
Fatty Liver Change in Korean Adults in a Systematic Social Distancing System Amid the COVID-19 Pandemic: A Multicenter Analysis

 , , , , , , , ,
, , , , , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
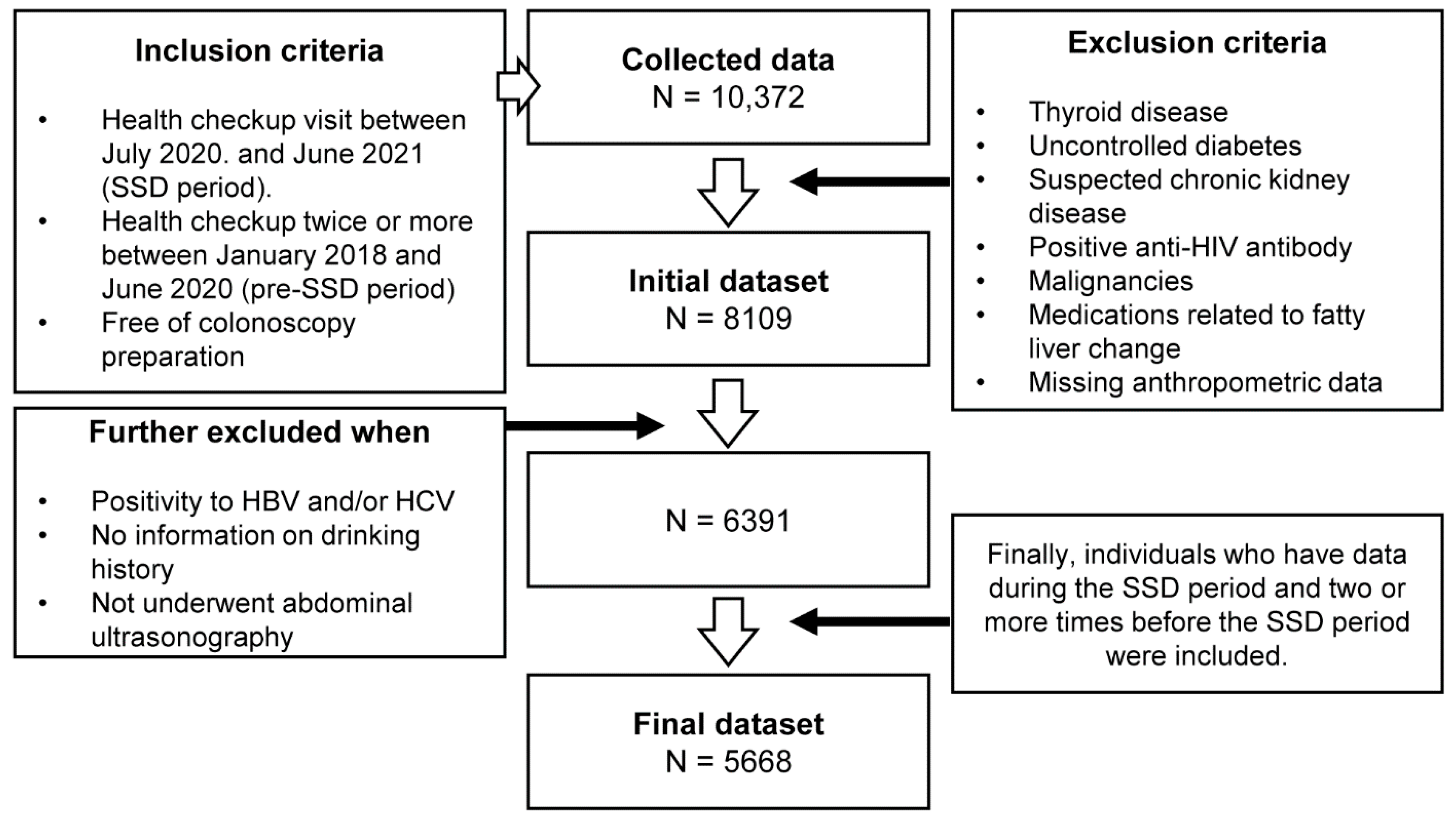
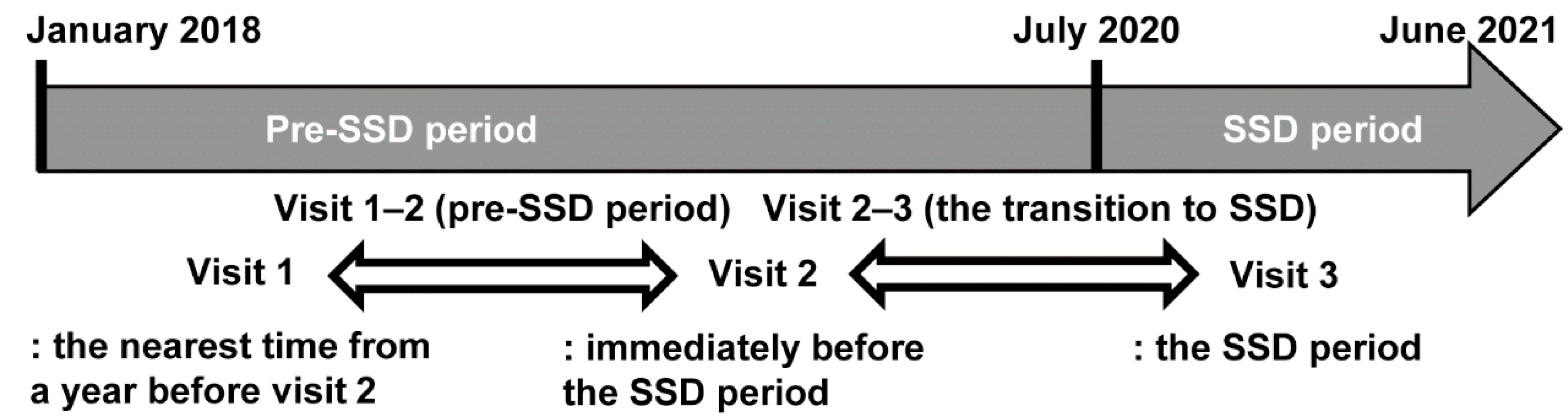
2.1. Study Design and Subjects
2.2. Primary and Secondary Endpoints
2.3. Measurements and Personal Medical History
2.4. Blood Sampling
2.5. Measurements of Fatty Liver
2.6. Normality in Liver Enzymes and FIB-4
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Subjects
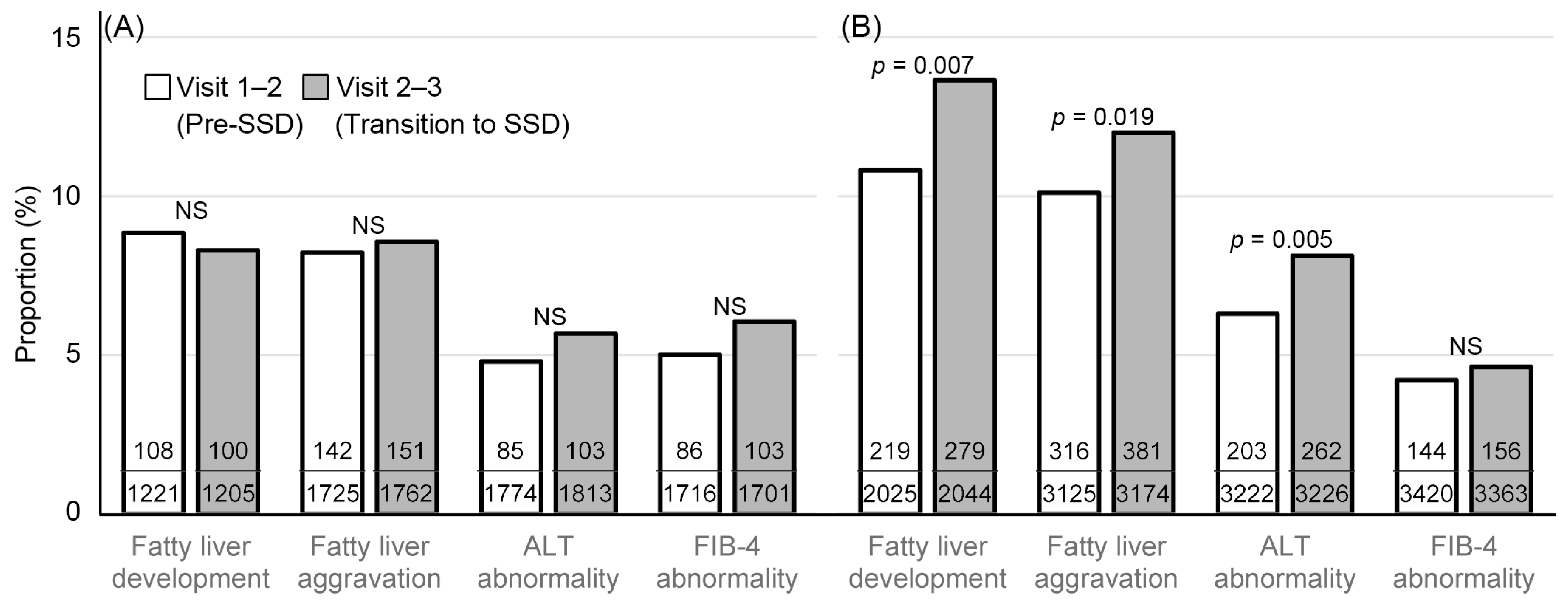
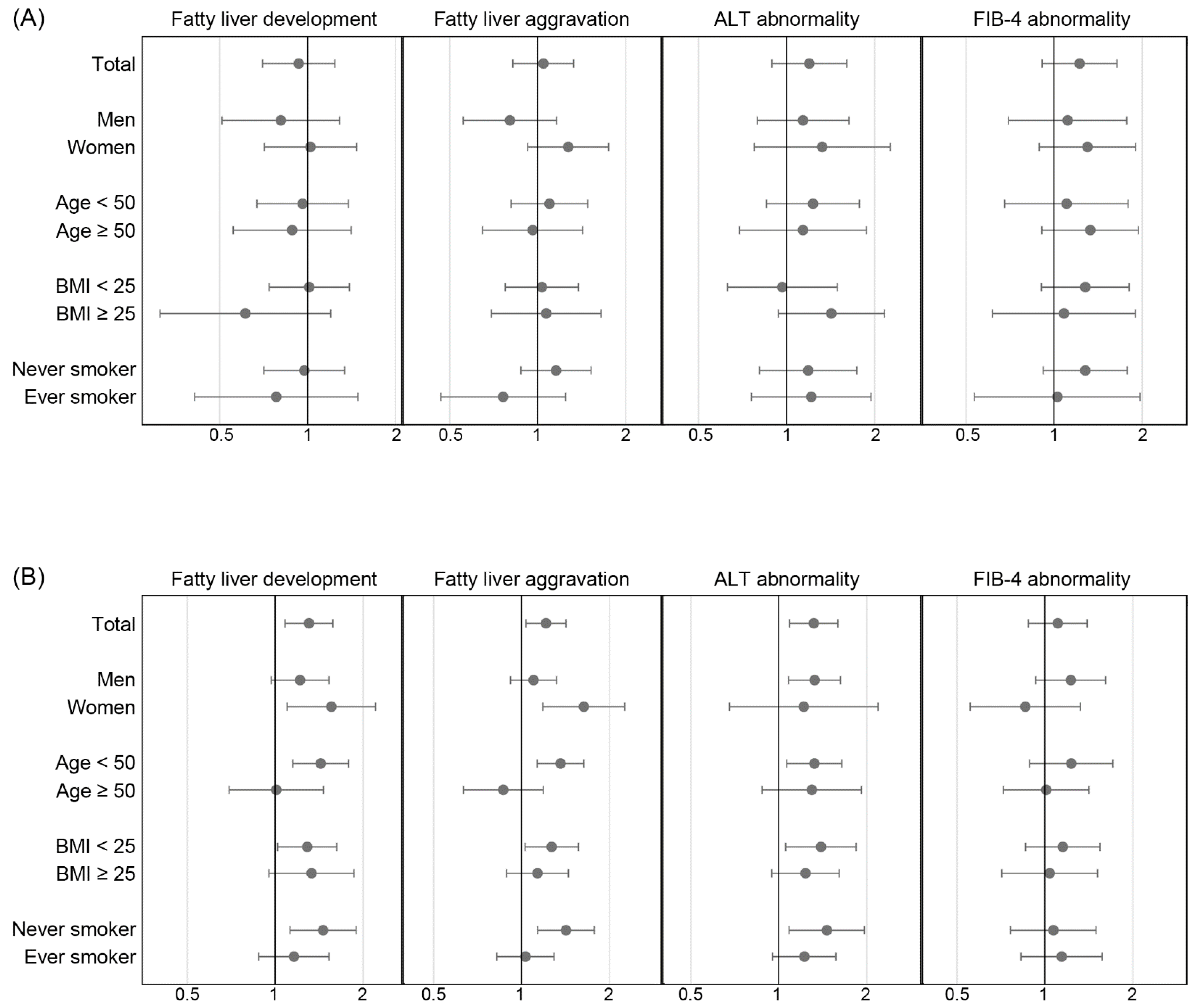
3.2. Changes in Liver Parameters over the Transition to the SSD Period
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mofijur, M.; Fattah, I.M.R.; Alam, M.A.; Islam, A.; Ong, H.C.; Rahman, S.M.A.; Najafi, G.; Ahmed, S.F.; Uddin, M.A.; Mahlia, T.M.I. Impact of COVID-19 on the social, economic, environmental and energy domains: Lessons learnt from a global pandemic. Sustain. Prod. Consum. 2021, 26, 343–359. [Google Scholar] [CrossRef] [PubMed]
- Witteveen, D.; Velthorst, E. Economic hardship and mental health complaints during COVID-19. Proc. Natl. Acad Sci. USA 2020, 117, 27277–27284. [Google Scholar] [CrossRef] [PubMed]
- Algahtani, F.D.; Hassan, S.U.; Alsaif, B.; Zrieq, R. Assessment of the Quality of Life during COVID-19 Pandemic: A Cross-Sectional Survey from the Kingdom of Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 847. [Google Scholar] [CrossRef] [PubMed]
- Karakose, T.; Ozdemir, T.Y.; Papadakis, S.; Yirci, R.; Ozkayran, S.E.; Polat, H. Investigating the Relationships between COVID-19 Quality of Life, Loneliness, Happiness, and Internet Addiction among K-12 Teachers and School Administrators—A Structural Equation Modeling Approach. Int. J. Environ. Res. Public Health 2022, 19, 1052. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Kim, R.G.; Medina, S.P.; Magee, C.; Khalili, M. Fatty Liver and the Coronavirus Disease 2019 Pandemic: Health Behaviors, Social Factors, and Telemedicine Satisfaction in Vulnerable Populations. Hepatol. Commun. 2022, 6, 1045–1055. [Google Scholar] [CrossRef]
- Clemmensen, C.; Petersen, M.B.; Sorensen, T.I.A. Will the COVID-19 pandemic worsen the obesity epidemic? Nat. Rev. Endocrinol. 2020, 16, 469–470. [Google Scholar] [CrossRef]
- Kim, E.S.; Kwon, Y.; Choe, Y.H.; Kim, M.J. Author Correction: COVID-19-related school closing aggravate obesity and glucose intolerance in pediatric patients with obesity. Sci. Rep. 2021, 11, 14284. [Google Scholar] [CrossRef]
- Woolford, S.J.; Sidell, M.; Li, X.; Else, V.; Young, D.R.; Resnicow, K.; Koebnick, C. Changes in Body Mass Index Among Children and Adolescents During the COVID-19 Pandemic. JAMA 2021, 326, 1434–1436. [Google Scholar] [CrossRef]
- Nassir, F.; Rector, R.S.; Hammoud, G.M.; Ibdah, J.A. Pathogenesis and Prevention of Hepatic Steatosis. Gastroenterol. Hepatol. 2015, 11, 167–175. [Google Scholar]
- Stickel, F.; Datz, C.; Hampe, J.; Bataller, R. Pathophysiology and Management of Alcoholic Liver Disease: Update 2016. Gut Liver 2017, 11, 173–188. [Google Scholar] [CrossRef]
- Kamper-Jorgensen, M.; Gronbaek, M.; Tolstrup, J.; Becker, U. Alcohol and cirrhosis: Dose-response or threshold effect? J. Hepatol. 2004, 41, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Mazzolini, G.; Sowa, J.P.; Atorrasagasti, C.; Kucukoglu, O.; Syn, W.K.; Canbay, A. Significance of Simple Steatosis: An Update on the Clinical and Molecular Evidence. Cells 2020, 9, 2458. [Google Scholar] [CrossRef] [PubMed]
- Rector, R.S.; Thyfault, J.P. Does physical inactivity cause nonalcoholic fatty liver disease? J. Appl. Physiol. 2011, 111, 1828–1835. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Lee, H.W.; Yoo, J.J.; Cho, Y.; Kim, S.U.; Lee, T.H.; Jang, B.K.; Kim, S.G.; Ahn, S.B.; Kim, H.; et al. KASL clinical practice guidelines: Management of nonalcoholic fatty liver disease. Clin. Mol. Hepatol. 2021, 27, 363–401. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.A. Social Distancing and Public Health Guidelines at Workplaces in Korea: Responses to Coronavirus Disease-19. Saf. Health Work 2020, 11, 275–283. [Google Scholar] [CrossRef]
- Park, I.N.; Yum, H.K. Stepwise Strategy of Social Distancing in Korea. J. Korean Med. Sci. 2020, 35, e264. [Google Scholar] [CrossRef]
- Meyer, J.; McDowell, C.; Lansing, J.; Brower, C.; Smith, L.; Tully, M.; Herring, M. Changes in Physical Activity and Sedentary Behavior in Response to COVID-19 and Their Associations with Mental Health in 3052 US Adults. Int. J. Environ. Res. Public Health 2020, 17, 6469. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Skotnicka, M.; Karwowska, K.; Klobukowski, F.; Wasilewska, E.; Malgorzewicz, S. Dietary Habits before and during the COVID-19 Epidemic in Selected European Countries. Nutrients 2021, 13, 1690. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, G.; Camussi, E.; Piccinelli, C.; Senore, C.; Armaroli, P.; Ortale, A.; Garena, F.; Giordano, L. Did social isolation during the SARS-CoV-2 epidemic have an impact on the lifestyles of citizens? Epidemiol. Prev. 2020, 44, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Grossman, E.R.; Benjamin-Neelon, S.E.; Sonnenschein, S. Alcohol Consumption during the COVID-19 Pandemic: A Cross-Sectional Survey of US Adults. Int. J. Environ. Res. Public Health 2020, 17, 9189. [Google Scholar] [CrossRef] [PubMed]
- Pollard, M.S.; Tucker, J.S.; Green, H.D., Jr. Changes in Adult Alcohol Use and Consequences During the COVID-19 Pandemic in the US. JAMA Netw. Open 2020, 3, e2022942. [Google Scholar] [CrossRef]
- Jurecka, A.; Skucinska, P.; Gadek, A. Impact of the SARS-CoV-2 Coronavirus Pandemic on Physical Activity, Mental Health and Quality of Life in Professional Athletes-A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 9423. [Google Scholar] [CrossRef]
- Karatas, S.; Yesim, T.; Beysel, S. Impact of lockdown COVID-19 on metabolic control in type 2 diabetes mellitus and healthy people. Prim. Care Diabetes 2021, 15, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Eberle, C.; Stichling, S. Impact of COVID-19 lockdown on glycemic control in patients with type 1 and type 2 diabetes mellitus: A systematic review. Diabetol. Metab. Syndr. 2021, 13, 95. [Google Scholar] [CrossRef]
- He, X.; Liu, C.; Peng, J.; Li, Z.; Li, F.; Wang, J.; Hu, A.; Peng, M.; Huang, K.; Fan, D.; et al. COVID-19 induces new-onset insulin resistance and lipid metabolic dysregulation via regulation of secreted metabolic factors. Signal Transduct. Target. Ther. 2021, 6, 427. [Google Scholar] [CrossRef]
- Satapathy, S.K.; Kuwajima, V.; Nadelson, J.; Atiq, O.; Sanyal, A.J. Drug-induced fatty liver disease: An overview of pathogenesis and management. Ann. Hepatol. 2015, 14, 789–806. [Google Scholar] [CrossRef]
- Kolaric, T.O.; Nincevic, V.; Kuna, L.; Duspara, K.; Bojanic, K.; Vukadin, S.; Raguz-Lucic, N.; Wu, G.Y.; Smolic, M. Drug-induced Fatty Liver Disease: Pathogenesis and Treatment. J. Clin. Transl. Hepatol. 2021, 9, 731–737. [Google Scholar] [CrossRef]
- Saverymuttu, S.H.; Joseph, A.E.; Maxwell, J.D. Ultrasound scanning in the detection of hepatic fibrosis and steatosis. Br. Med. J. (Clin. Res. Ed.) 1986, 292, 13–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saadeh, S.; Younossi, Z.M.; Remer, E.M.; Gramlich, T.; Ong, J.P.; Hurley, M.; Mullen, K.D.; Cooper, J.N.; Sheridan, M.J. The utility of radiological imaging in nonalcoholic fatty liver disease. Gastroenterology 2002, 123, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Pratt, D.S.; Kaplan, M.M. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N. Engl. J. Med. 2000, 342, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- Rosalki, S.; Rau, D.; Lehmann, D.; Prentice, M. Determination of serum γ-glutamyl transpeptidase activity and its clinical applications. Ann. Clin. Biochem. 1970, 7, 143–147. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Kaswala, D.H.; Lai, M.; Afdhal, N.H. Fibrosis Assessment in Nonalcoholic Fatty Liver Disease (NAFLD) in 2016. Dig. Dis. Sci. 2016, 61, 1356–1364. [Google Scholar] [CrossRef]
- COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. 2021. Available online: https://github.com/CSSEGISandData/COVID-19 (accessed on 1 October 2021).
- Julien, J.; Ayer, T.; Tapper, E.B.; Barbosa, C.; Dowd, W.N.; Chhatwal, J. Effect of increased alcohol consumption during COVID-19 pandemic on alcohol-associated liver disease: A modeling study. Hepatology 2022, 75, 1480–1490. [Google Scholar] [CrossRef]
- Joo, J.H.; Kim, H.J.; Park, E.C.; Jang, S.I. Association between sitting time and non-alcoholic fatty live disease in South Korean population: A cross-sectional study. Lipids Health Dis. 2020, 19, 212. [Google Scholar] [CrossRef]
- Chiang, D.J.; McCullough, A.J. The impact of obesity and metabolic syndrome on alcoholic liver disease. Clin. Liver Dis. 2014, 18, 157–163. [Google Scholar] [CrossRef]
- Fan, J.G.; Cai, X.B.; Li, L.; Li, X.J.; Dai, F.; Zhu, J. Alcohol consumption and metabolic syndrome among Shanghai adults: A randomized multistage stratified cluster sampling investigation. World J. Gastroenterol. 2008, 14, 2418–2424. [Google Scholar] [CrossRef]
- He, M.; Xian, Y.; Lv, X.; He, J.; Ren, Y. Changes in Body Weight, Physical Activity, and Lifestyle During the Semi-lockdown Period After the Outbreak of COVID-19 in China: An Online Survey. Disaster Med. Public Health Prep. 2021, 15, E23–E28. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.Y.; Song, S.-W.; Kim, H.-N.; Kang, S.G. Changes in Body Mass Index and Prevalence of Metabolic Syndrome during COVID-19 Lockdown Period. Korean J. Fam. Pract. 2021, 11, 304–311. [Google Scholar] [CrossRef]
- Thompson, K.; Dutton, D.J.; MacNabb, K.; Liu, T.; Blades, S.; Asbridge, M. Changes in alcohol consumption during the COVID-19 pandemic: Exploring gender differences and the role of emotional distress. Health Promot. Chronic Dis. Prev. Can. 2021, 41, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Guy, J.; Peters, M.G. Liver disease in women: The influence of gender on epidemiology, natural history, and patient outcomes. Gastroenterol. Hepatol. 2013, 9, 633–639. [Google Scholar]
- Becker, U.; Deis, A.; Sorensen, T.I.; Gronbaek, M.; Borch-Johnsen, K.; Muller, C.F.; Schnohr, P.; Jensen, G. Prediction of risk of liver disease by alcohol intake, sex, and age: A prospective population study. Hepatology 1996, 23, 1025–1029. [Google Scholar] [CrossRef]
- Kono, H.; Wheeler, M.D.; Rusyn, I.; Lin, M.; Seabra, V.; Rivera, C.A.; Bradford, B.U.; Forman, D.T.; Thurman, R.G. Gender differences in early alcohol-induced liver injury: Role of CD14, NF-kappaB, and TNF-alpha. Am. J. Physiol. Gastrointest. Liver Physiol. 2000, 278, G652–G661. [Google Scholar] [CrossRef] [Green Version]
- Schwenzer, N.F.; Springer, F.; Schraml, C.; Stefan, N.; Machann, J.; Schick, F. Non-invasive assessment and quantification of liver steatosis by ultrasound, computed tomography and magnetic resonance. J. Hepatol. 2009, 51, 433–445. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 5668) | Non-Drinker Group (N = 1972) | Alcohol Consumption Group (N = 3696) | p | |
|---|---|---|---|---|
| Age | 45.8 ± 8.9 | 47.8 ± 10.2 | 44.7 ± 7.9 | <0.001 |
| Sex (men) | 3362 (59.3%) | 800 (40.6%) | 2562 (69.3%) | <0.001 |
| Metropolitan area | 4452 (78.5%) | 1187 (60.2%) | 3265 (88.3%) | <0.001 |
| Hypertension | 756 (13.3%) | 254 (12.9%) | 502 (13.6%) | 0.484 |
| Diabetes | 276 (4.9%) | 118 (6.0%) | 158 (4.3%) | 0.005 |
| Dyslipidemia | 536 (9.5%) | 194 (9.8%) | 342 (9.3%) | 0.504 |
| Smoking | ||||
| Non-smoker | 3518 (62.1%) | 1526 (77.4%) | 1992 (53.9%) | <0.001 |
| Ex-smoker | 1120 (19.8%) | 253 (12.8%) | 867 (23.5%) | |
| Current smoker | 1030 (18.2%) | 193 (9.8%) | 837 (22.6%) | |
| Measurements | ||||
| Systolic BP (mm Hg) | 119.0 ± 14.2 | 118.4 ± 14.7 | 119.3 ± 13.9 | 0.037 |
| Diastolic BP (mm Hg) | 74.5 ± 10.7 | 73.5 ± 10.7 | 75.1 ± 10.6 | <0.001 |
| Pulse rate | 72.1 ± 11.5 | 72.2 ± 11.8 | 72.0 ± 11.4 | 0.495 |
| BMI (kg/m2) | 23.8 ± 3.4 | 23.4 ± 3.5 | 24.0 ± 3.3 | <0.001 |
| Laboratory tests | ||||
| AST (U/L) | 22.8 ± 10.7 | 21.7 ± 10.2 | 23.3 ± 10.9 | <0.001 |
| ALT (U/L) | 23.9 ± 17.8 | 22.0 ± 17.1 | 24.9 ± 18.0 | <0.001 |
| GGT (U/L) | 33.0 ± 36.3 | 24.7 ± 26.6 | 37.5 ± 39.9 | <0.001 |
| Glucose (mg/dL) | 96.0 ± 17.9 | 94.8 ± 17.2 | 96.7 ± 18.2 | <0.001 |
| FIB-4 | 0.95 ± 0.46 | 1.01 ± 0.55 | 0.92 ± 0.40 | <0.001 |
| Fatty liver on sonography | ||||
| No steatosis | 3246 (57.3%) | 1221 (61.9%) | 2025 (54.8%) | <0.001 |
| Mild | 1604 (28.3%) | 504 (25.6%) | 1100 (29.8%) | |
| Moderate-to-severe | 818 (14.4%) | 247 (12.5%) | 571 (15.4%) | |
| Visit 1 | Visit 2 | Visit 3 | p1–2 | p2–3 | |
|---|---|---|---|---|---|
| Alcohol consumer | 3696 (65.2%) | 3682 (65.0%) | 3637 (64.2%) | 0.265 | <0.001 |
| Response change | |||||
| From drinking to not drinking | 2.0% | 2.7% | |||
| From not drinking to drinking | 3.1% | 2.8% | |||
| Measurements | |||||
| Systolic BP (mm Hg) | 119.0 ± 14.2 | 119.7 ± 14.4 | 121.0 ± 14.0 | <0.001 | <0.001 |
| Diastolic BP (mm Hg) | 74.5 ± 10.7 | 74.3 ± 11.0 | 75.1 ± 11.1 | 0.066 | <0.001 |
| BMI (kg/m2) | 23.8 ± 3.4 | 23.9 ± 3.4 | 23.9 ± 3.4 | <0.001 | <0.001 |
| AST (U/L) | 22.8 ± 10.7 | 22.9 ± 11.0 | 23.4 ± 10.5 | 0.311 | 0.005 |
| ALT (U/L) | 23.9 ± 17.8 | 23.9 ± 18.4 | 24.6 ± 18.3 | 0.815 | 0.002 |
| GGT (U/L) | 33.0 ± 36.3 | 32.7 ± 36.8 | 31.5 ± 36.1 | 0.260 | <0.001 |
| Glucose (mg/dL) | 96.0 ± 17.9 | 97.2 ± 18.7 | 97.5 ± 18.3 | <0.001 | 0.114 |
| FIB-4 | 0.95 ± 0.46 | 0.99 ± 0.48 | 1.02 ± 0.49 | <0.001 | <0.001 |
| Fatty Liver Development | Fatty Liver Aggravation | ALT Abnormality | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | p | Odds Ratio | p | Odds Ratio | p | |
| Non-drinker group | ||||||
| Between visits 2 and 3 (vs. between visits 1 and 2) | 0.912 (0.684–1.216) | 0.529 | 1.034 (0.813–1.315) | 0.786 | 1.168 (0.862–1.583) | 0.317 |
| Age (/10 years) | 0.945 (0.825–1.082) | 0.415 | 0.934 (0.829–1.052) | 0.260 | 0.800 (0.684–0.936) | 0.005 |
| Men (vs. women) | 1.617 (1.117–2.343) | 0.011 | 1.155 (0.843–1.581) | 0.369 | 3.137 (2.122–4.638) | <0.001 |
| Obesity (≥25 kg/m2) | 1.910 (1.320–2.764) | <0.001 | 1.646 (1.257–2.154) | <0.001 | 2.908 (2.121–3.986) | <0.001 |
| Glucose (/10 mg/dL) | 1.184 (1.070–1.311) | 0.001 | 1.062 (0.985–1.145) | 0.117 | 1.068 (0.995–1.146) | 0.070 |
| Ever-smoker | 1.008 (0.643–1.578) | 0.973 | 1.066 (0.744–1.528) | 0.728 | 1.092 (0.755–1.580) | 0.640 |
| Alcohol consumption group | ||||||
| Between visits 2 and 3 (vs. between visits 1 and 2) | 1.300 (1.072–1.576) | 0.008 | 1.212 (1.033–1.422) | 0.018 | 1.320 (1.087–1.603) | 0.005 |
| Age (/10 years) | 1.041 (0.923–1.175) | 0.512 | 0.947 (0.854–1.050) | 0.299 | 0.852 (0.751–0.967) | 0.013 |
| Men (vs. women) | 1.355 (1.049–1.751) | 0.020 | 1.415 (1.135–1.765) | 0.002 | 3.859 (2.746–5.423) | <0.001 |
| Obesity (≥25 kg/m2) | 2.592 (2.096–3.206) | <0.001 | 1.846 (1.559–2.186) | <0.001 | 2.282 (1.872–2.782) | <0.001 |
| Glucose (/10 mg/dL) | 1.120 (1.058–1.186) | <0.001 | 1.041 (0.994–1.090) | 0.085 | 1.084 (1.036–1.134) | <0.001 |
| Ever-smoker | 1.058 (0.840–1.332) | 0.635 | 0.937 (0.778–1.128) | 0.492 | 1.019 (0.825–1.260) | 0.859 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haam, J.-H.; Hur, Y.-I.; Kim, Y.-S.; Kim, K.-K.; Kang, J.-H.; Ko, H.-J.; Cho, Y.J.; Choi, H.-I.; Lee, K.R.; Park, J.H.; et al. Fatty Liver Change in Korean Adults in a Systematic Social Distancing System Amid the COVID-19 Pandemic: A Multicenter Analysis. Int. J. Environ. Res. Public Health 2022, 19, 10444. https://doi.org/10.3390/ijerph191610444
Haam J-H, Hur Y-I, Kim Y-S, Kim K-K, Kang J-H, Ko H-J, Cho YJ, Choi H-I, Lee KR, Park JH, et al. Fatty Liver Change in Korean Adults in a Systematic Social Distancing System Amid the COVID-19 Pandemic: A Multicenter Analysis. International Journal of Environmental Research and Public Health. 2022; 19(16):10444. https://doi.org/10.3390/ijerph191610444
Chicago/Turabian StyleHaam, Ji-Hee, Yang-Im Hur, Young-Sang Kim, Kyoung-Kon Kim, Jee-Hyun Kang, Hae-Jin Ko, Yoon Jeong Cho, Hye-In Choi, Kyu Rae Lee, Jung Ha Park, and et al. 2022. "Fatty Liver Change in Korean Adults in a Systematic Social Distancing System Amid the COVID-19 Pandemic: A Multicenter Analysis" International Journal of Environmental Research and Public Health 19, no. 16: 10444. https://doi.org/10.3390/ijerph191610444