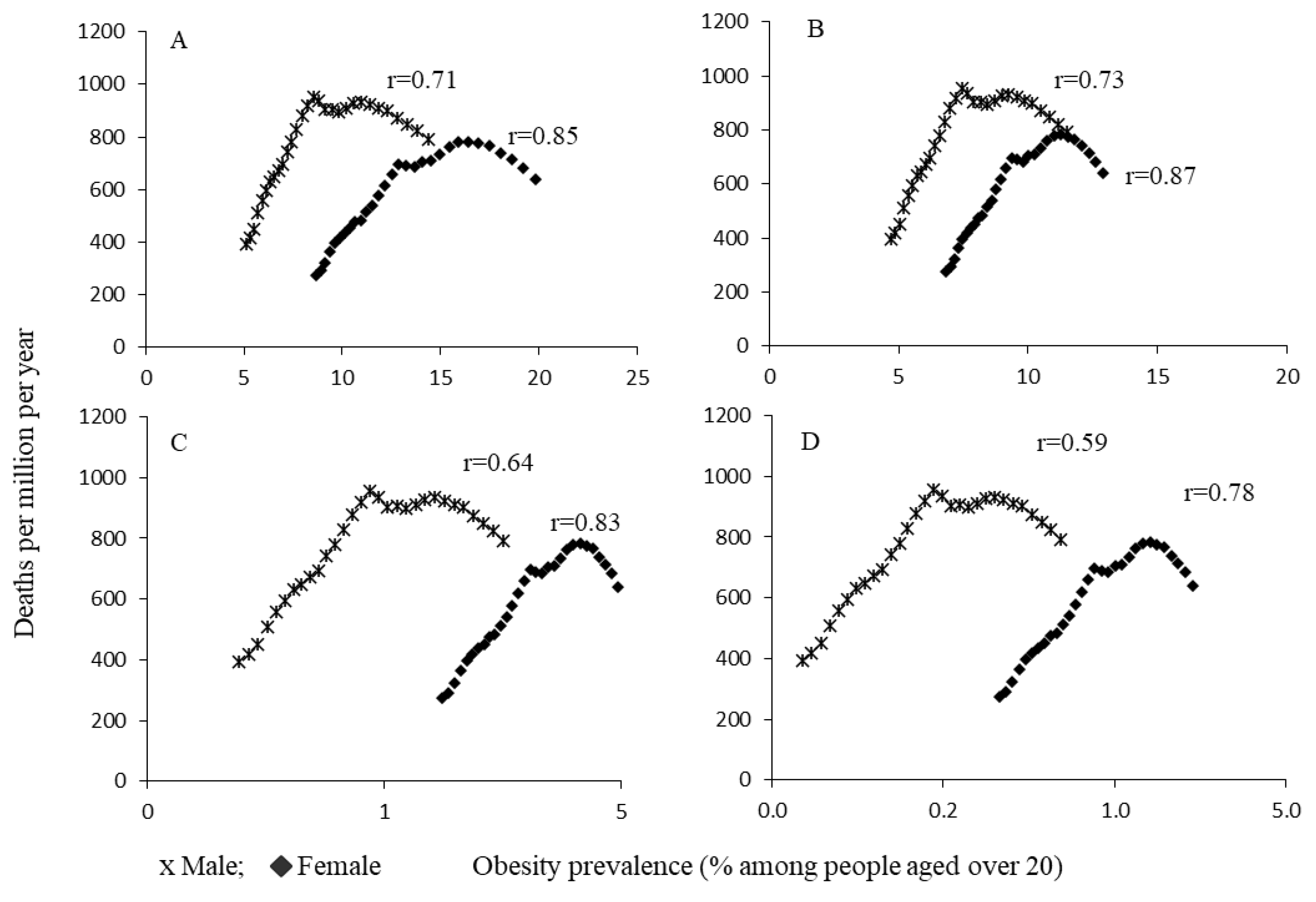
| B | ||||||||
| Class of Obesity | Regression parameters | Adjusted R2 | p value | |||||
| B0 | (95% CI) | p value | B1 | (95% CI) | p value | |||
| Male | ||||||||
| Obesity (BMI ≥ 30) | 376.6 | (217.8–535.4) | <0.0001 | 44.6 | (27.4–61.7) | <0.0001 | 0.50 | <0.0001 |
| Class I (BMI 30.0–34.9) | 299.9 | (125.4–474.3) | 0.001 | 61.9 | (39.8–84.1) | <0.0001 | 0.54 | <0.0001 |
| Class II (BMI 35.0–35.9) | 564.8 | (456.6–672.9) | <0.0001 | 201.6 | (108.5–294.7) | <0.0001 | 0.41 | <0.0001 |
| Class III (BMI ≥ 40) | 626.1 | (533.3–718.9) | <0.0001 | 647.2 | (308.7–985.6) | <0.0001 | 0.35 | 0.0005 |
| Female | ||||||||
| Obesity (BMI ≥ 30) | 51.2 | (−84.7–187.1) | 0.447 | 40.5 | (30.6–50.5) | <0.0001 | 0.71 | <0.0001 |
| Class I (BMI 30.0–34.9) | −133.5 | (−297.4–30.5) | 0.107 | 76.1 | (59.1–93.0) | <0.0001 | 0.75 | <0.0001 |
| Class II (BMI 35.0–35.9) | 215.2 | (113.2–317.3) | <0.0001 | 132.1 | (98.1–166.0) | <0.0001 | 0.69 | <0.0001 |
| Class III (BMI ≥ 40) | 357.2 | (276.2–438.2) | <0.0001 | 246.2 | (170.5–321.9) | <0.0001 | 0.61 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Usmanov, M.M.; Chimed-Ochir, O.; Batkhorol, B.; Yumiya, Y.; Hujamberdieva, L.M.; Kubo, T. Obesity, Burden of Ischemic Heart Diseases and Their Ecological Association: The Case of Uzbekistan. Int. J. Environ. Res. Public Health 2022, 19, 10447. https://doi.org/10.3390/ijerph191610447
Usmanov MM, Chimed-Ochir O, Batkhorol B, Yumiya Y, Hujamberdieva LM, Kubo T. Obesity, Burden of Ischemic Heart Diseases and Their Ecological Association: The Case of Uzbekistan. International Journal of Environmental Research and Public Health. 2022; 19(16):10447. https://doi.org/10.3390/ijerph191610447
Chicago/Turabian StyleUsmanov, Murodkhon Marufkhonovich, Odgerel Chimed-Ochir, Bilegt Batkhorol, Yui Yumiya, Lola Mamazairovna Hujamberdieva, and Tatsuhiko Kubo. 2022. "Obesity, Burden of Ischemic Heart Diseases and Their Ecological Association: The Case of Uzbekistan" International Journal of Environmental Research and Public Health 19, no. 16: 10447. https://doi.org/10.3390/ijerph191610447