
Promoting University Students’ Mental Health through an Online Multicomponent Intervention during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Methods
2.1. Study Design
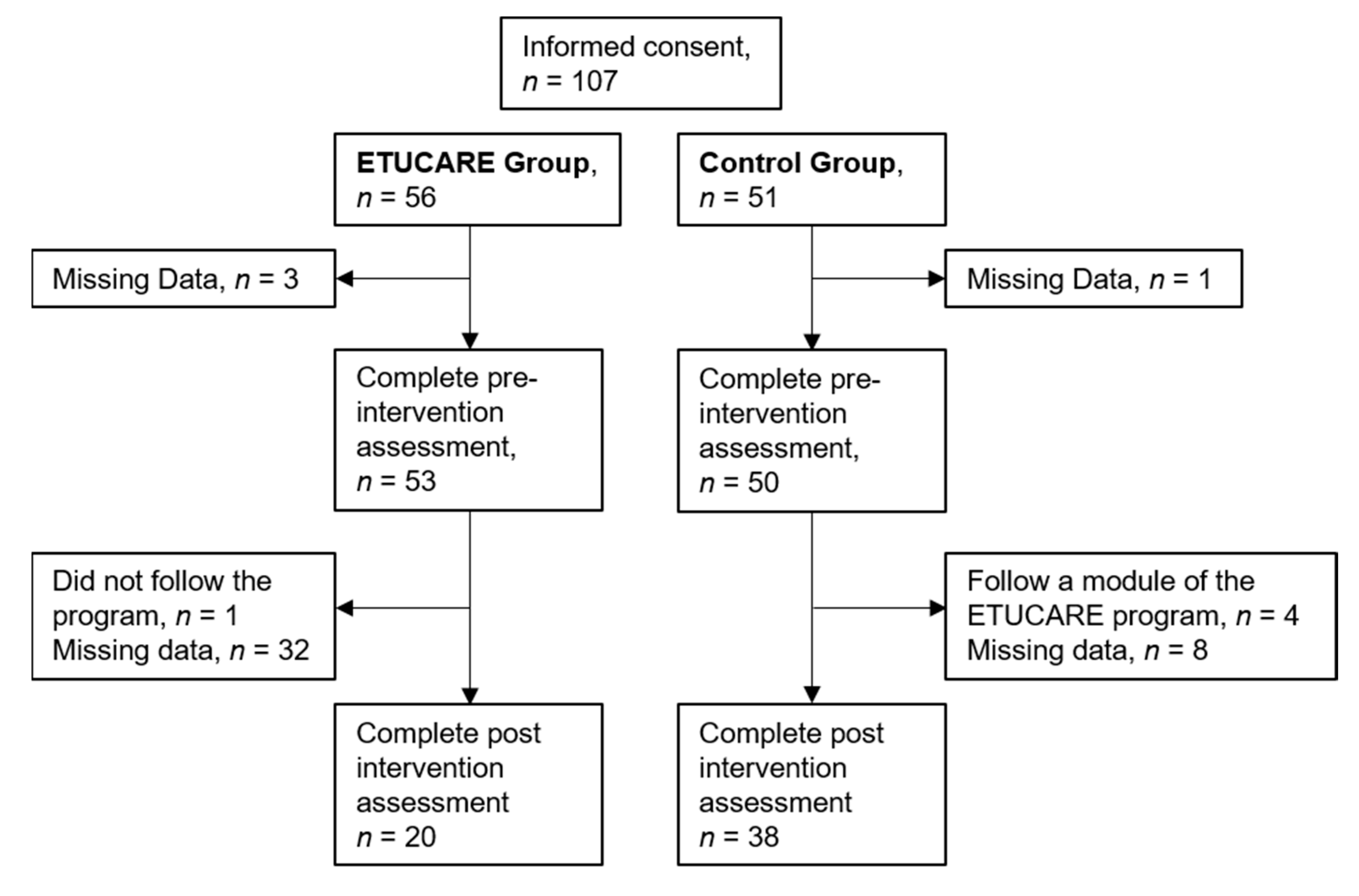
2.2. Participants and Procedure
2.2.1. Intervention Group
2.2.2. Control Group
2.3. Intervention
2.4. Measures
2.4.1. Kessler Psychological Distress Scale (K6)
2.4.2. The Generalized Anxiety Disorder 2-Item (GAD-2)
2.4.3. Patient Health Questionnaire 2-Item (PHQ-2)
2.4.4. The Insomnia Severity Index (ISI)
2.4.5. The Alcohol Use Disorders Identification Test-Concise (AUDIT-C)
2.4.6. The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS)
3. Results
3.1. Mental Health Problems at T0
3.2. Efficacy of the Web-Based Program on Student Mental Health Problems and Well-Being
3.3. Clinical Significance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fusar-Poli, P.; Correll, C.U.; Arango, C.; Berk, M.; Patel, V.; Ioannidis, J.P.A. Preventive psychiatry: A blueprint for improving the mental health of young people. World Psychiatry 2021, 20, 200–221. [Google Scholar] [CrossRef] [PubMed]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; Salazar de Pablo, G.; Il Shin, J.; Kirkbride, J.B.; Jones, P.; Kim, J.H. Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 2022, 27, 281–295. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, R.P.; Mortier, P.; Bruffaerts, R.; Alonso, J.; Benjet, C.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. WHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. J. Abnorm. Psychol. 2018, 127, 623–638. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.S.L. Student mental health: Some answers and more questions. J. Ment. Health 2018, 27, 193–196. [Google Scholar] [CrossRef] [Green Version]
- Fond, G.; Bourbon, A.; Auquier, P.; Micoulaud-Franchi, J.-A.; Lançon, C.; Boyer, L. Venus and Mars on the benches of the faculty: Influence of gender on mental health and behavior of medical students. Results from the BOURBON National Study. J. Affect. Disord. 2018, 239, 146–151. [Google Scholar] [CrossRef]
- Hazart, J.; Blanquet, M.; Debost-Legrand, A.; Perreve, A.; Léger, S.; Martoia, V.; Maurice, S.; Brousse, G.; Gerbaud, L. A screening focusing on aftereffects of alcohol consumption in a student population. A national cross-sectional survey. J. Prev. Med. Hyg. 2018, 59, E48. [Google Scholar]
- Perino, J.; Tournier, M.; Mathieu, C.; Letinier, L.; Peyré, A.; Perret, G.; Pereira, E.; Fourrier-Réglat, A.; Pollet, C.; Fatseas, M. Psychoactive substance use among students: A cross-sectional analysis. Fundam. Clin. Pharmacol. 2022. [Google Scholar] [CrossRef]
- Kovess-Masfety, V.; Leray, E.; Denis, L.; Husky, M.; Pitrou, I.; Bodeau-Livinec, F. Mental health of college students and their non-college-attending peers: Results from a large french cross-sectional survey. BMC Psychol. 2016, 4, 20. [Google Scholar] [CrossRef] [Green Version]
- Basson, M.J.; Rothmann, S. Pathways to flourishing among pharmacy students: The role of study demands and lecturer support. J. Psychol. Afr. 2019, 29, 338–345. [Google Scholar] [CrossRef]
- Weber, J.; Skodda, S.; Muth, T.; Angerer, P.; Loerbroks, A. Stressors and resources related to academic studies and improvements suggested by medical students: A qualitative study. BMC Med. Educ. 2019, 19, 312. [Google Scholar] [CrossRef]
- Mertens, G.; Gerritsen, L.; Duijndam, S.; Salemink, E.; Engelhard, I.M. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J. Anxiety Disord. 2020, 74, 102258. [Google Scholar] [CrossRef] [PubMed]
- Bergin, A.; Pakenham, K. Law student stress: Relationships between academic demands, social isolation, career pressure, study/life imbalance and adjustment outcomes in law students. Psychiatry Psychol. Law 2015, 22, 388–406. [Google Scholar] [CrossRef]
- Mokgele, K.R.; Rothmann, S. A structural model of student well-being. South Afr. J. Psychol. 2014, 44, 514–527. [Google Scholar] [CrossRef]
- Fawzy, M.; Hamed, S.A. Prevalence of psychological stress, depression and anxiety among medical students in Egypt. Psychiatry Res. 2017, 255, 186–194. [Google Scholar] [CrossRef]
- Martineau, M.; Beauchamp, G.; Marcotte, D. Efficacité des interventions en prévention et en promotion de la santé mentale dans les établissements d’enseignement postsecondaire. St. Ment. Québec 2017, 42, 165–182. [Google Scholar] [CrossRef] [Green Version]
- Grøtan, K.; Sund, E.R.; Bjerkeset, O. Mental health, academic self-efficacy and study progress among college students—The SHoT study, Norway. Front. Psychol. 2019, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Lipson, S.K.; Phillips, M.V.; Winquist, N.; Eisenberg, D.; Lattie, E.G. Mental health conditions among community college students: A national study of prevalence and use of treatment services. Psychiatr. Serv. 2021, 72, 1126–1133. [Google Scholar] [CrossRef]
- Theurel, A.; Witt, A. Identifying barriers to mental health help-seeking in French university students during the COVID-19 pandemic. Creat. Educ. 2022, 13, 437–449. [Google Scholar] [CrossRef]
- Morvan, Y.; Coulange, I.; Krebs, M.-O.; Boujut, E.; Romo, L. La santé psychique des étudiants. In Les Vies Etudiantes. Tendances et Inégalités; Giret, J.F., Van de Velde, C., Verley, E., Eds.; La Documentation Française: Paris, France, 2016; pp. 213–234. [Google Scholar]
- Verger, P.; Guagliardo, V.; Gilbert, F.; Rouillon, F.; Kovess-Masfety, V. Psychiatric disorders in students in six French universities: 12-month prevalence, comorbidity, impairment and help-seeking. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 189–199. [Google Scholar] [CrossRef]
- Kecojevic, A.; Basch, C.H.; Sullivan, M.; Davi, N.K. The impact of the COVID-19 epidemic on mental health of undergraduate students in New Jersey, cross-sectional study. PLoS ONE 2020, 15, e0239696. [Google Scholar] [CrossRef]
- Sun, S.; Goldberg, S.B.; Lin, D.; Qiao, S.; Operario, D. Psychiatric symptoms, risk, and protective factors among university students in quarantine during the COVID-19 pandemic in China. Glob. Health 2021, 17, 15. [Google Scholar] [CrossRef] [PubMed]
- Charbonnier, E.; Le Vigouroux, S.; Goncalves, A. Psychological vulnerability of French university students during the COVID-19 pandemic: A four-wave longitudinal survey. Int. J. Environ. Res. Public Health 2021, 18, 9699. [Google Scholar] [CrossRef]
- Roux, J.; Lefort, M.; Bertin, M.; Padilla, C.; Mueller, J.; Garlantézec, R.; Pivette, M.; Le Tertre, A.; Crepey, P. Impact de la Crise Sanitaire de la COVID-19 sur la Santé Mentale des Étudiants à Rennes, France; HAL Working Paper No. 03172226; HAL Open Sciene: Lyon, France, 2021. [Google Scholar]
- Wathelet, M.; Duhem, S.; Vaiva, G.; Baubet, T.; Habran, E.; Veerapa, E.; Debien, C.; Molenda, S.; Horn, M.; Grandgenèvre, P.; et al. Factors associated with mental health disorders among university students in France confined during the COVID-19 pandemic. JAMA Netw. Open 2020, 3, e2025591. [Google Scholar] [CrossRef] [PubMed]
- Arsandaux, J.; Montagni, I.; Macalli, M.; Texier, N.; Pouriel, M.; Germain, R.; Mebarki, A.; Kinouani, S.; Tournier, M.; Schück, S.; et al. Higher risk of mental health deterioration during the COVID-19 lockdown among students rather than non-students. The French confins study. medRxiv 2020. [Google Scholar] [CrossRef]
- Flaudias, V.; Iceta, S.; Zerhouni, O.; Rodgers, R.F.; Billieux, J.; Llorca, P.-M.; Boudesseul, J.; de Chazeron, I.; Romo, L.; Maurage, P.; et al. COVID-19 pandemic lockdown and problematic eating behaviors in a student population. J. Behav. Addict. 2020, 9, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Trabelsi, K. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: Insight from the ECLB-COVID19 multicenter study. Biol. Sport 2021, 38, 9–21. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Suárez-Iglesias, D.; Sanchez-Lastra, M.A.; Ayán, C. Impact of COVID-19 pandemic on university students’ physical activity levels: An early systematic review. Front. Psychol. 2021, 11, 624567. [Google Scholar] [CrossRef]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Bertrand, L.; Shaw, K.A.; Ko, J.; Deprez, D.; Chilibeck, P.D.; Zello, G.A. The impact of the coronavirus disease 2019 (COVID-19) pandemic on university students’ dietary intake, physical activity, and sedentary behaviour. Appl. Physiol. Nutr. Metab. 2021, 46, 265–272. [Google Scholar] [CrossRef]
- Olfert, M.D.; Wattick, R.A.; Saurborn, E.G.; Hagedorn, R.L. Impact of COVID-19 on college student diet quality and physical activity. Nutr. Health 2022. [Google Scholar] [CrossRef]
- Sahu, P. Closure of universities due to coronavirus disease 2019 (COVID-19): Impact on education and mental health of students and academic staff. Cureus 2020, 12, e7541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, W. Online and remote learning in higher education institutes: A necessity in light of COVID-19 pandemic. High. Educ. Stud. 2020, 10, 16–25. [Google Scholar] [CrossRef]
- Besser, A.; Flett, G.L.; Zeigler-Hill, V. Adaptability to a sudden transition to online learning during the COVID-19 pandemic: Understanding the challenges for students. Scholarsh. Teach. Learn. Psychol. 2022, 8, 85–105. [Google Scholar] [CrossRef]
- Lee, J. Mental health effects of school closures during COVID-19. Lancet Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef]
- Fernández-Castillo, A. State-anxiety and academic burnout regarding university access selective examinations in Spain during and after the COVID-19 lockdown. Front. Psychol. 2021, 12, 621863. [Google Scholar] [CrossRef]
- Zis, P.; Artemiadis, A.; Bargiotas, P.; Nteveros, A.; Hadjigeorgiou, G.M. Medical studies during the COVID-19 pandemic: The impact of digital learning on medical students’ burnout and mental health. Int. J. Environ. Res. Public Health 2021, 18, 349. [Google Scholar] [CrossRef]
- Laurent, L. Rapport d’information Fait au Nom de la Mission d’information sur les Conditions de la Vie Étudiante en France sur l’accompagnement des Étudiants: Une Priorité et un Enjeu d’avenir pour l’État et les Collectivités; Sénat: Paris, France, 2021; 283p, Available online: http://www.senat.fr/rap/r20-742/r20-7421.pdf (accessed on 16 June 2022).
- Haut Conseil de la Santé Publique. Avis du Haut Conseil de la Santé Publique Relatif à l’impact du COVID-19 sur la Santé Mentale; Haut Conseil de la Santé Publique: Paris, France, 2021; 124p, Available online: https://www.hcsp.fr/Explore.cgi/avisrapportsdomaine?clefr=1097 (accessed on 16 June 2022).
- Montagni, I.; Tzourio, C.; Cousin, T.; Sagara, J.A.; Bada-Alonzi, J.; Horgan, A. Mental health-related digital use by university students: A systematic review. Telemed. e-Health 2020, 26, 131–146. [Google Scholar] [CrossRef] [Green Version]
- Clement, S.; Schauman, O.; Graham, T.; Maggioni, F.; Evans-Lacko, S.; Bezborodovs, N.; Morgan, C.; Rüsch, N.; Brown, J.S.L.; Thornicroft, G. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol. Med. 2015, 45, 11–27. [Google Scholar] [CrossRef]
- Salaheddin, K.; Mason, B. Identifying barriers to mental health help-seeking among young adults in the UK: A cross-sectional survey. Br. J. Gen. Pract. 2016, 66, e686. [Google Scholar] [CrossRef]
- Davies, E.B.; Morriss, R.; Glazebrook, C. Computer-delivered and web-based interventions to improve depression, anxiety, and psychological well-being of university students: A systematic review and meta-analysis. J. Med. Internet Res. 2014, 16, e130. [Google Scholar] [CrossRef] [Green Version]
- Ebert, D.D.; Van Daele, T.; Nordgreen, T.; Karekla, M.; Compare, A.; Zarbo, C.; Brugnera, A.; Øverland, S.; Trebbi, G.; Jensen, K.L.; et al. Internet- and mobile-based psychological interventions: Applications, efficacy, and potential for improving mental health: A report of the EFPA E-Health Taskforce. Eur. Psychol. 2018, 23, 167–187. [Google Scholar] [CrossRef]
- Zhou, T.; Li, X.; Pei, Y.; Gao, J.; Kong, J. Internet-based cognitive behavioural therapy for subthreshold depression: A systematic review and meta-analysis. BMC Psychiatry 2016, 16, 356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, E.M.; Destree, L.; Albertella, L.; Fontenelle, L.F. Internet-based acceptance and commitment therapy: A transdiagnostic systematic review and meta-analysis for mental health outcomes. Behav. Ther. 2021, 52, 492–507. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Adam, S.H.; Baumeister, H.; Cuijpers, P.; Karyotaki, E.; Auerbach, R.P.; Kessler, R.C.; Bruffaerts, R.; Berking, M.; Ebert, D.D. Internet interventions for mental health in university students: A systematic review and meta-analysis. Int. J. Methods Psychiatr. Res. 2019, 28, e1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lattie, E.G.; Adkins, E.C.; Winquist, N.; Stiles-Shields, C.; Wafford, Q.E.; Graham, A.K. Digital mental health interventions for depression, anxiety, and enhancement of psychological well-being among college students: Systematic review. J. Med. Internet Res. 2019, 21, e12869. [Google Scholar] [CrossRef]
- Lehtimaki, S.; Martic, J.; Wahl, B.; Foster, K.T.; Schwalbe, N. Evidence on digital mental health interventions for adolescents and young people: Systematic overview. JMIR Ment. Health 2021, 8, e25847. [Google Scholar] [CrossRef]
- Bennett, C.B.; Ruggero, C.J.; Sever, A.C.; Yanouri, L. EHealth to redress psychotherapy access barriers both new and old: A review of reviews and meta-analyses. J. Psychother. Integr. 2020, 30, 188–207. [Google Scholar] [CrossRef]
- Torous, J.; Myrick, K.J.; Rauseo-Ricupero, N.; Firth, J. Digital mental health and COVID-19: Using technology today to accelerate the curve on access and quality tomorrow. JMIR Ment. Health 2020, 7, e18848. [Google Scholar] [CrossRef]
- Willems, S.H.; Rao, J.; Bhambere, S.; Patel, D.; Biggins, Y.; Guite, J.W. Digital solutions to alleviate the burden on health systems during a public health care crisis: COVID-19 as an opportunity. JMIR mHealth uHealth 2021, 9, e25021. [Google Scholar] [CrossRef]
- González-García, M.; Álvarez, J.C.; Pérez, E.Z.; Fernandez-Carriba, S.; López, J.G. Feasibility of a brief online mindfulness and compassion-based intervention to promote mental health among university students during the COVID-19 pandemic. Mindfulness 2021, 12, 1685–1695. [Google Scholar] [CrossRef]
- Krifa, I.; Hallez, Q.; van Zyl, L.E.; Braham, A.; Sahli, J.; Ben Nasr, S.; Shankland, R. Effectiveness of an online positive psychology intervention among Tunisian healthcare students on mental health and study engagement during the COVID-19 pandemic. Appl. Psychol. Health Well-Being 2021. [Google Scholar] [CrossRef] [PubMed]
- Charbonnier, E.; Trémolière, B.; Baussard, L.; Goncalves, A.; Lespiau, F.; Philippe, A.G.; Vigouroux, S.L. Effects of an online self-help intervention on university students’ mental health during COVID-19: A non-randomized controlled pilot study. Comput. Hum. Behav. Rep. 2022, 5, 100175. [Google Scholar] [CrossRef] [PubMed]
- Becker, T.D.; Torous, J.B. Recent developments in digital mental health interventions for college and university students. Curr. Treat. Options Psychiatry 2019, 6, 210–220. [Google Scholar] [CrossRef]
- van Agteren, J.; Iasiello, M.; Lo, L.; Bartholomaeus, J.; Kopsaftis, Z.; Carey, M.; Kyrios, M. A systematic review and meta-analysis of psychological interventions to improve mental wellbeing. Nat. Hum. Behav. 2021, 5, 631–652. [Google Scholar] [CrossRef]
- Schaeuffele, C.; Schulz, A.; Knaevelsrud, C.; Renneberg, B.; Boettcher, J. CBT at the crossroads: The rise of transdiagnostic treatments. Int. J. Cogn. Ther. 2021, 14, 86–113. [Google Scholar] [CrossRef]
- Przybylko, G.; Morton, D.P.; Renfrew, M.E. Addressing the COVID-19 mental health crisis: A perspective on using interdisciplinary universal interventions. Front. Psychol. 2021, 12, 644337. [Google Scholar] [CrossRef]
- Petrides, J.; Collins, P.; Kowalski, A.; Sepede, J.; Vermeulen, M. Lifestyle changes for disease prevention. Prim. Care Clin. Off. Pract. 2019, 46, 1–12. [Google Scholar] [CrossRef]
- Firth, J.; Solmi, M.; Wootton, R.E.; Vancampfort, D.; Schuch, F.B.; Hoare, E.; Gilbody, S.; Torous, J.; Teasdale, S.B.; Jackson, S.E. A meta-review of “lifestyle psychiatry”: The role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry 2020, 19, 360–380. [Google Scholar] [CrossRef]
- Achilles, M.R.; Anderson, M.; Li, S.H.; Subotic-Kerry, M.; Parker, B.; O’Dea, B. Adherence to e-mental health among youth: Considerations for intervention development and research design. Digit. Health 2020, 6, 2055207620926064. [Google Scholar] [CrossRef]
- Garrido, S.; Millington, C.; Cheers, D.; Boydell, K.; Schubert, E.; Meade, T.; Nguyen, Q.V. What works and what doesn’t work? A systematic review of digital mental health interventions for depression and anxiety in young people. Front. Psychiatry 2019, 10, 759. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Monahan, P.O.; Löwe, B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Janet, B.W.; Williams, J.B. The patient health questionnaire-2: Validity of a two-item depression screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol use disorders identification test. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COVIPREV Study. Available online: https://www.santepubliquefrance.fr/etudes-et-enquetes/coviprev-une-enquete-pour-suivre-l-evolution-des-comportements-et-de-la-sante-mentale-pendant-l-epidemie-de-covid-19 (accessed on 16 June 2022).
- Manea, L.; Gilbody, S.; Hewitt, C.; North, A.; Plummer, F.; Richardson, R.; Thombs, B.D.; Williams, B.; McMillan, D. Identifying depression with the PHQ-2: A diagnostic meta-analysis. J. Affect. Disord. 2016, 203, 382–395. [Google Scholar] [CrossRef]
- van Agteren, J.; Ali, K.; Fassnacht, D.B.; Iasiello, M.; Furber, G.; Howard, A.; Woodyatt, L.; Musker, M.; Kyrios, M. Testing the differential impact of an internet-based mental health intervention on outcomes of well-being and psychological distress during COVID-19: Uncontrolled intervention study. JMIR Ment. Health 2021, 8, e28044. [Google Scholar] [CrossRef]
- Zachariae, R.; Lyby, M.S.; Ritterband, L.M.; O’Toole, M.S. Efficacy of internet-delivered cognitive-behavioral therapy for insomnia—A systematic review and meta-analysis of randomized controlled trials. Sleep Med. Rev. 2016, 30, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kahale, L.A.; Diab, B.; Khamis, A.M.; Chang, Y.; Lopes, L.C.; Agarwal, A.; Li, L.; Mustafa, R.A.; Koujanian, S.; Waziry, R.; et al. Potentially missing data are considerably more frequent than definitely missing data: A methodological survey of 638 randomized controlled trials. J. Clin. Epidemiol. 2019, 106, 18–31. [Google Scholar] [CrossRef]
- Linardon, J.; Fuller-Tyszkiewicz, M. Attrition and adherence in smartphone-delivered interventions for mental health problems: A systematic and meta-analytic review. J. Consult. Clin. Psychol. 2020, 88, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, I.D.; Forand, N.R.; Strunk, D.R. Predictors of dropout in internet-based cognitive behavioral therapy for depression. Cogn. Ther. Res. 2019, 43, 620–630. [Google Scholar] [CrossRef] [PubMed]
- Borghouts, J.; Eikey, E.; Mark, G.; De Leon, C.; Schueller, S.M.; Schneider, M.; Stadnick, N.; Zheng, K.; Mukamel, D.; Sorkin, D.H. Barriers to and facilitators of user engagement with digital mental health interventions: Systematic review. J. Med. Internet Res. 2021, 23, e24387. [Google Scholar] [CrossRef]
- Looyestyn, J.; Kernot, J.; Boshoff, K.; Ryan, J.; Edney, S.; Maher, C. Does gamification increase engagement with online programs? A systematic review. PLoS ONE 2017, 12, e0173403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huckins, J.F.; daSilva, A.W.; Wang, W.; Hedlund, E.; Rogers, C.; Nepal, S.K.; Wu, J.; Obuchi, M.; Murphy, E.I.; Meyer, M.L.; et al. Mental health and behavior of college students during the early phases of the COVID-19 pandemic: Longitudinal smartphone and ecological momentary assessment study. J. Med. Internet Res. 2020, 22, e20185. [Google Scholar] [CrossRef]


{kind=link}
| Theme | Content | Weekly Panel of Exercises and Activities |
|---|---|---|
| Module 1: Mental Health Information | Definition of mental health, positive mental health, and common psychological problems Mental health risk and protective factors How and where to seek help for a mental health problem How to take care of one’s own mental health Program schedule | Online mental health self-assessment quizzes |
| Module 2: Stress management | Definition and explanation of stress and stressors Impact of stress on our body and feelings. Effect of physical activity and nature (e.g., birdsong, forest) on stress Relaxation strategies to cope with stress | Body scan meditation Breathing control exercise Progressive muscle relaxation Increasing “recharge” activities Increasing physical activity Increasing immersion in natural environment Problem resolution |
| Module 3: Procrastinaton and Motivation for Learning | Explanation of procrastination in everyday life Basic procrastination triggers Self-assessment tools to identify one’s own procrastination behaviors Definition of self-blame and its effects Misconceptions about failure and perfectionism Processes involved in motivation | Self-compassion exerciseMindful breathingSetting smart goals |
| Module 4: Sleep and insomnia | Definition and explanation of sleep and insomnia Introduction to the concept of the link between thoughts, feelings, and behaviour. Link between sleep, physical activity, and diet Self-assessment tools on sleep hygiene and sleep quality | Mindfulness meditation Worry journal Sleep hygiene Stimulus control for insomnia |
| Module 5: Self-Awareness | Introduction to the concept of self-esteem and to activities that could help to enhance self-esteem. Identifying and using one’s strength Identifying and reconnecting to one’s value | VIA Character Strengths Survey Cultivating one’s strengths Vision board Engagement in meaningful actions |
| Module 6: Emotion regulation | Definition and explanation of emotions and their usefulness in daily life Explanation of the link between thoughts, feelings, and behaviour Introduction to thinking errors and how to manage them Mood tracker tool Emotion regulation self-assessment Link between healthy behaviors and mood Introduction to positive emotion and strategies to cultivate positive emotions in daily life | Cognitive reappraisal Tolerating distress Reorientation of attention towards the positive and satisfying aspects of life Gratitude wall Savouring the present moment |
| Module 7: Meaningful Relationships | Discuss the importance of having a good relationship. Learn specific skills that are needed to get along with other people (communication skills and assertiveness) Assertiveness self-assessment Learn to deal with social problem | Random acts of kindness Reorientation of attention towards the positive in relationships Active listening Assertiveness exercise Gratitude letter |
| Module 8: Booster | Presentation of the highlights of the different modules | Continue exercises found to be helpful. |
| ETUCARE Group (n = 53) | Control Group (n = 50) | Total Sample (N = 103) | Main National Surveys | |
|---|---|---|---|---|
| Severe psychological distress | 40% | 27% | 34% | COVER: 60% CN2R: 22% |
| Anxiety | 57% | 51% | 54% | COVER: 38% CONFINS: 24% CN2R: 28% COVIPREV: 34% |
| Depression | 53% | 33% | 43% | COVER: 23% CONFINS: 33% CN2R: 16% COVIPREV: 43% |
| Sleep problems | 74% | 68% | 71% | COVIPREV: 73% |
| Hazardous drinking | 32% | 47% | 39% | BOURBON: 40% |
| ETUCARE Group | Control Group | Control Group vs. ETUCARE Group | ||||
|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | |||
| M (SD) | M (SD) | M (SD) | M (SD) | F (1, 56) | p | |
| Kessler 6 | 11.00 (4.34) | 10.50 (6.64) | 9.11 (4.33) | 9.97 (4.97) | 2.16 | 0.14 |
| Gad 2 | 2.90 (1.83) | 3.00 (1.86) | 2.79 (1.97) | 3.34 (1.92) | 1.46 | 0.23 |
| PHQ 2 | 2.90 (1.68) | 2.20 (1.58) | 1.84 (1.46) | 1.79 (1.58) | 3.41 | 0.07 |
| WEMWBS | 36.30 (7.67) | 40.10 (9.47) | 41.50 (8.76) | 41.76 (7.87) | 4.45 | 0.04 |
| ISI | 9.30 (5.78) | 9.90 (3.78) | 11.26 (5.00) | 10.24 (3.96) | 1.89 | 0.17 |
| Audit | 1.75 (1.89) | 1.55 (1.93) | 2.92 (2.77) | 3.13 (2.62) | 1.52 | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theurel, A.; Witt, A.; Shankland, R. Promoting University Students’ Mental Health through an Online Multicomponent Intervention during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 10442. https://doi.org/10.3390/ijerph191610442
Theurel A, Witt A, Shankland R. Promoting University Students’ Mental Health through an Online Multicomponent Intervention during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(16):10442. https://doi.org/10.3390/ijerph191610442
Chicago/Turabian StyleTheurel, Anne, Arnaud Witt, and Rebecca Shankland. 2022. "Promoting University Students’ Mental Health through an Online Multicomponent Intervention during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 16: 10442. https://doi.org/10.3390/ijerph191610442