
Donating Health Data to Research: Influential Characteristics of Individuals Engaging in Self-Tracking


Abstract
:1. Introduction
2. Background
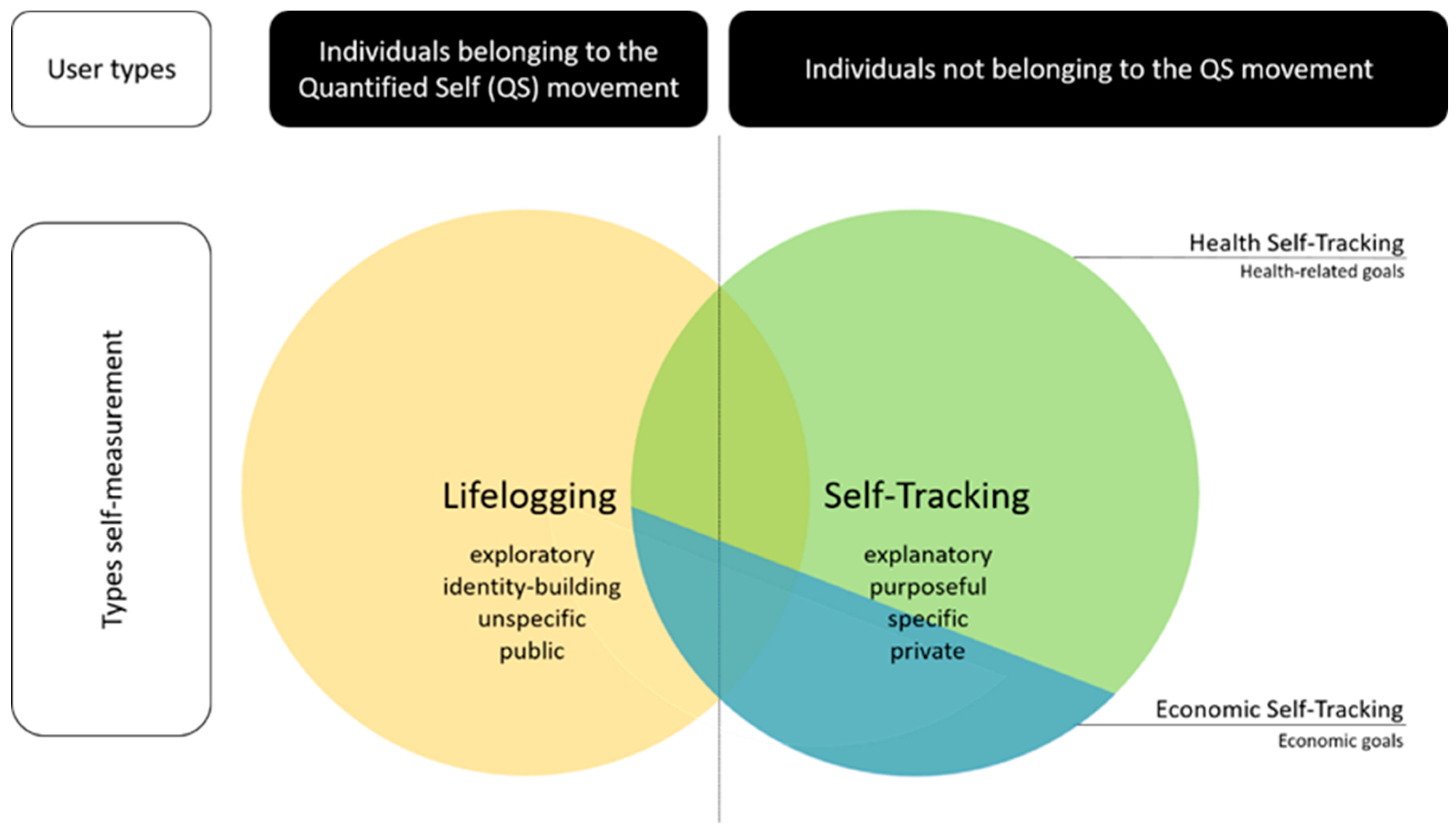
2.1. Self-Measurement Framework
2.2. Research Questions and Hypothesis Development
3. Materials and Methods
4. Results
4.1. Sample
4.2. Data Sharing and Showing Behaviors Compared to Data Donation Willingness
4.3. User Characteristics Influencing Data Donation Willingness
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mopas, M.S.; Huybregts, E. Training by feel: Wearable fitness-trackers, endurance athletes, and the sensing of data. Sens. Soc. 2020, 15, 25–40. [Google Scholar] [CrossRef]
- Hicks, J.L.; Althoff, T.; Kuhar, P.; Bostjancic, B.; King, A.C.; Leskovec, J.; Delp, S.L. Best practices for analyzing large-scale health data from wearables and smartphone apps. NPJ Digit. Med. 2019, 2, 45. [Google Scholar] [CrossRef] [PubMed]
- Kunz, T.; Lange, B.; Selzer, A. Datenschutz und Datensicherheit in Digital Public Health. Bundesgesundheitsblatt-Gesundh.-Gesundh. 2020, 63, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Budzinski, O.; Schneider, S. Smart Fitness: Ökonomische Effekte Einer Digitalisierung Der Selbstvermessung (Smart Fitness: Economic Effects of Digitalized Self-Tracking). Tech. Univ. Ilmenau Inst. Volkswirtsch. Diskuss. 2017, 43, 89–124. [Google Scholar]
- Pattison, J.E. Effects of touch on self-exploration and the therapeutic relationship. J. Consult. Clin. Psychol. 1973, 40, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Lupton, D. ‘It’s made me a lot more aware’: A new materialist analysis of health self-tracking. Media Int. Aust. 2019, 171, 66–79. [Google Scholar] [CrossRef]
- Fox, N.J. Personal health technologies, micropolitics and resistance: A new materialist analysis. Health 2017, 21, 136–153. [Google Scholar] [CrossRef] [Green Version]
- Swan, M. Emerging patient-driven health care models: An examination of health social networks, consumer personalized medicine and quantified self-tracking. Int. J. Environ. Res. Public Health 2009, 6, 492–525. [Google Scholar] [CrossRef]
- Sanders, R. Self-tracking in the digital era: Biopower, patriarchy, and the new biometric body projects. Body Soc. 2017, 23, 36–63. [Google Scholar] [CrossRef]
- Whitson, J.R. Foucault’s fitbit: Governance and gamification. In The Gameful World: Approaches, Issues, Applications; MIT Press: Cambridge, MA, USA, 2014; pp. 339–358. [Google Scholar]
- Heyen, N.B. From self-tracking to self-expertise: The production of self-related knowledge by doing personal science. Public Underst. Sci. 2020, 29, 124–138. [Google Scholar] [CrossRef] [Green Version]
- Karkar, R.; Zia, J.; Vilardaga, R.; Mishra, S.R.; Fogarty, J.; Munson, S.A.; Kientz, J.A. A framework for self-experimentation in personalized health. J. Am. Med. Inform. Assoc. 2016, 23, 440–448. [Google Scholar] [CrossRef] [Green Version]
- Korjian, S.; Gibson, C.M. Digital technologies and the democratization of clinical research: Social media, wearables, and artificial intelligence. Contemp. Clin. Trials 2022, 117, 106767. [Google Scholar] [CrossRef]
- Saleem, J.J.; Wilck, N.R.; Murphy, J.J.; Herout, J. Veteran and Staff Experience from a Pilot Program of Health Care System–Distributed Wearable Devices and Data Sharing. Appl. Clin. Inform. 2022, 13, 532–540. [Google Scholar] [CrossRef]
- Abdullah, S.; Arshad, J.; Khan, M.M.; Alazab, M.; Salah, K. PRISED tangle: A privacy-aware framework for smart healthcare data sharing using IOTA tangle. In Complex & Intelligent Systems; Springer: Berlin/Heidelberg, Germany, 2022; pp. 1–19. [Google Scholar]
- Marchioro, T.; Kazlouski, A.; Markatos, E. How to Publish Wearables’ Data: Practical Guidelines to Protect User Privacy. Stud. Health Technol. Inform. 2022, 294, 949–950. [Google Scholar] [PubMed]
- FDA. Real-World Evidence. Available online: https://www.fda.gov/science-research/science-and-research-special-topics/real-world-evidence (accessed on 22 July 2022).
- Shaw, D.M.; Gross, J.V.; Erren, T.C. Data donation after death: A proposal to prevent the waste of medical research data. EMBO Rep. 2016, 17, 14–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strotbaum, V.; Pobiruchin, M.; Schreiweis, B.; Wiesner, M.; Strahwald, B. Your data is gold–Data donation for better healthcare? It-Inf. Technol. 2019, 61, 219–229. [Google Scholar] [CrossRef]
- Gay, V.; Leijdekkers, P. Bringing health and fitness data together for connected health care: Mobile apps as enablers of interoperability. J. Med. Internet Res. 2015, 17, e260. [Google Scholar] [CrossRef]
- Sharon, T. Self-tracking for health and the quantified self: Re-articulating autonomy, solidarity, and authenticity in an age of personalized healthcare. Philos. Technol. 2017, 30, 93–121. [Google Scholar] [CrossRef] [Green Version]
- Niknejad, N.; Ismail, W.B.; Mardani, A.; Liao, H.; Ghani, I. A comprehensive overview of smart wearables: The state of the art literature, recent advances, and future challenges. Eng. Appl. Artif. Intell. 2020, 90, 103529. [Google Scholar] [CrossRef]
- Lupton, D. Data mattering and self-tracking: What can personal data do? Continuum 2020, 34, 1–13. [Google Scholar] [CrossRef]
- Lupton, D. Self-Tracking Modes: Reflexive Self-Monitoring and Data Practices. Available at SSRN 2483549. 2014. Available online: https://ssrn.com/abstract=2483549 (accessed on 4 May 2021).
- Lomborg, S.; Frandsen, K. Self-tracking as communication. Inf. Commun. Soc. 2016, 19, 1015–1027. [Google Scholar] [CrossRef] [Green Version]
- Gurrin, C.; Smeaton, A.F.; Doherty, A.R. Lifelogging: Personal big data. Found. Trends Inf. Retr. 2014, 8, 1–125. [Google Scholar] [CrossRef]
- Wolf, G. What is The Quantified Self? In Quantified Seld Homepage; 2011; Available online: https://quantifiedself.com/blog/what-is-the-quantified-self/ (accessed on 4 May 2021).
- Lee, V.R. The Quantified Self (QS) Movement and Some Emerging Opportunities for the Educational Technology Field. Educ. Technol. 2013, 53, 39–42. [Google Scholar]
- Nafus, D.; Sherman, J. Big data, big questions|this one does not go up to 11: The quantified self movement as an alternative big data practice. Int. J. Commun. 2014, 8, 11. [Google Scholar]
- Selke, S. Einleitung. In Lifelogging: Digitale Selbstvermessung und Lebensprotokollierung Zwischen Disruptiver Technologie und kulturellem Wandel; Selke, S., Ed.; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2016; pp. 1–21. [Google Scholar]
- Choe, E.K.; Lee, N.B.; Lee, B.; Pratt, W.; Kientz, J.A. Understanding quantified-selfers’ practices in collecting and exploring personal data. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Toronto, ON, Canada, 26 April–1 May 2014; pp. 1143–1152. [Google Scholar]
- Sjöklint, M.; Constantiou, I.D.; Trier, M. The Complexities of Self-Tracking-An Inquiry into User Reactions and Goal Attainment. Available at SSRN 2611193. 2015. Available online: https://ssrn.com/abstract=2611193 (accessed on 4 May 2021).
- Lupton, D. Understanding the human machine [Commentary]. IEEE Technol. Soc. Mag. 2013, 32, 25–30. [Google Scholar] [CrossRef]
- Jones, D.H. All the moments of our lives: Self-archiving from Christian Boltanski to lifelogging. Arch. Rec. 2015, 36, 29–41. [Google Scholar] [CrossRef]
- Doherty, A.R.; Caprani, N.; Conaire, C.Ó.; Kalnikaite, V.; Gurrin, C.; Smeaton, A.F.; O’Connor, N.E. Passively recognising human activities through lifelogging. Comput. Hum. Behav. 2011, 27, 1948–1958. [Google Scholar] [CrossRef] [Green Version]
- Bolanos, M.; Dimiccoli, M.; Radeva, P. Toward storytelling from visual lifelogging: An overview. IEEE Trans. Hum.-Mach. Syst. 2016, 47, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Ferdous, M.S.; Chowdhury, S.; Jose, J.M. Analysing privacy in visual lifelogging. Pervasive Mob. Comput. 2017, 40, 430–449. [Google Scholar] [CrossRef]
- Wang, P.; Smeaton, A.F. Semantics-based selection of everyday concepts in visual lifelogging. Int. J. Multimed. Inf. Retr. 2012, 1, 87–101. [Google Scholar] [CrossRef] [Green Version]
- Petkov, N. Automatic segmentation of indoor and outdoor scenes from visual lifelogging. In Applications of Intelligent Systems: Proceedings of the 1st International APPIS Conference 2018; IOS Press: Amsterdam, The Netherlands, 2018; p. 194. [Google Scholar]
- Brophy-Warren, J. The New Examined Life: Why more people are spilling the statistics of their lives on the Web. The Wall Steet Journal, 6 December 2008. [Google Scholar]
- Hesse, M. Bytes of Life: For Every Move, Mood and Bodily Function, There’s a Web Site to Help You Keep Track. The Washington Post, 9 September 2008. [Google Scholar]
- Zillien, N.; Fröhlich, G.; Dötsch, M. Zahlenkörper. In Präsenzen 2.0: Körperinszenierung in Medienkulturen; Hahn, K., Stempfhuber, M., Eds.; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2015; pp. 77–94. [Google Scholar]
- Jayanthi, R.; Rama, S. IOT Based Smart Energy Tracking System. Int. J. MC Sq. Sci. Res. (IJMSR) 2017, 9, 98–108. [Google Scholar] [CrossRef]
- Kaye, J.J.; McCuistion, M.; Gulotta, R.; Shamma, D.A. Money talks: Tracking personal finances. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Toronto, ON, Canada, 26 April–1 May 2014; pp. 521–530. [Google Scholar]
- King, C.E.; Sarrafzadeh, M. A survey of smartwatches in remote health monitoring. J. Healthc. Inform. Res. 2018, 2, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Paré, G.; Leaver, C.; Bourget, C. Diffusion of the digital health self-tracking movement in Canada: Results of a national survey. J. Med. Internet Res. 2018, 20, e177. [Google Scholar] [CrossRef]
- Reeder, B.; David, A. Health at hand: A systematic review of smart watch uses for health and wellness. J. Biomed. Inform. 2016, 63, 269–276. [Google Scholar] [CrossRef]
- Williamson, B. Algorithmic skin: Health-tracking technologies, personal analytics and the biopedagogies of digitized health and physical education. Sport Educ. Soc. 2015, 20, 133–151. [Google Scholar] [CrossRef]
- Maltseva, K.; Lutz, C. A quantum of self: A study of self-quantification and self-disclosure. Comput. Hum. Behav. 2018, 81, 102–114. [Google Scholar] [CrossRef]
- Meadows, M.; Hatzakis, T. Getting to know you? New business models for privacy and the quantified self. Soc. Bus. 2018, 8, 13–20. [Google Scholar] [CrossRef]
- Lupton, D. “Sharing Is Caring:” Australian self-trackers’ concepts and practices of personal data sharing and privacy. Front. Digit. Health 2021, 15. [Google Scholar] [CrossRef]
- Schiel, R.; Bieber, G.; Thomas, A. Smartwatch und-phone für Therapie-und Monitoring bei Kindern und Jugendlichen mit Typ-1-Diabetes. Diabetol. Und Stoffwechs. 2014, 9, P146. [Google Scholar] [CrossRef]
- Piwek, L.; Ellis, D.A.; Andrews, S.; Joinson, A. The rise of consumer health wearables: Promises and barriers. PLoS Med. 2016, 13, e1001953. [Google Scholar] [CrossRef]
- Fotopoulou, A.; O’Riordan, K. Training to self-care: Fitness tracking, biopedagogy and the healthy consumer. Health Sociol. Rev. 2017, 26, 54–68. [Google Scholar] [CrossRef] [Green Version]
- Lentferink, A.J.; Oldenhuis, H.K.; de Groot, M.; Polstra, L.; Velthuijsen, H.; van Gemert-Pijnen, J.E. Key components in eHealth interventions combining self-tracking and persuasive eCoaching to promote a healthier lifestyle: A scoping review. J. Med. Internet Res. 2017, 19, e277. [Google Scholar] [CrossRef] [PubMed]
- Salamati, F.; Pasek, Z.J. Personal wellness: Complex and elusive product and distributed self-services. Procedia CIRP 2014, 16, 283–288. [Google Scholar] [CrossRef] [Green Version]
- Haggerty, R.J.; Mrazek, P.J. Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research; National Academies Press: Cambridge, MA, USA, 1994. [Google Scholar]
- Ajana, B. Personal metrics: Users’ experiences and perceptions of self-tracking practices and data. Soc. Sci. Inf. 2020, 59, 654–678. [Google Scholar] [CrossRef]
- Liao, Y. Sharing Personal Health Information on Social Media: Balancing Self-presentation and Privacy. In Proceedings of the 10th International Conference on Social Media and Society, Toronto, ON, Canada, 19–21 July 2019; pp. 194–204. [Google Scholar]
- Ohme, J.; Araujo, T.; de Vreese, C.H.; Piotrowski, J.T. Mobile data donations: Assessing self-report accuracy and sample biases with the iOS Screen Time function. Mob. Media Commun. 2021, 9, 293–313. [Google Scholar] [CrossRef]
- Gimpel, H.; Nißen, M.; Görlitz, R. Quantifying the quantified self: A study on the motivations of patients to track their own health. In Proceedings of the 34th International Conference on Information Systems, ICIS 2013, Milan, Italy, 15–18 December 2013. [Google Scholar]
- Kent, R. Self-tracking health over time: From the use of Instagram to perform optimal health to the protective shield of the digital detox. Soc. Media+ Soc. 2020, 6, 2056305120940694. [Google Scholar] [CrossRef]
- Lyall, B. The ambivalent assemblages of sleep optimization. Rev. Commun. 2021, 21, 144–160. [Google Scholar] [CrossRef]
- von Entreß-Fürsteneck, M.; Buchwald, A.; Urbach, N. Will I or will I not? Explaining the willingness to disclose personal self-tracking data to a health insurance company. In Proceedings of the 52nd Hawaii International Conference on System Sciences, Maui, HI, USA, 8–11 January 2019. [Google Scholar]
- Skatova, A.; Ng, E.; Goulding, J. Data donation: Sharing personal data for public good. In Application of Digital Innovation; N-Lab: London, UK, 2014. [Google Scholar]
- Evans, R.; Ferguson, E. Defining and measuring blood donor altruism: A theoretical approach from biology, economics and psychology. Vox Sang. 2014, 106, 118–126. [Google Scholar] [CrossRef] [Green Version]
- Penner, L.A.; Dovidio, J.F.; Piliavin, J.A.; Schroeder, D.A. Prosocial behavior: Multilevel perspectives. Annu. Rev. Psychol. 2005, 56, 365–392. [Google Scholar] [CrossRef] [Green Version]
- De Waal, F.B. Putting the altruism back into altruism: The evolution of empathy. Annu. Rev. Psychol. 2008, 59, 279–300. [Google Scholar] [CrossRef]
- Skatova, A.; Goulding, J. Psychology of personal data donation. PLoS ONE 2019, 14, e0224240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, A.; Wyatt, S.; Kelly, S.E. The Gift of Spit (And the Obligation to Return it) How consumers of online genetic testing services participate in research. Inf. Commun. Soc. 2013, 16, 236–257. [Google Scholar] [CrossRef]
- Foufi, V.; Timakum, T.; Gaudet-Blavignac, C.; Lovis, C.; Song, M. Mining of textual health information from Reddit: Analysis of chronic diseases with extracted entities and their relations. J. Med. Internet Res. 2019, 21, e12876. [Google Scholar] [CrossRef]
- Baboukardos, D.; Gaia, S.; She, C. Social performance and social media activity in times of pandemic: Evidence from COVID-19-related Twitter activity. Corp. Gov. Int. J. Bus. Soc. 2021, 21, 1271–1289. [Google Scholar] [CrossRef]
- Guo, J.W.; Radloff, C.L.; Wawrzynski, S.E.; Cloyes, K.G. Mining twitter to explore the emergence of COVID-19 symptoms. Public Health Nurs. 2020, 37, 934–940. [Google Scholar] [CrossRef]
- Seifert, A.; Christen, M.; Martin, M. Willingness of older adults to share mobile health data with researchers. GeroPsych 2018, 31, 41. [Google Scholar] [CrossRef]


{kind=link}
| Probability to Donate | Sharing Results | Showing Results | ||
|---|---|---|---|---|
| N | Valid | 919 | 919 | 919 |
| Missing | 0 | 0 | 0 | |
| Mean | 4.51 | 2.09 | 1.94 | |
| Median | 4.60 a | 0.64 a | 0.80 a | |
| Std. Deviation | 3.542 | 3.195 | 2.662 | |
| Variance | 12.549 | 10.209 | 7.088 | |
| Skewness | 0.087 | 1.374 | 1.320 | |
| Std. Error of Skewness | 0.081 | 0.081 | 0.081 | |
| Kurtosis | −1.431 | 0.509 | 0.737 | |
| Std. Error of Kurtosis | 0.161 | 0.161 | 0.161 | |
| Range | 10 | 10 | 10 | |
| Minimum | 0 | 0 | 0 | |
| Maximum | 10 | 10 | 10 | |
| Percentiles | 25 | 0.92 b | .b,c | .b,c |
| 50 | 4.60 | 0.64 | 0.80 | |
| 75 | 7.73 | 3.54 | 3.40 | |
| Unstandardized Coefficients | Standardized Coefficients | ||||
|---|---|---|---|---|---|
| B | Std. Error | Beta | t | Sig. | |
| (Constant) | 27.892 | 6.436 | 4.333 | 0.000 | |
| Frequency of tracking | 4.459 | 1.985 | 0.072 | 2.246 | 0.025 |
| Vital-parameter tracking | 5.864 | 2.430 | 0.078 | 2.413 | 0.016 |
| Sharing results | 1.282 | 0.459 | 0.116 | 2.791 | 0.005 |
| Showing results | 1.338 | 0.581 | 0.101 | 2.302 | 0.022 |
| Reason: Wanting Feedback | 1.558 | 0.465 | 0.124 | 3.352 | 0.001 |
| Relevancy of privacy | −1.090 | 0.419 | −0.082 | −2.600 | 0.009 |
| donating money | 1.191 | 0.320 | 0.116 | 3.715 | 0.000 |
| Sex | 6.921 | 2.390 | 0.091 | 2.896 | 0.004 |
| Age | −3.988 | 1.782 | −0.073 | −2.238 | 0.025 |
| Unstandardized Coefficients | Standardized Coefficients | ||||
|---|---|---|---|---|---|
| Model | B | Std. Error | Beta | t | Sig. |
| (Constant) | 40.094 | 2.983 | 13.441 | 0.000 | |
| Curiosity—no goal | −1.512 | 2.880 | −0.020 | −0.525 | 0.600 |
| Self-Motivation | 5.751 | 2.608 | 0.081 | 2.205 | 0.028 |
| Self-Monitoring | 5.230 | 2.603 | 0.074 | 2.009 | 0.045 |
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| (Constant) | 35.482 | 1.584 | 22.398 | 0.000 | |
| reason: proud | 0.049 | 0.447 | 0.005 | 0.110 | 0.913 |
| reason: desire for feedback | 2.008 | 0.516 | 0.160 | 3.890 | 0.000 |
| reason: to motivate others | 1.462 | 0.467 | 0.149 | 3.130 | 0.002 |
| no reason | 0.868 | 0.376 | 0.075 | 2.309 | 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pilgrim, K.; Bohnet-Joschko, S. Donating Health Data to Research: Influential Characteristics of Individuals Engaging in Self-Tracking. Int. J. Environ. Res. Public Health 2022, 19, 9454. https://doi.org/10.3390/ijerph19159454
Pilgrim K, Bohnet-Joschko S. Donating Health Data to Research: Influential Characteristics of Individuals Engaging in Self-Tracking. International Journal of Environmental Research and Public Health. 2022; 19(15):9454. https://doi.org/10.3390/ijerph19159454
Chicago/Turabian StylePilgrim, Katharina, and Sabine Bohnet-Joschko. 2022. "Donating Health Data to Research: Influential Characteristics of Individuals Engaging in Self-Tracking" International Journal of Environmental Research and Public Health 19, no. 15: 9454. https://doi.org/10.3390/ijerph19159454